
Abstract
Fungal keratitis is a sight-threatening corneal infection affecting over a million people annually. Natamycin, a polyene extracted from Streptomyces natalensis, remains the only FDA-approved drug for the treatment of fungal keratitis. The conventional treatment involves a 5% ophthalmic natamycin solution, administered at a high frequency during the initial treatment phase and subsequently tapered based on the observed clinical response. Although it demonstrates a broad spectrum of activity, its efficacy is hindered by limited corneal penetration due to its high molecular weight and low aqueous solubility.
This review consolidates current knowledge on fungal keratitis, including prevalence, risk factors, and etiology. It provides a comprehensive evaluation of natamycin, covering its pharmacology, mechanism of action, antifungal spectrum, and clinical applications while addressing the limitations of conventional natamycin therapy and ocular barriers that restrict drug delivery. Furthermore, the review highlights recent advances in both nanotechnology-based and non-nanotechnology-based natamycin delivery strategies to enhance corneal bioavailability.
Despite promising preclinical outcomes in terms of bioavailability and retention, no alternative natamycin formulations have yet progressed to clinical trials or commercialization. Further efforts are required to advance these delivery systems into clinical trials and realize their potential to improve outcomes in fungal keratitis.
Keywords
Introduction
Natamycin, the only Food and Drug Administration (FDA) approved antifungal agent for the treatment of fungal keratitis, belongs to the polyene class and exhibits broad-spectrum antifungal activity.1–3 It acts by inhibiting glucose and amino acid transport across the plasma membrane, thereby selectively and temporarily inhibiting membrane transport proteins specific to ergosterol, ultimately causing fungal cell death. 4
Fungal keratitis, also called keratomycosis, oculomycosis, or mycotic keratitis, is a corneal infection caused by a wide range of fungi. Fungi can infiltrate deeper into the stroma and Descemet’s membrane of the cornea. Healing of the ulcer can cause corneal scarring, which may necessitate corneal transplantation. 5 If left untreated, it can cause corneal perforation, leading to panophthalmitis or orbital cellulitis, which in turn may lead to meningitis and death. Globally, more than a million people develop fungal keratitis, with 8%–11% requiring the removal of the eye, leading to blindness. 6
Natamycin is marketed as an ophthalmic product at 5% (50 mg/mL). It is frequently sold under the brand name Natacyn→ (US FDA-approved, manufactured by Alcon Laboratories), while various formulations, such as Natamet (manufactured by Sun Pharma, India) and Natasol (a water-soluble formulation), have been documented in the literature. Typically, it is administered at a rate of one drop every hour or two. After the initial 3–4 days, the frequency of administration is subsequently decreased to one drop every 3–4 hours, based on the clinical response. This continues till the wound is fully healed. Even when keratitis is clinically resolved, topical medication is suggested for at least 4 weeks, to be administered at a frequency of four times a day. 4 Natamycin is the preferred treatment for filamentous keratitis, particularly for Fusarium species. Natamycin has fewer side effects, lower rates of resistance, and less harmful effects when compared to amphotericin B and azoles. 7 However, its use in deep stromal keratitis is constrained by its weak corneal stromal penetration, necessitating combination therapy in severe cases. 5
This review provides an overview of current knowledge on natamycin, including its chemistry and mechanism of action, as well as a few reports of comparative clinical research comparing natamycin with other antifungals, which demonstrate its greater effectiveness in treating fungal keratitis. It further discusses the key challenges limiting its therapeutic efficacy and examines the formulation strategies developed to overcome these barriers. Finally, the review highlights existing gaps in the ocular delivery of natamycin and its clinical translation. It outlines future avenues for research and development toward a more effective, patient-friendly therapy.
Methods
Using pertinent terms such as “natamycin,” “ocular delivery,” “fungal keratitis,” and “natamycin drug delivery systems,” a search was performed on PubMed, Scopus, and Google Scholar. Several clinical trials, comparative studies, experimental studies, and review papers were found through the search. Studies that particularly address natamycin’s pharmacological properties, clinical uses in fungal keratitis, comparative efficacy with other antifungal drugs, or innovative ocular administration techniques designed to improve its therapeutic efficiency were included. Articles without experimental or clinical data or those that are not explicitly related to ocular drug delivery are excluded. The selected literature was combined to provide a comprehensive narrative overview of current understanding and developments in the management of fungal keratitis with natamycin.
Fungal Keratitis: Prevalence, Risk Factors, and Etiology
