
Abstract
Purpose:
To investigate how parents of children with SMA who are treated with disease modifying therapies cope with hopes and worries related to disease progression, and to investigate their needs for counseling and rehabilitation initiatives.
Methods:
The design of this study was qualitative using the Interpretive Description methodology and Joyce Travelbee's theory of interpersonal aspects. The method was semi-structured interviews conducted in Denmark at the homes of the parents or through the online platform Teams between February 29 and May 3, 2024.
Findings:
Seventy-five parents representing 41 children were invited. Twenty-six parents of 20 children participated in the study. Twenty-four parents were interviewed at home and two were interviewed online. The key element of the parents’ narratives was the reality of the diagnosis: the trajectory toward the diagnosis, getting the diagnosis, and the hope related to the effect af disease modifying therapies. At the same time, they experienced grief related to the uncertainty of the disease progression while hoping for normalcy in the future: a ‘normal’ child and a ‘normal’ life. Finally, they struggled with balancing professional counseling to maintain hope.
Conclusions:
The families need coordinated, multidisciplinary care and information on disease modifying therapies, including what they can actively do to increase the effectiveness of the treatment. Counseling should include facilitated peer-support and acknowledge differences in children in terms of development, how they respond to the disease modifying therapy, and its long-term effects. Health professionals must tailor their support to the families’ needs and sustain their hopes for the future.
Keywords
Introduction
Spinal muscular atrophy (SMA) is a hereditary neurogenerative disease caused by mutations in the SMN gene. 1 SMA is a progressive disease that causes muscle weakness of the muscles in the extremities and trunk.1,2 SMA varies widely in severity, and the incidence is estimated to be 1 in 10,000 live births globally.1–3 SMA has historically been classified into five subtypes depending on onset and achieved motor function.1–3 Type I is characterized by onset before 6 month of age, and untreated children with this type will not sit independently. 2 Type II is characterized by onset between 6 and 18 months, and untreated children with this type will not stand and walk independently. Type III is characterized by onset after 18 months, often after the children have achieved independent ambulation. Type 0 and IV are rare forms. 2 The symptoms vary in extent depending on time of onset, but involve muscle weakness, delayed and impaired motor function, scoliosis, respiratory problems, and affected bulbar muscles that impair orofacial functions, including deficits in voice, articulation and swallowing.4,5
With the introduction of disease modifying therapies, there has been a dramatic positive change in survival, achievement of motor function, and in the overall progression of the disease, and consequently the prior classifications are phased out.2,6 Three therapies aiming at restoring the SMN protein have been approved for treatment. They can be divided into two groups: gene therapy, where the defective SMN1 gene is replaced (Onasemnogene abeparvovec), and splicing modifiers of SMN2 (Nusinersen and Risdiplam).2,6–8 The three disease modifying therapies were approved by FDA and EMA from 2016–2021.9,10
The disease modifying therapies are now available worldwide – however, their availability can vary according to type of SMA, age, and legislation and insurance coverage of the specific country.11,12 With disease modifying therapies, many countries have introduced newborn screening to ensure early diagnosis and treatment which are paramount to achieve favorable outcomes for the child with SMA. 13 The first disease modifying therapy for SMA in Denmark was approved for SMA type I and II in 2018, and in 2024 the treatment was approved for all types of SMA. 14 Newborn screening for SMA was introduced in Denmark in 2023. 15
The disease-modifying treatments are not curative, but children with infantile onset SMA who receive treatment have better chances of survival and reach more major motor milestones than those not treated. 16 This means that more Danish families now live with SMA. The treatments offer new perspectives on life with SMA for children, their parents, and health professionals as they represent hope of improved health, quality of life, and participation, but are also associated with new challenges. 17
Having a child with a rare and possibly life-threatening or chronic genetic disease poses a significant challenge for the parents. The new approved targeted therapies have been shown to provide hope,18,19 however there are currently only approved treatments for 5% of all rare genetic diseases. Parents often take responsibility for finding and gaining access to treatment in the hope of alleviating their child's symptoms and suffering. 20 Feeling gratitude and hope can strengthen parents’ adjustment to the fact that their child has to live with a rare condition and thereby promote positive experiences. 20 Knowledge about Danish parents of children with SMA who receive disease modifying treatment, their need for information and counseling on the diagnosis, treatment options, and prognosis, and how the health system caters to these needs is scarce.
The objective of this study was to investigate how parents of children with SMA who are treated with disease modifying therapies cope with hopes and worries related to disease progression, and to investigate their needs for counseling and rehabilitation initiatives.
Patients and methods
Design and theory
The design of this study was qualitative using the Interpretive Description methodology and Joyce Travelbee's theory of interpersonal aspects such as suffering, meaning, hope and communication.21–23
Interpretive Description is an inductive methodology seeking a coherent conceptual description and in-depth interpretation of relationships and patterns within a phenomenon with the aim of improving practice. 21 The methodology requires integrity in the research purpose arising from a current practice challenge, an understanding of what we know and do not know based on evidence. Interpretive Description recognizes that the ‘clinical brain’ is not satisfied with ‘pure’ description and therefore seeks primarily to investigate connections, relationships and patterns in the phenomenon being researched. 21
To analyze, decipher, and understand hope and grief, Joyce Travelbee's theory was used as inspiration as it deals with how people search for meaning in the things that happen to them. 23 Travelbee describes how health professionals must support the sick person and the family in maintaining hope and avoiding hopelessness. She argues that, as professionals, we can support families with tools to find hope, and that through this, changes leading to something better can and will occur. 23 In addition, health professionals can make themselves available and address the concerns and difficulties of the sick person or their family, while at the same time covering physical care and rehabilitation needs. 23
Setting
The study was conducted in the context of the National Rehabilitation Center for Neuromuscular Diseases (RCFM) 24 which is a highly specialized private hospital under the National Board of Health. 25 The majority of children with SMA in Denmark are referred to the center for lifelong specialized rehabilitation and counseling. RCFM collaborates with and facilitates rehabilitation in local community health and social settings and in the regional services.26,27 The professionals at RCFM work closely with families who have children with SMA in multidisciplinary teams consisting of nurses, doctors, physiotherapists, occupational therapists, psychologists, and social workers.
