
Abstract
Introduction
Myasthenia gravis (MG) is a rare, debilitating autoimmune disease associated with pathogenic immunoglobulin G autoantibodies directed against components of the neuromuscular junction. The autoimmune nature of the disease and long-term immunosuppressive treatment may increase susceptibility to infections and malignancies, but studies investigating the association between MG and infections or malignancies remain scarce.
Methods
We conducted a retrospective, observational study using Optum's deidentified Market Clarity Data (Market Clarity) to evaluate the incidence rate (IR) of infections and malignancies in US-based patients with MG in a real-world setting. Adults with ≥2 diagnosis claims of MG were identified over a 2-year period (2016–2019) and propensity score (PS) matched with controls from the general population without MG. Patients with malignancies in the 1-year look-back period were excluded.
Results
Patients with MG (N = 5002) were compared with the PS-matched general population (N = 20,008). The IR of serious infections (primary outcome) was higher in the MG cohort compared with the general population (52.81 vs 31.46 per 1000 person-years [PY], respectively). IRs of opportunistic infections (87.48 vs 57.01 per 1000 PY) and infection-related death (3.98 vs 1.94 per 1000 PY) were also higher in the MG cohort compared with the general population. The overall rate of malignancy was higher in the MG cohort compared with the general population (73.55 vs 50.01 per 1000 PY, respectively).
Conclusions
In this analysis, patients with MG were more susceptible to serious infections, infection-related death, and malignancies.
Introduction
Myasthenia gravis (MG) is a rare, chronic, and debilitating autoimmune neuromuscular disease associated with pathogenic immunoglobulin G (IgG) autoantibodies directed against components of the neuromuscular junction.1–3 The US prevalence of MG is estimated to be 320.2 cases per million people, with >80,000 individuals currently living with MG. 4 Typically, patients with MG initially experience ocular symptoms, and most progress to generalized MG, which can involve bulbar, axial, limb, and respiratory muscle weakness.2,5
MG may predispose patients to infections due to several aspects relating to the clinical course of disease, underlying autoimmune mechanisms, and management. Bulbar and respiratory muscle weakness among patients with MG may increase the likelihood of aspiration and respiratory infections, 5–8 with pneumonia being the most common infection and etiology of all-cause mortality.5,9,10 Approximately 15% to 20% of patients with MG experience myasthenic crisis during their lifetime, resulting in respiratory failure that requires hospitalization with intubation and mechanical ventilation, thus compounding the risk of respiratory infections.11,12 Conversely, infection has been proposed as an external factor that may trigger or worsen MG.13,14 The use of immunosuppressive treatment also increases the risk of infections in patients with MG, although the estimated magnitude of increased risk resulting from immunosuppressive treatment varies in the literature.9,15
Evidence suggests that the autoimmune nature of the disease and prolonged use of certain immunosuppressive treatments may also predispose patients with MG to malignancies.16,17 There is a well-known association between malignancies of the thymus and MG, with 10% to 15% of patients with MG developing thymomas; however, data on the link between MG and extrathymic malignancies are less clear.7,18–20 An increased risk of extrathymic cancers, including lymphoid and digestive tract malignancies, has been observed in MG, with greater frequency in older patients, patients with thymoma-associated MG, patients experiencing greater disease severity, and patients receiving intravenous IgG (IVIg) treatment.16,20–22 While a separate nationwide case-control study did not observe a significantly elevated risk of extrathymic cancers within a general MG cohort, 19 another study in a similar patient population with MG reported an increased risk of nonmelanoma skin cancer compared with matched controls. 23 Similarly, disparate results have been observed regarding the association between therapies used in the management of MG and risk of malignancies. A recent systematic review and meta-analysis found no significantly increased risk of secondary malignancy with azathioprine use, 24 while other studies observed increased incidence of extrathymic malignancies with increased exposure to nonsteroidal immunosuppressive therapies (NSISTs), including azathioprine.23,25
To date, the studies that have investigated the relationship between MG and infections or malignancies have used varying methodologies to identify patients with MG, may not have included matched controls, and have been mostly based outside of the US.10,11,20–22,26 There is evidence of increased infection risk in other autoimmune conditions, but data regarding real-world experience in patients with MG compared with a matched non-MG population are limited.15,27 Another critical barrier to examining the risks of infrequent adverse events, such as serious infection or malignancies, is the lack of sufficiently large sample sizes, particularly in the setting of rare diseases. 28 Real-world data may provide insightful information on patients’ health status, the natural disease course, or standard of care. 29 Therefore, we conducted a retrospective observational study using claims data to evaluate the risk of infection and malignancy in a large, US-based population of patients with MG in a real-world setting to generate evidence to provide context and a point of comparison for future research.
Methods
Data source
Anonymized claims data used to conduct this study were from Optum's deidentified Market Clarity Data, which deterministically link medical and pharmacy claims with electronic health record data from providers across the continuum of care. 30 This dataset provided information on diagnoses and medications. 30 The data were statistically deidentified under the Health Insurance Portability and Accountability Act of 1996 Privacy Rule's Expert Determination method and managed according to Optum® customer data use agreements. 31 The full data availability period was from January 1, 2015, to December 31, 2019.
Study design
This was a retrospective claims study of patients with MG. Non-MG controls were identified from a 5% random sample of the general population. A propensity score (PS) analysis with a 1:4 match was conducted to increase robustness of the study, comparing outcomes between the MG and non-MG groups.
