
Abstract
Background:
Health plan policies managing neuromuscular disease (NMD) therapies may impose burdensome requirements on patients and providers. While prior research has explored payer restrictions for rare NMD treatments, limited evidence exists on policies specifically governing therapy initiation and reauthorization.
Objectives:
To examine initial and reauthorization coverage policies for therapies targeting five NMDs—Duchenne muscular dystrophy, amyotrophic lateral sclerosis, spinal muscular atrophy, generalized myasthenia gravis, and Lambert-Eaton myasthenic syndrome—across all U.S. state Medicaid programs and leading commercial health plans.
Methods:
We constructed a database of coverage decisions issued by 50 states and DC Medicaid programs and 35 major commercial insurers, including both fee-for-service and managed care organizations. We analyzed (1) policy availability and coverage frequency, (2) initial coverage requirements (e.g., subgroup restrictions, step therapy, prescriber type), (3) reauthorization criteria, and (4) approval durations.
Results:
Of 1204 potential decisions, 908 (75%) had publicly available policies. Of these, 558 (46%) included reauthorization criteria. Among covered therapies, 96% imposed restrictions beyond FDA label indications. Requirements varied by payer type, NMD, and therapy. Average approval durations were 6 months for initial coverage and 10 months for reauthorization.
Conclusions:
Many plans lacked publicly accessible policies, and most covered therapies were subject to restrictive requirements. These barriers—such as step therapy, narrow prescriber criteria, and short approval periods—may delay treatment and disrupt care continuity. Findings underscore the need for greater transparency and reform in prior authorization and pharmacy benefit design to support timely access to NMD therapies.
Introduction
Neuromuscular diseases (NMD) encompass a broad group of rare conditions, most with prevalence rates between 1 and 10 per 100,000 population, that typically involve progressive, irreversible, chronic muscle weakness, fatigue, and impaired motor function. 1 Recent advances in diagnostic technology and treatments targeting specific genetic disease pathways have led to earlier diagnoses and improved disease management. 2 The U.S. Food and Drug Administration (FDA) has approved NMD treatments via expedited review programs, which speed patient access to therapies that address unmet treatment needs for serious conditions. 3 Therapies indicated for NMDs can be complex to administer and costly. For example, onasemnogene abeparvovec-xioi, a gene therapy for spinal muscular atrophy, has a one-time cost of $2.1 million, 4 while edaravone for amyotrophic lateral sclerosis carries an annual cost of about $170,000. 5
Health insurance coverage determines patients’ access to NMD therapy. 6 Health plans may use utilization management tools such as prior authorization (i.e., requiring approval of a treatment before it will be covered) and step therapy protocols (i.e., requiring patients to first try lower cost treatments before accessing a drug) to steer members towards medically necessary and/or cost-effective treatments.7–9 However, these practices can impose patient and prescriber barriers and delays in care10–14 and risk the progression of patients’ condition while families navigate insurance coverage and approval. Patients with Duchenne muscular dystrophy (DMD) and their caregivers reported insurance coverage as one of the main factors affecting treatment adherence. 15 These practices can also introduce administrative burdens for patients and providers in the form of learning costs (e.g., searching for patient eligibility criteria), compliance costs (e.g., submitting medical record documentation for prior authorization), and cause psychological stress for patients and families who must navigate the authorization process.16–18 Marginalized communities, including people with disabilities, disproportionately bear these burdens. 17
While prior research documented frequent restrictions in commercial health plan coverage of DMD, amyotrophic lateral sclerosis (ALS), and spinal muscular atrophy (SMA) treatments, 19 important coverage features remain underexplored. Specifically, little is known about (i) the extent to which health plans make neuromuscular disease (NMD) coverage policies publicly available, and the criteria plans use for reauthorization—that is, requirements patients must meet to continue receiving treatment. Limited transparency in these areas can create barriers to understanding coverage determinations and add administrative complexity, potentially leading to treatment delays and disruptions for patients and providers.