The author group consisted of researchers and health professionals (all women) working at RCFM, with different backgrounds (nurse, physiotherapists, doctor, and anthropologist) and many years of experience within the field of neuromuscular diseases (NMD). The interviews were carried out by the first author (nurse and professor in neuromuscular rehabilitation) who did not know the participants before the study.
Sample and participants
The inclusion criteria were parents of children <14 yrs of age with SMA receiving disease modifying therapy. The parents had to speak and understand either Danish or English to be able to participate in the interviews. At the time of inclusion, parents of 48 children with SMA registered at RCFM met the inclusion criteria. Some of the parents represented the same child and were cohabiting. Parents who met the inclusion criteria were invited by email sent through a secure digital mailbox [e-Boks] used by hospitals or other public authorities when they contact patients directly.
Data generation
The participants had a choice of being interviewed in their home or online. Twenty-four parents opted for an interview at home and two for an interview through the online platform of Teams. All interviews were conducted by the first author between February 29 and May 3, 2024. The interviews were semi-structured. Some parents participated as a couple, and during most interviews, the child with SMA was at home, but did not participate in the interviews. All families participated voluntarily, and confidentiality was maintained throughout the interviews. All participants were promised anonymity and were informed that they should only answer what they wanted to.
Patient involvement processes and bringing forward patient priority issues for research are integral to research at RCFM where we adhere to the Strategy for Patient-Oriented Research Patient Engagement Framework (SPOR). 28 To ensure relevance of the study's aim and to ensure that the questions were relevant and did not cause the parents to be emotionally negatively affected, we involved a young person with SMA in their twenties who had recently started disease modifying therapy and two parents of a child receiving disease modifying therapy. Some of the interview questions were changed based on the feedback from the three people. All interviews were conducted without interruption, and all families indicated that the questions were relevant and appropriate. Had the parents felt emotional distress during the interviews they would have had the opportunity to be referred to a psychologist at RCFM.
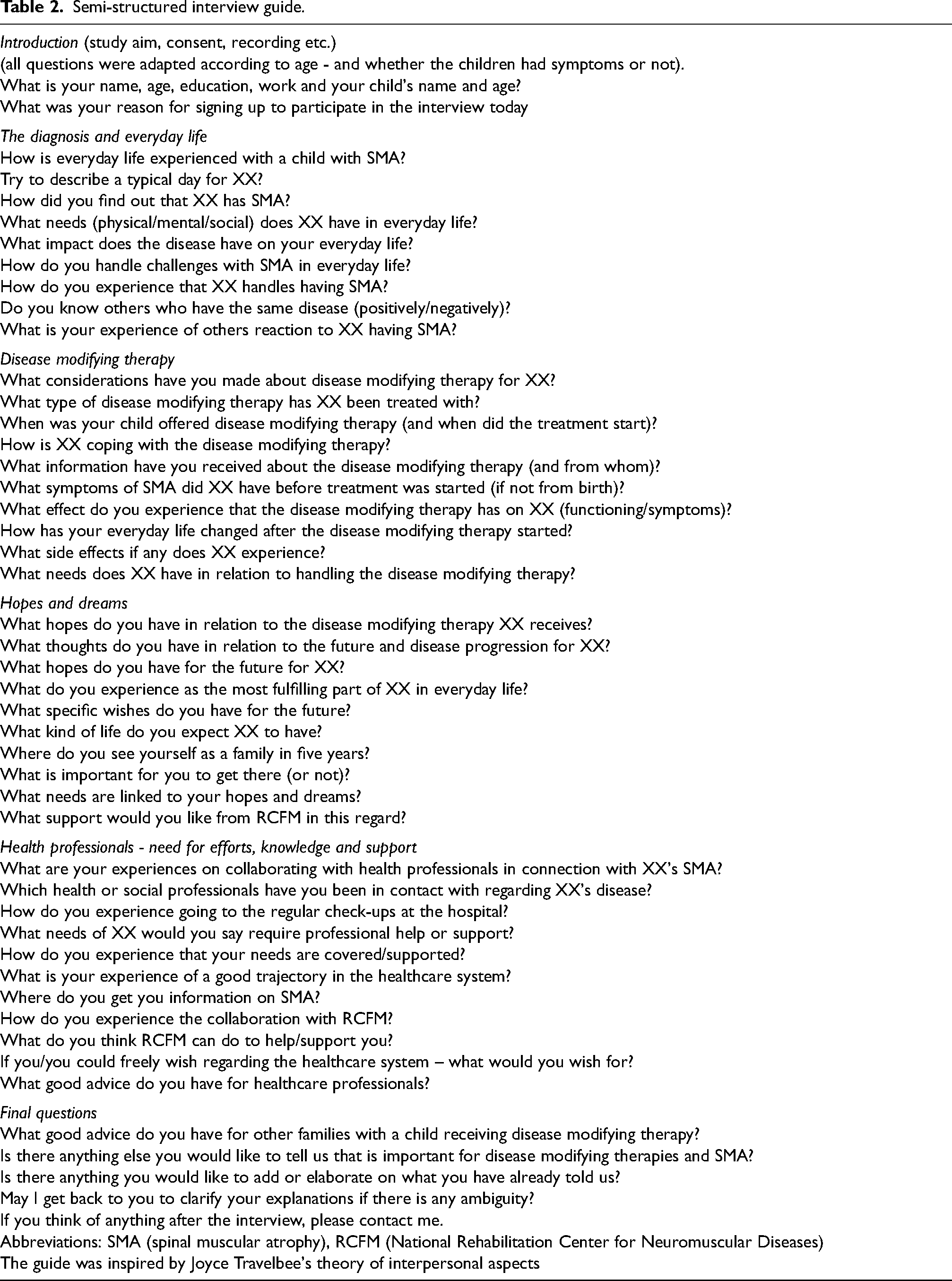
Demographic data on participants and their children with SMA are displayed in Table 1. All participants and children were anonymized. The questions related to diagnosis, daily life, the disease modifying therapy, hopes and dreams, and their need for professional knowledge and support. (Table 2).