It is estimated that there are 1,051,787 incidences of fungal keratitis worldwide each year, with Asia (939,859) and Africa (75,196) having the highest estimated incidences, while Europe (99) has the lowest. 6 According to the 2024 global epidemiological review, 8%–16% of all culture-positive infectious keratitis cases globally are caused by fungal keratitis, with 90% of cases occurring in tropical and subtropical countries, 8 which may be primarily associated with the climate (high temperature and relative humidity) and any ocular trauma related to agricultural activities. 9
The highest reported incidence worldwide is 73 per 100,000 in Nepal. 10 Over 10 years and 5 months, 1,360 patients with culture-proven mycotic keratitis were seen at a single hospital in Hyderabad, India. 11 In comparison, over 6 years, 654 patients with a similar condition were seen at another institution in Northern China. 11 According to Gonzales et al., the Madurai district of South India had an annual incidence of corneal ulceration of 113 per 100,000 individuals, which was 10 times higher than that in Olmsted County, Minnesota, in the United States.12,13 Among 110 patients with culture-positive microbial keratitis, a 12-year review in South Korea (2011–2022) identified 32 cases of fungal keratitis. 14 A national report from Iraq estimated the incidence of fungal keratitis at 14 per 100,000 people, indicating a persistent regional burden. 15
The Swiss cohort (2012–2023) reported 206 confirmed cases of fungal keratitis, caused mainly by Candida spp. 16 According to a 2021–2025 Italian tertiary-center assessment, 13% of all cases of microbial keratitis were fungal keratitis (29/221). 17 A 9-hospital Spanish series (2010–2022) identified 77 cases of fungal keratitis; the main risk factors were prior corticosteroid use, keratoplasty, and trauma. 18 A 20-year Canadian multi-center study (2003–2022) documented 138 cases. 19 Throughout the course of eight and sixteen years, respectively, mycotic keratitis was reported in just 56 patients in Melbourne, Australia, and 61 eyes (57 individuals) in New York, USA.20,21
The most prevalent external cause of fungal keratitis is the traumatic entry of fungal components or spores into the outer corneal layers. About 55%–65% of all cases of fungal keratitis are caused by trauma involving vegetative sources.22,23 Particularly in developed nations, the growing use of contact lenses (CL) in recent years has been a significant contributing cause to the occurrence of fungal keratitis. The use of topical drugs, such as corticosteroids, the presence of underlying ocular diseases, keratopathy, and previous eye surgery, are other related ocular factors. Immunosuppression and diabetes mellitus are examples of systemic risk factors. 24
Yeasts are more prevalent in developed nations and have been linked to immunocompromised individuals, while in developing countries, filamentous fungi are the primary etiological agents and are frequently related to vegetative matter trauma. Most fungi associated with keratitis are saprophytic. Aspergillus, Fusarium, Candida, Curvularia, and Penicillium are common pathogenic species; the most common ones are Fusarium (37%–62%) and Aspergillus (24%–30%). A total of 154 fungal species/genera were identified across 61 countries in the first-ever worldwide prevalence assessment of fungal keratitis caused by rare species from January 1963 to March 2023. India reported the highest number of instances, taxa, and species, whereas Australia had the highest pooled prevalence. 25 According to Prajna et al., Aspergillus, Fusarium, and Curvularia species are the most common etiologies from northern and eastern India, while Fusarium species are the most common organisms in the western and southern parts of the country.23,26 According to a recent tertiary-center study from Eastern China (2021–2024), trauma was the leading risk factor, and Fusarium was responsible for 49% of 174 confirmed cases. 27 A retrospective analysis of 68 confirmed cases over 17 years from two Western Australian tertiary institutions found that prior corticosteroid use was a significant risk factor, with Fusarium (37%) and Candida (28%) predominating.28,29
It is crucial to understand the epidemiology and organisms of fungal keratitis to emphasize the urgent need for potent antifungal medications for the eyes.
Natamycin: An Antifungal Drug
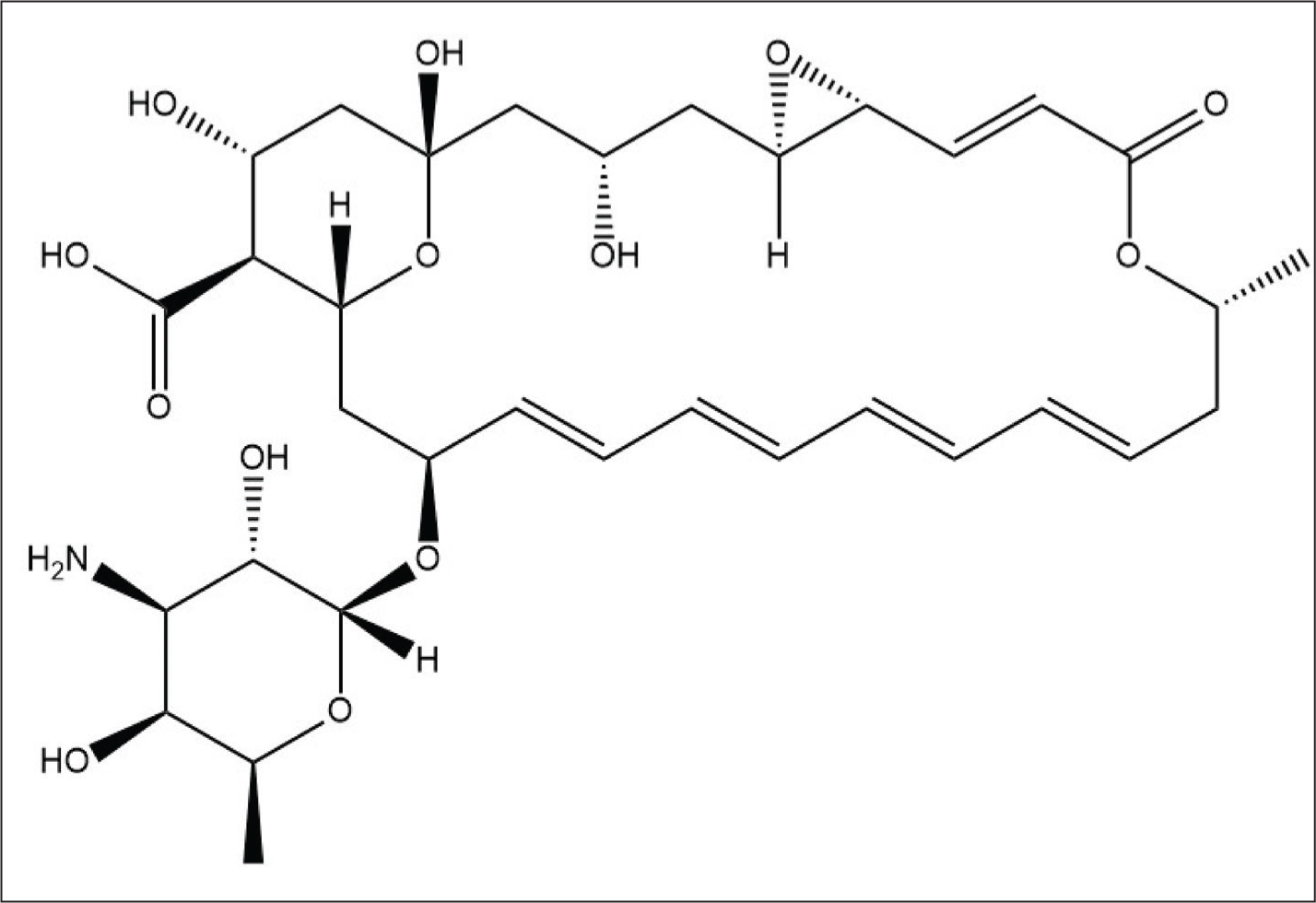
Natamycin was initially isolated in 1955 from a fermented broth of a soil sample of Streptomyces natalensis from South Africa by the Netherlands’ Gist-brocades Research Laboratories.30,31 For industrial production, Streptomyces gilvosporeus and S. natalensis are employed in fermentation. 32 The isolated compound was called pimaricin and later renamed Natamycin by the World Health Organization (WHO), which requires antibiotics produced by Streptomyces to end in “-mycin.” This is because they wanted the product’s name to reflect the organism that made it. Natamycin, which means “obtained from Streptomyces natalensis,” replaced pimaricin as the new name. 33 It is a polyene with a molecular weight of 665.75 g/mol and has an empirical formula C33H47NO13 (Figure 1). According to the Biopharmaceutics Classification System (BCS), natamycin is classified as a Class IV drug, characterized by low solubility and permeability.