To address these gaps, we examined initial and reauthorization coverage policies for therapies indicated for five NMDs – DMD, ALS, SMA, generalized Myasthenia Gravis (gMG), and Lambert-Eaton myasthenic syndrome (LEMS) – across all state Medicaid programs and the largest US commercial plans by covered lives. 20 Stratifying by payer type (commercial and Medicaid), and by drug and indication, we described (1) the proportion of plans with a publicly available coverage policy and the extent to which policies covered the therapy, (2) initial coverage requirements – including subgroup restrictions, step therapy restrictions, prescriber requirements, and the duration of initial approval, (3) reauthorization requirements, from relatively permissive (requiring only some sort of response) to most restrictive (requiring an improvement in the patients’ condition) and (4) the duration of reauthorization approval. Findings may inform policymaking and advocacy to reform coverage transparency and prior authorization/reauthorization processes.
Methods
Data source and sample
We created a novel dataset of publicly availably coverage policies for 14 branded NMD therapies: edaravone and sodium phenylbutyrate/taurursodiol for ALS; casimersen, deflazacort, eteplirsen, golordirsen, and viltolarsen for DMD; eculizumab, efgartigimod alfa, and ravulizumab-cwvz for gMG; amifampridine phosphate for LEMS; and nusinersen, risdiplam, and onasemnogene abeparvovec for SMA. Supplemental Table 6 includes further details on the included therapies.
For commercial health plans, our starting point was the Tufts Medical Center Specialty Drug Evidence and Coverage (SPEC) Database. SPEC includes specialty drug coverage policies, including any coverage restrictions, issued by 18 large US commercial health plans representing 70% of commercially insured lives in the US. 20 For this study, we added coverage policies issued by the next 17 largest US commercial health plans. We queried each plan's online coverage policy portal by first searching for the therapy's generic and brand name; we searched for the indication if previous searches produced no results. A second researcher repeated the search if no policy was found as a final confirmatory step. We defined publicly available policies as those accessible on a plan's website. If no policy was available online, we did not contact the plan to request coverage information. Supplemental Table 7 lists the 35 commercial plans included.
To obtain Medicaid fee-for-service coverage policies, we searched publicly available health plan sites for the 50 states and District of Columbia (DC) Medicaid programs in April-May of 2023 using the approach outlined above, i.e., searching each state and DC's Medicaid program's online policy portal. This search process is described in further detail in prior work. 21
Analysis
The unit of analysis was a health plan-drug-indication, e.g., one health plan's policy for edaravone for ALS. We conducted analyses assessing the following: (1) policy availability, (2) initial coverage requirements, and (3) reauthorization coverage requirements. Because the federal Medicaid Drug Rebate Program requires state Medicaid plans to cover all FDA-approved outpatient drugs from participating manufacturers, we did not compare the frequency of drug coverage exclusions across plan types. 22
Policy availability
Coverage policy availability was categorized into three mutually exclusive designations: (1) No policy (health plan did not issue a publicly available policy for the therapy, either because a health plan did not issue ANY publicly available coverage policies or because a health plan did not issue a coverage policy for the drug of interest); (2) Unclear/limited information available (the health plan issued some coverage information, but the information was insufficient to understand patient eligibility, e.g., the plan listed the drug in a formulary without accompanying information on patient eligibility criteria), or (3) Policy available (plan issued a policy document describing patient eligibility criteria).
Initial coverage requirements
For policies we designated as available, we classified policies as “covered” (therapy is available under a set of patient eligibility criteria, with or without restrictions), or “not covered” (therapy is excluded from coverage, e.g., because the plan deemed the treatment to be not medically necessary).
Among policies that covered the therapy, we reported how often plans imposed the following restrictions beyond the drugs’ FDA label indications: (1) Subgroup restrictions, i.e., whether the health plan restricted the eligible patient population based on the severity or progression of disease; (2) Step therapy restrictions, i.e., a requirement that patients received treatment with another therapy before accessing the drug; and (3) Prescriber requirements, i.e., a requirement that a certain type of physician or specialist prescribed the drug (or be consulted prior to prescription). We also reported the mean number of steps by type of payer and drug-indication pair and the standard deviations. We categorized prescriber requirements from least to most restrictive as: (1) Consultation with a specialist, (2) Prescription by a specialist, or (3) Prescription by a specialist with expertise. Lastly, we reported the availability of initial approval duration and approval duration in months.