Demographic data on participants and their children with spinal muscular atrophy (SMA).
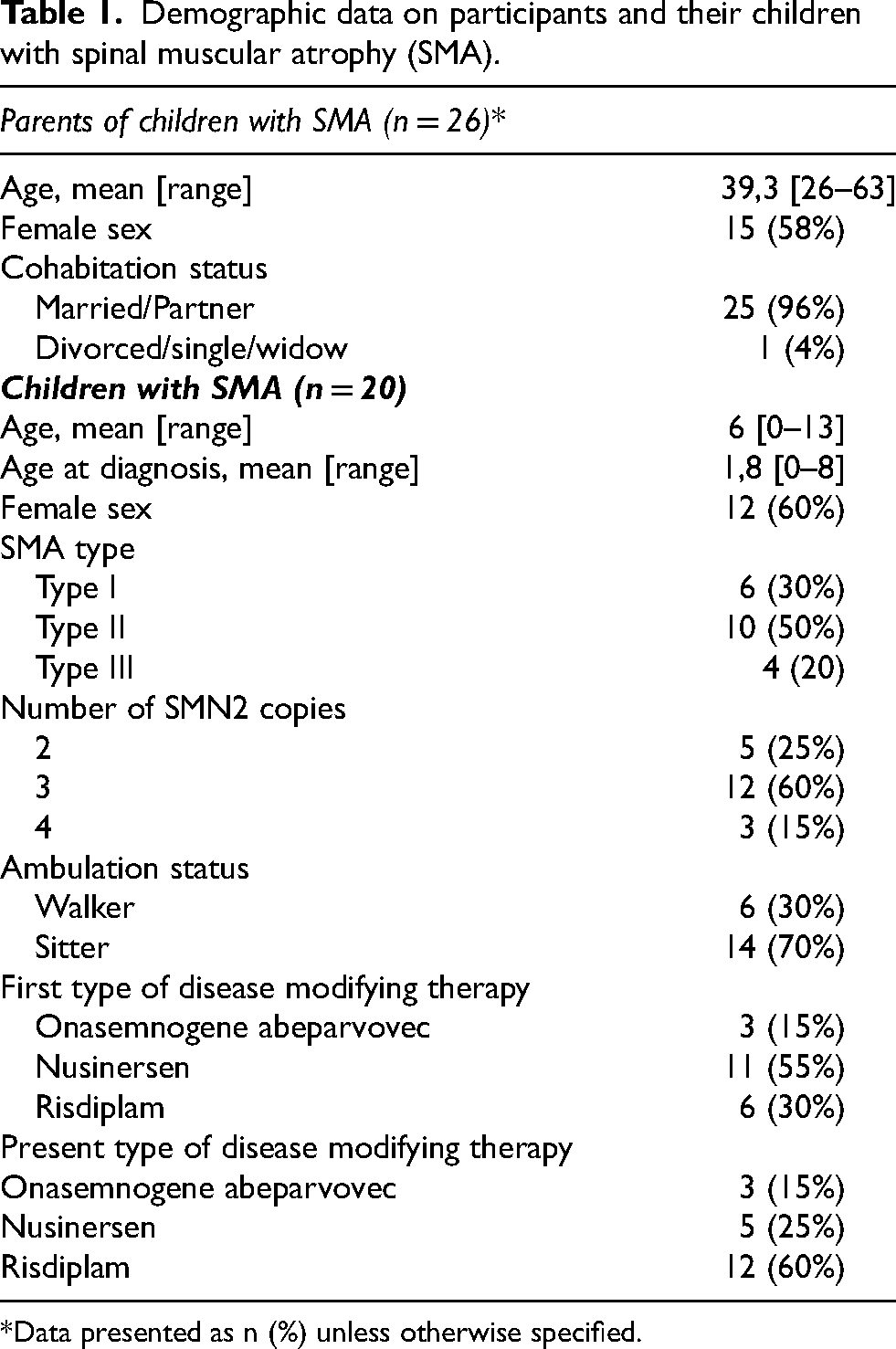
*Data presented as n (%) unless otherwise specified.
Semi-structured interview guide.
Data analysis
The analysis was inspired by Joyce Travelbee's theory of interpersonal aspects such as suffering, meaning, hope, and communication21–23 and guided by the four-step process in the Interpretive Description methodology (Table 3):
Illustration of the analysis and coding process leading up to the final categorical themes - guided by the Interpretive Description Methodology and the lens of Joyce Travelbee's theory of interpersonal aspects such as suffering, meaning, hope and communication.

Step 1) Data was transcribed into text and uploaded to NVivoTM16, and an initial coding was conducted. Four of the authors were engaged in the first analytical step (CH/PZD/UW/AM), reading the interviews and defining codes which we used to code all data. We defined 10 initial codes.