Study period
The study period was January 1, 2016, through December 31, 2019—before the COVID-19 pandemic, thereby avoiding any bias of the pandemic on the incidence of serious infections, which could have been influenced by changes in health care access, infection control measures, and patient behavior during the pandemic. Patients were identified for study inclusion during a 2-year window between January 1, 2016, and December 31, 2017 (ie, the “identification period”). Although patients were required to have at least 2 claims with diagnostic codes for MG, the date of the first diagnosis code was considered the index date, whereby subsequent outcomes were then assessed (Supplementary Figure 1). In addition, a 1-year period before index was used to assess baseline characteristics and inclusion/exclusion criteria (ie, the “look-back period”).
Study population and baseline characteristics
Adult patients (aged ≥18 at index date) with MG were identified based on at least 2 office visits with a diagnosis code of MG (International Classification of Diseases [ICD] codes 358.0, 358.00, or 358.01 [ninth revision; ICD-9] or G70.0, G70.00, or G70.01 [tenth revision; ICD-10]) separated by at least 4 weeks or 1 hospital discharge and 1 office visit, each using MG diagnosis codes separated by at least 4 weeks; this process of identifying patients with MG in the real-world setting has been previously described. 32 Patients were further required to meet continuous insurance enrollment during the look-back and assessment periods, with no coverage gap lasting >30 days. The control cohort was identified from a 5% random sample of the general population in Market Clarity. Patients from this sample were PS matched 1:4 with patients with MG to yield the control cohort. Patients from both MG and comparator cohorts were excluded if they had ≥1 claim related to malignancy in the look-back period. This would eliminate patients with MG with thymoma in the look-back period but not eliminate patients with thymoma/thymectomy prior to the look-back period.
The following baseline characteristics were compared between patients with MG and the non-MG general population cohort and were used in propensity score matching (PSM): age at index (continuous), sex at index (male or female), Charlson Comorbidity Index (CCI) calculated based on comorbidities discovered in the 12-month period before index (continuous), 33 geography at index (Northeast, Midwest, South, or West), insurance status at index (commercial, Medicare, Medicaid, or multiple), the calendar year of index, presence of select autoimmune condition (yes/no), and presence of obesity (yes/no) in the 12 months before index. Prevalence of non-MG hospitalizations (continuous) was also measured and considered an adjustable variable for PSM.
Study outcomes
The outcomes of interest in this study included infections, malignancies, and outcome-related deaths.
Primary outcome
The primary outcome for this study was incidence rate (IR) of serious infection. Serious infections included all types of infections that (1) required either hospitalization or an emergency department (ED) visit with an admitting (primary) diagnosis of infection or (2) resulted in death.
Secondary outcomes
Secondary outcomes included IRs of infections by organ system (eg, respiratory, urinary) and those associated with opportunistic pathogens. Opportunistic infections were selected based on Standardized Medical Dictionary for Regulatory Activities (MedDRA) Queries but were found to have limited overlap with ICD codes. Therefore, opportunistic infections were grouped by pathogen and the literature was evaluated to ensure inclusion of pathogens that are relevant in autoimmune disease. 34 Opportunistic infections were then mapped to ICD-10 codes using the name of the pathogen (Supplementary Table 1).
Malignancies were assessed and grouped according to the ICD-10 classification system by location. Malignancies were classified as solid tumors or malignant lymphoid, hematopoietic, and related tissue neoplasms, and additionally as thymic or extrathymic.
Lastly, outcome-related death was attributed to an event if the event occurred in the same month and year or 2 weeks before the month and year of death, consistent with approaches taken in other claims data analyses. If the visit was a hospitalization or ED visit, death was automatically considered to be related to the event of interest.
Statistical analysis
Continuous baseline variables were reported as mean (SD) or median (IQR). Categorical baseline variables were reported as frequencies and percentages. Outcomes were reported as IRs (in person-years), which were defined as the number of outcome-related events (eg, infections, malignancies) during the assessment period divided by the total person-time of observation during the study. Incidence rate ratios (IRRs) and 95% CIs were also reported for all outcomes and were adjusted and corrected for zero cells using the Haldane-Anscombe correction factor. 35
PSM of patients with and without MG was done using a 2-step approach. The first step was a 1:1 match (age, sex, geographic region) to assign an index date to patients without MG and define the baseline period for quantifying baseline characteristics (including hospitalizations and comorbidities). These initially matched patients without MG were then assigned the same index date as that of their matched counterpart with MG. The index date assignment for patients without MG was undertaken to provide the same baseline and follow-up time periods for the comparison of outcomes between patients with and without MG.
The second step of PSM was applied to control for the differences in all baseline clinical and demographic characteristics between patients with and without MG. Patients were matched on the logit of the PS at a 1:4 ratio, using the greedy nearest neighbor with a caliper distance of 0.2 times the SD of the logit of the PS. The balance of variables between patients with and without MG was assessed both before and after matching using the standardized mean difference (SMD), with a value of <0.1 denoting acceptable balance. 36
Missing data were present for certain categorical variables, such as insurance status and geographical region. In these instances, the missing-indicator method 37 was used to address the issue of missing data, and a value of “unknown” was assigned to data that were missing. The proportion of patients who were assigned that value is presented in Table 1.