Reauthorization coverage requirements
Plan reauthorization requirements were assessed in two ways: (1) the availability of requirements and (2) the treatment response requirements patients must satisfy to continue receiving the therapy We categorized treatment response requirements a priori, ranking them from least to most restrictive as follows: (1) A Non-specific treatment benefit, i.e., some sort of treatment response but no specific definition of what constitutes a response; (2) Slowed disease progression or decline to a minimum threshold, i.e., maintenance of function above an absolute or relative threshold, compared to expected disease progression; (3) Stabilization or maintenance, i.e., a cessation of disease progression; or (4) Improvement. If a coverage policy allowed for multiple treatment responses –e.g., improvement, stability or slowed decline—we used the least restrictive option (i.e., slowed disease progression or decline to a minimum threshold in this example). Lastly, we reported the availability and duration of reauthorization in months.
Results
Policy availability
Among the 1204 plan-drug-indication combinations, in 296 (25%) cases we did not find a publicly available coverage policy: 13% for commercial plans; 33% for Medicaid plans. In 187 cases (16%), unclear/limited information was available; 25% for Medicaid plans, 2% for commercial plans. Figure 1 and Supplemental Table 1 details combined policy availability and policy availability by plan type and drug/indication.
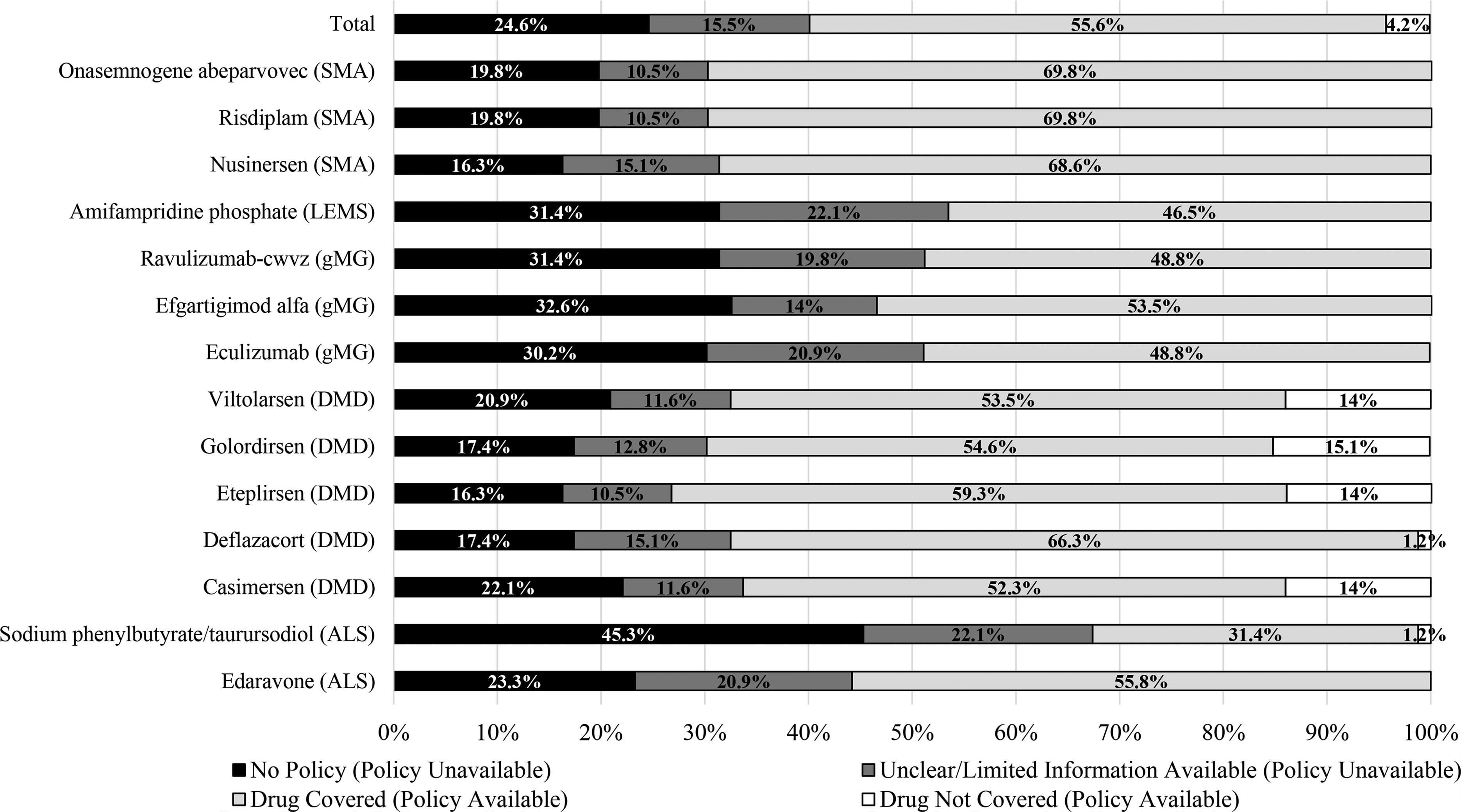
Overall policy availability (n = 1204 plan-drug-indication combinations).