Step 2) A process distinguishing between the codes’ specific conditions and general patterns in relation to the research question took place. Three of the authors (CH/PZD/AM) condensed the 10 codes into five subthemes. We made a critical appraisal of the relationships within data and their relevance for thematic options leading to the primary categorization.
Step 3) A critical assessment of relationships within data, as well as their relevance for thematic options leading to the primary categorization (CH/PZD/AM). In step three of the analysis, two categorical themes were defined.
Step 4) The main messages, categorical themes and subthemes are established along with the final interpretation and thematic structure in relation to the research question (CH/PZD/AM) (Table 3). The final condensation, description and interpretation and the final findings, their hierarchies and relationships are illustrated in a figure in the results section (CH/PZD/AM).
Findings
In all, 75 parents representing 41 children were invited. Twenty-six parents (∼35%) to 20 children participated in the study (Table 1). The analysis showed how parents of children with SMA who have been offered disease modifying therapies cope with hopes and worries in relation to the disease progression and revealed their needs for information, advice, and rehabilitation initiatives. One important element of the parents’ narratives was the reality of the diagnosis: the trajectory toward the diagnosis, getting the diagnosis, and the hope related to the disease modifying therapy, but also grief related to uncertainty of the future and disease progression. When they realized that life had taken an unexpected turn, hoping for normalcy – a ‘normal’ child and a ‘normal’ life – became central for the parents. The new life situation led to challenges with managing everyday life and maintaining both their own and their children's social relations. They needed professional support, but were challenged with balancing professional counseling, not getting overwhelmed by information and losing hope at an early stage. They found it hard to cope with the prospect of their children's future dependency, and they needed to learn from and share knowledge with others (Figure 1).
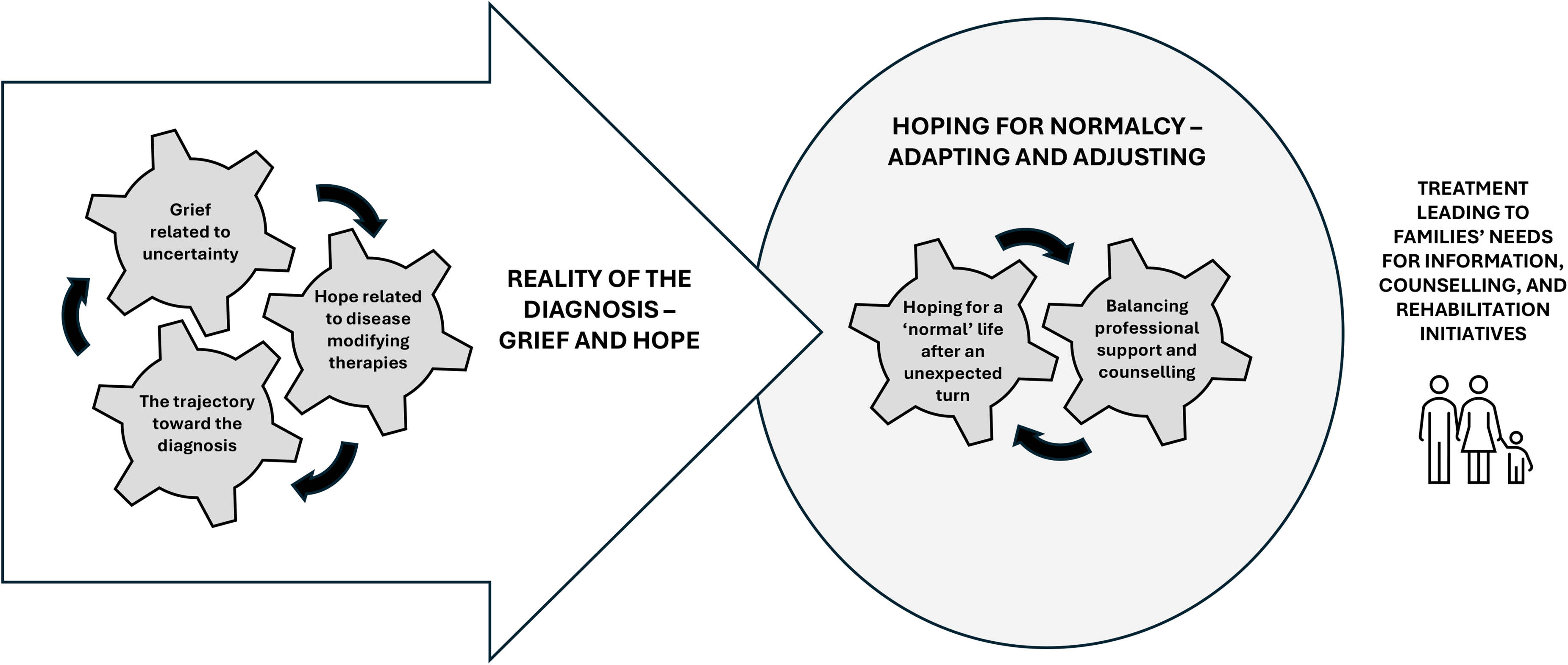
Understanding how parents of children with SMA who are treated with disease modifying therapies cope with hopes and worries related to disease progression, and their needs for counseling and rehabilitation initiatives.
Reality of the diagnosis - grief and hope
The trajectory toward the diagnosis
For the parents whose children were not diagnosed through newborn screening, the time leading up to the diagnosis had been long and difficult. They had all realized something was wrong with their child; some had noticed a decrease in physical function and feared it was serious, others had found out through the health visitor who came to their house after birth, or through relatives. Once referred to diagnostic assessment, the road toward the diagnosis could still be long and uncertain. For parents whose children were diagnosed through newborn screening, the diagnosis came as a shock. They had left the hospital with what they thought was a healthy child, only to find out that their child was seriously ill.