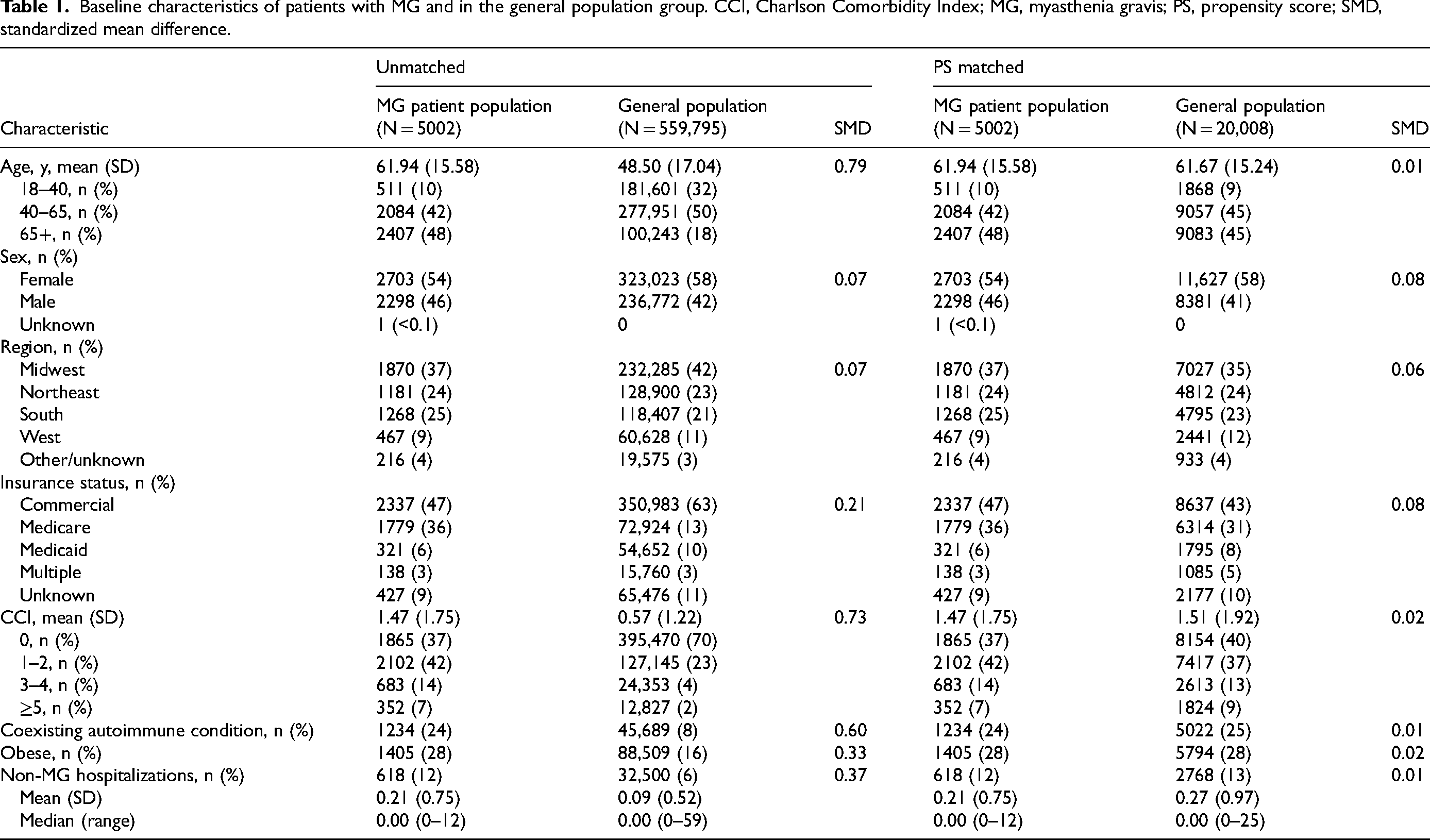
Baseline characteristics of patients with MG and in the general population group. CCI, Charlson Comorbidity Index; MG, myasthenia gravis; PS, propensity score; SMD, standardized mean difference.
Stratified analyses
To explore the effect of background immunosuppressive treatment on outcomes, unadjusted stratified analyses were performed in the population of patients with MG based on whether they had been prescribed immunosuppressive treatment (≥1 claim) during the look-back period. Immunosuppressive treatments included corticosteroids, NSISTs (azathioprine, cyclophosphamide, cyclosporine, methotrexate, mycophenolate/mycophenolate mofetil, and tacrolimus), rituximab, and eculizumab. For exploratory analyses on malignancies, immunosuppressive treatment was further divided into corticosteroids and NSISTs.
Results
Population characteristics
A total of 36,195 patients were identified as having MG during the 2-year identification period, of whom 5002 met all inclusion and exclusion criteria (Figure 1); 20,008 patients from the non-MG general population were PS matched as described above. Prior to PSM, patients with MG had a higher average age (61.94 years) and CCI (1.47) compared with the non-MG general population (48.50 years and 0.57, respectively). The cohort with MG had a lower proportion of patients with commercial insurance coverage and greater proportions of patients who were on Medicare, who had another autoimmune condition, and who were considered obese; the proportion of patients with non-MG hospitalizations during the look-back period and the mean number of hospitalizations were also higher in the MG cohort. After matching, patients with MG were similar in age and CCI compared with the non-MG general population (61.67 years and 1.51, respectively), and all baseline SMDs were <0.1 (Table 1). PS density graphs further confirmed a satisfactory match between cohorts, as overlap between the densities appeared to be adequate (Supplementary Figure 2).