Initial coverage requirements
Overall, among publicly available coverage policies, NMD therapies were excluded in 51 cases (4%) (Figure 1). All exclusions were from commercial health plans, which denied coverage in 51 instances (10%), whereas no state Medicaid FFS program excluded coverage (Supplemental Table 1 & Supplemental Table 2).
Among available policies that conferred some degree of coverage (n = 670), 646 (96%) imposed at least one type of coverage requirement beyond the drug's FDA label (i.e., a subgroup restriction, step therapy restriction, and/or prescriber requirement). One hundred thirty-three policies (20%) imposed one type of coverage requirement; 337 (50%) imposed two types of coverage requirements (100 subgroup restriction + step therapy, 162 subgroup restriction + prescriber requirement, 75 prescriber requirement + step therapy), and 176 policies (26%) imposed all three types (data not shown).
Overall, commercial plans applied restrictions more frequently; for example, subgroup and step therapy criteria were present in 85.5% and 57.8% of commercial coverage policies, compared with 58% and 57.4% of Medicaid policies, respectively (Supplemental Table 2). In contrast, Medicaid plans were somewhat more likely to include prescriber requirements, which were present in 76.4% of Medicaid policies compared with 62.2% of commercial policies (Supplemental Table 2).
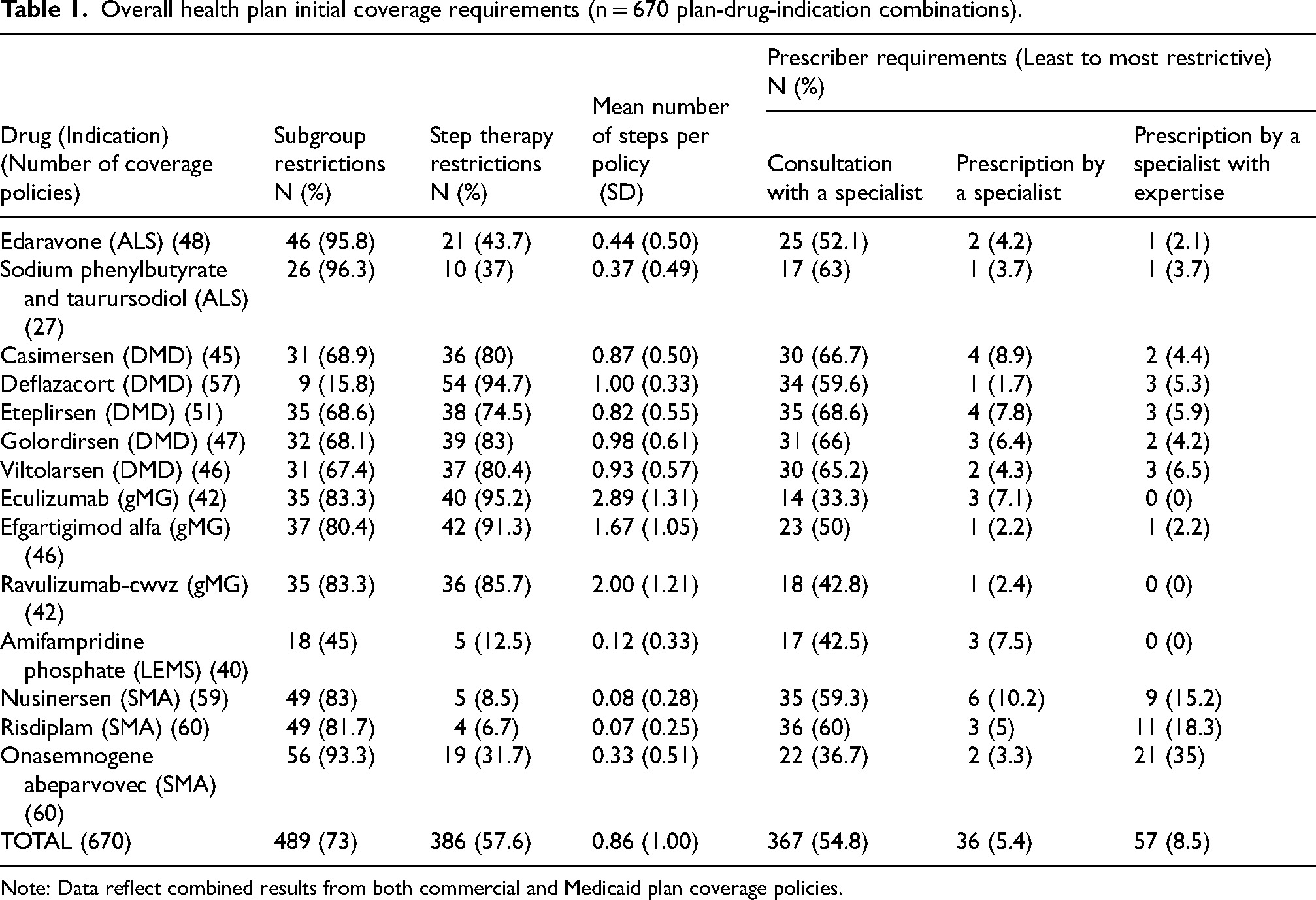
Four hundred eight-nine policies (73%) included at least one subgroup restriction (Table 1). Restrictions most commonly pertained to a required range of respiratory function, motor function, activities of daily living (ADL), symptom duration, and scores on indication-specific clinical assessment measures (e.g., the Quantitative Myasthenia Gravis scale or the ALS Functional Rating Scale) (Supplemental Table 8). These requirements are not included in the FDA-approved indication statement.
Overall health plan initial coverage requirements (n = 670 plan-drug-indication combinations).
