
Abstract
Introduction
Myotonic dystrophy type 1 (DM1) is characterized by a lifelong progressive muscular weakness associated with life-threatening events such as chronic respiratory failure (CRF). Early identification of patients at risk remains challenging.
Objective
To identify clinical and biological markers predictive of CRF onset and survival in a large DM1 cohort.
Methods
We conducted a retrospective cohort study of 126 DM1 adult patients followed from 2000 to 2024 at Rouen University Hospital. The primary outcome was the first forced vital capacity (FVC) ≤ 70% of predicted value. Prognostic factors were analyzed using Cox proportional hazards models with the start of follow-up at the time of diagnosis of DM1 and were followed until the outcome occurred, or death (censorship according to Kalbfleisch & Prentice approach to competing risks).
Results
During a median follow-up of 12.5 years, 45 patients developed FVC ≤ 70%. Muscular impairment rating scale (MIRS) (HR: 1.85, 95%CI:1.30–2.63) and conduction/rhythm disorders (HR: 3.13, 95%CI: 1.37–7.31) at diagnosis were independent predictors of FVC ≤ 70% adjusted on age, female sex (HR: 1.54, 95%CI: 0.82–2.91) and cataract at diagnosis (HR: 0.50, 95%CI: 0.22–1.16). CTG repeats ≥400 was associated with a doubled risk of respiratory decline but did not reach statistical significance. The 20-year mortality rate was 32%. MIRS (HR: 2.34, 95%CI:1.22- 4.51), male sex and older age at diagnosis significantly predicted death.
Conclusions
Muscular impairment and cardiac rhythm/conduction disorders at diagnosis were strong predictors of respiratory complications. MIRS, male sex and older age at diagnosis were predictors of mortality in DM1. These prognostic markers should inform clinical management strategies to improve survival in DM1 patients.
Keywords
Introduction
Myotonic dystrophy type 1 (DM1) is a rare muscular disease characterized by a lifelong progressive muscular weakness that can be associated with life-threatening events such as chronic respiratory failure (CRF). These events are difficult to predict and contribute to a shortened life expectancy.1–4
Clinically, DM1 is characterized by progressive muscle weakness and myotonia. The extent of muscular impairment is associated with multiorgan dysfunction, such as cardiac, neurologic and ocular systems. 5 Mathieu et al. highlighted the relevance of the muscular impairment rating scale (MIRS) in predicting multisystem involvement and prognosis in DM1 patients. 6 Moreover, cardiovascular complications, including cardiac arrhythmias and conduction defects, are documented in DM1 and have been linked to the length of the CTG repeats.7–10 The impact of CTG repeats on respiratory muscle function is poorly understood, but it is believed to contribute to significant respiratory disturbances. 4 Muscle weakness and myotonia can lead to respiratory complications such as pneumonia, atelectasis, and CRF, all of which can adversely affect the survival rate.
Recent investigations aimed to understand the relationship between different organ dysfunction of the disease and the progression of respiratory dysfunction. 4 Respiratory involvement is thought to more likely occur in patients with longer disease evolution, larger CTG expansion, and weaker individuals.
However, findings were inconsistent: some studies demonstrated correlations between larger CTG expansions and reduced vital capacity or forced vital capacity, as well as with hypercapnia, or the need for non-invasive ventilation5,11,12 whereas others reported no such associations.13,14 These discrepancies likely reflect methodological limitations and small sample sizes, and no clear consensus exists regarding CTG repeats size as a predictor of respiratory decline.
By contrast, muscular impairment showed a more consistent relationship with respiratory involvement. Some studies found that higher Muscular Impairment Rating Scale (MIRS) scores were significantly associated with impaired spirometry parameters;3,5 though cross-sectional design and small sample size studies limit the robustness of these findings.
Explaining this methodological difficulty is likely the definition of respiratory failure. Respiratory failure has variably been defined by spirometry cutoffs (FVC < 50% predicted), by arterial blood gas abnormalities (diurnal hypercapnia), by nocturnal hypoventilation criteria from sleep studies.15,16 Given this heterogeneity, conclusion regarding the course of the respiratory impairment remains difficult to provide.
Therefore, improved understanding of the risk factors associated with chronic respiratory failure in DM1 could lead to timely and targeted pulmonary assessments and therapeutic interventions. 17 Consensus guidelines on CRF management in DM1 emphasize the importance of pulmonary assessment to enhance prognosis. 15 Despite consensus guidelines, important questions remain regarding respiratory failure in DM1 patients. Reliable prognostic markers are therefore needed to tailor respiratory follow-up which can improve survival. 17
The aims of this study were to identify clinical and biological markers predictive of CRF onset and survival in patients with DM1.
Material and methods
Study design
We conducted a retrospective cohort study involving all adult patients with a DM1 diagnosis performed between 2000 and 2024 at Rouen University Hospital. The study was approved by the institutional ethics committee of our university (approval number E2022-31). This study was conducted according to STROBE guidelines (Appendix).
Population
Patients were screened from electronic health records (EHRs) using two sources (the department's registry and hospital diagnostic coding systems). All data was extracted from EHRs and paper-based health records, except death. In addition to health records, deaths were extracted from the French death registry provided by the Institut National de la Statistique et des Études Économiques (INSEE); 18 linkage errors were considered more likely for female patients due to maiden names. DM1 could be diagnosed due to family screening or spontaneous visits guided by symptoms. Diagnosis was based on symptoms and/or family history and increased CTG repeats.
A total of 157 patients were screened from our database. All patients with a diagnosis of DM1 and followed in the neuromuscular diseases centre of Rouen university hospital were included. Patients diagnosed before January 1st, 2000 were excluded in a post hoc decision, due to poor medical charts and screening bias. Screening bias was confirmed by the Pearson's R correlation between age at diagnosis and date of diagnosis in patients diagnosed before year 2000 (R = 0.49, 95% CI 0.11 to 0.74, p = 0.01).
Outcomes
Events corresponding to DM1 natural history were recorded. Recorded events were: (1) death, (2) first pulmonary function test (PFT) with forced vital capacity (FVC) ≤ 70% of predicted value, (3) noninvasive ventilation (NIV) initiation, (4) first occurrence of cataract, (5) first occurrence of a cardiac rhythm or conduction disorder, (6) first fitting of a pacemaker or defibrillator. Events could occur before or after the diagnosis of DM1. Imprecise date of events (with year but not month and day) mentioned in consultation reports were imputed to June 15th.
