
Abstract
Background:
In a previous study we demonstrated that standardized tapering off subcutaneous immunoglobulin (SCIG) is a safe way to identify remission in patients with chronic inflammatory demyelinating polyneuropathy (CIDP). However, clinical characteristics and dosage of SCIG in patients in remission are unknown.
Methods:
In the present study, we aimed to identify characteristics of patients in remission during tapering off SCIG. Participants received a stable SCIG dosage and followed a standardized tapering off regimen providing 90%, 75%, 50%, 25% and 0% of the initial dose, every 12th week, pending no deterioration occurred. All patients were followed for 164 weeks after inclusion and were evaluated with disability scores, quality of life score (EQ-5D-5L), blood samples and clinical examination.
Results:
Receiving a dosage of SCIG >25 g/week predicts a higher risk of relapse, OR 6.3 (95CI 1.8-20.2)(p = 0.004), but not when considering body weight (SCIG >0.3 g/kg/week), OR 3.3 (95CI 1.0-9.7)(p = 0.05). Moreover, a higher level of serum NfL OR 8.2 (95CI 1.1-93.3)(p = 0.04) predicts relapse. Low scores on EQ-5D-5L at baseline predicted increased risk of relapse. Serum calprotectin was similar in patients with relapse and in remission. Evaluating measurements from baseline, final visit and the last visit before final visit (LVBF), we found that deterioration in clinical performance could not be predicted at LVBF based on any of the tests performed.
Conclusion:
Patients experiencing a relapse of CIDP during tapering off SCIG seem to receive a total higher dosage of immunoglobulin and had a higher sNfL prior to tapering off compared to patients without a relapse.
Keywords
Introduction
Subcutaneous immunoglobulin (SCIG) is effective as maintenance treatment of chronic inflammatory demyelinating polyneuropathy (CIDP).1–3 In our previous study we demonstrated that during standardized tapering off SCIG treatment, 36% of patients were in remission with no response to treatment. 4 This is in line with an epidemiological study of CIDP suggesting a remission rate of approximately 30%. 5
Factors predicting remission are sparsely described in CIDP patients receiving maintenance therapy. So far, no studies have evaluated which clinical evaluations or biomarkers predict outcome or remission in CIDP. We have reported that frequent clinical control during tapering off SCIG did not improve detection of clinical deterioration as compared to less frequent control and patients’ self-registration. 4
Measurement of neurofilament light chain (NfL) in CIDP has been suggested as a biomarker of disease activity, however, findings have been conflicting, and therefore NfL is not an established biomarker for CIDP.6–8 Calprotectin in one study appeared to be a potential marker for disease activity, but this has not been confirmed by others. 9
Based on the findings obtained in our tapering off study, we aimed to perform post-hoc analyses to evaluate characteristics of remission and relapse during SCIG tapering off. The predictive value of anthropometrics, clinical test performances and dosage of IgG at baseline was analysed in relation to outcome of dose reduction. In addition, we evaluated whether earlier findings at intermediate visits could be used to predict relapses.
Finally, we aimed to evaluate whether biomarkers reflecting axonal degeneration and inflammation (serum NfL (sNfL) and serum calprotectin) are related to risk of relapse.
Material and methods
Full details of the study evaluating standardized tapering off SCIG in CIDP have previously been reported. 4 A brief outline is provided here: Patients with CIDP and stable treatment with SCIG (>3 months) participated in the study. In all patients the weekly dosage of SCIG was regularly tapered off following the regimen (fraction of individual weekly dosage before enrolment): 90%, 75%, 50%, 25% and 0% given for 12 weeks each. Participants were randomized to be evaluated every 6th (frequent) or 12th (less frequent) week, and if no deterioration occurred, the dosage was further reduced. If deterioration occurred, participants were excluded from further tapering off and the dosage was increased to the lowest dosage providing clinical stability. For participants in whom complete tapering off was successful, the final evaluation was performed 12 weeks after end of treatment. In addition, two years after each patient's last evaluation a final status regarding immunoglobulin treatment was made.
Blood samples were drawn at every visit centrifuged and stored as serum in vials of 0.5-1.0 mL at −80 oC for up to 5 years prior to analyses with no thawing or refreezing in between.