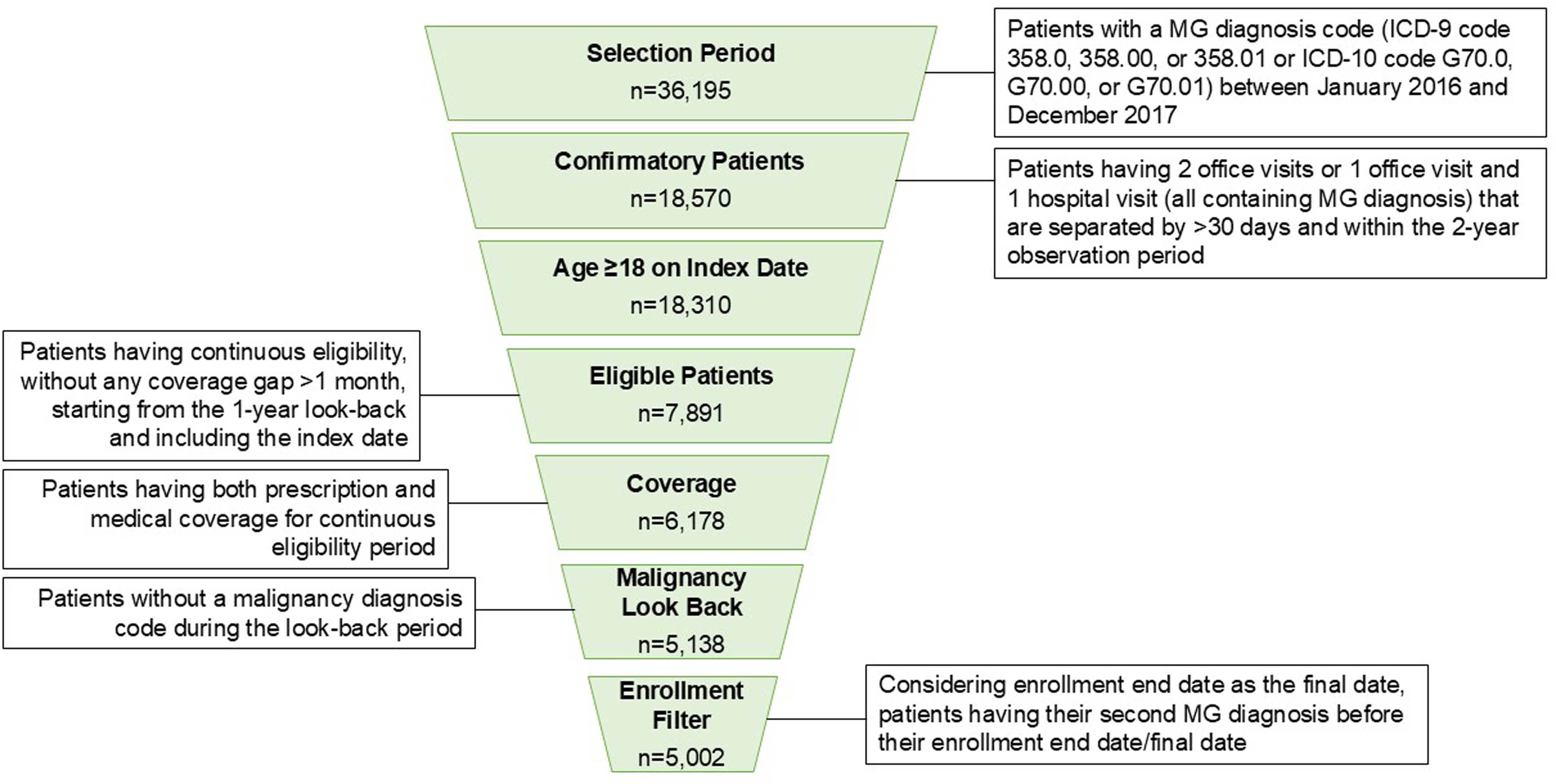
Selection criteria for patients with MG. MG, myasthenia gravis.
Infections
Serious infections
Compared with the PS-matched general population, patients with MG experienced more serious infections, including pneumonia, bronchitis, influenza, sepsis, skin infections, urinary tract infections, and serious herpetic infections, in addition to gastrointestinal (GI) infections, serious fungal infections, and viral infections (unspecified site) (Figure 2). Patients with MG also had higher rates of infection-related death compared with the general population (IRR, 1.93; 95% CI, 1.28–2.90). In general, the absolute rates for most serious infections were higher in patients with MG compared with the general population (Supplementary Table 2). The rate of serious upper respiratory tract infections was not notably different in patients with MG compared with the general population.
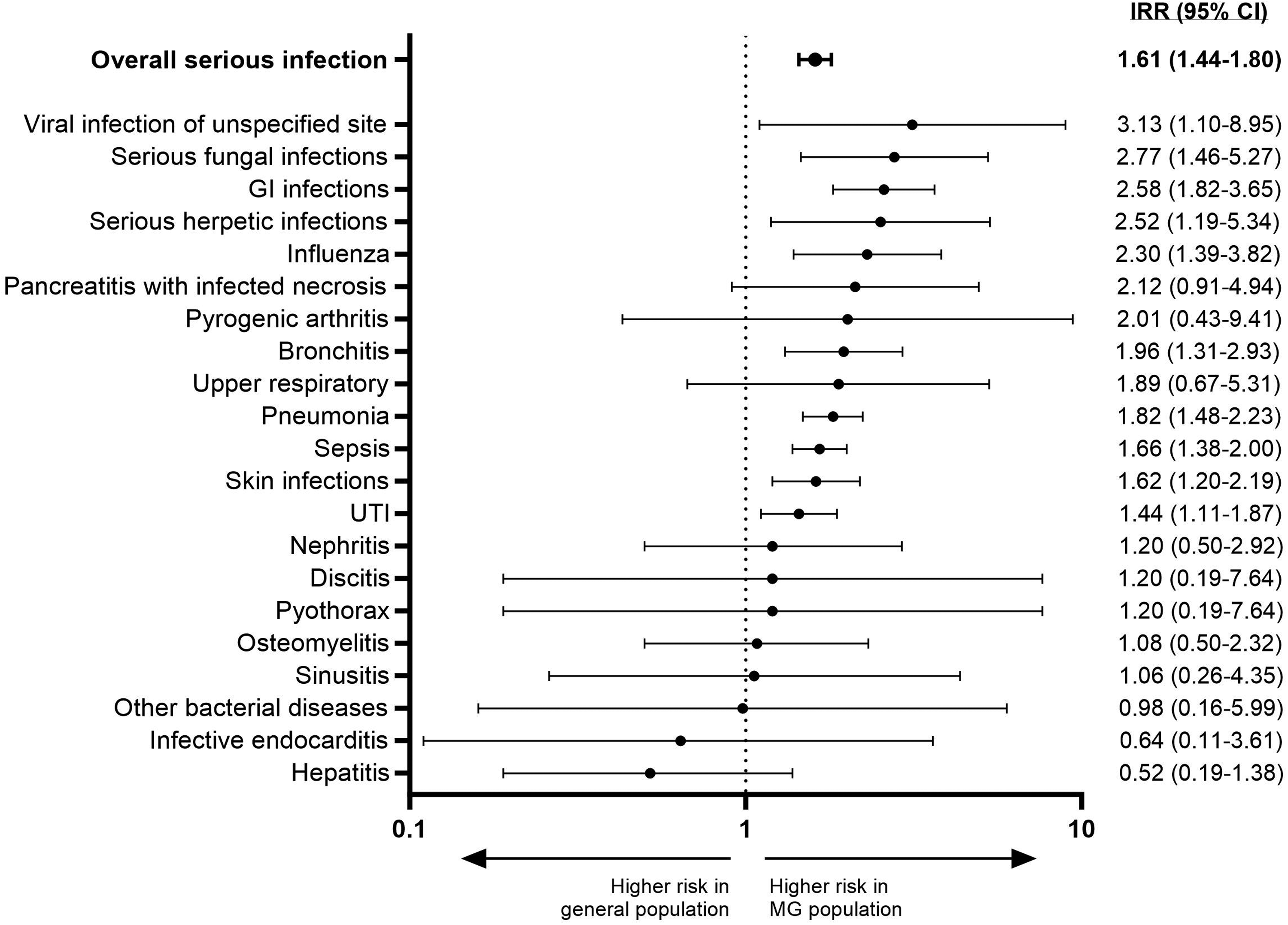
Serious infections in the MG patient population and the general population. Serious infections with an event count >3 in either group are shown. GI, gastrointestinal; IRR, incidence rate ratio; MG, myasthenia gravis; UTI, urinary tract infection.
Opportunistic pathogens and overall infections by organ