Data collection
The first assessment included a systematic examination by a neurologist. Variables at diagnosis included demographics, CTG repeats, and muscular impairment rating scale (MIRS). 6
During the follow-up, further assessment was done by specialists (pulmonologist, cardiologist, ophthalmologist).
Cardiac assessment included clinical examination and a 24-h ambulatory ECG Holter monitoring, repeated annually or earlier if symptoms.
Pulmonary function tests (PFT) were done if patient had respiratory symptoms (e.g., dyspnoea). Repetitions of PFT were possible depending on the results of first PFT and patient's evolution. Before respiratory failure, PFT were performed depending on clinical symptoms. During follow-up of respiratory failure, patients were followed every 6 to 12 months if stable, every 3 to 6 months if under NIV.
PFT was performed with spirometry or plethysmography (Jaeger, Germany) according to standards of the European Respiratory Society. 19 Values were expressed as a percentage of the normal predicted value for age, sex and height. 20 These procedures are repeated at least three times, and the best value is recorded.
We adopted FVC ≤ 70%predicted as chronic respiratory failure definition, since it represents a pragmatic, objective, and widely used threshold in neuromuscular cohorts, while avoiding the variability of symptom-based assessments or sleep-study definitions and allowing comparability with several previous DM1 studies.5,11,21
NIV was initiated for either nocturnal hypoventilation (confirmed by sleep studies) or daytime hypercapnia (confirmed by diurnal arterial blood gas), as recommended. 22
Date rounding
In the analyzable sample (n = 126 patients), only the year of diagnosis, but not month or day was known in 74 / 126 (58.7%) patients. This was simply imputed to June 15th of the year. All dates of cataract, pacemakers and cardiac rhythm/conduction disorders were recorded with the precision of one year and were imputed to June 15th of the year. All dates of PFTs, NIV initiations and deaths were recorded with month and day precision.
Statistical methods
Statistics used prognostic models based on Cox models with the start of follow-up (time 0) at the time of diagnosis of the DM1. For each outcome, patients were followed until the outcome occurred, or death (censorship according to Kalbfleisch & Prentice approach to competing risks). In other cases, they were administratively censored on January 1st, 2025. Patients for whom the outcome occurred before baseline (time 0) were excluded from the related Cox prognostic model (left censorship) but were included in the Kaplan-Meier curves. Rubin's rule and Wald's tests were used to pool and estimate hazard ratios in the multivariable Cox models fitted on 500 multiply imputed data sets.
Covariables of the prognostic models (female sex, number of CTG repeats ≥ median, age at diagnosis, MIRS at time of diagnosis, cataract at time of diagnosis and cardiac rhythm/conduction disorder at time of diagnosis) were chosen a priori, based on the literature, as predictors of poor prognosis. Two variables had missing data: MIRS at the time of diagnosis, multiply imputed by predictive mean matching models and number of CTG repeats, multiply imputed by logistic regression. All Cox models covariables and outcomes (quantitative time to outcome and binary outcome) were used as multiple imputation predictors.
For 6 patients with cataract, the date of cataract was not found but the history of cataract was already mentioned in the DM1 diagnostic visit. The 6 missing times to diagnosis of cataract were simply imputed by the predicted value of a linear model explaining the time between diagnosis of the DM1 and the cataract by a linear effect of the age at diagnosis and a linear effect of the date of diagnosis (ranging from 2000 to 2024) in the sample of patients with cataract occurring before diagnosis of the DM1. One patient had an unknown diagnosis date, but since the first PFT was in 2003 and the mean delay between diagnosis and first PFT was 3.6 years, the diagnosis was assumed to be before 2000 and the patient was excluded. After simple imputation of time to cataract and exclusion of patients diagnosed before 2000, Cox models were fitted with other data multiply imputed by chained equations with 500 samples.
Results
Of the 126 patients included (64 female, mean ± standard deviation age at diagnosis: 36.2 ± 16.5 years), 103 had at least one PFT and 23 had no PFT at all and were assumed to have FVC > 70% of the predicted value at all times.
The median number of CTG repeats was 400 (interquartile range (IQR): 132, 700). Excluding 3 patients with no muscular impairment rating scale (MIRS) data, 52 / 123 (42.3%) patients had no muscular symptoms at diagnosis (MIRS = 1) highlighting the impact of familial screening in early disease detection. In contrast, 16 (13.0%) patients had proximal limb weakness (MIRS ≥4), indicating potential diagnosis delays (Table 1).
Baseline characteristics of patients at the time of diagnosis of DM1.