Note: Data reflect combined results from both commercial and Medicaid plan coverage policies.
Plans varied in their use of clinical outcome assessments to determine eligible subgroups (Supplemental Table 8). For instance, for eteplirsen for DMD, Massachusetts Medicaid required beneficiaries to be ambulatory and have five timed function tests: timed 10-meter walk/run, timed floor (supine) to stand, timed four-step descend, timed four-step climb, timed sit to stand), whereas another Pennsylvania Medicaid required significantly fewer eteplirsen restrictions but still required a prescription by a specialist and general baseline testing (Supplemental Table 8). Additionally, for efgartigimod alfa for gMG, plans varied with respect to their application of the same functional assessment measures, for example, one plan required a baseline MG-ADL score of ≥5 whereas another required a score of ≥6 (Supplemental Table 8).
Plans implemented step therapy restrictions in 386 (58%) policies (Table 1). However, plans imposed different numbers of prior therapy requirements even for the same drug (Supplemental Table 8). For example, one policy for eculizumab for gMG required 4 steps (an acetylcholinesterase inhibitor + two immunosuppressive therapies + intravenous immunoglobulin or plasmapheresis/plasma exchange); whereas another policy for the same drug required 3 steps (ravulizumab + efgartigimod + immunosuppressive therapy) (Supplemental Table 8). Further, not all plans imposed step therapy restrictions in the same way, e.g., some plans specified a required minimum duration of step therapy whereas others did not (Supplemental Table 8).
Four hundred sixty policies (69%) included prescriber requirements (Table 1). Fifty-five percent of policies required consultation with a specialist, 5.4% required prescription by a specialist, and 8.5% required prescription by a specialist with expertise (Table 1). The frequency and onerousness of prescriber requirements also varied by drug and indication (Table 1 & Supplemental Table 2).