I got a call from the chief physician at XX hospital, he said that a disease had been found in the heel prick test, and it was a very serious muscle disease. So, when you get this call and this message… well I don't think I fully understood that it was real. Muscle disease, that's a very broad term. It could be some kind of arthritis I thought or something else. [xxx] Then he said, But there are some treatments for the disease now that you can treat your child with. But we must find the specific type of her disease” and stuff like that. [xxx] Then he just said “You must promise me one thing. After you hang up, you must not Google this disease”. [xxx] “You have to come in tomorrow”. Oh no… I came into the living room, and my husband said “Who was it?”, and then I just broke down and….(Mother to a one-year-old girl, ID15)
I didn’t realize until we got home what kind of message we had received… it was serious shit. The combination of incurable and progressive and life-shortening, those were the three words that were connected. That meant that we probably wouldn't…that XX probably wouldn't survive. It was a huge shock. I totally broke down and of course so did my wife. But as I said, she had probably suspected it. We were waiting at home, and it wasn't very nice to be all alone. At the time we hadn’t had any contact with the hospital, except for a call. Everything was uncertain and everything fell apart. At the hospital we spoke to the treating doctors and were introduced to the fact that there was a possibility of some treatment. (Dad to a seven-year-old boy, ID12).
Hope related to disease modifying therapies
The parents were grateful for the healthcare system having made disease modifying therapies available. The treatment represented hope for the parents and for those children who were old enough to understand the implications of their disease and the treatment possibilities. Parents who had fought to have the authorities approve the treatments and whose children had lived the first part of their lives without the possibility of disease modifying therapies hoped to reverse or at least stop the disease progression. They hoped for small but important effects of the treatment and saw little improvements like their child being able to get up on the couch in a different way or walking on stairs differently. The parents of the very young children hoped that the treatment would mean survival, a cure, or a standstill in the disease progression.
I didn't know if, if I would still have my daughter by Christmas. I started planning her funeral in my head. It was very traumatic and very, very unpleasant… I remember that around Christmas, I really PRAYED for a miracle. Well… on Christmas Eve I really, really prayed for a miracle. I bought her a magic wand because I thought, well… This is what you need, honey. And it was like that. Completely. We went to the hospital, and they told us about the treatment. Well… well, it was a MIRACLE. That it existed. It was…It was like a miracle, and that's how I still see it. (Mother to a one-year-old girl, ID1).
I said to the doctor, “I must ask you, the way I understood the disease before I came here today, chances were that he would be able to walk. Now it sounds completely different. How am I supposed to understand that?” Then he said: “If that's what you believe, then I have to say no. I can’t say anything but no, no, no and again no. The only expectation I can give you is that he will sit on his own. Everything else will be miracles”. Then I just broke down and thought, that's not what I was promised. I know that they can’t promise anything, but that's not what I expected. I expected that it would all just take a little longer and some extra work, but…there was a beacon and there was hope that we would end in a good place. Not because life in a wheelchair isn’t a good place but…it wasn’t…you know… I had hoped for something different, and he completely broke that dream. (Mother to a two-year-old boy ID3).
Grief related to uncertainty
Despite the positive effects of the disease modifying therapy, the parents were uncertain about their children's future. They worried about how much effect the treatment would have on their child's disease and how long it would last. They explained that they had pinned all their hopes on the disease modifying therapy only to realize it was not the cure or the miracle they had hoped for. They grieved that their children's functioning would be impaired despite the disease modifying therapy. The parents were also uncertain about what effect they could expect from the treatment and what to expect in general, and they worried that their hopes would be unrealistic and lead to disappointment.
Our dreams and hopes have always been that XX can walk. Will he walk by himself? Um…That has been our main goal. Not that he should be able to walk most of the day, but if he could just walk for some hours during the day, so that in the long run he can go to the bathroom by himself and maybe just walk a short distance from the car and in and out and things like that. It's our goal that he can do as much as possible. Because we were told that after approximately four years, the disease modifying therapy would stop working. That's what we were told at the time, that things would come to a standstill. […] We said: “We have to fight for the first four years to develop as many motor skills as possible”. He is developing every day and all the time. So yes…, 2 weeks ago he didn't dare to walk the distance from the chair to the kitchen. He can do it himself now. (Mother to a four-year-old boy ID7).
Dad: Well, we hope that he will be independent and he… that the disease progression will be postponed. That the disease modifying therapy will continue to work, so to speak.
Mother: And that he will keep getting it.
Dad: Yes, that he has access to treatment. It's really important. That's mostly what we're afraid of, isn't it…? If at some point you must pay a lot or something […].
Mother: But still…access to treatment when he's older is so important…Because we don't really know what it does…or doesn’t do?
Dad: I don't think they can… I mean, you can always argue that the children should have the disease modifying therapy. It's more like if something unexpected should happen… If there's a war or whatever. All those things make me think “Oh no”.
Mother: Catastrophic thoughts. Yes. Because we're so dependent on the treatment now, aren't we? So, we MUST have it!
Dad: Yes. We must have this disease modifying therapy so that he can have the best possible life!
(Parents to a one-year-old boy ID11).
Hoping for normalcy – adapting and adjusting
Hoping for a ‘normal’ life after an unexpected turn
The parents told that the child's severe diagnosis had caused an unexpected turn in life, going from a ‘normal’ life to a life different from what they had anticipated. After accepting that life turned out differently, the participants explained that even though they would adjust to their new life conditions, they were still weighed down by an underlying grief because they knew their child was in for a struggle. They constantly touched upon the ‘normal’ versus the ‘abnormal’ and explained how they focused on what was normal in the children's lives and did not dwell on thoughts about the future. All the parents talked about the wish for a ‘normal’ life for their children and noted that the doctor had said that their children could have a good life after receiving disease modifying therapy. They all described how important it was for them to keep the hope alive and that a way to do so was to live in the present. They hoped that their child would have a life that included friends, a partner, children, an education, and a job. The parents reflected on what a normal life would look like for a child with SMA.
