
Abstract
The 2025 MDA Gene Therapy Summit brought together leading researchers, clinicians, and industry representatives to discuss the latest advancements and challenges in the development and clinical translation of genetic therapies for neuromuscular disorders. The meeting featured in-depth presentations on clinical trials, therapeutic developments, and regulatory pathways for AAV-mediated gene therapies, highlighting both successes and challenges in the field.
Gene therapy landscape
The Alliance for Regenerative Medicine (ARM), the leading international advocacy organization championing the benefits of engineered cell therapies and genetic medicines, reports a maturing gene therapy sector comprising nearly 3,000 developers and 2,000 active clinical trials, bolstered by a 30 percent increase in investment to $15.2 billion in 2024 (ARM’s Q4 2025 sector data update reports 1856 developers and 2130 active clinical trials 1 ). The regulatory and clinical testing pipelines remain robust; as of the meeting date, 12 gene therapies were projected for approval in 2025 and 51 active trials for neuromuscular diseases (ARM’s Q4 2025 sector update reports 6 new approvals were made in the US and 3 in Europe 1 ). Data from the Tufts NEWDIGS program and supported by ARM, indicate that orphan gene therapies are approximately 2 to 3.5 times more likely to achieve FDA approval than traditional drugs when entering clinical trials, outperforming the broader pipeline at all clinical trial phases. To accommodate these breakthroughs, the U.S. healthcare system is adapting through initiatives such as Medicaid reforms aimed at increasing patient affordability and value-based contracting. FDA initiatives like the START (Support for clinical Trials Advancing Rare Disease Therapeutics) program have been established to streamline approvals and support rare disease therapies, while the Center for Medicare and Medicaid Innovation (CMMI) is piloting outcome-based agreements via the Cell and Gene Therapy Access Model to help states manage access to gene therapies for people living with sickle cell disease. While already approved gene therapies for sickle cell disease and hemophilia illustrate the potential long-term cost-effectiveness of one-time, potentially curative treatments, the clinical and economic impact of gene therapies will vary across diseases and products. Specifically, long-term follow up studies for approved gene therapies, such as Zolgensma (SMA) and Elevidys (DMD) are required to fully deduce the economic and clinical impact of these neuromuscular disease gene therapies. Despite persistent challenges in cost, access and regulatory hurdles, experts agree that one-time gene therapies are poised to redefine the standards of care for genetic diseases and improve healthcare outcomes worldwide.
Gene therapy programs for DMD
The summit invited three companies (Sarepta, Pfizer, REGENXBIO) with DMD microdystrophin gene therapy programs to provide updates.
Sarepta’s Elevidys initially received accelerated approval from the FDA in June 2023 for ambulatory patients aged 4–5 years old. This was followed by expansion of the regulatory approval in June 2024, which granted traditional approval for all ambulatory patients aged 4 and older and accelerated approval for non-ambulatory patients. These decisions were primarily informed by the EMBARK trial (n = 125), which found that secondary functional outcomes demonstrated clinically meaningful treatment effect. 2 Biomarker analysis further confirmed consistent micro-dystrophin expression across the broader cohort. Topline three-year efficacy results have recently become available, showing slowing of disease progression by measures of North Star Ambulatory Assessment (NSAA), time-to-rise, and 10 Meter Walk/Run test (10MWR), with increasing divergence from expected course of disease over time. While adverse effects such as nausea, vomiting, liver injury, and thrombocytopenia were observed in the initial clinical studies, fatalities due to acute liver failure (ALF) in the post-marketing experience supported the addition of a boxed warning in late 2025 regarding the risks of acute serious liver injury and liver failure. Consequently, as of late 2025, dosing in the ENVISION trial, which is designed to evaluate the long-term efficacy and safety for non-ambulatory and older populations was paused to investigate safety signals and refine monitoring protocols which now correspond to the recently published guidelines for administration of gene therapy products in DMD. 3 The FDA officially restricted the use of Elevidys to only ambulatory patients. In response, Sarepta has initiated a new cohort in the ENDEAVOR trial (Study 9001-103) to evaluate co-administration of prophylactic sirolimus to evaluate its use as an immunosuppressant to mitigate these severe liver risks in the non-ambulatory population.
REGENXBIO’s RGX-202 program initially enrolled 11 patients aged 4–11 years (with enrollment later expanding to a total of 13 patients at study conclusion) in the Phase 1/2 AFFINITY Duchenne Trial. The study evaluated safety, micro-dystrophin expression, and exploratory functional outcomes. Results demonstrated consistent micro-dystrophin expression in muscle biopsies, with all patients achieving levels exceeding 10% of normal dystrophin. Functional assessments showed positive trends in mobility, including faster 100-meter walk times, while safety data indicated no serious adverse events (SAEs), myocarditis, or myositis. Following these promising results, RGX-202 has since completed enrollment of 30 patients in its pivotal Phase 3 trial as of October 2025 and remains on track to pursue accelerated FDA approval in 2026. Of note, RERGENXBIO chose from the outset of the study to utilize a prophylactic immune suppression regimen of sirolimus and eculizumab.