Among available policies that conferred some degree of coverage (n = 670), 467 (70%) provided the duration of initial approval (75% of commercial and 63% of Medicaid policies) (Supplemental Table 3 & Supplemental Table 4). Initial approval was 6.4 months on average, although this varied by drug and indication as well as within the same drug (Supplemental Table 3 & Supplemental Table 4).
Reauthorization of coverage requirements
Among policies that conferred some degree of drug coverage (n = 670), 540 (81%) specified reauthorization requirements (Table 2): 308 (84%) commercial policies, 232 (76%) Medicaid policies (Supplemental Table 5). The proportion varied by payer type, drug, and indication (Table 2 & Supplemental Table 5). Eighty-five policies required a non-specific treatment benefit, 180 required slowed disease progression, 179 required stabilization or maintenance, and 96 required improvement (Table 2). Treatment response requirements also varied by drug and by indication across plans (Table 2 & Supplemental Table 5).
Overall health plan reauthorization of coverage requirements (n = 540 drug-indication combinations).
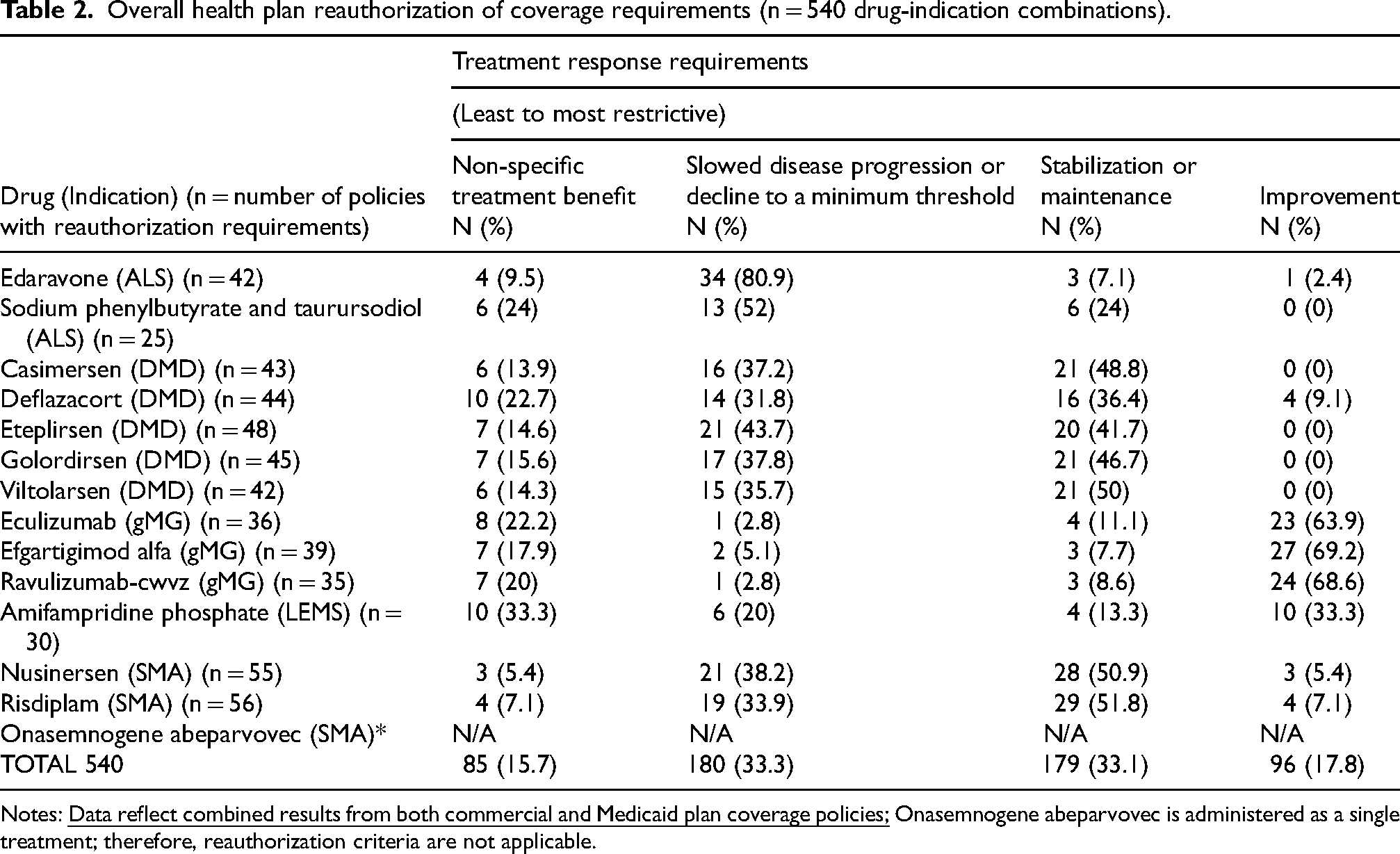
Notes:
Plans varied in the type and amount of evidence they required to demonstrate treatment response. For example, one policy for deflazacort for DMD required submission of medical records to demonstrative an improvement or maintenance of 6-min walk test score and 10% weight loss from baseline, while another required physician attestation of a “positive clinical response” (Supplemental Table 8).