Structure of Natamycin (Created with ChemDraw).
Polyenes bind directly to ergosterol in the fungal cell membrane, causing membrane dysfunction that may involve pore formation (e.g., amphotericin B) or inhibition of ergosterol-dependent membrane processes (e.g., natamycin). Azoles and allylamines inhibit key enzymes in the ergosterol biosynthesis pathway (lanosterol 14-α-demethylase and squalene epoxidase, respectively), leading to reduced ergosterol levels and impaired membrane integrity. 34 Echinocandins, on the other hand, block β-(1,3)-D-glucan synthase, a key enzyme in the fungal cell wall (Figure 2).35,36 Natamycin is primarily fungistatic and acts by selectively binding to ergosterol, without forming pores in the fungal membrane, unlike other polyene antifungal drugs, which are fungicidal by forming pores. Ergosterol binding disrupts membrane integrity and interferes with essential membrane-associated functions, such as endocytosis, exocytosis, and vacuolar fusion, thereby inhibiting fungal cell growth with minimal membrane permeabilization.37–41 Molecular simulation studies by Szomek et al. reported that natamycin preferentially aggregates in ergosterol-rich membranes, forming a complex, which significantly disrupts membrane integrity. In parallel, natamycin markedly reduces the activity of the ergosterol-dependent lysine transporter Lyp1, suggesting that ergosterol sequestration impairs essential cellular transport. 42 Transcriptomic findings by Welscher et al. further demonstrated that natamycin reduces arginine uptake at amounts that impede cell development without causing cell death. They also showed that the addition of natamycin totally prevented the uptake of proline and glucose. 43 Recent mechanistic advances have revealed that natamycin binds to the fungal plasma membrane in a purely sterol-dependent manner, with a significantly higher affinity for ergosterol than for cholesterol. This explains the selective binding of natamycin to yeast cells, rather than to mammalian cells that contain cholesterol. After binding, natamycin forms nanoclusters within the membrane, inducing significant membrane distortion, increasing permeability to small cations, such as propidium iodide, by lowering the membrane dipole potential without creating ion pores. 44 A 2025 study found that natamycin directly binds to the fungal sterol-regulatory transcription factor FfSR, preventing its liquid-liquid phase separation. This interference suppresses ergosterol production at the transcriptional level by preventing the development of transcriptional condensates necessary for ERG gene activation. 45 This affects fungal cell proliferation, thereby exerting antifungal activity.
Mechanism of Action of Natamycin, Amphotericin B, Azoles, Echinocandins, and Allylamines (Created in https://BioRender.com ).

Natamycin exhibits antifungal efficacy against both filamentous and non-filamentous fungal species and has a higher and more pronounced effect on filamentous types than the non-filamentous ones. 46 According to one meta-analysis, natamycin was particularly effective in treating early-stage Fusarium keratitis compared to other antifungals. 47 The size of the inhibition zones in natamycin susceptibility tests and clinical outcomes were significantly correlated in a Chinese study of 525 patients, of whom 19.25% tested positive for Fusarium. 48 Higher cure rates and lower evisceration rates were associated with larger inhibition zones. Although isolates are susceptible in vitro, natamycin monotherapy may not be effective in a substantial proportion of Fusarium patients. In one study, although Fusarium isolates were sensitive to natamycin, 46.6% of cases required keratoplasty, regardless of when they were presented. 49 12.8% of patients treated with natamycin in the Mycotic Ulcer Treatment Trial I either needed therapeutic keratoplasty or advanced perforation.3,50
Natamycin Versus Other Antifungals
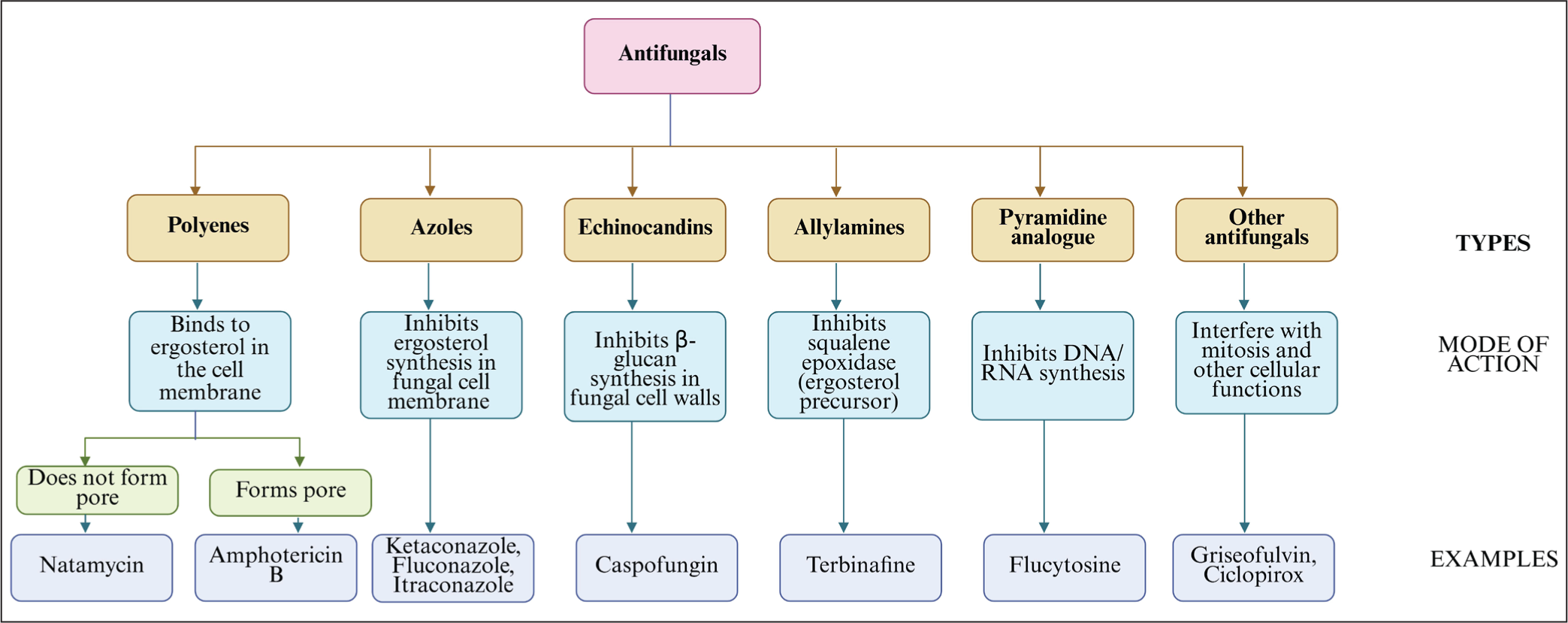
A variety of antifungal drugs, classified into different groups (Figure 3), have been used to treat fungal keratitis. Natamycin (5%), voriconazole (1%–2%), and amphotericin B (0.15%–0.3%) are frequently used topical agents, particularly as first-line therapy. Apart from these, topical ketoconazole (1%–2%), itraconazole (1%), fluconazole (1%), econazole (1%), miconazole (1%), clotrimazole (1%), flucytosine (1%), and caspofungin (0.5%) are also used. In some cases, subconjunctival miconazole (10 mg in 0.5 mL), fluconazole (0.5–1.0 mL of a 2% solution), intravenous miconazole or amphotericin B (600–1200 mg/day), oral ketoconazole (200–600 mg), itraconazole (100–200 mg), fluconazole (50–200 mg), or voriconazole (400 mg) per day are also advised. In severe or refractory cases, 5 mg of amphotericin B and voriconazole are injected intrastromally.51–55 Comparative data, however, show that only a few antifungal medications consistently offer therapeutic efficacy in clinical settings (Table 1).