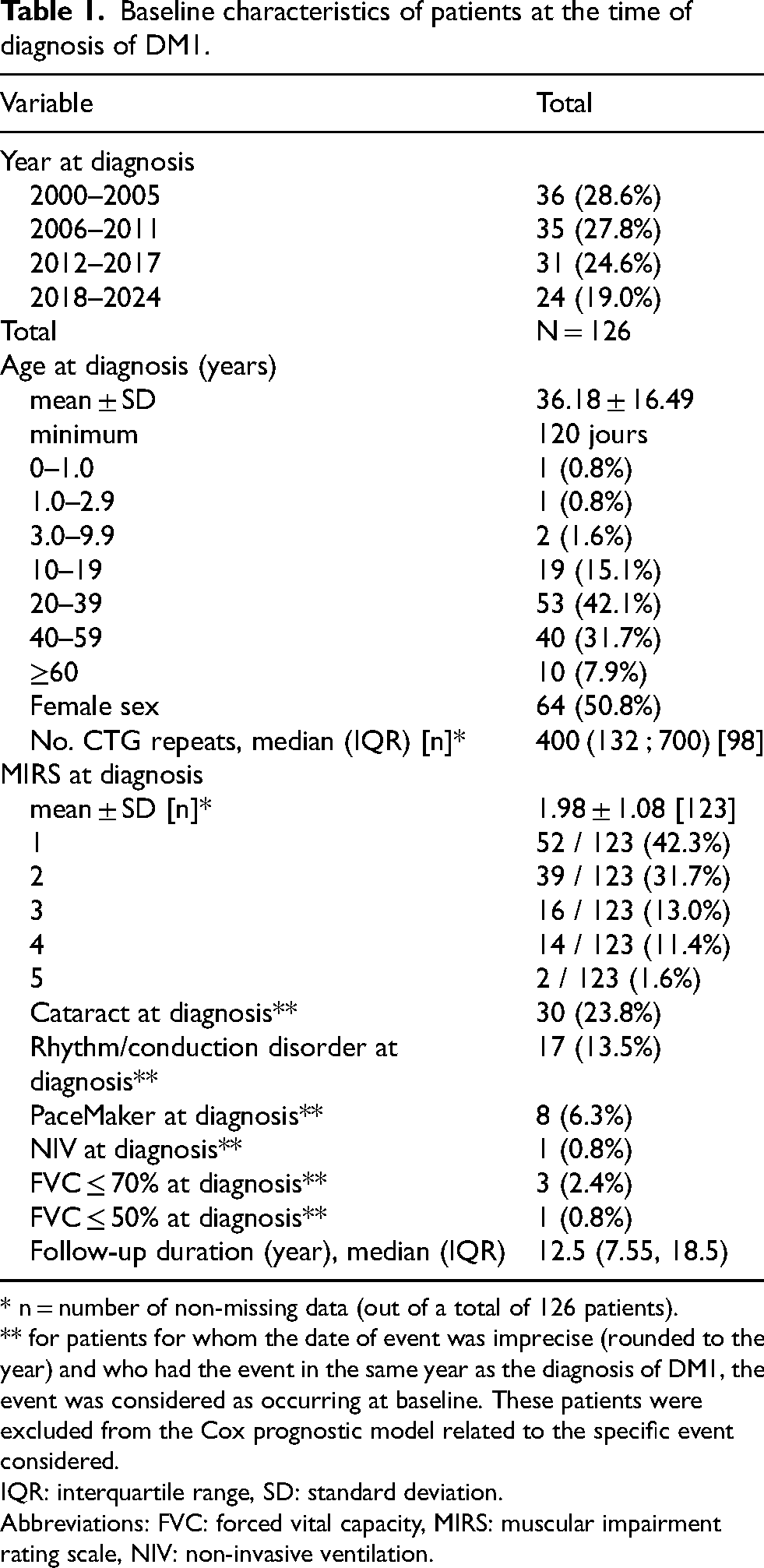
* n = number of non-missing data (out of a total of 126 patients).
** for patients for whom the date of event was imprecise (rounded to the year) and who had the event in the same year as the diagnosis of DM1, the event was considered as occurring at baseline. These patients were excluded from the Cox prognostic model related to the specific event considered.
IQR: interquartile range, SD: standard deviation.
Abbreviations: FVC: forced vital capacity, MIRS: muscular impairment rating scale, NIV: non-invasive ventilation.
The median duration of follow-up until death or administrative censorship in 2025, was 12.5 (IQR: 7.55, 18.50) years. Excluding 3 FVC ≤ 70% occurring before diagnosis, 45 first FVC ≤ 70% (36.6%) occurred during follow-up. Respiratory data of the first PFT with FVC ≤ 70% are shown in Table 2.
Respiratory data at first pulmonary function test with forced vital capacity ≤70% of predicted value.
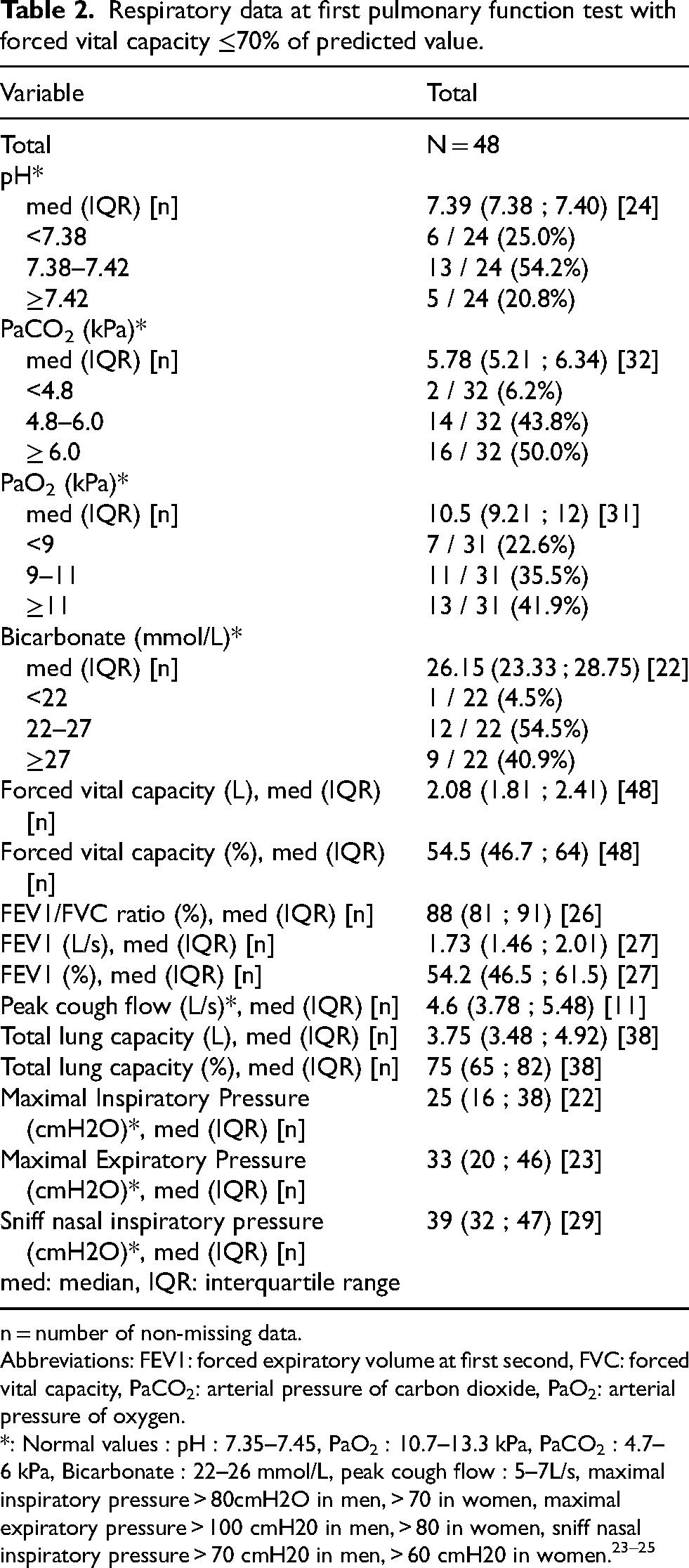
n = number of non-missing data.