Of the 670 policies that conferred some degree of coverage, 393 (59%) provided the duration of reauthorization (Supplemental Table 3); 225 (62%) commercial, 168 (55%) Medicaid policies (Supplemental Table 4). The mean reauthorization approval duration was approximately 10 months across plans, and while there were some differences between drugs and indications, we found less variation in plans’ reauthorization durations compared to initial durations (as measured by the magnitude of the standard deviation) (Supplemental Table 3 & Supplemental Table 4).
Discussion
Our analysis of NMD therapy coverage policies revealed issues with coverage transparency and frequent coverage requirements and restrictions. We report three main findings: (1) health plans did not provide publicly accessible coverage policies in 25% of cases (Figure 1); (2) when policies were available, plans frequently imposed restrictions on initial and continued access; and (3) requirements, restrictions, and approval durations varied within and between health plan, drug, and indication.
First, health plans issued a publicly available coverage policy in three of every four cases. This is less frequent than previous studies of commercial policy availability (94–100%) for neurology and cell and gene therapies, possibly due to our inclusion of smaller commercial health plans, and in line with existing estimates of Medicaid policy availability (30–41%).19,21,23 Even fewer policies specified reauthorization requirements and approval durations. Many NMD therapies are life-long therapies therefore patients must undergo multiple reauthorizations for access. A lack of transparency and policy availability impose a “learning cost” on patients and providers and may lead to coverage denials 24 and delayed access to treatment. 25 Because NMD therapy effectiveness depends on administration before a certain age or disease stage, such delays have the potential to compromise health. Informed decision making by patients and providers depends on coverage transparency and more easily accessible coverage information could encourage health plan accountability. 26
The second main finding relates to the frequency and burden of coverage restrictions in available policies. Although state Medicaid programs covered all therapies under the federal Medicaid Drug Rebate Program mandate, some commercial plans excluded therapies. 22 When plans did cover therapies, approximately 9 in 10 policies imposed at least one restriction beyond the FDA label, and about 3 in 4 included two or more types of restrictions. Multiple coverage restrictions can create onerous requirements that delay access to care, impose compliance costs, and burden the healthcare system.10,11 One study estimated that patients, providers, health plans, and manufacturers collectively spend about $93.3 billion annually navigating and challenging UM processes. 27 In some cases, these barriers may not only delay but ultimately prevent patients from receiving timely or optimal care. This issue is particularly relevant in neuromuscular disease (NMD) care, where 70% of surveyed providers reported that coverage restrictions hinder initiation of disease-modifying therapy. 1 While prescriber requirements may be appropriate for therapies involving genetic testing, provider networks must ensure equitable access to specialty care—particularly for patients in rural or underserved areas. 28
Further, onerous reauthorization requirements can disrupt treatment as patients and providers work to meet documentation and clinical criteria for continued access—an issue that is compounded when plans set short approval durations, requiring these burdensome processes to be repeated more frequently. Among commercially insured adults with SMA, nusinersen persistence fell from 67% at 6 months to 57% at 1 year, which study authors hypothesized coincided with plans’ approval duration. 29 Restrictive reauthorization criteria may reduce long term adherence and persistence with NMD therapies which is critical for patients who already have obtained access. While we found that the duration of reauthorization approval tended to be longer than that of initial approval, frequent visits to NMD centers may impose transportation costs and disrupt patients’ and care partners’ schedules. 30