She's going to live in there, and then she'll get the big room, when or if she has a wheelchair. Well…, of course we hope that she can have a normal a life as possible. And we hope she can go to the same school as XX. And they're building a huge new school. Yes…and we're just so happy that she is the way she is, because she's very outgoing, and she's very, very trusting, um…a little too trusting sometimes. (Mother to a two-year-old girl, ID2).
Well, I think you often hear people say that you must see the possibilities instead of the limitations… and tackle the problems when they arise…. and not let them overwhelm you…I think maybe you have to overestimate, the child's ability or you have to try to normalize it. Or think in relation to normalcy. Otherwise, you can easily end up almost giving up in advance. Because it's a bit more of a hassle, and they can't do as much anyway and all that. We've talked about that, that we think it's important that we also have big ambitions on her behalf, just like we have on behalf of our other child. (Dad of a twelve-year-old girl, ID6).
When we want to plan trips or visit family abroad it's super hard. So, we can't do that. I compare myself to my friends who have children the same age as mine, they have a different life. They just jump on a plane, visit people, and do this and that. We can't do that… XX finds it a bit hard too. We want to experience things. It is a constant challenge for your self-confidence when you’re unable to move around as you want to. (Mother to a three-year-old girl, ID19).
Many of the parents expressed a need for role models – other children with SMA – to be inspired from and share knowledge with, while some parents were reluctant to meet other people with SMA, afraid of what they might see. Most of the parents had gained a lot from meeting other parents, and their children from meeting other children with SMA. Having someone to emulate, who represented hope about living with the disease and the disease modifying therapy meant a lot to many of the parents.
Balancing professional support and counseling
Most of the parents expressed gratitude for the multidisciplinary rehabilitation initiatives from NMD health specialists. They had received help with coordinating counseling and guidance. Many of the parents requested knowledge on the effect and the long-term prospects of the disease modifying therapy. They acknowledged that the NMD health professionals were also new to the disease modifying therapies and therefore might be reluctant to say anything about the effect of the treatment and the children's development.
We got the information about the disease modifying therapy, that it COULD help. They didn't want to set our hopes too high by saying that they had seen this or that. Off course, we asked about the prospects of the disease modifying therapy and would it work? And then she said that “We can't say whether it will work or not”. (Mother to a thirteen-year-old boy, ID10).
We felt that the health professionals’ counselling was being forced upon on us. We had to sit down and decide on a wheelchair and a ceiling hoist and all those really annoying things…. Knowing that she was starting disease modifying therapy, and that was what mattered to us. It was disappointing. We were disappointed that there wasn't…Well, there wasn't even one word about the disease modifying therapy. There was no hope from the health professionals. There was no hope for us as a family. It was all purely negative. That was the feeling we got. But we were also in a place where we were extremely susceptible, and it didn't take much to send us off course. It wasn't a very good process […]. We just had a completely different approach to it. We had no doubt at all that when she started treatment, we would probably have a child who could do many, many other things. (Dad to a seven-year-old girl, ID9).
However, several of the parents had experienced feeling overwhelmed by information they had not requested, which had hampered their hopes and dreams. They explained that the information they had received from the health professionals had not been adjusted to their specific needs and had not accounted for the fact that the prognosis might change with the disease modifying therapies. This information overload, the parents explained, had caused worries and anxieties about the future and, for some, ruined their hopes for their children. The parents all emphasized the importance of adjusting information to the individual family and not just delivering the whole package’. They argued that their reason for not wanting all the information at once was that they wished to preserve their hopes and minimize worries, anxiety, and grief to keep their family life intact for as long as possible.
Mother: Yes, especially from the rehabilitation specialists, there was a focus on everything that she would never be able to do. “You can forget about this, and she will never be able to do that, and this you’ll have to redo, and here you need a special bed, and the bathroom, no, that's not big enough either. We have to do something about this”. It was difficult. One thing is that we just got so much information from the hospital, but that we suddenly also had to redo everything in our entire house, it was just completely wrong. All the things they said! “She will never be able to do that”…and it turned out that it wasn't right.
Dad: […] It was very overwhelming.
Mother: Yes, and you just don't need all this information on the same day. We were completely taken aback. That's how we experienced it, and it was difficult. […] We didn't have to know everything at once. After all, we had been diagnosed very, very, very recently.
Dad: And you have just recovered a little and then you’re put down again. (Parents of a five-year-old girl, ID17).
Discussion
Suffering is a human condition, and as a result, grief and anxiety can manifest in various ways and may be regarded as a threat to one's needs and stability. 23 When parents experience unforeseen events like their child being diagnosed with a severe disease, they may face instability and a temporary loss of control. 23 The parents in our study described this as a loss of clarity, a suddenly unstable world, a shock leading to drastic choices, not knowing how to handle the situation, or even wishing to commit suicide. Even though they had expected that something serious was wrong with their child and some of them had waited for a diagnosis for a long time, the shock of getting the diagnosis was immense to them all. Other studies have shown that a long diagnostic trajectory can cause distress among parents due to a lack of knowledge about the disease or because it is difficult for them to distinguish normal from abnormal development.29,30 The parents are confronted with fear of losing their child prematurely, fearing the child's loss of functions, having to make difficult treatment choices, and having to come to terms with lost hopes and expectations. 29
In the present study, the disease modifying therapies represented hope for the parents, and they explained that they considered the possible treatments a miracle. This has also been illustrated in other studies where parents described the disease modifying therapies of children with SMA as representing hope which can take different shapes and be used as a strength.17,31 Hope manifested differently in the parents: some hoped that the disease modifying therapy would remove all symptoms of the SMA, while others did not hope too much or found that hope gave rise to new challenges. 17 Likewise, the parents in our study had various approaches to hope, but common for them all were that they found some degree of hope in the disease modifying therapy. They were aware that children respond differently to the disease modifying therapies and were aware not to compare their child with other children with SMA.