Classification of Antifungal Agents (Created in https://BioRender.com ).
Studies Comparing the Efficacy of Natamycin and Other Antifungal Agents in the Treatment of Fungal Keratitis.


Prajna et al. conducted a randomized controlled trial (RCT) to evaluate the effect of topical natamycin and topical econazole, finding that natamycin was as effective as econazole in improving vision in cases of Fusarium keratitis. 56 Kalavathy et al. compared the healing effect of topical natamycin vs. topical itraconazole against Fusarium and Aspergillus species. The healing rate was better with natamycin for Fusarium, but there was no difference in healing against Aspergillus and Curvularia. 57 Another study compared the effect of topical voriconazole 1% and topical natamycin 5%. The clinical outcomes, including visual acuity, scar size, and perforations, did not differ significantly among the study groups. 58 Arora et al. did a similar study and concluded that both topical voriconazole and natamycin are equally efficient in treating fungal keratitis. 59 Although it shows similar effectiveness against non-Fusarium infections, voriconazole is not as suitable as a primary treatment due to its higher cost, instability in suspension, and limited commercial availability.
A recent case study of Curvularia geniculata keratitis demonstrated that patients treated with natamycin monotherapy and another patient who received combination therapy of topical natamycin and voriconazole experienced complete recovery and outstanding visual results. 60 Another study compared the efficacy of topical natamycin (5%) or Natasol (1%) with a combination therapy of natamycin (5%) and voriconazole (1%) in patients with mild to moderate fungal keratitis. The Natasol group had a trend of early reepithelialization, and all groups showed comparable improvement in corrected distance visual acuity. 61
The Mycotic Topical Treatment Trial I, conducted by Prajna et al. in 2013, showed that natamycin yielded better clinical outcomes against filamentous fungi, especially Fusarium. The perforation of the cornea in the natamycin-treated group compared to the voriconazole-treated group was less. The need for therapeutic keratoplasty was also less in the natamycin-treated group. 3 This RCT remains the most compelling data supporting natamycin’s higher efficacy, especially against Fusarium. Topical natamycin and oral ketoconazole both showed statistically similar effects in treating the ulcer features. There was no statistically significant difference in baseline features or the rate of healing between the two groups. 62 The natamycin-treated group showed better vision in Fusarium-infected patients compared to the voriconazole-treated group in another study by Sharma et al. 63
Intrastromal natamycin treatment is more effective than topical treatment, primarily because it delivers the drug directly to the site of infection, reducing the difficulty of natamycin reaching the infection. Intrastromal natamycin showed better healing compared to intrastromal voriconazole and intrastromal amphotericin B in recalcitrant fungal keratitis. 64 However, routine use of intrastromal injections in primary care settings is limited due to their invasiveness and need for surgical expertise.
In a study on Candida keratitis corneal isolates by Spierer et al., amphotericin B (0.2%) and natamycin (5%) showed equal efficacy with a total (100%) growth inhibition. An overall inhibition rate of 85% was demonstrated with voriconazole 1%, with 77% inhibition against Candida albicans and 93% against non-albicans species. However, fluconazole 0.2% was an unsatisfactory option for treating fungal keratitis due to its weak antifungal efficacy. 1 In a rabbit model study of Aspergillus keratitis, both micafungin 150 μg and natamycin 5% effectively reduced epithelial defect, infiltration size, and hypopyon. Micafungin showed a greater reduction in hypopyon height than natamycin, but there was no statistically significant difference in lesion size between the two groups. 65
It is crucial to note that many comparison studies have small sample sizes and regional biases, which may limit the broad applicability of their results. These clinical studies collectively suggest that natamycin is the most reliable and well-established first-line treatment for filamentous keratitis, particularly for Fusarium infections.