Clinical evaluation
We evaluated disability with the Overall Disability Sum Score (ODSS) with a range from 0 (not disabled) to 12 (severely disabled) and the Rasch built overall disability score for CIDP (RODS), consisting of 24 items describing usual daily living activities. Each item is scored from 0 (easy to perform) to 2 (cannot perform), giving a total range of 0 to 48.10,11 Quality of Life (QoL) was assessed using the European Quality of Life – 5 dimensions – 5 levels questionnaire (EQ-5D-5L) including a Visual Analogue Scale (VAS). An index value based on the score from the five items: mobility (MB), self-care (SC), usual activities (UA), pain/discomfort (PD) and anxiety/depression (AD) was calculated. Index value was based on normative values from the Danish population. 12 Each item ranges from 1 to 5 according to level of influence. The VAS determined the patient's self-evaluated health on the day of examination using a range from 0 (worst health) to 100 (best health).
Manual muscle strength was assessed using the modified Medical Research Council (MRC) sum score with bilateral evaluation of shoulder abduction, elbow flexion/extension, wrist flexion/extension, hip flexion, knee flexion/extension and ankle dorsal flexion each ranging from 0 (no movement) to 5 (normal strength) resulting in a maximum score of 90 points. Hand-held grip strength was determined using a JAMAR dynamometer based on the average of a triple, bilateral measurement.
Dexterity was determined using the 9-hole-peg test (9-HPT) and walking performance with the 10-meter-walk test (10-MWT). All tests were performed twice, and the average value was used in further analyses.
The criteria for clinical meaningful deterioration were an increase in the ODSS of ≥ 1 point and/or a decrease in grip strength of >4 kg. 4
In this post hoc analysis values from baseline and final visits were compared to data from the last visit before final (LVBF) to study whether a pending deterioration had occurred.
Measurements of serum NfL and calprotectin
NfL and calprotectin concentrations were detected in serum samples from baseline and last visit in each patient. NfL was measured by the NF-lightVR assay using the ultrasensitive SimoaTM HD-1 platform (Quanterix#, Lexington, MA, USA). The measurement range is 1.4-1800 ng/L. For comparison, the reference values from Department of Biochemistry at Aarhus University Hospital were used. 13
Circulating calprotectin was analysed using the Phadia 250 EliATM Calprotectin flouroenzymimmunoassay (research use only, Thermo Fisher Scientific, Freiburg, Germany). The measurement range is 3.8-6000 ng/mL.
Statistics
As this is a post-hoc analysis, no power calculations were made.
Comparison of continuous data between the two groups (relapse and remission) were analysed with paired or unpaired t-tests or Wilcoxon's signed rank test when appropriate. Fisher's exact test was used due to the low number of participants for analysing the odds ratio (OR) of relapse. Because of multiple comparisons Bonferroni post-test was used, using a p-value of (0.05/10 = 0.005) being significant.
Results
Fifty-five patients were included in the study, 28 being randomized to frequent evaluation every 6th week and 27 to evaluation every 12th week. All participants followed the same tapering off regimen, and there was no difference in the rate of relapse comparing the two groups. 4 In total, 35 participants (64%) from the entire cohort experienced relapse following tapering off SCIG treatment and 20 participants (36%) went into remission. We included all relapsing participants encompassing both patients fulfilling the clinical criteria for deterioration (n = 23) as well as those not fulfilling the criteria who refused further dose reduction (n = 12). The average follow-up for these patients was 167 days (range: 42 to 447).
Serum NfL and calprotectin
For serum analyses for NfL and calprotectin we had samples from 32 participants (relapse) and 19 participants (remission). At baseline serum NfL (sNfL) was higher in patients with a later relapse as compared to patients without a relapse (16.4 ng/L (range: 4.9 to 90.2) versus 13.1 ng/L (range: 4.5 to 31.4) (p = 0.026)). At the end of the study there was no statistically significant difference, 17.3 ng/L (range: 5.6 to 59.6) versus 12.2 ng/L (range: 4.3 to 43.5) (p = 0.123). Comparing baseline and end of study values of sNfL, the two groups did not differ (Figure 1A).