Pfizer’s Phase 3 randomized double-blind placebo-controlled trial (CIFFREO) reported that it failed to meet primary (change in NSAA score at 52 weeks) and secondary (10-meter walk/run, rise from floor velocity) endpoints. This outcome occurred despite the therapy achieving significant reductions in creatine kinase (CK) levels and robust micro-dystrophin expression (up to 50% dystrophin-positive fibers), highlighting a discrepancy where favorable biomarker observations failed to translate into actual clinical benefit within the duration of the study. While the study design was sufficient to detect improvements, patient variability and a strong placebo effect, bolstered by the higher corticosteroid regimen doses required to manage AAV related adverse events (also administered to the placebo group), contributed to the non-significant results at the relevant timepoints and ultimately led Pfizer to discontinue the program. This failure underscored critical lessons for the field, specifically that the presence of microdystrophin expression alone might not necessarily translate into clinical benefit. It is possible that there are differences in the functionality of the different microdystrophins that ongoing clinical trials will help to clarify. Lastly, safety ceilings for high-dose AAV9 delivery must be carefully managed following fatal adverse events in this and in related studies.
Discussion summary: DMD gene therapy programs
Randomized, double-blind, placebo-controlled trials remain the gold standard for evaluating efficacy in gene therapy, though establishing full therapeutic benefit may require larger cohorts and extended study durations. There is an urgent need to refine patient selection and stratification based on mutation types, baseline immune responses, and expected clinical benefit. Pulmonary function, often declining late in DMD disease progression, should be included as a secondary outcome measure requiring long-term monitoring. To strengthen regulatory confidence, use of confirmatory trials was emphasized, with full enrollment ideally completed at the time of initial approval. Safety protocols should prioritize standardized reporting of hospitalizations and adverse event tracking to provide clinicians with real-time safety data. Strategies to mitigate complement activation in gene therapy recipients, including the prophylactic use of Eculizumab, were discussed, though questions remain regarding its long-term necessity. From a manufacturing standpoint, standardization of potency assays and rigorous control of vector quality - including empty capsid content and lot-to-lot variability - are critical to ensuring consistent dosing and clinical efficacy. Recent clinical evidence has underscored the potential safety implications of manufacturing-related factors, with a case study reporting hepatotoxicity associated with product quality attributes and manufacturing byproducts. 4 Finally, addressing logistical barriers, including access to complementary medications, variability in insurance approvals, the need for provider retraining, and enhanced data-sharing mechanisms among industry, regulatory agencies, and clinicians are all essential for capturing real-world safety and efficacy data necessary to maximize patient benefits.
Discussion Panel: Patient insights on gene therapy decisions
This Q & A panel, moderated by Dr. Barry Byrne, brought together individuals living with DMD and caregivers, who shared personal experiences and perspectives on treatment decisions, clinical trials, and the evolving landscape of gene therapy. A primary theme explored was the difficulty families face in accessing and interpreting medical information necessary for making informed treatment decisions, exacerbated by a lack of published data on gene therapy outcomes, particularly for older, non-ambulatory patients. This information often forces families to conduct independent research, navigating a complex mix of clinical, industry, and patient community-led resources. The emotional and ethical complexities of clinical trial eligibility were also explored, with participants describing the agonizing process of weighing potential therapeutic benefits against risks of unforeseen adverse events. Some families expressed frustration when excluded from treatment due to restrictive criteria such as pre-existing antibody status or age restrictions. The discussion further addressed concerns regarding selection bias in clinical trials, noting that a preference for participants with optimal baseline health conditions may limit real-world applicability of findings for the broader DMD population. By contrasting the rare disease framework with more established fields like oncology, the panel emphasized the need for improved regulatory frameworks and standardized treatment guidelines. Looking toward, the panelists expressed a strong desire for technical advancements such as full-length dystrophin production, viable redosing strategies, and the use of adjunctive therapies, such as fibrosis-reducing agents, to optimize long-term physiological outcomes. The session concluded with a call for systemic shifts towards greater data transparency and a transition in clinical priorities that value long-term survival and quality of life alongside traditional ambulatory measures.
Discussion Panel: Post-approval real-world experience of Elevidys
The panel discussion on Elevidys (delandistrogene moxeparvovec) focused on clinical considerations in its transition from clinical trials to commercial use, with insights from pediatric neuromuscular neurologists Perry Shieh (UCLA), Diana Bharucha Goebel (NIH), Aravindhan Veerapandiyan (Arkansas Children’s Hospital), and Julie Parsons (Children’s Hospital at Colorado). Drawing on institutional experiences from the Zolgensma rollout, panelists emphasized the importance of informed hospital preparedness to navigate logistical hurdles, including patient prioritization and geographic access disparities for families in rural areas and complex insurance authorization processes that required hospitals to choose between buy-and-bill models or specialty pharmacy distribution. To mitigate the significant financial risks associated with high-cost gene therapies, early engagement with hospital finance teams became a standard operational requirement. Pre-treatment management involved standardized memos of understanding to align family expectations, alongside comprehensive baseline assessments, including antibody screening and cardiac evaluations, typically completed within a 30–90-day window. Delays in insurance approvals often required retesting to maintain eligibility. Post-treatment monitoring revealed a high rate of complications (≈75%), including nausea, vomiting, transaminitis, and rare cases of hyperCKemia, necessitating multidisciplinary care teams that included neurologists, hepatologists, and cardiologists. Institutions implemented close follow-up protocols, with some establishing dedicated gene therapy on-call teams to manage emergent complications, such as elevated troponin levels. Ethical dilemmas also emerged, including cases where adolescent patients refused treatment despite parental insistence, requiring ethics team interventions, and unexpected lab abnormalities that prompted further clinical evaluation. The panel also discussed the uncertainty surrounding antibody threshold exclusions and the potential need for re-dosing strategies. Overall, the discussion highlighted the complexity of integrating gene therapy into clinical practice, emphasizing the need for continued refinement of eligibility criteria, improved financial models, and enhanced long-term patient monitoring to ensure safe and equitable access to Elevidys.