Abbreviations: FEV1: forced expiratory volume at first second, FVC: forced vital capacity, PaCO2: arterial pressure of carbon dioxide, PaO2: arterial pressure of oxygen.
*: Normal values : pH : 7.35–7.45, PaO2 : 10.7–13.3 kPa, PaCO2 : 4.7–6 kPa, Bicarbonate : 22–26 mmol/L, peak cough flow : 5–7L/s, maximal inspiratory pressure > 80cmH2O in men, > 70 in women, maximal expiratory pressure > 100 cmH20 in men, > 80 in women, sniff nasal inspiratory pressure > 70 cmH20 in men, > 60 cmH20 in women.23–25
At first PFT with FVC ≤ 70%, half of the patients had hypercapnia (PaCO2 ≥ 6 kPa), while 23% had hypoxemia (PaO2 < 9 kPa). Inspiratory and expiratory muscle strength were markedly reduced with median maximal inspiratory pressure of 25 (IQR: 16, 38) cmH2O and expiratory pressure of 33 (IQR: 20, 46) cmH2O.
In the 126 patients we observed 26 NIV initiations between 0.77 year before diagnosis and 20.91 year after diagnosis. In the 26 patients with NIV initiation, we found the following causes of NIV initiation: hypercapnia (≥ 6 kPa) for 15 patients, following acute hypercapnic respiratory failure for 2 patients, and not clearly stated in 9 patients.
Of the 26 patients with NIV initiation, 13 had a PFT at ± 180 days of the NIV initiation. The mean ± standard deviation of FVC (% of predicted value) was 59.6% ± 19.4% (n = 10 observations) and PaCO2 was 6.58 ± 0.81 (n = 12 observations) for this PFT.
Overall, in the 126 patients, 103 had at least one PFT with a median delay from diagnosis at +1.3 (IQR: 0.4 ; 6.2) years for the first PFT performed at Rouen University Hospital. Of these 103 patients with at least one PFT, the mean ± standard deviation of FVC was 78.1% ± 21.8% (95% CI: 73.6% to 82.5%), lower than normal (100%) but higher than at NIV initiation (59.6%); mean ± SD PaCO2 at first PFT was 5.64 ± 0.91 kPa (95% CI: 5.42 to 5.87, n = 66 observations), lower than at NIV initiation (6.58 kPa).
Multivariable Cox models revealed that the MIRS at the time of diagnosis and cardiac conduction/rhythm disorders at diagnosis were independent predictors of respiratory decline. CTG repeat length demonstrated a trend toward association with respiratory decline (Table 3). Notably, every incremental increase in MIRS score at diagnosis elevated the hazard of FVC ≤ 70% by 85% (HR: 1.85, 95%CI 1.30 to 2.63, p = 0.0006). Cardiac rhythm or conduction disorders at diagnosis were independently associated with respiratory decline (HR: 3.13, 95%CI 1.37 to 7.13, p = 0.007). CTG repeats ≥400 was associated with a doubled risk of respiratory decline.
Multivariable cox prognostic models explaining the delay between diagnosis and events (time 0 = diagnosis), with censorship at death for all outcomes but death.
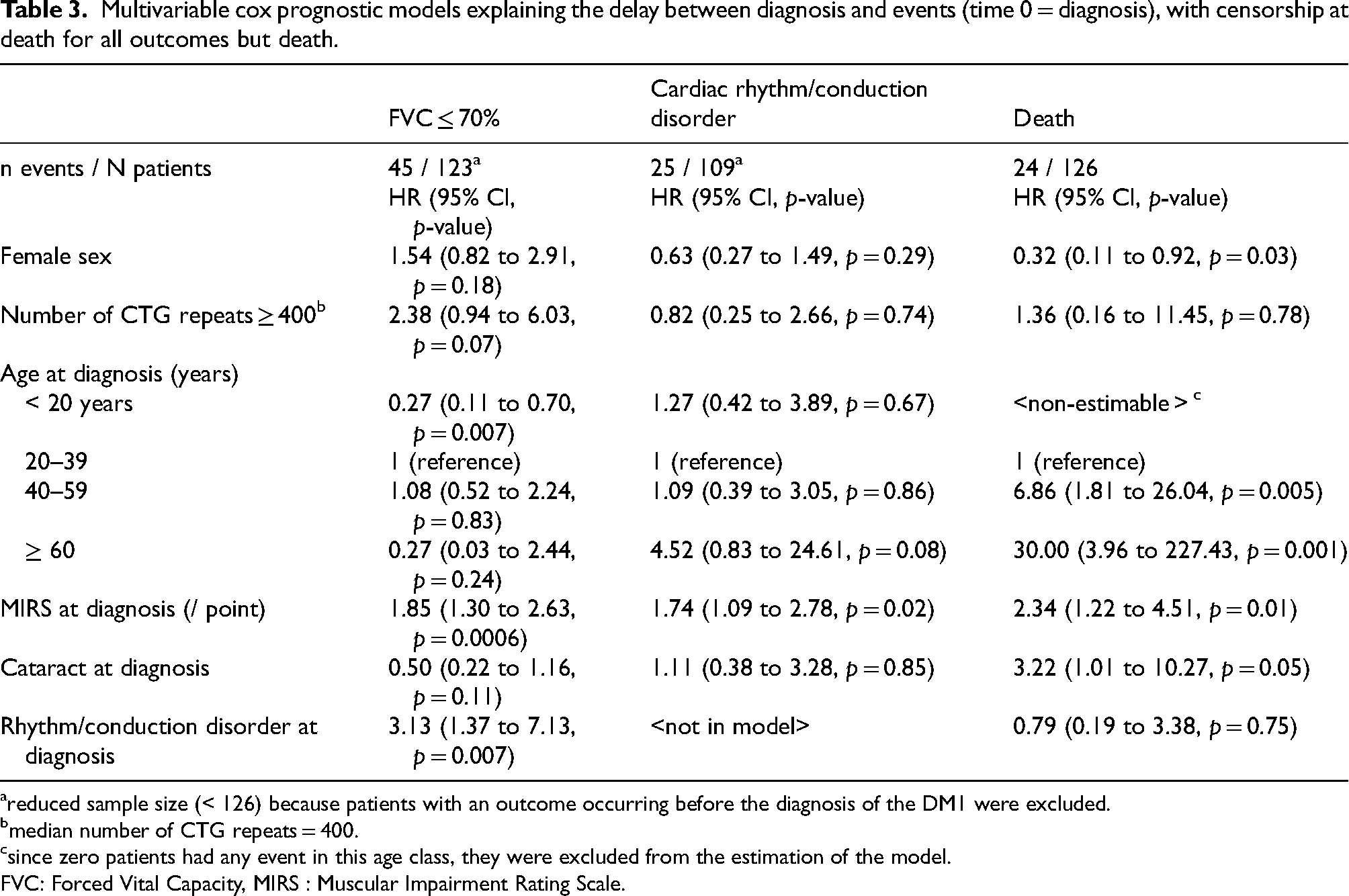
reduced sample size (< 126) because patients with an outcome occurring before the diagnosis of the DM1 were excluded.