Compared with the general population, patients with MG were more prone to infections associated with opportunistic pathogens, including those due to Pneumocystis jirovecii, Cryptococcus, Klebsiella, Pseudomonas (including Burkholderia and Stenotrophomonas species), Candida, and herpes viruses (herpes simplex, herpes zoster, and varicella) (Figure 3). Similar to serious infections, the absolute IRs for most opportunistic infections were higher in patients with MG compared with the general population (Supplementary Table 3). Other infections associated with opportunistic pathogens, including reactivation of tuberculosis or hepatitis B, did not occur at higher rates in patients with MG compared with the general population. For overall infections, patients with MG experienced more systemic infections and infections occurring in the central nervous system (CNS), upper and lower respiratory tracts, GI system (including liver and gallbladder), and urinary tract (including kidney) compared with the general population (Supplementary Figure 3). Overall, the absolute IRs for infections in most organ systems were higher in patients with MG compared with the general population (Supplementary Table 4).
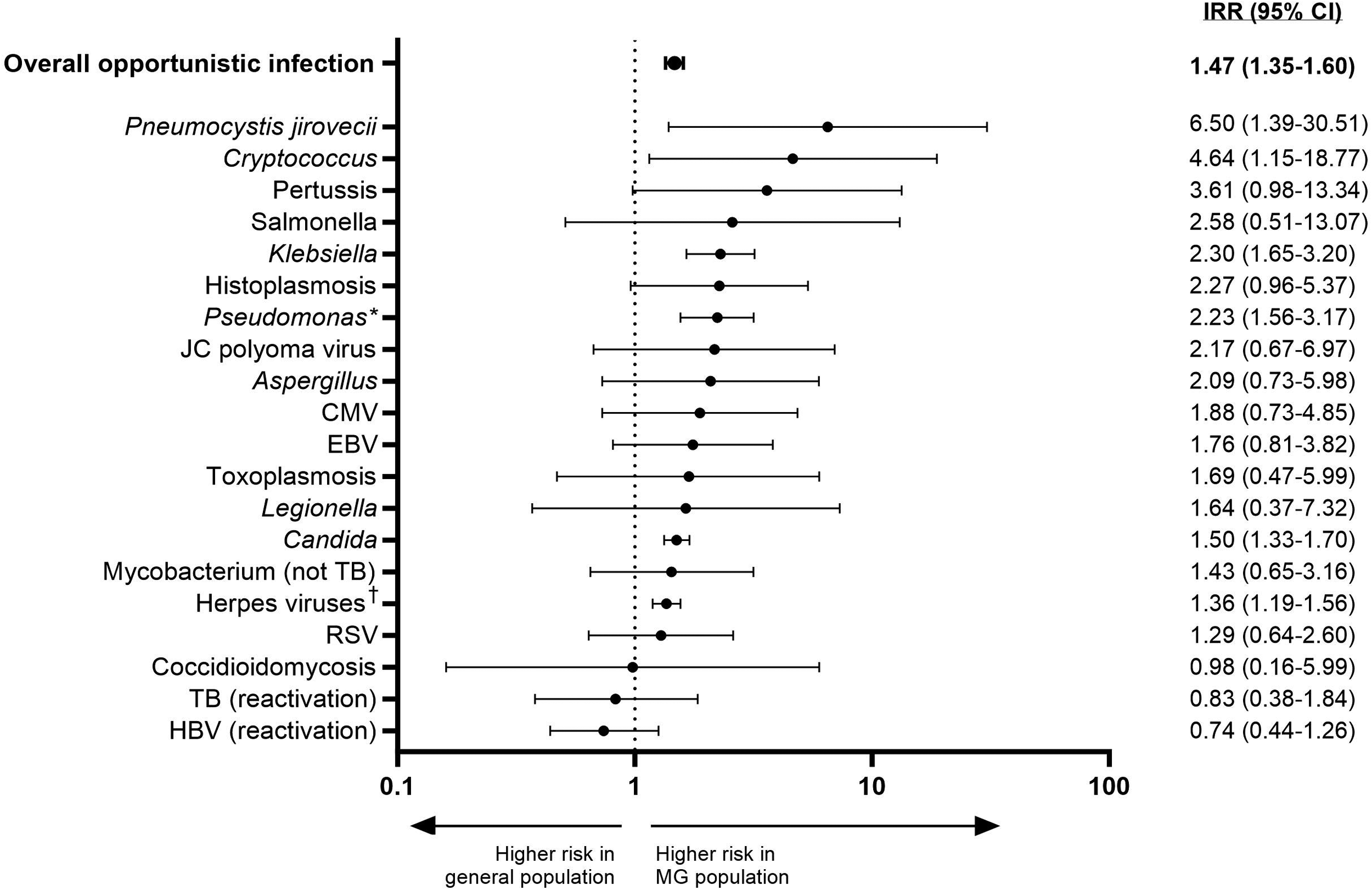
Infections associated with opportunistic pathogens in the MG patient population and the general population. Opportunistic infections with an event count >3 in either group are shown. *Including Burkholderia and Strenotrophomonas. †Including herpes simplex, herpes zoster, and varicella. CMV, cytomegalovirus; EBV, Epstein-Barr virus; HBV, hepatitis B virus; IRR, incidence rate ratio; JC, John Cunningham; MG, myasthenia gravis; RSV, respiratory syncytial virus; TB, tuberculosis.