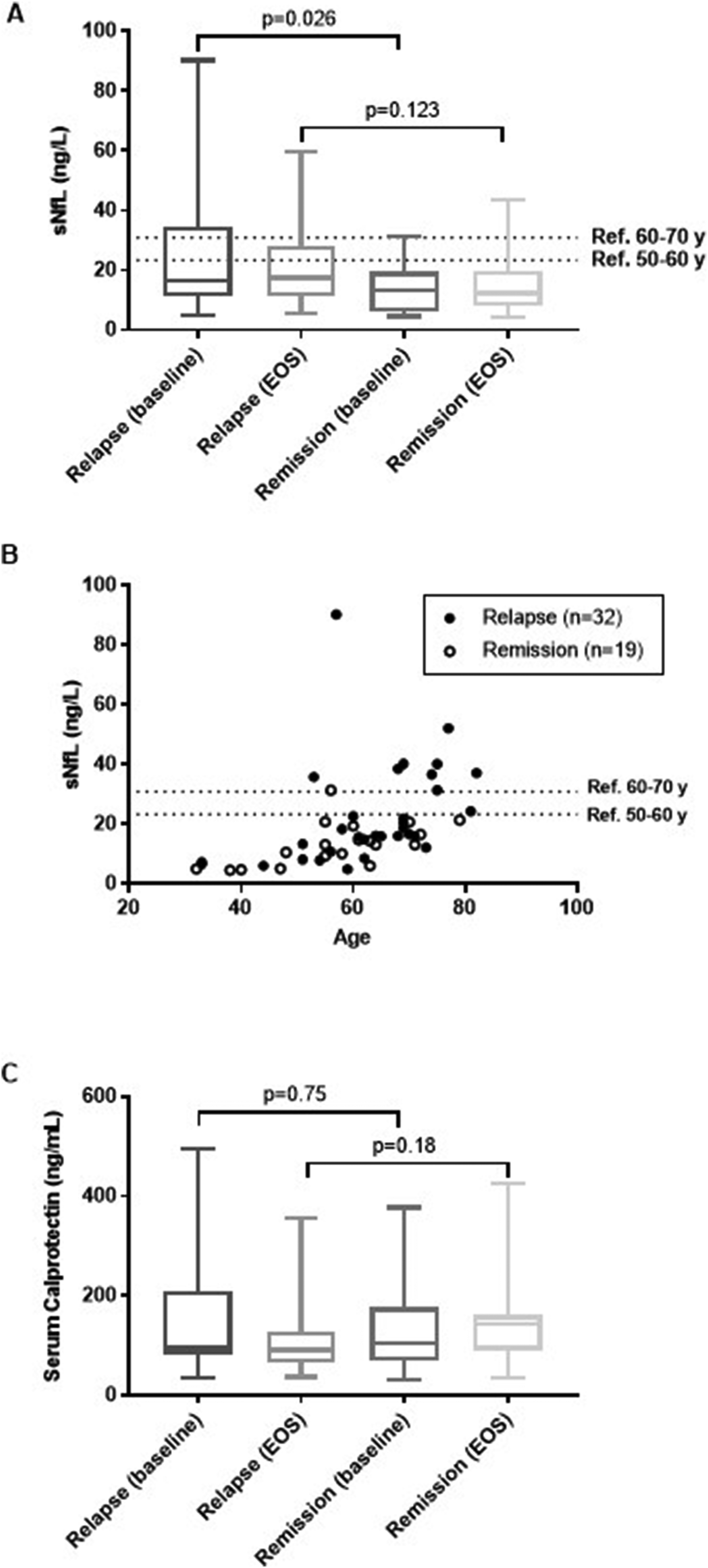
Mean levels of serum neurofilament light chain (sNFL) and serum calprotectin (A): sNFL in patients with relapse versus remission at baseline and at end-of-study (EOS) (B): Individual sNFL levels at baseline versus age (C): Serum calprotectin in patients with relapse versus remission at baseline and at end-of-study (EOS).