Optimizing success and durability of gene therapy for DMD
The age of gene therapy recipients has been established as a critical determinant of treatment success, thus highlighting the importance of receiving an early diagnosis for DMD, and the implementation of a nationwide newborn screening program. Intervening before significant muscle deterioration occurs optimizes the therapeutic window and increases the potential for better outcomes. Beyond age, the effectiveness of gene therapy is influenced by a complex interplay of factors, including muscle fiber transduction efficiency, the patient’s underlying mutation, and variation in individual immune response profile. Additionally, the duration and timing of corticosteroid use remain under-researched but are believed to be a significant factor in the overall short term therapeutic response. While early intervention may be a favorable approach to maximizing gene expression in the greatest percentage of myofibers, the inability to transduce or correct satellite cells would lead to progressive dilution of the therapeutic effect and shorten durability of expression across the musculature.
The discussion also covered longitudinal outcomes of gene therapy. From clinical trial data, extending as far as 6.7 years post-treatment, all analyzed patients exhibited detectable levels of micro-dystrophin mRNA and protein levels, though the degree of expression and functional benefit varied. This disconnect between expression and function is exemplified by a striking case where a patient maintained stable function years after gene therapy in contrast to others who showed disease progression despite significant dystrophin expression. Due to the dual mechanisms of nuclear domain of micro-dystrophin expression and of the enlargement of muscle fibers associated with the patients’ growth, micro-dystrophin expression in young patients could, in the long term, lead to patchy micro-dystrophin localization, thereby weakening the protective effect of micro-dystrophin along the muscle fibers. These observations underscore that additional factors, outside of micro-dystrophin expression, such as the percentage of dystrophin-positive fibers, the presence of naturally occurring exon-skipping, and corticosteroid appear to play a role in contributing to observed differences in treatment outcomes and shape the long-term physiological trajectory of the disease post-treatment.
Gene editing considerations
Presentations in this session by Scott Harper (Nationwide Children’s Hospital) and Christopher Nelson (University of Arkansas) highlighted common challenges in gene editing for muscular dystrophies using CRISPR-Cas systems. The use of CRISPR-Cas13 delivered via AAV to knockdown DUX4 expression on the RNA level, showed limited long-term durability due to an immune response against the Cas13 protein. 5 T-cell-mediated elimination of treated cells underlies the loss of efficacy of this treatment over time. A point to consider is that the potential for T-cell mediated immune response may also be dependent on the mode of delivery and the expected duration of the CRISPR-Cas9 transgene expression. The lack of precision in genome editing was also raised. Long-read sequencing technologies revealed unintended modifications such as off-target effects, AAV vector integrations at double-strand breaks, chromosomal rearrangements, and exon skipping associated with CRISPR-Cas9 applications in DMD. 6 These findings underscore the challenge of ensuring both the safety and precision of gene editing therapies. To address these concerns, next-generation tools like base editors and prime editors were suggested as potential solutions for improving accuracy and minimizing genomic disruptions, but the long-term presence of foreign bacterial proteins in the body remain an immunological concern with these advanced editing technologies.
Vector and promoter sequence considerations
This session examined advanced strategies for vector and promoter sequence optimization, focusing on achieving tissue-specific expression, avoiding off-target effects, and fine-tuning transgene levels to balance therapeutic efficacy and safety. Speakers presented data-driven approaches involving synthetic regulatory cassettes, transcription factor interactions, microRNA-based regulation, and tissue-specific promoter design.
Steve Hauschka (University of Washington) highlighted the importance of precise regulatory control of therapeutic protein levels to avoid toxicity or insufficient efficacy. Data from the GTEx database illustrated the wide range of natural gene expression levels in muscle, from highly expressed genes like skeletal muscle actin to low-expression genes related to Golgi enzymes. The concept of synthetic regulatory cassettes was introduced, including an artificial enhancer that significantly increased expression levels compared to native creatine kinase enhancers. However, concerns were raised about the potential risks of transgene overexpression when applying these constructs for therapeutic applications.
Sharif Tabebordbar (Kate Therapeutics) presented research on vector sequence optimization for safety and efficacy, focusing on Limb-Girdle Muscular Dystrophy 2A (Calpainopathy). The primary objective was to utilize tissue-specific promoters combined with microRNA binding sites to selectively avoid cardiac expression to prevent potential cardiotoxicity. In non-human primates (NHPs), this approach achieved an 80-fold decrease in transgene mRNA expression in heart relative to skeletal muscles.
Further expanding on dose-sensitive regulation, Steven Gray (UT Southwestern) presented an autoregulatory strategy using microRNA-based approaches for MECP2 in Rett Syndrome, a condition where both deficiency and overexpression are pathogenic. By employing a microRNA-responsive autoregulatory element (miRare), the Gray and Sinnett laboratories created a feedback loop, ensuring transgene expression was silenced in wild-type cells while being active in deficient cells. 7 This approach avoided the Rett-like toxicity seen with unregulated vectors in preclinical mouse studies. A clinical trial initiated in 2023 (Taysha Gene Therapies) reported early motor and communication improvements in treated Rett Syndrome patients.