Third, we found significant variation in requirements and restrictions by payer type, drug, and indication. Inconsistent coverage for the same therapy means that patients in different states, or in the same state with different health plans, have differential access to treatment. Variation may be a result of a lack of consensus guidelines for specific therapeutic areas within NMD7,31 which may lead plans to draw on variable sources such as FDA labels, clinical trial inclusion and exclusion criteria, or economic evaluations. 32 In light of expert panel recommendations to revise ALS coverage restrictions, 31 our findings suggest that scrutiny of the clinical appropriateness of other NMD coverage requirements may be warranted as well. More real-world and patient-centered data can help health plans, providers, and patients converge on evidence-informed decisions.33,34
Our findings have implications for pharmaceutical policy and practice. First, commercial and government payer policies should be published, transparent, and accessible for patients with chronic irreversible NMDs. Additionally, our finding of a lack of coverage transparency suggests that federal reforms targeting pharmaceutical prior authorization and step therapy requirements would be beneficial. For example, the Centers for Medicare and Medicaid Services’ proposal to improve coverage transparency, automate prior authorization processes, and expedite review 35 could be impactful for patients with Medicaid if expanded to include physician-administered drugs, some of which may be covered under plan medical benefits. The finding of variation in reauthorization requirements suggests a need for regulation to limit these differences and align to clinical care. 14 Finally, health plans should revisit benefit design, taking into consideration the health system consequences of onerous coverage restrictions—including preventable morbidity and mortality from delayed or abandoned treatment10,12,1336–38; increased costs,39,40 physician burnout, and clinical errors.41,42 New designs could include value-based payment models 43 or instant approval processes. 44
Limitations
This study has several limitations. First, we did not assess unpublished coverage policies not available to the public or from Children's Health Insurance Program plans, small commercial plans, or Medicaid managed care plans (which must legally provide equally generous coverage than is offered by fee-for-service plans 45 ). In addition, we excluded Medicare Part D formulary information because these formularies do not sufficiently describe the eligible patient population for inclusion in our analysis. Second, in an attempt to summarize across types of NMD, we did not examine all aspects of coverage (e.g., age of eligibility or diagnostic testing requirements). Third, we did not examine coverage denial appeals processes. Fourth, we did not examine patients’ actual use of NMD therapies, which would require electronic health record or claims data. Lastly, all policies were extracted in May 2023 therefore current policies may have changed. These limitations suggest our findings represent a conservative characterization of the burden associated with accessing NMD treatments. Future work should examine other aspects of administrative costs, including psychological and time burdens to patients, families, and providers.
Conclusions
A person's access to therapies to treat rare neuromuscular diseases depends on what coverage their insurance happens to offer. Our findings of gaps in transparency, frequent requirements and restrictions, and wide variation in coverage may inform ongoing debate surrounding prior authorization reform and pharmacy benefit design. Overly restrictive policies may negatively impact clinical outcomes and health-related quality of life for people living with these chronic, irreversible, and oftentimes fatal neuromuscular diseases.
Supplemental Material
sj-docx-1-jnd-10.1177_22143602251405815 - Supplemental material for U.S. health plan coverage of Neuromuscular Disease Therapies: An assessment of policy availability and restrictions
Supplemental material, sj-docx-1-jnd-10.1177_22143602251405815 for U.S. health plan coverage of Neuromuscular Disease Therapies: An assessment of policy availability and restrictions by A Alex Levine, Julia A Rucker, Alex Cockerham, Joel Cartner and James D Chambers in Journal of Neuromuscular Diseases
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research study was supported by the Muscular Dystrophy Association and Sarepta Therapeutics, Inc.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AL, JR, JCh, and JCa have no conflicts of interest to disclose.
AC is an employee and shareholder of Sarepta Therapeutics, Inc.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.