It is well established that sNfL increases with age, 13 and by interpreting our reference values (<23.3 ng/L for 50-60 years and <30.9 ng/L for 60-70 years) it seems that there is an over representation of patients with relapse who has a sNfL > 23.3 ng/L irrespective of age, as only one patient of 19 (5%) in remission had a value exceeding this limit, whereas for patients with relapse, 10 of 32 (31%) had a value > 23.3 ng/L (Figure 1B).
Serum calprotectin was similar in the two groups at baseline: 94 ng/mL (range: 35 to 494) versus 104 ng/mL (range: 31 to 377) (p = 0.75) and at end-of-study: 90 ng/mL (range: 36 to 356) versus 143 ng/mL (range: 34 to 424) (p = 0.18) (Figure 1C).
Prediction of relapse from baseline data
At enrolment, comparing patients staying in remission and patients with patients experiencing a relapse, patients relapsing received a higher weekly dose of SCIG, 30 gram per week (range: 9.9 to 49.5) as compared to patients in remission, 23.1 gram per week (range: 9.9 to 56) (p = 0.047) (Table 1).
Anthropometrics and clinical characteristics of CIDP patients.
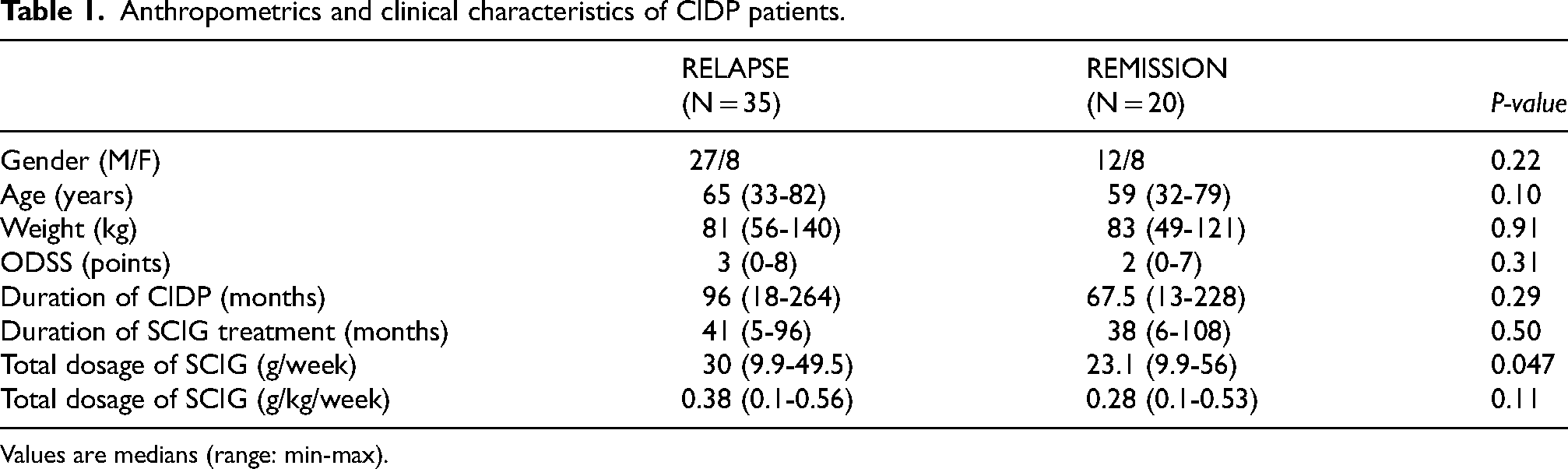
Values are medians (range: min-max).
Odds ratio for relapse during SCIG withdrawal in relation to anthropometrics and baseline characteristics.