Malignancies
In the general population, no thymic malignancies were observed. In the MG population, the IR of thymic malignancies was 5.9 per 1000 person-years (95% CI, 4.31–7.49). If all malignancies were combined, patients with MG were more likely to develop extrathymic malignancies, solid malignancies, and overall malignancies compared with the general population (Figure 4). Higher rates were observed in patients with MG compared with the general population for Hodgkin lymphoma, malignancies of the CNS (including malignancies of the eye and brain), malignancies of male genital organs, and melanoma (or other malignancies related to skin). The rates of malignancy-related death did not differ between patients with MG and the general population (IRR, 1.73; 95% CI, 0.67–5.31). The absolute IRs for malignancies were generally higher in patients with MG than in the general population (Supplementary Table 5).
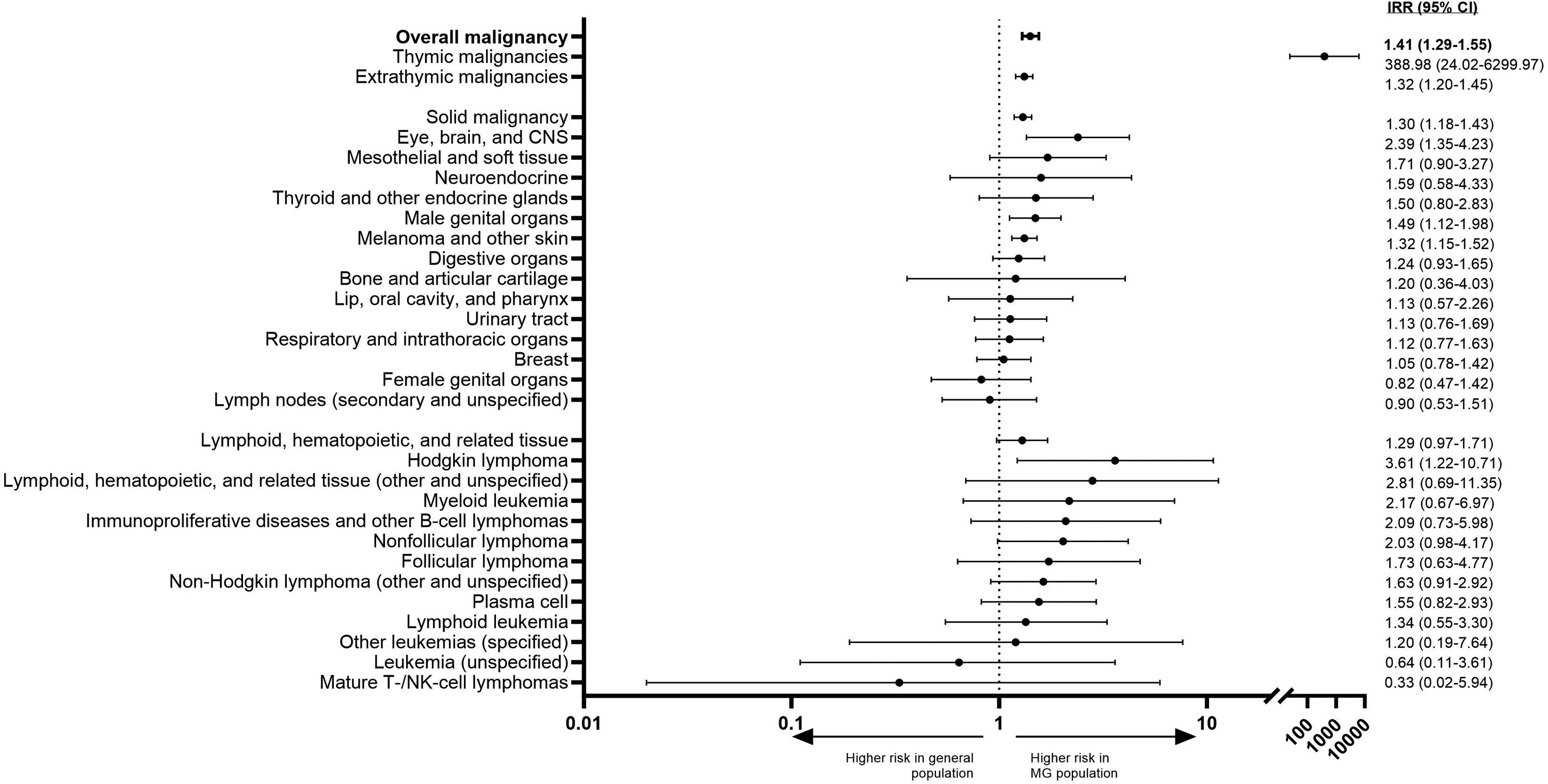
Malignancies in the MG patient population and the general population. Malignancies with an event count >3 in either group are shown. Malignant neoplasms of ill-defined, other secondary, and unspecified sites are not reported. CNS, central nervous system; IRR, incidence rate ratio; MG, myasthenia gravis; NK, natural killer.