Disease modifying therapies have been marketed since 2016, and their long-term effects are still tested in clinical trials.24,32–34 One effect is that the treatments result in new SMA phenotypes whose disease trajectories differ significantly from the natural history and cross traditional subtypes, and therefore clinical approaches must be modified. 35 The parents in our study expressed grief related to their child's disease and constant worries about the future related to the uncertainty of the disease progression and the long-term effect of the treatment. This is in line with research illustrating that, in spite of the positive effects of the treatments, parents still carry a significant emotional load manifesting as worries about living up to treatment criteria. 36 Additionally parents also experience dilemmas concerning treatment and care choices,17,37 and concerns for their child's future and health. 38 This is in line with our findings showing that the parents were in need of reassurance from the healthcare professionals regarding their parenting and their child's development.
Newborn screening is available in many countries, and this quicker road to diagnosis may reduce the emotional impact on families. However, it is important for health professionals to understand and support the grieving and uncertain parents by focusing on hope for the child and the positive effects of the treatment. The families that receive information about their child's SMA diagnosis a few days after it is born need support and counseling to handle the new reality. The parents need multidisciplinary care and care coordination with information on disease modifying therapies, support in their choices of treatment (or no treatment), and information on what they can actively do to assist the disease modifying therapy, e.g., with special nutrition and physical exercise. 3 In their support for and counseling of parents, health professionals must acknowledge that children with SMA are different and that they develop and respond to the disease modifying therapies in different ways.
Hope motivates human behavior and helps people handle difficult and stressful situations like severe illness and suffering. 23 Hope is a mental condition characterized by the wish or expectation to obtain something achievable like, in this study, treatment to cure a disease or to prevent death. 23 The parents in the present study were addressing hope for their child's life and living a ‘normal life’ after their lives had taken a turn for the unexpected when their child was diagnosed with SMA. In a prior study on children with SMA and Duchenne muscular dystrophy we also found that the emergence of new disease modifying therapies carried hope for the parents, hope for a cure for their child, or hope for a more independent life. 39 Research has, however, shown that parents and health professionals tend to be overly optimistic due to the immense hopes and expectations invested in the new disease modifying therapies.38,40 The sometimes idealized hopes may pose a challenge for the parents when they are confronted with a reality where the treatment may not be as effective as expected and they therefore have to downsize their hopes. 38 Still, parents have emphasized that even small positive physical changes are perceived as meaningful and carry hope. 40 It is important that the health professionals carefully balance counseling and guidance on disease modifying therapies, including the fact that the treatments sometimes do not have the positive effect that was hoped for, to sustain the parents’ hopes for their children's future. 39
The concept and terminology of ‘normal’ is complex, and health professionals’ use of the term ‘normal’ in their patient-related discourse may significantly shape interactions between them and their patients.41,42 Health professionals should be aware of their discourse and how they talk about normalcy, intentionally or unintentionally, as it may have a potential impact on what a patient or parent to a child patient might experience. 41 As health professionals we must increase our curiosity about how the idea of normalcy works and be critically reflective about how we use terminology about normalcy in our practices and patient communications. 41 After accepting that life did not turn out as expected, the parents adjusted to the new conditions, although with an underlying grief. The Danish psychologist Svend Brinkman argues that we are all like everyone else, like someone else, and like no one else.43,44 Brinkman's way of addressing normalcy may be useful for health professionals in counseling and endorsing hope for the families who wish for normalcy, emphasizing that every person and every family will be like everyone else, like someone else, and like no one else.
The parents in the present study were burdened by the many emotional and practical issues consuming their everyday lives and by the shifts in their lives regarding jobs and self-identity. Finding meaning when a child gets a serious illness can be difficult and pointless, nevertheless meaning often presents itself from the situation humans are in. 23 The parents all explained how they went from the overwhelming experience of the diagnosis into ‘management mode’ despite having different ways of handling the many everyday tasks. Despite their ability to act on practical issues, the parents experienced an underlaying grief because of the disease, knowing their child would always depend on others. Some parents also grieved their child's lack of social relations and over the absence of the social life and spontaneity they had had early in life. This is in line with a recent review that demonstrated several sources of psychosocial burden for parents of children with SMA, especially a negatively affected quality of life, moderate to high levels of caregiver burden and distress, and negatively affected physical and mental health. 45
The parents in the present study also reported a heavy psychosocial burden related to seeking and getting professional help and support and the stress related to the uncertainty. They found themselves caught between having received disease modifying therapy for their children but not knowing what to expect from it in the long run. The disease modifying therapies are new, and health professionals and researchers still do not know the long-term effects, meaning that the parents and children live with uncertainty, unsure of what to hope for, expect, and deal with.