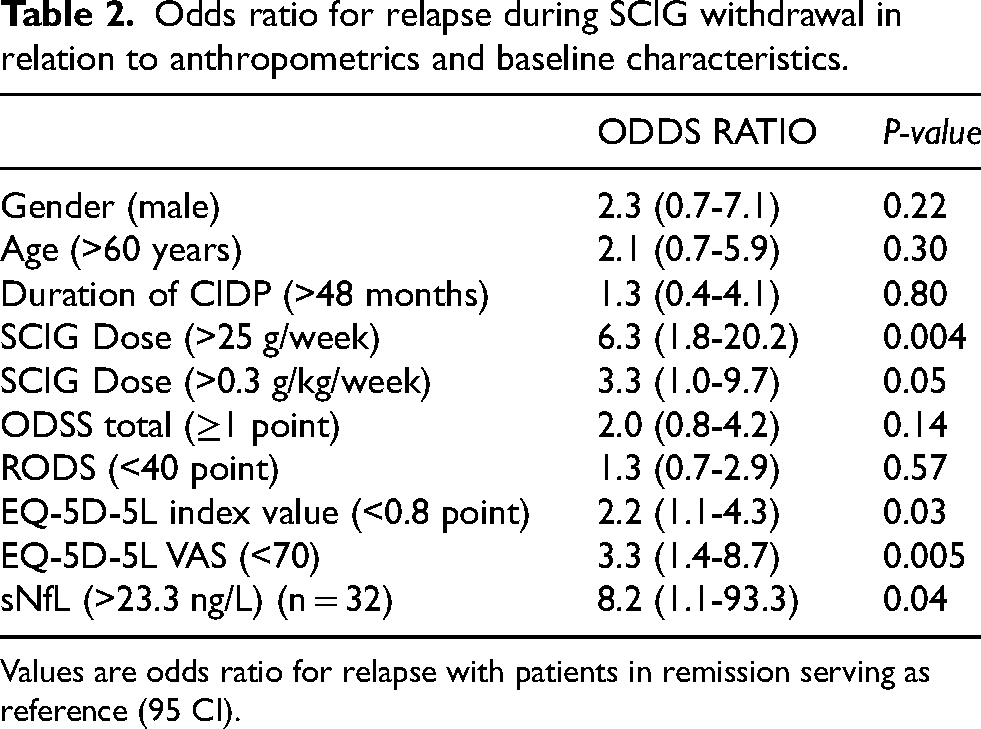
Values are odds ratio for relapse with patients in remission serving as reference (95 CI).
At baseline, the odds ratio (OR) for a relapse due to tapering off SCIG was 6.3 (95CI 1.8 to 20.2) (p = 0.004) if dosage of SCIG exceeded 25 g/week. Evaluating SCIG in relation to body weight, the OR did not reach statistical significance however the OR was still clearly higher, OR 3.3 (95CI 1.0 to 9.7) (p = 0.05). There was no difference in the clinical assessments (e.g., ODSS, RODS, MRC, grip strength etc.).
EQ-5D-5L was different for the VAS scale, OR 3.3 (95CI 1.4 to 8.7) (p = 0.003), but not for the index value, OR 2.2 (95CI 1.1 to 4.3) (p = 0.03), when corrected for multiple comparison.
sNfL levels exceeding 23.3 ng/L was found to be a risk for relapse having an OR of 8.2 (95CI 1.1 to 93.3) (p = 0.038) (Table 2).
Prediction of relapses from final and intermediate data
Six patients had a relapse before the first follow-up visit and were not included in the following analyses. The average interval between baseline visits and LVBF was 131 days (range: 53 to 364) and 60 days (range: 19 to 98) between LVBF and the final visit.
ODSS, grip strength, 10-MWT, RODS and EQ-5D-5L did not differ comparing baseline and intermediate evaluation (LVBF), however a deterioration was observed between LVBF and the final evaluation. Evaluating changes in measurements between baseline and LVBF, there was no change in 10-MWT, RODS, grip strength or QoL whereas ODSS improved, although not clinically meaningful (Table 3).
Changes in clinical measurements between baseline, last visit before final (LVBF) and final visit in patients with relapse.