Stratified analyses
Among patients with MG, 2204 received immunosuppressants during the 1-year look-back period, and 2798 did not. Those with immunosuppressant use during the look-back period were, on average, younger and more medically complex, with a greater percentage having another autoimmune condition and a history of non-MG hospitalizations compared with those who did not receive immunosuppressants (Supplementary Table 6).
In unadjusted analyses, patients with MG and a history of immunosuppressant use had increased rates of overall serious and opportunistic infections compared with patients with MG who did not use immunosuppressive treatment in the look-back period (Supplementary Figure 4; Supplementary Figure 5a). Although no matching or statistical comparisons were performed, patients with MG without immunosuppressant use in the look-back period still had numerically higher IRs of many serious infections compared with the general population (Supplementary Table 7). However, the IRs of infection-related death did not differ between the two groups (Supplementary Table 8).
Additionally, patients with MG who had a history of immunosuppressant use during the look-back period had increased rates of systemic infections and infections (Supplementary Figure 5b). Although no matching was performed and statistical comparison was not possible, the absolute IRs for opportunistic and organ-specific infections were generally higher in patients with MG who had a history of immunosuppressant use compared with patients with MG who did not (Supplementary Table 8; Supplementary Table 9).
Patients with MG who had a history of immunosuppressant use during the look-back period had increased rates of mesothelial malignancies and non-Hodgkin lymphoma compared with patients with MG who did not use immunosuppressive treatment (Supplementary Figure 6). However, malignancy-related deaths did not differ between patients with MG based on use of immunosuppressants during the look-back period (IRR, 0.89; 95% CI, 0.18–4.52). Since the risk of developing malignancies may differ for corticosteroids and NSISTs, exploratory analyses of malignancies by the type of immunosuppressive treatment were also performed (Supplementary Table 10). IRs for malignancies were evaluated in cohorts of patients with a history of corticosteroid use only (n = 1434), NSIST use only (n = 310), both corticosteroid and NSIST use (n = 460), and no immunosuppressant use (n = 2798); however, no statistical comparison between groups was performed.
Discussion
In this study, we used the Market Clarity Data to provide a comprehensive assessment of the infection and malignancy risk in a large US-based population of 5002 patients with MG compared with the general population. PSM resulted in a comparator cohort that was well matched with the MG cohort for relevant demographic and clinical baseline characteristics, allowing for comparison of outcomes between patients with MG and the general population while minimizing selection bias. Additionally, we further stratified patients with MG by immunosuppressant use to better understand the risk of malignancy by the type of immunosuppression used. To our knowledge, this is the first study that holistically assessed infection and malignancy risk in patients with MG. These data fill an important gap in understanding the background risk of infection and malignancy in patients with MG.
We found that overall risk of serious infections was higher in patients with MG compared with the matched general population. These findings are consistent with those of a prior Canadian study, in which the IR of serious infections was 2 times greater in patients with MG vs PS-matched controls (72.5 vs 35.0 per 1000 person-years, respectively), with respiratory infections, bacterial pneumonia, and sepsis being among the most frequent serious infection types in that study as well. 5 Our study also confirmed the previous finding that immunosuppressive therapies are frequently used to treat MG but are also known to increase susceptibility to infections.7,9,27 While no formal statistical comparison was performed, rates of many serious infections were numerically higher in those with MG who did not receive immunosuppressants during the look-back period compared with the general population. This finding suggests that other factors inherent to MG may contribute to increased infection risk in addition to the use of immunosuppressive therapies. 5
We also observed that patients with MG had a higher risk of infections associated with opportunistic pathogens compared with the general population. Literature on the incidence or prevalence of opportunistic infections in patients with MG is scarce, potentially owing to a lack of standardized definitions (eg, infections frequently seen in people with weakened immune systems) and the limitations related to ICD and MedDRA matching, despite efforts to standardize mapping.9,34,38,39 For example, prior data on Candida infection in patients with MG are available but limited exclusively to case reports.40–42 Additionally, prior literature on the incidence of herpes virus infections in patients with MG is limited and anecdotal, underscoring the importance of our finding that herpes viruses were common in this population and also highlighting the medical need for vaccination in these patients.42–46 In contrast, varicella zoster has been among the most common identifiable pathogens underlying infections in prior studies of patients with MG, and infection occurred at a higher frequency in those with MG vs a PS-matched control cohort in the aforementioned real-world Canadian study.5,9
The overall risk of malignancy was higher in patients with MG compared with the general US population in our study, which is consistent with a prior study conducted in Taiwan that showed patients with MG had an increased risk of extrathymic malignancies. 18 Additionally, in our study, there was an increased IR of melanoma and other neoplasms of the skin in patients with MG compared with the general population, with patients with MG who had a history of NSIST use having the highest IR. Findings on malignancy risk in patients with MG are not always consistent, which could be attributed to methodological differences, such as the length of the observational period or geographic location.18,47 Other differences could be attributed to variations in the underlying patient population, such as age, incidence of concurrent autoimmunity,18,19 or the extent of exposure to immunosuppressants. 25 Patients with a history of either NSIST or corticosteroid use had higher rates of mesothelial and soft tissue malignancies than patients with no history of immunosuppressant use, and this rate appeared cumulative in patients with a history of both NSIST and corticosteroid use; however, given the rarity of these events, further confirmation of this finding is warranted.