median number of CTG repeats = 400.
since zero patients had any event in this age class, they were excluded from the estimation of the model.
FVC: Forced Vital Capacity, MIRS : Muscular Impairment Rating Scale.
The 20-years overall mortality rate was of 31.9% (95%CI 18.7 to 43.0%) (Figure 1, Table 4). MIRS severity (HR: 2.34 per MIRS point, 95%CI 1.22 to 4.51, p = 0.01), older age at diagnosis, and male gender emerged as significant independent predictors of mortality (Table 3).
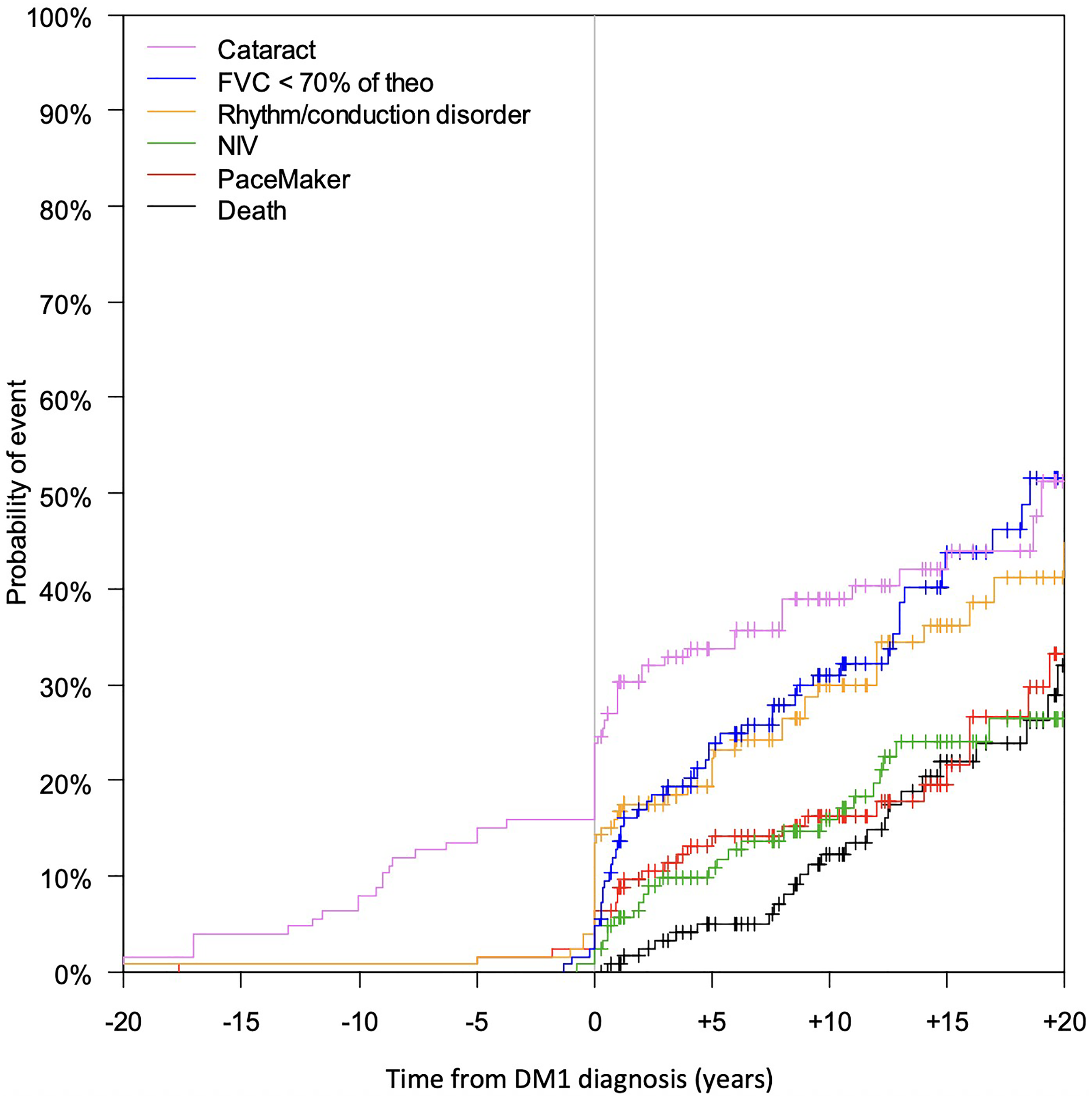
Kaplan-Meier curves describing the occurrence of events from time of DM1 diagnosis. Negative values are possible, describing events occurring before the diagnosis of DM1. The strong “step” observed at the time of diagnosis can be explained by rounding of event dates to the year (i.e., the diagnosis of DM1 and the event occurred in the same year but not necessarily at the same date); crosses represent censorships.
Kaplan-Meier estimated cumulative risks of events.