Discussion summary: Gene-editing, durability and sequence considerations
The discussion centered around newborn screening, and clinical trial methodologies in the context of Duchenne muscular dystrophy (DMD) and related neuromuscular diseases. A key topic was the value of baseline biopsy data in assessing treatment efficacy and its role in clinical trials. Centralizing the sharing of results and maintaining well-controlled datasets was emphasized as a need for refining exon-skipping therapies and understanding how different genotypic variations respond to treatment.
Beyond therapeutic intervention, the implementation of nationwide newborn screening was identified as a transformative tool. Speakers noted its role in facilitating informed family planning and the early detection of neurodevelopmental comorbidities, such as autism spectrum disorder. The debate also touched on the implications of newborn screening on reproductive decisions, with some arguing that its presence does not necessarily change parental choices.
Technical concerns were raised regarding the disconnect between expression-function where post-treatment micro-dystrophin levels do not always correlate with functional motor outcomes. This variability, combined with the understudied long-term impact of various corticosteroid regimens, complicates the use of micro-dystrophin as a primary surrogate endpoint. Furthermore, the correlation between cognitive involvement and neuromuscular weakness remains a complicated factor in predicting overall treatment efficacy.
Gene therapy delivery was another critical area of discussion, particularly regarding dosing strategies. There was debate over whether dosing should be based on body weight or lean muscle mass, with concerns about potential vector uptake into non-target tissues such as adipose tissue. Factors such as a patient’s metabolic state and physical movement during administration were also identified as variables that could influence vector distribution.
Lastly, the immune response to CRISPR-Cas9 gene editing tools remains a primary hurdle for in vivo editing, given their bacterial origin. While some studies suggest a level of tolerance, the potential for T-cell-mediated immune responses against non-human proteins continues to challenge the long-term durability of in vivo gene editing approaches.
The session concluded with reflections on the broader implications of gene therapy and its evolving role in treating neuromuscular disorders. Researchers acknowledged that while current approaches have limitations, ongoing studies and technological advancements may lead to more refined and effective therapeutic strategies in the future.
Innate and adaptive immune responses in gene therapy
This session brought together leading researchers to discuss immune-related challenges, mechanistic insights, and strategies to enhance the safety and efficacy of AAV-based gene therapies. The presentations covered a broad range of topics, including complement activation, T cell responses, seropositivity challenges, regulatory T cell modulation, and innovations in vector engineering.
Melissa Spencer (UCLA) highlighted that AAV gene therapy delivers viral loads up to 100 million times higher than natural infections, triggering unique innate immune responses. Research in the mdx mouse model demonstrated that redosing leads to treatment rejection, driven by the formation of AAV-antibody immune complexes. These complexes activate complement cascades (C3 consumption) and inflammatory chemokine responses (CXCL10, CCL2, CCL4), which in turn prime the adaptive immune system. Dr. Spencer detailed how antigen-presenting cells, particularly monocytes and plasmacytoid dendritic cells, sense these complexes through Fc receptors to trigger downstream immune activation. 8 These findings underscore the need for improved preclinical models that more accurately reflect human immune responses to guide effective immune modulation strategies.
Roland Herzog (Indiana University) examined CD8+ T cell responses in AAV gene therapy, focusing on the innate immune pathways that drive cytotoxic T cell activation. Multiple redundant innate immune activation pathways, including TLR9, IL-1 signaling, and double-stranded RNA sensing via TLR3, can contribute to CD8+ T cell responses. 9 A key finding was that at high vector doses, multiple immune pathways become active, making immune suppression difficult. In contrast, lower AAV doses show dependence on specific innate immune pathways, which could be more effectively targeted with immune suppression strategies. He also explored vector engineering approaches to minimize CD8+ T cell activation, such as CpG depletion to reduce TLR9 activation and the use of muscle-specific promoters to limit immune activation outside target tissues. Importantly, it was observed that systemic AAV delivery can induce unexpected CD8+ T cell infiltration in the liver, potentially leading to delayed liver toxicity, a finding that has significant implications for AAV safety in clinical applications.
Barbara Sullivan (Ultragenyx) addressed the challenge of seropositivity in AAV gene therapy, emphasizing how pre-existing neutralizing antibodies (NAbs) impact patient eligibility and treatment outcomes. Data from seroprevalence studies show that many patients harbor pre-existing NAbs to AAV, preventing them from receiving gene therapy. A major issue in the field is the lack of standardized thresholds for antibody titers, which complicates eligibility determination for clinical trials. Strategies to overcome seropositivity barriers, include longitudinal retesting to assess sero-reversion and potential immune modulation strategies such as plasmapheresis or B cell depletion. Preclinical data from non-human primate studies demonstrate that low antibody titers may not always prevent liver transduction, whereas high titers lead to rapid vector clearance in the spleen.
Carrie Miceli (UCLA) presented research on innate and adaptive immune memory in DMD and its implications for gene therapy. 10 Using single-cell RNA sequencing, her team analyzed immune cell populations in muscle biopsies from DMD patients pre- and post-gene therapy, identifying clonal expansion of T central memory and effector memory populations. Notably, no common expanded T cell receptor (TCR) clones were found across individuals, suggesting a highly patient-specific immune memory formation. These findings indicate that pre-existing immune memory in muscle may contribute to inflammatory responses following gene therapy, underscoring the importance of immune suppression strategies to improve treatment outcomes.