Antifungal Activity of Natamycin
MIC has become a crucial tool for guiding successful treatment of fungal keratitis, as antifungal resistance continues to increase and new antifungal drugs are developed. MIC is the lowest drug concentration that, after a specific incubation period, inhibits visible fungal growth. 66
According to a previous study, natamycin has shown varied MICs for Candida, ranging from 1 to 2 μg/mL against C. albicans and 150 μg/mL against C. parasilopsis.67–69 While the MIC of natamycin was reported to be 4–8 μg/mL against 20 Fusarium strains, that of amphotericin B and voriconazole varies from 0.5 to >16 μg/mL and 2–16 μg/mL, respectively, according to an in vitro antifungal activity investigation by Cordoba et al. against 29 Fusarium isolates.70,71 MICs of amphotericin B and voriconazole were found to be 0.5–4 μg/mL and 0.125–2 μg/mL, respectively, in a comparable investigation conducted by Arkin et al. against 82 Aspergillus spp., whereas natamycin showed a MIC range of 5–40 μg/mL against 191 spp. of Aspergillus.72,73 Natamycin has demonstrated sporicidal action against a small number of Fusarium and Aspergillus fungal spores. 74
Approximately 600 fungal isolates from corneas and CL were examined in a larger retrospective epidemiological investigation conducted at the UK National Mycology Reference Laboratory. MICs for natamycin, voriconazole, econazole, posaconazole, itraconazole, amphotericin B, and voriconazole were tested. For Fusarium spp., all isolates (100%) were susceptible, with a modal MIC of 4 mg/L. In comparison, only 60% of the isolates were sensitive to voriconazole, and nearly two-thirds were sensitive to amphotericin B, despite the lower median MICs of these drugs. In contrast, natamycin displayed lesser activity against Aspergillus spp., with only 74% of isolates being sensitive, and MICs were higher (often ≥4 mg/L). In comparison, voriconazole and amphotericin had significantly superior activity, with 100% and 96% susceptibility, respectively, and lower MICs (approximately 0.25–0.5 mg/L). Candida isolates were susceptible to natamycin, voriconazole, and amphotericin B, with natamycin maintaining full activity despite higher MICs than those of the azoles. The authors concluded that natamycin is the most effective first-line treatment for Fusarium-dominated fungal keratitis; however, if Aspergillus is found, treatment should be changed to or combined with voriconazole (or amphotericin B), as these drugs are more effective against Aspergillus in vitro. 75
A study was conducted by Streekstra et al. to track and assess the emergence of antifungal resistance against natamycin. 76 Twenty distinct strains were chosen, including species that cause ocular infections, such as A. terreus, A. fumigatus, F. solani, F. oxysporum, C. parapsilosis, C. albicans, and C. krusei. A little statistically insignificant rise in MIC (1.2–12.8 μg/mL vs. 1.2–13.2 μg/mL) was noted after extended exposure to natamycin. An increase in MIC was noted for Aspergillus and Candida species, but not for Fusarium species.67,76–79 The majority of filamentous fungi, including Fusarium and some strains of Aspergillus, exhibit susceptibility and no development of resistance to natamycin. Only a small number of strains are inherently less sensitive to it. This low propensity to develop resistance is a significant advantage for natamycin compared to triazoles, which are facing increasing resistance.
Challenges Associated with Natamycin Therapy
Physicochemical Limitations
Natamycin exhibits several physicochemical limitations that significantly limit its ocular delivery and therapeutic efficacy. Its permeability coefficient (Papp) is 7.28×10–2 cm/h, and log P varies between –3.5 and –1.7, indicating suboptimal lipophilicity for corneal penetration. The low transcellular permeability of natamycin is caused by a high polar surface area (231 Å), seven hydrogen bond donors, and 13 hydrogen bond acceptors.80–82 Structurally, natamycin is a tetraene, where the four conjugated double bonds form a chromophore, which is associated with the 25-carbon lactone ring. The hydroxylated backbone confers hydrophilicity to the molecule, while the four conjugated double bonds in the lactone central core impart lipophilicity. Natamycin contains one basic (mycosamine) and one acidic (carboxylic) group, conferring amphoteric and zwitterionic properties. Unsaturated tetraene chromophore contributes to natamycin’s aqueous insolubility, while hydroxyl and zwitterionic carboxyl groups help explain its relative insolubility in organic solvents. 83 With pKa values of ~4–4.5 (carboxyl) and ~8.6 (amine), its isoelectric point is ~6.5, and it remains electrophoretically neutral between pH 5–9.81,83 Although it promotes broad-spectrum antifungal activity, this dual charge state restricts passive diffusion across the corneal epithelium.
Because natamycin is poorly soluble in water and most organic solvents, its formulation diversity is limited. The hydrophobic region promotes aggregation and adds to instability in aqueous suspension. In neutral conditions, thermal and pH stability are favorable, maintaining 92.2% after 14 days in darkness at 4°C and withstanding temperatures of up to 50°C for several days or sterilization at 116°C for 30 minutes with minimal loss. However, rapid hydrolysis occurs at pH levels below 3 (mycosamine cleavage) or above 9 (lactone saponification into inactive natamycoic acid), resulting in instability and decreased antifungal efficacy and activity.32,84,85
Furthermore, natamycin is prone to photo-oxidation and photo-degradation via cleavage of the chromophore upon light absorption; therefore, solutions should be kept in the dark. 68 According to Velpandian et al., natamycin’s poor photostability in typical ophthalmic conditions was confirmed by a ~15% decrease in active content by day 15 and total degradation by day 30 when exposed to fluorescent light (500 lux). 86 This highlights natamycin’s susceptibility to environmental conditions, underscoring the need for protected storage and advanced stabilizers to ensure reliable ophthalmic shelf life and effectiveness.