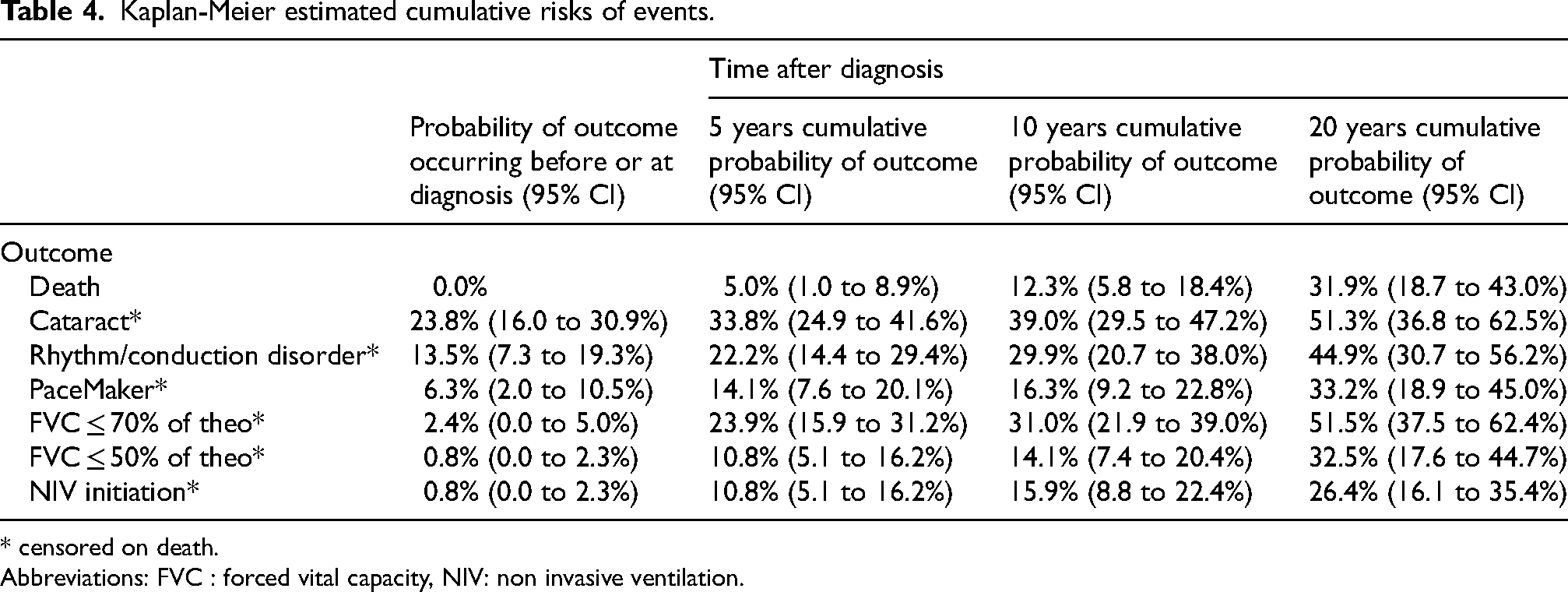
* censored on death.
Abbreviations: FVC : forced vital capacity, NIV: non invasive ventilation.
Figure 2 described the occurrence of death and respiratory failure from the time of DM1 diagnosis according to age, sex, CTG repeats, cardiac rhythm or conduction disorders at diagnosis, MIRS at diagnosis and cataract. FVC ≤ 70% was more likely to occur in patients with MIRS at diagnosis ≥3, presence of cardiac rhythm or conduction disorders at diagnosis, CTG repeats ≥400 and older age.
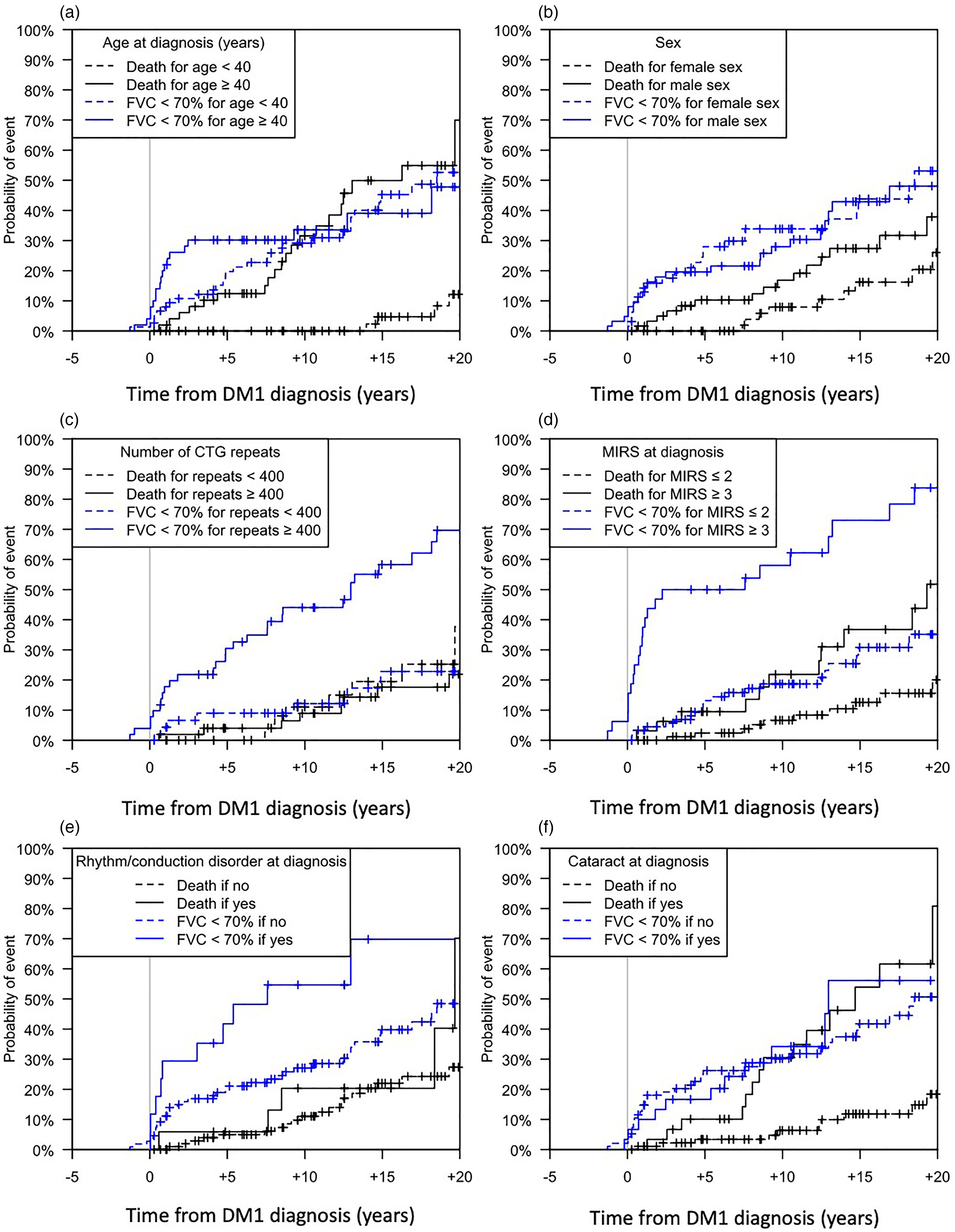
Kaplan-Meier curves describing the occurrence of events from time of DM1 diagnosis according to exposition factors. Negative values are possible, describing events occurring before the diagnosis of DM1.