Nayla Mumneh and Seemin Ahmed (Novartis) provided a clinical perspective on immune-related challenges in AAV gene therapy. They highlighted pre-treatment considerations, including screening for pre-existing antibodies, liver function assessments, and infection monitoring to mitigate adverse immune reactions. Post-treatment monitoring for hepatotoxicity, thrombocytopenia, complement activation, and potential tumorigenicity was emphasized, with an overview of current immunosuppressive regimens used in clinical trials. Additionally, they discussed ongoing efforts to optimize AAV capsid engineering to reduce immunogenicity, off-target effects and improve transduction efficiencies and enhance target-specific gene delivery.
Armando Villalta (UC Irvine) presented novel strategies for modulating regulatory T cells (Tregs) to suppress anti-transgene immune responses against dystrophin in DMD gene therapy. 11 Preclinical studies showed that Treg depletion exacerbates dystrophin-specific immunity, whereas expanding Tregs through IL-2 therapy (or potentially CAR-Tregs) suppresses these responses. His research suggests that Treg expansion strategies could help mitigate immune responses to transgene expression in gene therapy, offering a potential immunomodulatory approach to enhance gene therapy durability and safety, and immune tolerance to dystrophin.
Discussion summary: Immune considerations
The discussion session focused on advancements in single-cell sequencing, immune responses, gene therapy strategies, and biomarker identification in DMD and other neuromuscular diseases.
Biomarker identification and immune profiling
A significant point of discussion was the potential of using peripheral blood signals in addition to muscle biopsies for biomarker identification. The panel emphasized the ongoing search for peripheral markers that could differentiate patients based on their inflammatory profiles, particularly those dominated by complement activation or TNF-gamma signaling. A promising avenue involves correlating serum tenascin C levels with muscle fibroblast activity to identify disease severity and predict therapeutic response.
Inflammation, fibroblasts, and gene therapy response
Panelists examined the role of fibroblast mobilization and inflammatory memory in DMD and other dystrophies. Evidence suggests that chronic inflammation leaves a lasting imprint on the immune response, influencing therapeutic outcomes. Discussions highlighted how altered splicing regulation in an inflammatory environment could create a hostile environment for exon skipping therapies and gene therapy efficacy. Understanding these baseline inflammatory signals is critical for improving patient stratification and managing expectations for therapeutic durability.
Therapeutic strategies and complement pathway inhibition
The session explored therapeutic interventions targeting inflammatory and immune pathways. Blocking complement activation upstream, such as through C3 inhibitors, was suggested as a potential strategy to enhance gene therapy effectiveness. However, concerns were raised regarding the long-term stability of regulatory T cells (Tregs) in immunotherapies, given their potential plasticity and risk of converting into effector cells in an inflammatory environment. The combination of CAR Tregs with IL-2-based stabilization approaches was proposed as a means to enhance efficacy and safety.
Gene therapy delivery and immune risks
Differences in immune responses to intravenous versus intrathecal administration of gene therapy were examined, particularly concerning off-target effects and potential toxicities. The panel debated the risks of high-dose vector administration in the presence of pre-existing antibodies, noting that complement-mediated toxicity could be a limiting factor in dose escalation. Furthermore, liver-mediated immune tolerance in gene therapy was questioned, particularly in the context of ubiquitously expressed promoters such as those used in Zolgensma.
Future directions and cross-disciplinary insights
Looking ahead, a cross-disciplinary approach, incorporating insights from autoimmune diseases, nephrology, and chronic inflammatory disorders, was suggested to help improve understanding of the role of innate immune memory in gene therapy. Key areas for future study include B-cell repertoire analysis to better understand immune priming and response variability. By integrating clinical observations with molecular profiling, the field can move towards more personalized, risk-mitigated treatment protocols.
Cardiac considerations in gene therapy
This session featured presentations on cardiovascular risks associated with gene therapy, focusing on critical insights into mechanisms of cardiac injury, advanced imaging and cardiac function assessments, and therapeutic advancements in gene therapy to address underlying cardiac defects.
Barry Byrne (University of Florida) detailed the cardiac safety profiles of AAV9 and rh74 serotypes, identifying the first two weeks post-infusion as a critical window for innate immune-mediated risk. This period is marked by acute complement activation, macrophage and neutrophil involvement, and the onset of antibody production. He highlighted that endothelial injury can lead to myocardial edema and platelet depletion, noting that vector kinetics differ between serotypes, which directly influences cardiac biodistribution and the subsequent inflammatory response. His presentation underscored the necessity for intensive early monitoring to detect potential cardiac complications with signs of endothelial injury, platelet depletion, and complement activation.
Chet Villa (Cincinnati Children’s Hospital) discussed the natural history of cardiac progression in DMD, emphasizing that myocardial deterioration often precedes functional decline. 12 While traditional measures like systolic function may appear preserved, cardiac MRI (CMR) can reveal significant underlying tissue-level changes, including progressive fibrosis and fat replacement. Dr. Villa presented longitudinal data demonstrating progressive right ventricular and atrial remodeling in DMD patients highlighting that CMR can be an essential tool for tracking disease evolution. These findings reinforce the necessity of early therapeutic intervention to mitigate irreversible myocardial loss.
Jonathan Schwartz (Rocket Pharma) presented Phase 1 results for RPA501, an AAV9-based gene therapy for Danon disease, a monogenic disorder leading to severe hypertrophic cardiomyopathy. 13 Patients treated with RPA501 exhibited improved left ventricular mass, cardiac biomarkers, and overall function. Patients with advanced fibrosis demonstrated limited therapeutic benefit, highlighting the need for precise patient selection. He also detailed the immune-modulatory regimen used to mitigate adverse effects, particularly the thrombotic microangiopathy (TMA) observed in some patients. The presentation emphasized the importance of tailoring immunosuppressive protocols to enhance both safety and efficacy in gene therapy.