Due to its poor solubility and instability, natamycin is only available as an aqueous suspension, not as a solution, but suspensions are susceptible to microbial contamination and sedimentation, which can result in inconsistent dosing, reduced shelf life, and reduced therapeutic consistency. 87
Clinically, natamycin shows poor ocular retention, with only ~5% of the medication reaching the desired ocular region.88,89 To achieve therapeutic concentrations within the infected tissue, a prolonged therapy duration of 4–6 weeks is necessary. This is accomplished by high-frequency administration. 90
Patient-centric Limitations
The success of the treatment largely depends on patient adherence. Patients are subjected to a significant practical and economic burden during the treatment, which involves hourly instillation during the intense phase and protracted tapering over weeks. Hence, they must deliver 12–24 doses daily, which is challenging without a caregiver’s assistance. Since most patients are elderly, their low vision and lack of dexterity lead to skipping doses, resulting in less-than-ideal drug exposure and worse clinical outcomes.91,92 In resource-constrained homes, maintaining proper sterile conditions and storage is challenging, which raises the risk of contamination. Furthermore, frequent dosing requires several bottles of natamycin, which cost around $106.40 per bottle ($140 in Peru, $4 in Indonesia, and £330 in the UK), thereby increasing treatment costs. 93 Low-income and rural communities are disproportionately affected by this burden. The necessity to travel for regular follow-ups, multiple concurrent medications, and difficulty maintaining the dosage while working further reduces compliance.93–95
Natamycin is not easily accessible in several sub-Saharan African countries or in Europe (including the United Kingdom), despite being the only topical ophthalmic antifungal listed on the 22nd WHO Model List of Essential Medicines (2021).96–98 A global assessment by Global Action Fund for Fungal Infections (GAFFI) reported that natamycin is not readily available in Nepal, Ecuador, Chile, and Madagascar. It must be specially imported into the Philippines and Denmark. In several low- and middle-income countries, natamycin ophthalmic products are not locally registered. 99 In several other countries, natamycin is authorized and used as a food preservative; however, there is no equivalent authorization for ophthalmic use, which limits clinical access to eye-drop formulations (Table 2). These regulatory and supply barriers have clinical implications, including the need for compounded alternatives, delays in receiving the proper treatment, and a higher risk of poor visual outcomes.100,101

These physicochemical limitations, along with real-world challenges, underscore the urgent need for advanced formulation strategies that can overcome solubility and stability limitations, thereby reducing the need for frequent dosing.
Ocular Barriers
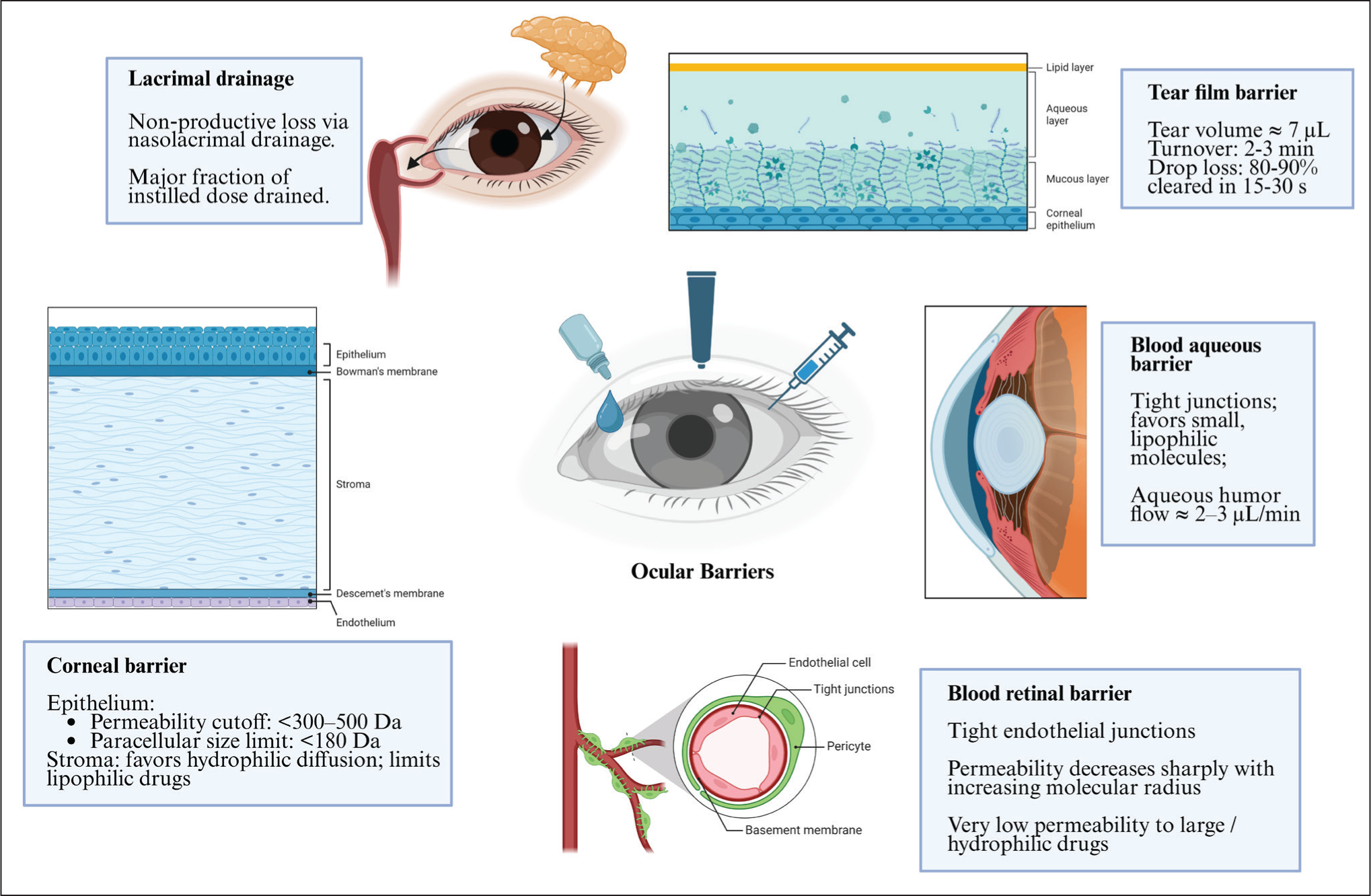
Most ocular diseases can be treated with powerful medications, but their therapeutic efficacy is sometimes compromised by various ocular barriers, including the tear film, conjunctival, corneal, and blood-ocular barriers (Figure 4). Static and dynamic ocular barriers are features of human ocular architecture that prevent harmful chemicals, including therapeutic drugs, from entering various parts of the eye. Static barriers include the corneal epithelium, stroma, endothelium, and blood-aqueous barrier (BAB). Dynamic barriers include tear dilution, conjunctival barrier, and blood-retinal barrier (BRB).89,102 Foreign substances are prevented from reaching the blood by the blood-ocular barriers. They are divided into two categories: the BAB in the anterior segment and the BRB in the posterior segment of the eye. 104
Barriers to Ocular Drug Delivery (Created in https://BioRender.com ).