While claims-based studies offer the advantage of large and diverse study populations, they also present methodological issues that should be considered. One such aspect of US-based claims dataset studies is that the look-back period is usually limited. The look-back period in this study constituted 1 year of observation, which is typical for US studies. Although it is generally accepted that complete remission can occur after 5 years without relapse, a look-back period of that length would not be feasible in a US claims database study and would hinder sample size, limiting the ability to detect rare events. Thus, a limited observational period may not capture the long-term effects of MG or immunosuppressive therapy. Lastly, the approach for attributing death to an event could have resulted in misattributions, since an event occurring in the same month as death may not necessarily substantiate that the event was the cause of death.
The findings from this study rely on the assumption that the exposure precedes the outcome, but there is the possibility that malignancies captured in this study occurred before the diagnosis of MG. Additionally, immunosuppressant use was not adjusted for, so patients could have received immunosuppressive therapy for conditions other than MG, which may have resulted in an overestimation of the effect of MG on study outcomes. Therefore, we tried to control for autoimmune disorders, many of which require the use of immunosuppressants, and conducted exploratory stratification analyses showing that patients with MG who had a history of immunosuppressant use had higher rates of infections and malignancies compared with patients with MG who did not have a history of immunosuppressant use.
In conclusion, this observational, retrospective claims database analysis provides a comprehensive summary of the risks of infection and malignancy in real-world patients with MG in the US. Despite the study's limitations, these data provide important insights with implications for long-term management of these patients. Due to the risk of infections, including those caused by opportunistic pathogens, it is important for patients to adhere to recommended country-specific guidelines for vaccinations in adults. Considering the safety risks associated with both underlying disease and established immunosuppressive therapies, these results suggest a need to incorporate newer therapies into evolving management paradigms for patients with MG.
Supplemental Material
sj-docx-1-jnd-10.1177_22143602251403092 - Supplemental material for Analysis of infections and malignancy risks among patients with myasthenia gravis compared with matched controls in a US real-world setting
Supplemental material, sj-docx-1-jnd-10.1177_22143602251403092 for Analysis of infections and malignancy risks among patients with myasthenia gravis compared with matched controls in a US real-world setting by Jana Podhorna, Charlotte Ward, Kushal B. Naik, Ikjae Lee, Yuebing Li, Tobias Ruck, Elizabeth Teperov and Jeffrey T. Guptill in Journal of Neuromuscular Diseases
Footnotes
Acknowledgments
Medical writing and editorial support were provided by Sydney Eck, PharmD, and Jason Dunkelberger, PhD (Precision AQ), and funded by argenx. All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Jana Podhorna, Elizabeth Teperov, Charlotte Ward, and Kushal B. Naik. Initial manuscript development was performed by Jana Podhorna and Charlotte Ward, and all authors commented on previous versions of the manuscript. All authors were involved in interpretation of findings. Ikjae Lee, Yuebing Li, Tobias Ruck, and Jeffrey T. Guptill evaluated clinical relevance of the findings. All authors read and approved the final manuscript. Portions of the content within this manuscript were presented at American Academy of Neurology Annual Meeting on April 13–18, 2024, in Denver, Colorado, and Myasthenia Gravis Foundation of America Scientific Session at the American Association of Neuromuscular & Electrodiagnostic Medicine Meeting on October 15–18, 2024, in Savannah, Georgia.
Ethics approval
The study protocol was submitted for institutional review board approval, but because the patient data were deidentified, the board determined that the study was exempt from review, and patient consent was not required.
Funding
This study was sponsored and funded by argenx.
Conflicts of interest
JP, ET, and JTG are employees of argenx. CW and KBN are consultants with ZS Associates. IL has received research funding from the National Institutes of Health, Myasthenia Gravis Foundation of America, American Academy of Neurology, CReATe consortium, and American Brain Foundation and received consulting fees/honoraria from Amylyx, Alexion, Regeneron, Roche/Genentech, MedLink, and Medscape. None of the funders influenced the study design or analysis.
YL has received research support from argenx and served as a consultant for argenx, UCB Pharma, Alexion, Catalyst, and Immunovant.
TR has received honoraria for speaking and advice and travel support from argenx, Alexion, Celgene/BMS, Biogen, Johnson & Johnson, UCB, Roche, Sanofi Genzyme, Merck, Novartis, and Teva and research funding from Alexion, argenx, Biogen, Novartis, Merck, Roche, Sanofi Genzyme, and SERB Pharmaceuticals.
Data availability statement
The data analyzed in this study was obtained from Optum and the availability of these data are subject to restrictions. Data presented in the current study were used under license and are not publicly available. argenx is committed to responsible data sharing and data are available from the authors upon reasonable request and with permission from Optum.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.