Besides the psychosocial aspects, a recent survey among families with children with SMA treated with disease modifying therapies in Europe showed that families with a child with SMA spend 4 h per week in average on physiotherapy, and that 65% of the children experience nutrition problems with 20% being on a special diet. 46 Some families are overburdened by care tasks and struggle with unmet needs relating to information, care coordination, treatment decisions, and supportive care services. 45 It is therefore important to take professional initiatives to prevent caregiver burnout and to facilitate peer-support which has been shown beneficial for people with SMA and their families.45,47
Finally, some parents in the present study addressed the issue of receiving an overload of negative information from health professionals which made it difficult to maintain hope for their idea of a normal life for their child and for the family. A lack of sensitivity in how health professionals inform patients about a serious SMA diagnosis can compound the parents’ negative experiences. 29 Studies have shown that parents want disease-specific information and knowledge, targeted support in everyday life, and help with organizing care. 48 As mentioned earlier a, recent study on caregivers’ expectations on disease-modifying treatments has shown that both parents and patients report that even small changes in function are noticed as important. 40 The increased expectations from parents and patients have changed remarkedly after treatment has become available, 40 and professional counseling to the parents and patients’ should support this perception of hope. Information and counseling to families living with SMA should target these issues and be balanced to meet the individual families’ needs for information and support. This can be done by applying systematic screenings based on a list of relevant items for unmet needs and by assessing the impact of SMA on the patients’ everyday lives.49,50
Methodological considerations
We invited all families with a child with SMA < 14 years of age registered with RCFM to participate in the study. Our sampling represented 35% of this population of which 58% were mothers and 42% fathers, a distribution considered to represent the population well. The families included Danish families and families of other nationalities, from both rural and urban areas, and with children of various ages and stages of the disease, ensuring participant diversity and representative credibility. However, it can be considered a limitation in the study that we do not know if those who chose to participate are the ones who in specific have difficulties in handling hope and grief associated with having a child with SMA who is being treated with disease modifying therapy. This might have been investigated further by member checking which we did not perform. Finally, it might be considered a study limitation that we have not performed any measurements on the children to assess their function before and after starting medical treatment, but we are investigating this in another study.
The mixed composition of the author group consisting of researchers and health professionals with different backgrounds ensured researcher triangulation. Further the various author perspectives offered a critical assessment of relationships between data, as well as their relevance to the research question, and reduced possible assumptions and/or presuppositions. We ensured analytical logic by using the interpretive description four-step analysis, and we were three researchers working together during the analysis and interpretation, ensuring various perspectives and minimizing potential preconceptions in our coding or theme development. The first author, who is an experienced interviewer conducted all the interviews in the participants’ own homes (except for two which were conducted online by choice of the participants). Being in the safety of their own homes seemed to make the participants calm and relaxed and there did not seem to be any potential concerns related to their honesty and openness during the interviews. The parents found themselves between being relieved they had received disease modifying therapies for their children and not knowing what to expect in the long run. The disease modifying therapies are new and health professionals and researchers still do not know the long-term effects, meaning that the parents and children must live with uncertainty, unsure of what to hope for, expect, and deal with.
Based on our sample and participant representation, our consistency in questions using an interview guide, our analytical transparency by using a table to visualize the analysis process, we assess that our findings are of high internal validity and that our findings are transferable to other similar contexts and countries.
Conclusion and recommendations
This Danish study shows how parents of children with SMA receiving disease modifying therapies cope with hopes and worries in relation to disease progression. A key element in the parents’ narratives was the reality of the diagnosis – the trajectory toward the diagnosis, getting the diagnosis, and the hope related to the disease modifying therapies, but at the same time grief related to the uncertainty of the future and disease progression. Hoping for normalcy – a ‘normal’ child and a ‘normal’ life – and management of everyday life, maintaining relations, and the need for support – were also an essential part of the parents’ stories. It is important that health professionals understand and support the parents in their grief and uncertainty by focusing on hope for the child and the treatment and on how to handle the new reality. The parents need multidisciplinary care and care coordination, information on the disease modifying therapies, support in their treatment choices, and counseling on what they can actively do to assist the disease modifying therapy. The support and counseling of the parents must encompass facilitated peer-support and acknowledge the differences in children, their development, and their responses to the disease modifying therapies as well as the long-term effect of the treatments. The health professionals must be cautious of how they talk about normalcy in their practices when communicating and counseling patients and make sure to endorse hope for the families by emphasizing that every person and every family will be like everyone else, like someone else, and like no one else. Health professionals should not overwhelm the families by giving unsolicited information about the diagnosis or disease progression but instead support the families in maintaining hope for the future. Professional information and counseling should focus on support with everyday life and organizing care. The counseling must be balanced to meet the individual families’ needs for information and support. To prevent caregiver burnout among the parents, professionals should systematically screen for unmet needs using a check list of relevant items. Future research should focus on physical and mental burnout among parents of children with SMA.
Footnotes
Abbreviations
Acknowledgements
We would like to thank all the families who participated in this study and shared their stories, making this study possible.
ORCID iDs
Ethics approval and consent to participate
This study was approved by The Central Region Committees on Health Research Ethics [request no. 202/2023 Jr.no. 1-10-72-109-23]. According to the Consolidation Act on Research Ethics Review of Health Research Projects, Consolidation Act number 1338 of 1 September 2020, section 14 2 notification of interview surveys to the research ethics committee system is only required if the project involves human biological material. The study was performed in accordance with the Declaration of Helsinki. 51 All participants were informed about the study in writing and verbally. Written consent was obtained from all participants. The participants were informed that their consent could be withdrawn anytime and that their data would be anonymized.
Consent for publication
Informed consent for publication was obtained from the participating families.
Author's contributions
Charlotte Handberg conceptualization and design (equal); methodology; formal analysis (lead), writing the original draft (lead); review and editing (lead).
Pia Zinck Drivsholm formal analysis (supporting), review and editing (supporting).
Ulla Werlauff conceptualization and design (equal), review and editing (supporting).
Sanne Okkels Birk Lorenzen review and editing (supporting).
Annette Mahoney conceptualization and design (equal); formal analysis and editing (supporting), writing the introduction draft (supporting); review and editing (supporting).
Funding
The patient organization the Danish Muscular Dystrophy organization.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.