Precorneal Barriers
Capacity of Cul-de-sac
The maximum capacity of a cul-de-sac in human beings is 30 μL. When the lower eyelid returns to its natural position, the reduction is approximately 70%–80%. Additionally, the capacity of the cul-de-sac is lowered by ocular infection and allergic reactions. 104 Given that the duration of residence and concentration of the drug are closely related to its activity, the cul-de-sac’s small capacity lowers the concentration of the drug in the eye, which lessens the therapeutic effect.
Lacrimal Drainage
Lacrimation, non-productive absorption, and solution drainage in the conjunctiva can altogether lead to drug loss from lacrimal fluid. 105 Histologically, the walls of the nasolacrimal duct and the lacrimal sac are vascularized, making them potential sites for systemic absorption. The eye drops first combine with lacrimal fluid after topical administration. Because lacrimal fluid is constantly being produced, the drug’s contact period with ocular tissues is about 1–2 minutes. The lacrimal sac’s higher canaliculus receives about half of the medication, while the lower portion receives the remaining portion. Patient’s age, reflex blinking, and the volume of the instilled medication are among the variables that affect the concentration of the topically applied drug. 106 Smaller amounts are readily removed from the lacrimal sac, but larger volumes readily enter the nose from the nasolacrimal sac.107,108 Moreover, protein binding and drug metabolism may further impede drug absorption. 104
Tear Film and Tear Turnover
Tears create a hydrophilic coating over the ocular surface and remove dirt and pathogens. Mucin found in the tear film also acts as a barrier for topical drugs. 7 The estimated volume of human tears is 7 μL, and tears are rapidly renewed every 2–3 minutes; hence, most topically applied treatments wash out within 15–30 seconds after instillation. 109 As a result, only a small amount of the drug that is used on the cornea successfully penetrates the cornea. The hydrophilic characteristics of natamycin and its suspension lead to rapid washout, similar to other suspensions that perform poorly compared to the soluble lipophilic voriconazole, which benefits from mucoadhesion and reduced tear dilution, despite having a similar tear turnover rate. 31
Corneal Barriers
The biggest static barrier, the cornea, is made up of epithelium, Bowman’s layer, stroma, Descemet’s membrane, and endothelium. The epithelial layers, five to seven in number, are tightly packed with non-keratinized, stratified squamous epithelial cells, linked by tight junctions. This prevents the paracellular diffusion of hydrophilic molecules while permitting the absorption of hydrophobic ones.110,111 Molecules greater than 10Å are effectively prevented by the corneal epithelium. 112 Stroma is a dense layer composed of water. The epithelium prevents the passage of large molecules and hydrophilic drugs, while the stroma blocks lipophilic drugs. 113 The endothelium protects corneal transparency and selectively allows larger molecules and hydrophilic drugs to penetrate the aqueous humor. In a rabbit model study by Zhao et al., single dose topical 5% natamycin resulted in corneal concentrations of 299 ng/g and aqueous humor levels of 27 ng/mL (permeability ratio 0.02–0.23), which are significantly lower than 34 μg/g in cornea and 14.7 μg/mL in aqueous humor (ratio 0.1–1.26) for 1% voriconazole. The ratio stays around 0.005 even after repeated natamycin dosing. Voriconazole’s transcellular passage is preferentially allowed by lipophilic corneal epithelium, whereas natamycin is more restricted via paracellular routes because of tight junctions. 114 Generally, the degree of ionization, charge, hydrophobicity, and molecular weight of the drug influence the rate of corneal penetration. As a result, transcorneal penetration is the rate-limiting step in the transportation of drugs from lacrimal fluid to aqueous humor. 104
Sclera
Compared to the cornea, the sclera has better permeability for hydrophilic substances that diffuse through the collagen network. The significant determinants of drug penetration through the sclera are molecular charge, molecular weight, and molecular radius.115,116 Compared to more permeable alternatives, natamycin’s greater size limits transscleral access by reducing scleral pore diffusion (~10-fold slower than smaller antifungals like voriconazole for hydrophilic routes). 31
Blood-ocular Barriers
The BAB is present on the anterior part of the eye, which blocks various substances from penetrating the intraocular environment. The physical-chemical properties of the drugs and the osmotic pressure determine the drug’s capacity to permeate through BAB. 117 It enables the transportation of small and lipophilic drugs. 104 Due to tight intercellular junctions that restrict the passage of hydrophilic molecules or those of high molecular weight, this barrier is poorly permeable. Diffuse ions and small solutes move via intercellular spaces. Depending on their selectivity, active transporters can also influence the passive diffusion of drugs. Tight junctions of the iris vasculature restrict the flow of chemicals from plasma to the iris stroma when it comes to the drugs that are administered systemically. Substances cannot pass through the non-pigmented ciliary epithelium tight junctions to reach the posterior chamber from the ciliary body stroma. BAB regulates the flow of molecules from plasma into aqueous humor and between the anterior and posterior segments. Drug penetration is further impeded by the 2.0–3.0 mL/min aqueous humor drainage. 118
The BRB is present in the posterior region of the eye and is made up of retinal pigment epithelium (RPE) cells and retinal endothelial cells. 119 BRB primarily prevents substances from diffusing into the retina from systemic circulation. The inner BRB is composed of retinal capillary endothelial cells, features tight intercellular junctions, and prevents hydrophilic compounds and macromolecules from entering the retina. The RPE is situated between the choriocapillaris, and photoreceptors make up the outer BRB. The permeability of molecules across the BRB decreases with an increase in radius. Lipophilic drugs penetrate the RPE by the transcellular pathway, whereas hydrophilic substances mostly permeate through tight junctions (paracellular routes). 118
This understanding facilitates the design of novel delivery systems and enhances natamycin’s bioavailability.