Interestingly, a cataract preceded the DM1 diagnosis in 30 (23.8%) patients (Table 1
Discussion
Our findings confirmed the prognostic value of muscular impairment (MIRS) and cardiac conduction or rhythm disorders for respiratory failure; as well as male sex, older age and MIRS for mortality in DM1. These markers should inform clinical decisions, particularly regarding the timing of interventions such as pulmonary function testing and therapeutics.
Our results highlighted a high prevalence (36.6%) of respiratory failure (FVC ≤ 70%), with a 20-years respiratory failure probability of 52% from diagnosis of DM1. This aligns with previous findings showing high prevalence of respiratory insufficiency; being the most frequent organ failure.26–28 Despite its complex etiology, respiratory failure has mainly been linked to muscular weakness and restrictive lung patterns. 3 Mathieu et al. highlighted the relevance of the muscular impairment rating scale to assess the disease severity in DM1 patients. 6 The disease pathophysiology, characterized by muscular weakness and myotonia, leads to a restrictive lung pattern and ultimately chronic respiratory failure. Begin et al. previously demonstrated the link between inspiratory muscle weakness and chronic hypercapnia. 3
In our study, we chose to use FVC ≤ 70%of predicted value as a pragmatic and widely used marker of restrictive impairment in neuromuscular disorders. The choice of 70% rather than 50% of predicted value was made to detect early respiratory impairment, as a value of 50% often reflects already advanced disease. A potential limitation of our study is the possibility of submaximal effort during PFTs in patients with facial weakness or cognitive impairment, which may lead to underestimation of respiratory function. To minimize this bias, all pulmonary function tests were performed by trained technicians with extensive experience in neuromuscular disease assessments, and only technically acceptable maneuvers were retained according to European Respiratory Society standards. 19 Furthermore, the respiratory laboratory in our University Hospital conducts a high volume of assessments, averaging approximately 1200 to 1500 PFTs per year, which ensures familiarity with these measures and reliability of the respiratory data included in our study.
Our study identifies early prognostic markers to help in timely respiratory intervention for DM1 patients. Early detection of respiratory decline could enable timely initiation of NIV as well as physiotherapy to slow down respiratory decrease. Chatwin and Simonds 29 suggested that in-exsufflation used alongside home mechanical ventilation and physiotherapy can improve survival. Inspiratory and expiratory muscle weakness showed a strong predictive value for respiratory insufficiency, as suggested by Wenninger et al. 30 Other authors have suggested the utility of arterial blood gas and spirometry indices as primary indicators for NIV requirement. 31 In our study, peak flow, maximal inspiratory and expiratory pressure as well as sniff nasal inspiratory pressure were not available in a sufficient proportion of patients to allow robust analysis. Moreover, these parameters require pulmonary function testing that are not easily available. Our study proposes an improved method for screening early respiratory failure, which can be effectively utilized by neurologists and medical practitioners.
Although previous cohorts have suggested the association between disease severity and respiratory outcomes, 16 our study is one of the largest cohorts with one of the longest follow-ups, evaluating the benefit of MIRS at diagnosis as a prognostic tool in incident respiratory failure, independent of age, sex and CTG size. Our results suggest that MIRS, a simple bedside scale, can stratify respiratory risk early in the disease course, even in ambulatory conditions.
Cardiac rhythm/conduction dysfunction have been described as risk factors for sudden death in DM1, 8 but their relationship to respiratory decline has been less studied. Our findings suggest that cardiac abnormalities may serve as a marker of severity, correlated with respiratory muscle involvement. Our findings are consistent with a previous Italian longitudinal study reported by Mazzoli et al. 32 In this study, cardiac comorbidities were present in more than 60% of patients and in over 90% of those requiring NIV and were independently associated with faster FVC decline and greater risk of respiratory deterioration. Association may be explained by the effect of arrhythmias and conduction defects, possibly impairing perfusion of respiratory muscles and contributing to respiratory fatigue. However, the causal direction of this association remains uncertain, as both organ systems may be independent expressions of the multisystem disease severity.
Concerning genetic markers, other studies reported correlations between the size of the CTG repeats and the age of the first symptoms and the severity of the disease. 2 Cardiac disorders were also associated with CTG repeat expansion.9,33,34 However, this correlation remains controversial.35,36 Few studies focused on showing the association between respiratory muscles weakness and the expansion of CTG repeats.4,12,32 This correlation is important since it would allow early identification of patients at risk of respiratory failure. Monteiro et al. had found that CTG repeats were correlated with hypoxemia. 12 This finding is corroborated by Boussaïd et al., who highlighted the relationship between high CTG repeats and compromised respiratory function, particularly peak cough flow. 4 In our study CTG repeats ≥400 was associated with a doubled risk of respiratory decline but did not reach statistical significance (p = 0.07). This trend toward an association between genetics and respiratory failure should encourage implementing genetic testing to assess CTG repeats early in the disease course to tailor monitoring frequency and intervention strategies to improve long-term patient outcomes.