Clinical case studies
Three case studies covering fatal or serious adverse events related to gene therapy interventions were presented in this session.
Case 1: Fatal Case Of Gene Therapy for Spinal Muscular Atrophy with Progressive Myoclonic Epilepsy (SMA-PME) presented by Odile Boespflug-Tanguy (Université Paris Cité).
SMA-PME is a rare lysosomal storage disorder affecting the nervous system, caused by mutations in the acid ceramidase (ASAH1) gene. 14 The disease manifests as juvenile-onset muscle weakness resembling SMA Type 2 or 3, followed by severe epilepsy and progressive neurodegeneration. Patients initially retain ambulation but later lose mobility due to myoclonic seizures rather than SMA progression. Most succumb before age 14 due to respiratory complications or status epilepticus. A novel AAV9 gene therapy was developed to deliver the functional ASAH1 gene. The therapy was tested in a 15-year-old female with advanced SMA-PME under compassionate use who had progressive epilepsy, worsening motor function, and mild restrictive respiratory function but normal liver, kidney, and hematologic health. The patient had minimal pre-existing anti-AAV9 antibodies and received prophylactic immunosuppressive therapy (sirolimus and corticosteroids) prior to treatment. However, three days post-infusion, the patient exhibited a drop in platelet count, elevated D-dimers, and signs of systemic inflammation, leading to a cardiogenic shock that was unresponsive to treatment, requiring ECMO support. Despite interventions, the child deteriorated and passed away on day seven post-treatment. Autopsy findings revealed severe vascular leakage, multi-organ failure, and atrial fibrosis, but no myocarditis or microangiopathy. The acute SAE and shortened clinical course prevented efficacy assessment of GNT0009. Small amounts of ACDase protein were observed in the CNS, but at significantly lower levels than in peripheral organs. The case underscores the risks of high-dose systemic AAV9 delivery, the role of pre-existing inflammation in severe adverse reactions, and the need for alternative strategies such as intrathecal administration or CNS-specific vectors.
Case 2: Fatal Recurrent Rhabdomyolysis After Gene Therapy for DMD presented by Kristi Jones (Children’s Hospital at Westmead).
A four-year-old boy with DMD, carrying a de novo exon 45-48 deletion in the dystrophin gene, was enrolled in a clinical trial for AAV-mediated micro-dystrophin gene therapy. His early symptoms included intermittent limping/leg pain after strenuous exercise, difficulty rising from floor with Gowers’, unable to run or climb, and a persistently elevated creatine kinase (CK) level above 10,000 U/L. Despite his genetic deletion being in-frame (suggesting a Becker-like phenotype), he exhibited a Duchenne-like clinical presentation. His pre-treatment muscle biopsy showed significant endogenous dystrophin expression (25-50% of normal levels), which was unexpected for his genotype. Following gene therapy infusion at the standard 2 × 1014 vector genomes per kg dose, he showed initial improvement in motor skills, becoming Gowers’ negative. However, seven weeks post-treatment, he developed severe pain, dark urine (myoglobinuria), and CK elevation to 125,000 U/L, consistent with rhabdomyolysis. This episode resolved with IV fluids, corticosteroids, and analgesia, but over 14 months, he suffered 17 recurrent episodes. Despite treatment with a range of immune modulators (sirolimus, rituximab and IVIG), he only responded to pulse corticosteroids. Extensive investigations—including genetic, immunological, metabolic, and histopathological studies—failed to identify a clear trigger or etiology. Anti-dystrophin antibodies were only mildly elevated, and immune profiling did not show a significant T-cell response to transgene dystrophin. Muscle biopsies taken between episodes and during crises showed minimal inflammation, questioning an immune-mediated etiology. During the 17th episode, he suffered sudden hyperkalemia-induced cardiac arrest, despite having normal or low potassium levels in prior episodes. Post-mortem analysis revealed widespread patchy necrotizing myopathy across multiple muscle groups, showing evidence of temporal heterogeneity with a mix of both recent and older foci of muscle damage but no significant cardiac or renal pathology. His case may suggest a novel interaction between endogenous and transgene dystrophin, leading to focal membrane instability and progressive myopathy. Future gene therapy trials may need to consider endogenous dystrophin levels as a potential risk factor.
Case 3: Severe Infusion Reactions in Twins with Spinal Muscular Atrophy (SMA) and High Anti-AAV9 Antibodies presented by Peter Kang (University of Minnesota).
Fraternal twin boys diagnosed with SMA (0 copies of SMN1, 3 copies of SMN2) were potentially eligible for AAV9-mediated SMN1 gene therapy but were found to have high pre-existing anti-AAV9 antibodies, making standard treatment unsafe. As they were approaching their second birthday, a regimen of plasmapheresis (11 exchanges per twin), rituximab (B-cell depletion), and immunosuppressive therapy was implemented to lower anti-AAV9 antibody titers. After successful reduction of antibody levels, both twins received intravenous AAV9 gene therapy. However, severe infusion reactions developed approximately 10 minutes after initiation. Both twins experienced urticaria, wheezing, and dry heaving/emesis. The infusions were stopped. The patients recovered but received only a fraction of the intended dose of gene therapy. This recently published case highlights the risks posed by high pre-existing AAV9 antibodies, even when antibody titers are medically lowered. 15 Of note, the plasmapheresis circuit priming utilized IVIG which can be positive for anti-AAV antibodies and may have contributed to the observed infusion reaction. These findings underscore the need to develop improved immune evasion strategies and alternative delivery methods, such as vector engineering and non-viral gene delivery vehicles, to optimize the safety of gene therapy in patients with pre-existing immunity.