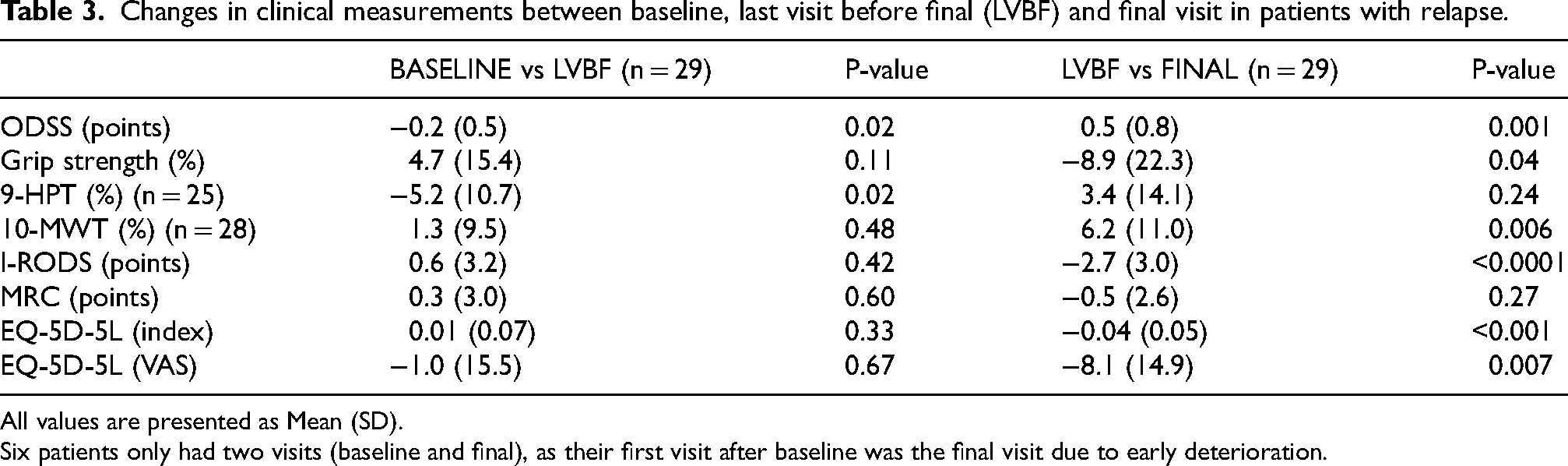
All values are presented as Mean (SD).
Six patients only had two visits (baseline and final), as their first visit after baseline was the final visit due to early deterioration.
Discussion
We found that a dosage of SCIG > 25 g/week was more frequent in patients experiencing a relapse, but when adjusting for body weight it did not reach statistical significance. Also, patients relapsing had a lower QoL and a higher sNfL compared to patients staying in remission. Clinical deterioration could not have been predicted at the LVBF, as clinical measurements from baseline to LVBF was unchanged, and the deterioration was between LVBF and final visit.
Previous studies have shown that 30-40% of CIDP patients will remit during their disease course with no further need for treatment. 14 This is the first study to evaluate if relapse of CIDP can be predicted prior to or during tapering off SCIG. In clinical practice the decision to stop treatment is primarily based on disappearance of symptoms and neurological deficits but patients with CIDP can also have irreversible deficits where medical treatment no longer has effect. The EAN/PNS guidelines recommend frequent attempts of tapering off therapy to detect responsiveness. 15 A recent study of patients with CIDP treated with intravenous immunoglobulin (IVIG) found that the same percentage of patients experienced relapses following randomization to blinded withdrawal of IVIG or IVIG at unaltered dosage. 16 These results indicate that detection of being in remission in CIDP is difficult. Nonetheless, to avoid unnecessary therapy withdrawal should be attempted as recommended. 15 In support, our previous study showed that 36% of clinically stable patients with CIDP treated with SCIG could be tapered off treatment. Furthermore, in patients experiencing a relapse, average dosage could be reduced with 10%. 4
Several studies have aimed to identify biomarkers reflecting disease activity, however until now these attempts have remained unsuccessful. Recently, NfL has been proposed to be a useful biomarker as, in several studies, NfL was found higher in blood and cerebrospinal fluid in CIDP compared to healthy controls, and in patients with active CIDP compared to patients in remission.6,8,9 However, these findings need further confirmation prior to recommendation for use in daily clinical practice.8,17 Based on our findings, sNfL could be related to activity in CIDP, but we could only demonstrate a difference between relapse and remission at inclusion. Therefore, further studies are warranted before it can be decided whether sNfL has a role in future evaluation of CIDP disease activity. In a recent meta-analysis Kodal et al. concluded that the usefulness of NfL in serum and cerebrospinal fluid is divergent and the included studies disagree about the interpretation of NfL in CIDP. 8 Our findings are in line with this understanding. We could not detect a difference in relapsing patients, from baseline to end-of-study, but this could be due to the short follow-up between enrolment and end-of-study, and that some patients had symptoms indicating a relapse that did not fulfil the predefined criteria.