The relationship between age at diagnosis and respiratory decline in our study suggested that younger DM1 patient could have a slower respiratory decline. A few retrospective longitudinal studies have evaluated the respiratory decline. Thil et al. 21 suggested that the rate of decline could vary over time with an average annual decline in FVC of approximately - 0.7%. Abrupt deterioration was seen early in the course of disease. Mazzoli et al. findings 32 highlighted a correlation between earlier disease onset, younger patient age, and accelerated respiratory deterioration in DM1 patients. Our findings could be explained by a less long evolution of the disease given a protective factor compared to patients of age 20 to 39 years old.
On the other hand, our finding that older age at diagnosis was associated with increased risk of mortality may reflect that late diagnosis potentially due to diagnostic delay, during which unrecognized respiratory decline had already occurred, increasing the severity of the complications. This finding has also been found by Werlauff et al. 28 who demonstrated that older age at diagnosis was associated with a higher risk of mortality with an average age at death of 58 years; and diagnostic delay may increase the risk of adverse event.
Beside older age, our results found male sex, and higher MIRS at diagnosis as predictors of mortality. These findings are consistent with recent literature. A gender disparity has been reported in previous study highlighting that men have more severe muscular impairment, worse cardiac and respiratory involvement, and higher mortality compared with women. 37 Our results also showed that higher MIRS at diagnosis correlated with higher mortality, underlining the importance of muscle weakness examination at diagnosis to predict further severity and guide follow-up.
Together, these findings emphasize that early recognition is necessary as diagnostic delay is frequently observed in DM1 and may postpone targeted follow-up and medical interventions. Early diagnosis of cataract also could serve for reducing delay in DM1 diagnosis. Our result regarding the diagnosis of cataract have also been suggested by other authors as helpful to prevent diagnostic delay. 38 Indeed, Cataract represents a frequent organ manifestation in DM1. Although there is no clear pathophysiological rationale linking cataract to respiratory impairment, we considered it relevant to include in our analysis given its ease of documentation and its value as an early diagnostic marker.
Limitation
Study limitations include its retrospective, single-center design limiting generalizability. However, we obtained one of the largest cohorts of DM1 patients.
A further limitation of our study lies in its observational design, which is not well suited to determine the causal effect of non-invasive ventilation on outcomes. NIV was not prescribed at random; rather, its initiation reflected a clinical indication in patients with more advanced respiratory involvement, making it a marker of disease severity rather than an intervention that can be directly compared between individuals. This created both an indication bias (patients receiving NIV are by definition sicker than those who do not) and a potential contraindication bias (frailer patients or those with significant comorbidities may not be adherent to NIV despite meeting criteria).
Moreover, we cannot know whether arterial blood gas (ABG) are prognostic biomarkers because they were not performed without symptoms. Arterial blood gases were not performed systematically in our center, which means in our retrospective methodology we were not able to answer the utility of ABG as prognostic biomarkers. Due to the non-systematic nature of ABG testing, we did not include it as a predictor in the Cox models.
Central dysfunction in DM1 may account for the observed variability in CTG repeats prediction of FVC ≤ 70%. There was a non-significant trend of association between CTG repeats and risk of FVC ≤ 70%. This lack of significance could be explained by a moderate association between CTG repeats and respiratory failure. Respiratory failure has two components: central and peripheral. The cause of the central component is not well known and may be less related to CTG repeats than the peripheral component. 39 However, our study was not designed to explore central component and its contribution to the lack of significance in the association between CTG repeats and FVC ≤ 70%.
In practice, the proposed biomarkers could help identify patients who may benefit from earlier PFTs, especially in centers where routine respiratory follow-up is not performed in asymptomatic patients. For example, a patient diagnosed with DM1, MIRS ≥3, and cardiac rhythm or conduction defect would be considered high-risk and warrant early PFT after diagnosis.
In conclusion, muscular impairment and cardiac disorders identified at diagnosis were independent predictors of respiratory failure in patients with DM1, after adjustment for age and sex. These findings provide novel, clinically actionable markers available at the time of diagnosis, supporting earlier and more personalized decisions regarding pulmonary monitoring. To prevent respiratory failure, patients with MIRS ≥3, cardiac disorders and maybe CTG repeats over 400 and older age should benefit of early respiratory evaluation.
Supplemental Material
sj-docx-1-jnd-10.1177_22143602251386258 - Supplemental material for Predictors of respiratory failure and survival in myotonic dystrophy type 1
Supplemental material, sj-docx-1-jnd-10.1177_22143602251386258 for Predictors of respiratory failure and survival in myotonic dystrophy type 1 by Marie-Anne Melone, Ivana Dabaj, Maxime Patout, André Gillibert, Elise Artaud-Macari, Lucie Guyant-Marechal, Anne-Laure Bedat-Millet, Anne-Marie Guerrot, Mathieu Salaun, Soumeya Bekri, Antoine Cuvelier and Abdellah Tebani in Journal of Neuromuscular Diseases
Footnotes
Ethical considerations
This study involves human participants and was conducted in accordance with the Declaration of Helsinki. It was approved by the institutional ethics committee of our university hospital under approval number E2022-31.
Consent to participate
All subjects were informed of the use of their data for research purposes through institutional communication in accordance with the GDPR and French data protection regulation. No opposition was recorded.
Authors contributions
MAM, ID, MP, AG, SB, AC and AT contributed to conceptualization, data curation, formal analysis, investigation, methodology, project administration, resources, software, supervision, validation, visualization, writing – original draft and editing. EAM, LGM, ALB, AMG, MS contributed to data curation, investigation, review and editing.
All authors had final responsibility for the decision to submit for publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MAM received support for attending meetings from Asten Santé, Epione Santé. MP received grants from Fisher & Paykel, Resmed, Asten Santé, consulting fees from Philips Respironics, Air Liquide Médical, Resmed, ISIS medical, Asten Santé, GSK, honoraria for lecture from Philips Respironics, Asten Santé, Resmed, Air Liquide Medical, SOS Oxygène, Antadir, Chiesi, Jazz Pharmaceutical, Loewenstein, Fisher & Paykel, Bastide Medical, Orkyn, Elivie, ISIS medical, support for attending meetings from Asten Santé, Vitalaire, SANOFI, participation on data safety monitoring board for Resmed, Philips Respironics, Asten Santé, stocks on Kernel Biomedical, receipt of equipment from Philips, Respironics, Resmed, Fisher & Paykel. Other authors declare not to have any conflicts of interest that may be considered to influence directly or indirectly the content of the manuscript.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.