Discussion summary: Immunosuppression and surveillance
This discussion session covered a broad spectrum of topics, including laboratory monitoring, autopsy protocols, gene therapy considerations, long-term patient outcomes, regulatory challenges, and data-sharing efforts. A primary focus was on laboratory markers for complement activation, including TNM, C5B9, C3, C4, and schistocytes, which serve as critical indicators of immune activity. Factor H and Factor I were also discussed as potential markers of immune recovery, though their clinical accessibility remains limited outside of research settings.
Autopsy and tissue collection protocols were another major point of discussion, highlighting the necessity of establishing clear guidelines and engaging cooperative pathologists. The initial focus on cardiac and pulmonary tissues has expanded to include neurological and gastrointestinal samples, as well as investigations into bladder pathology due to emerging retention issues in young adults. The process of acquiring biobanked tissue for research has proven bureaucratically complex, with institutional hesitation in releasing preserved samples. Early engagement with biobank and pathology teams was recommended to prevent delays in accessing critical research materials.
Gene therapy considerations, informed by Rocket Pharmaceuticals’ RPA501 experience, particularly in relation to promoter selection, tissue targeting and study design, were also explored. The use of a ubiquitous promoter, such as CMV enhancer with CBA, was initially chosen due to the systemic nature of the disease under investigation. However, clinical and regulatory priorities, particularly FDA emphasis within early-phase development, established a clear directive to prioritize cardiac outcomes while including assessments of skeletal muscle and neurological function. In regard to study design, the RPA501 experience underscored practical limitations of intensive tissue sampling strategies in both trials and long-term follow-up. While skeletal muscle biopsies were included to support mechanistic understanding, they were consistently found to be poorly tolerated by patients and difficult to implement as a routine, protocol-driven assessment. Initial findings from skeletal muscle biopsies were largely negative, but assay evolution and patient reluctance to undergo repeated biopsies necessitate a selective approach towards establishing long-term follow-up protocols.
The long-term monitoring of the Phase 1 patients suggested meaningful improvements in quality-of-life, with individuals engaging in independent living, full-time schooling, and even sports activities. While these successes are promising, they remain largely anecdotal and underscore the need for more structured and quantitative long-term assessments, particularly in neurocognitive and neuromuscular domains to accurately characterize durability of benefit and functional impact over time. The challenges of demonstrating conclusive efficacy in clinical trials were also discussed, particularly in the context of cardiac MRI-based biomarkers. Regulatory bodies such as the FDA have evolved in their stance on cardiac biomarkers but continue to pose challenges in establishing suitable endpoints beyond major adverse cardiac events (MACE), which are not practical in rare disease trials.
Data sharing and institutional collaboration were recognized as critical yet challenging endeavors. Despite IRB approvals, legal and institutional barriers have impeded efforts to share clinical imaging data, underscoring the need for a robust, standardized data-sharing framework. Ongoing initiatives, including the creation of an imaging biorepository and harmonization of myocardial injury response protocols, were highlighted as essential steps toward improving research efficiency.
Lastly, concerns regarding immunogenicity in gene therapy were raised, particularly in seropositive patients. The threshold for preexisting antibodies remains an open question, with cases suggesting that a prior asymptomatic infection may influence immune response post-therapy. Further investigations into B-cell receptor profiling may provide insights into underlying susceptibility factors. Collaboration with industry partners and regulatory agencies will be essential in refining eligibility criteria and optimizing immune management strategies.
Overall, the discussion emphasized the need for interdisciplinary collaboration, proactive planning for research logistics, and continued efforts to refine clinical trial methodologies in the context of immunosuppression and gene therapy surveillance.
PPMD-MDA collaborative effort on best practices for gene therapy administration
A collaborative initiative between Parent Project Muscular Dystrophy (PPMD) and the Muscular Dystrophy Association (MDA) convened a dedicated workgroup to establish best practices for the clinical administration of gene therapy in Duchenne muscular dystrophy (DMD). This effort was prompted by the expanded label and accelerated approval of Elevidys, which necessitates standardization to minimize variability in clinical practices across institutions administering gene therapy. The primary objective was to create a standardized framework to ensure institutional readiness, rigorous patient selection, and comprehensive safety monitoring. An open call invited expert clinicians and representatives from existing workgroups to participate in a series of six weekly meetings. The workgroups engaged in in-depth discussions covering multiple aspects of gene therapy dosing, gathering clinical protocols from various institutions, and synthesizing them into a cohesive set of best practices. A consensus document was published to guide both clinicians and patients on several key areas of gene therapy administration including: a) Institutional readiness; b) Patient selection and eligibility; c) Pre-dosing considerations; d) Dosing day protocol; e) Post-infusion and long term monitoring. 3
By addressing variability in clinical practice and institutional readiness, these published guidelines aim to improve therapeutic outcomes, safeguard patient health, and promote equitable access to treatment. This collaborative effort serves as a foundational framework that will continue to evolve alongside the gene therapy landscape to optimize patient care.