Serum calprotectin in CIDP has only been described in one study by Stascheit et al. and was proposed to be related to disease activity. They described that calprotectin was lower in CIDP patients in remission compared to patients with active disease. 9 We could not confirm this in our study.
There are some limitations of our study. We included both patients who reported deterioration in their clinical condition and those who fulfilled the predefined criteria for clinical meaningful deterioration. This is a frequent situation in care of patients with CIDP and reflects a fundamental challenge as to whether treating physicians should focus on subjective or objective measures. Approximately, two-thirds of the patients with relapses fulfilled the criteria for deterioration, while one-third decided to leave the study because of a subjective perception of deterioration. Therefore, the remission rate may be higher than the 36% reported.
Our study underscores that it remains challenging to predict relapse prior to tapering off treatment, however standardized tapering off offers a safe and effective way to identify patients in remission. Many patients are reluctant to reduce immunoglobulin treatment due to fear of relapse. Performing stepwise reduction with frequent clinical tests increases adherence to tapering off as patients feel more secure. On the other hand, it is important to align expectations to what the clinician and the patient define as relapses, e.g., reports from the patient or clinical measurements. Overall, we recommend more focus on the possibility of remission in CIDP patients. Based on our findings we suggest that remission is unlikely in patients receiving a dose of SCIG > 25 g/week, a sNfL > 23.3 ng/L and/or EQ-5D-5L VAS < 70.
Conclusion
Predicting remission in a patient with CIDP receiving maintenance therapy with SCIG is challenging. We found that a higher dose of SCIG, a higher level of sNfL and lower level of QoL by EQ-5D-5L VAS indicate a higher risk of relapse during tapering off SCIG. Pending relapse cannot be predicted by clinical tests and evaluations during tapering off.
Footnotes
Acknowledgements
None
Ethical considerations,registrations,and patient consent
All participants gave written informed consent before the screening procedure to participate. The study was approved by the Central Denmark Region Committee on Health Research Ethics (1-10-72-177-17) and the Danish Medicines Agency (2017113751) and registered in the EU Clinical Trials Register (EudraCT 2017-002024-24) by 9 June 2017.
Author contributions
Lars K. Markvardsen: Drafting/revision of the manuscript for content, including medical writing for content. Major role in the acquisition of data. Study concept and design. Analysis and interpretation of data.
Helga Haahr-Lillevang: Major role in the acquisition of data and revision of the manuscript for content, including medical writing for content. Study concept and design. Interpretation of data.
Tobias Sejbæk: Major role in the acquisition and interpretation of data.
Tina Parkner: Major role in the acquisition of data and revision of the manuscript for content, including medical writing for content.
Søren Sindrup: Major role in the acquisition of data and revision of the manuscript for content, including medical writing for content. Interpretation of data.
Johannes Jakobsen: Major role in the acquisition of data and revision of the manuscript for content, including medical writing for content. Study concept and design. Interpretation of data.
Henning Andersen: Major role in the acquisition of data and revision of the manuscript for content, including medical writing for content. Study concept and design. Interpretation of data.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Danish Regions, (grant number 16/2885).
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Markvardsen has received honoraria from CSL Behring, Alexion, Amicus and Takeda Pharma and served as advisory board members at Takeda Pharma and CSL Behring.
Dr. Sejbæk has nothing to disclose.
Dr. Parkner has nothing to disclose.
Dr. Sindrup has nothing to disclose.
Dr. Jakobsen received speaker honoraria from Takeda Pharma A/S.
Dr. Haahr-Lillevang has nothing to disclose.
Dr. Andersen has received honoraria from Novo, Amicus, Alexion, Lundbeck, Zealand Pharma, and served as member of advisory board at NMD Pharma, Amicus, Alexion, Biogen, UCB Pharma.
Data availability
The dataset used and analyzed in this study will be made available upon request by the corresponding author to qualified researchers (i.e., affiliated with a university, research institution or hospital).