Concluding remarks
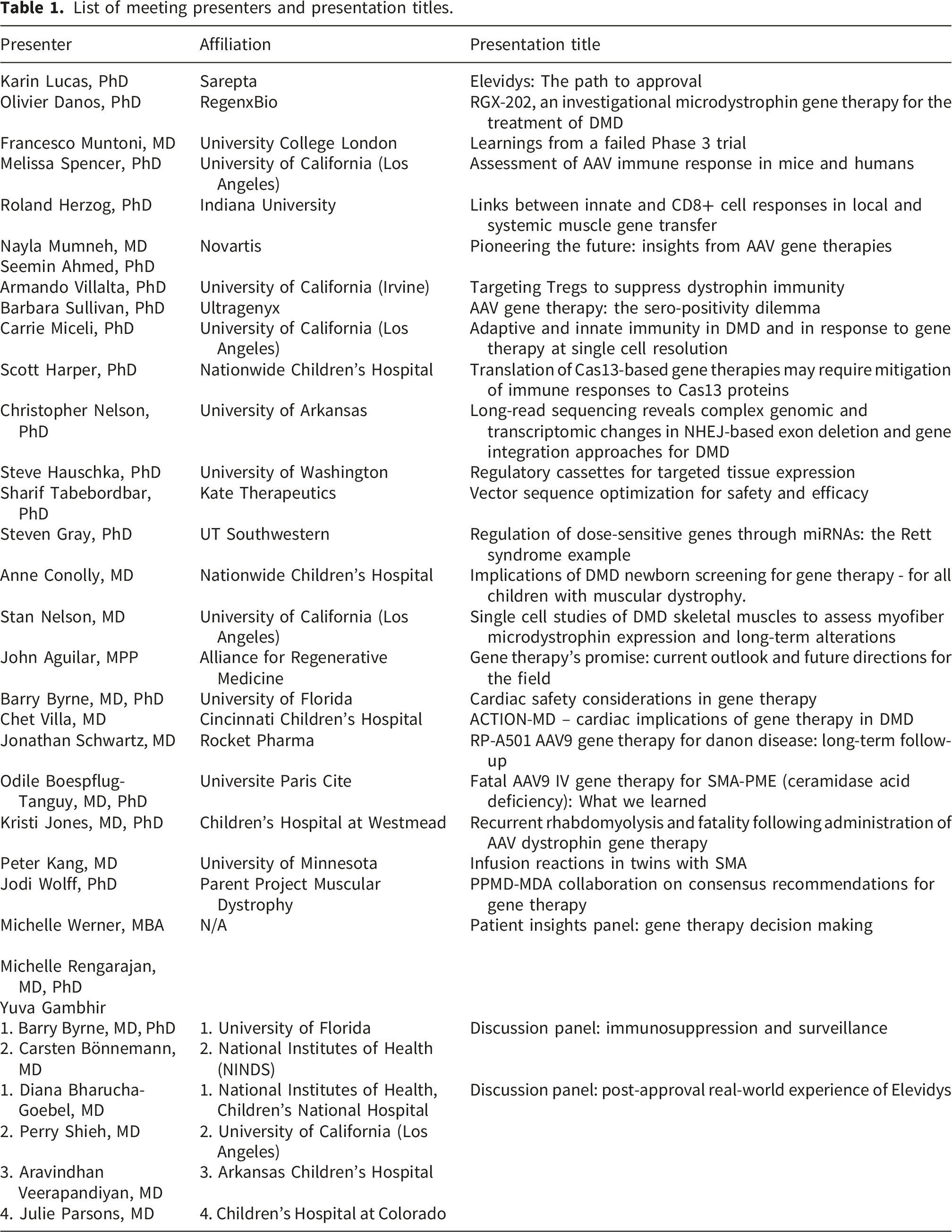
List of meeting presenters and presentation titles.
Key sessions emphasized the need for rigorous, well-powered clinical trials with standardized endpoints, longitudinal follow-up, and robust biomarker strategies to assess therapeutic efficacy and safety over time. Presentations highlighted the significance of patient-specific variables, such as age, genotype, and immune status in influencing therapeutic outcomes, underscoring the necessity for refined stratification strategies in trial design. While immune-mediated complications remain central barriers, advancements in capsid engineering and immune modulation strategies, including regulatory T cell enhancement offer a promising roadmap for a future with safer and potentially enabling re-dosing of AAV vectors.
The real-world implementation of therapies like Elevidys into clinical practice has exposed systemic challenges around institutional readiness, payer systems, adverse event surveillance, and ethical considerations, but also provide unique opportunities to study the impact of gene therapy in much larger cohorts. This evolution of gene therapy entering clinical care is supported by consensus-driven guidelines such as the PPMD-MDA collaborative effort in outlining best practices. Patient and caregiver panels further emphasized the importance of transparent and accessible data, equitable trial inclusion, and outcome measures that reflect real-world concerns, including quality of life and long-term functional capacity. Taken together, the discussions at this summit reinforce the imperative for continued cross-disciplinary collaboration, integration of real-world evidence, and harmonization of regulatory and clinical approaches to advance the field toward durable, equitable, and patient-centered gene therapy solutions for neuromuscular disease.
Footnotes
Acknowledgements
The Muscular Dystrophy Association would like to acknowledge Affinia Therapeutics, Askbio, Astellas, Benitec Biopharma, Insmed, Lexeo Therapeutics, ML Bio Solutions, Novartis, Pfizer, RegenxBio, Sarepta Therapeutics and Solid Biosciences for contributing to the meeting sponsorship.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.