Methods to Improve Ocular Delivery
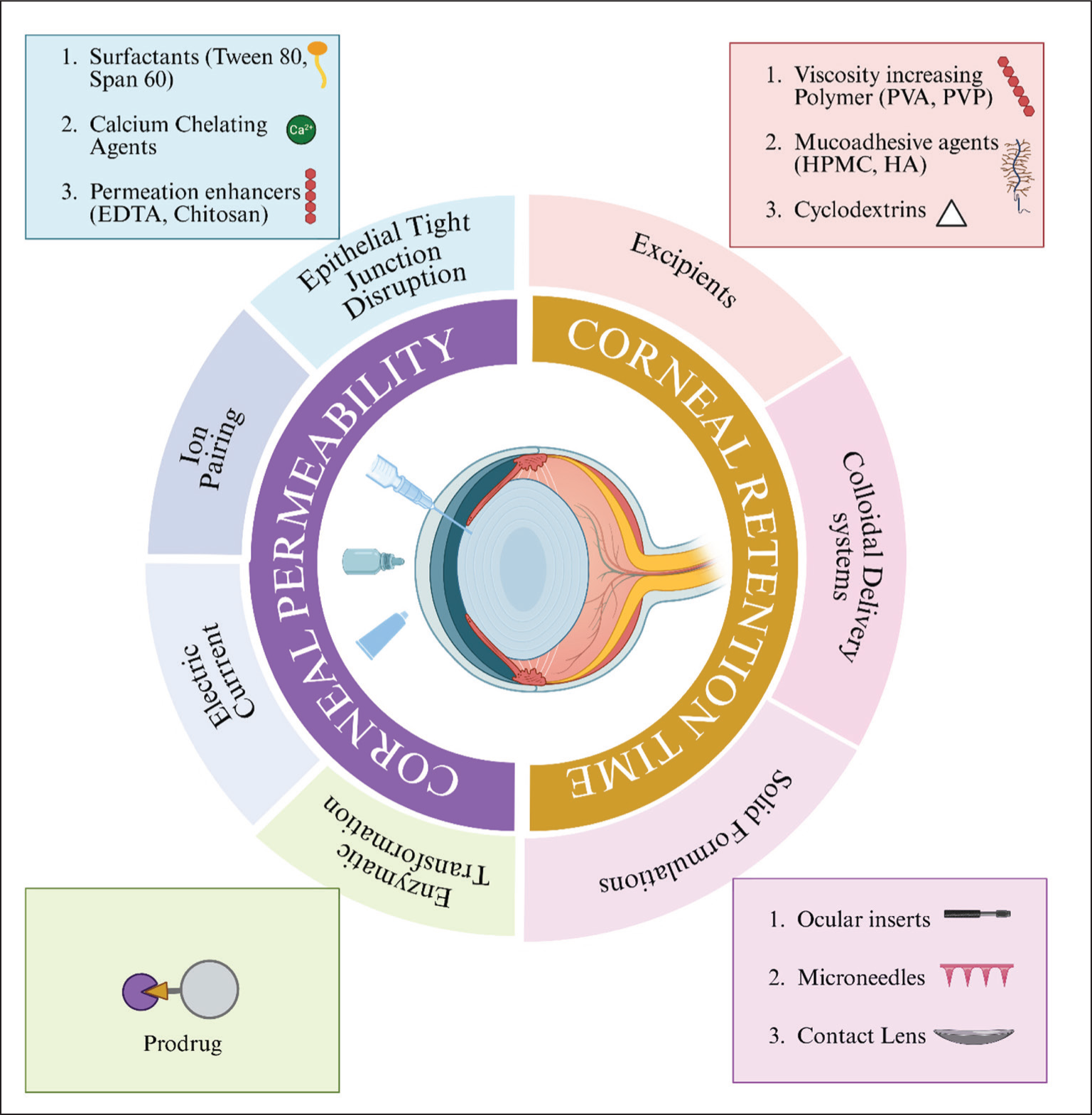
Effective ocular drug delivery is highly challenging due to multiple protective barriers and the rapid clearance of drugs from the ocular surface. Numerous techniques (Figure 5) have been developed to enhance drug release patterns, prolong corneal retention time, and improve drug permeability, thereby promoting therapeutic efficacy. These techniques aim to minimize systemic side effects while increasing patient compliance, reducing dosing frequency, and enhancing drug absorption and effectiveness.
Strategies to Improve Ocular Delivery (Created in https://BioRender.com ).
Increasing Ocular Permeability
Improves the absorption of topically applied drugs. The permeability of drugs across ocular barriers can be improved using prodrugs, permeation enhancers, and other approaches.115,120 For instance, adding surfactants, permeability enhancers, calcium chelating agents, and ion pairs to alter the physicochemical properties of ionized drugs and/ or disrupt the epithelial tight junctions. 121 For the drug molecules to get through the ocular tear barrier and to reach the cornea, they must possess the right lipophilic and hydrophilic qualities. The prodrug approach alters the drug’s physicochemical properties to enhance passive or active diffusion.122,123 A prodrug that undergoes enzymatic conversion within the corneal tissue to become active can also be used. 124 The inclusion of permeation enhancers increases the permeability of ophthalmic medications. These substances temporarily modify the surface of the cornea and conjunctiva to promote rapid drug absorption. Permeation enhancers such as chelating compounds, bile salts, ethers, EDTA, surfactants, and ophthalmic preservatives like benzalkonium chloride can increase drug bioavailability.127–130 Additionally, cyclodextrin (CD) enhances the solubility and bioavailability of hydrophobic drugs by forming complexes. These complexes also decrease local tissue inflammation and increase corneal retention time. 131 Electroosmosis and electrorepulsion effects can be enhanced by applying a low-intensity electrical current, thereby improving drug permeation through the membrane.
Increasing Corneal Retention Time
Adding excipients is one method to lengthen the corneal retention period. Viscosity-enhancing polymers can be an excipient. Drug retention duration and absorption are improved by a variety of viscosity enhancers, including sodium carboxymethylcellulose, polyalcohol, hydroxypropyl methylcellulose (HPMC), and hydroxy methylcellulose. 131 High viscosity eyedrops, however, cause blurred vision, irritate many people, and are not administered accurately. 132 Compared with simple solutions, in situ gels, which can be temperature-, ion-, or pH-sensitive, offer prolonged contact time.133,134 The class of at least 20 O-glycosyl proteins with an anionic charge, known as mucin, makes up the mucus gel layer that covers the ocular surface. A prolonged retention time is provided by excipients, such as chitosan, which allows adherence to the mucus gel layer. CD, which covalently binds to mucoadhesive polymers, can help extend residence time and improve drug solubility. 132 Numerous colloidal delivery systems have been developed to enhance ocular delivery. Solid polymeric devices also provide a sustained release of ocular drugs. However, patients typically reject solid techniques due to pain and visual disturbances. 135
Natamycin Delivery Systems
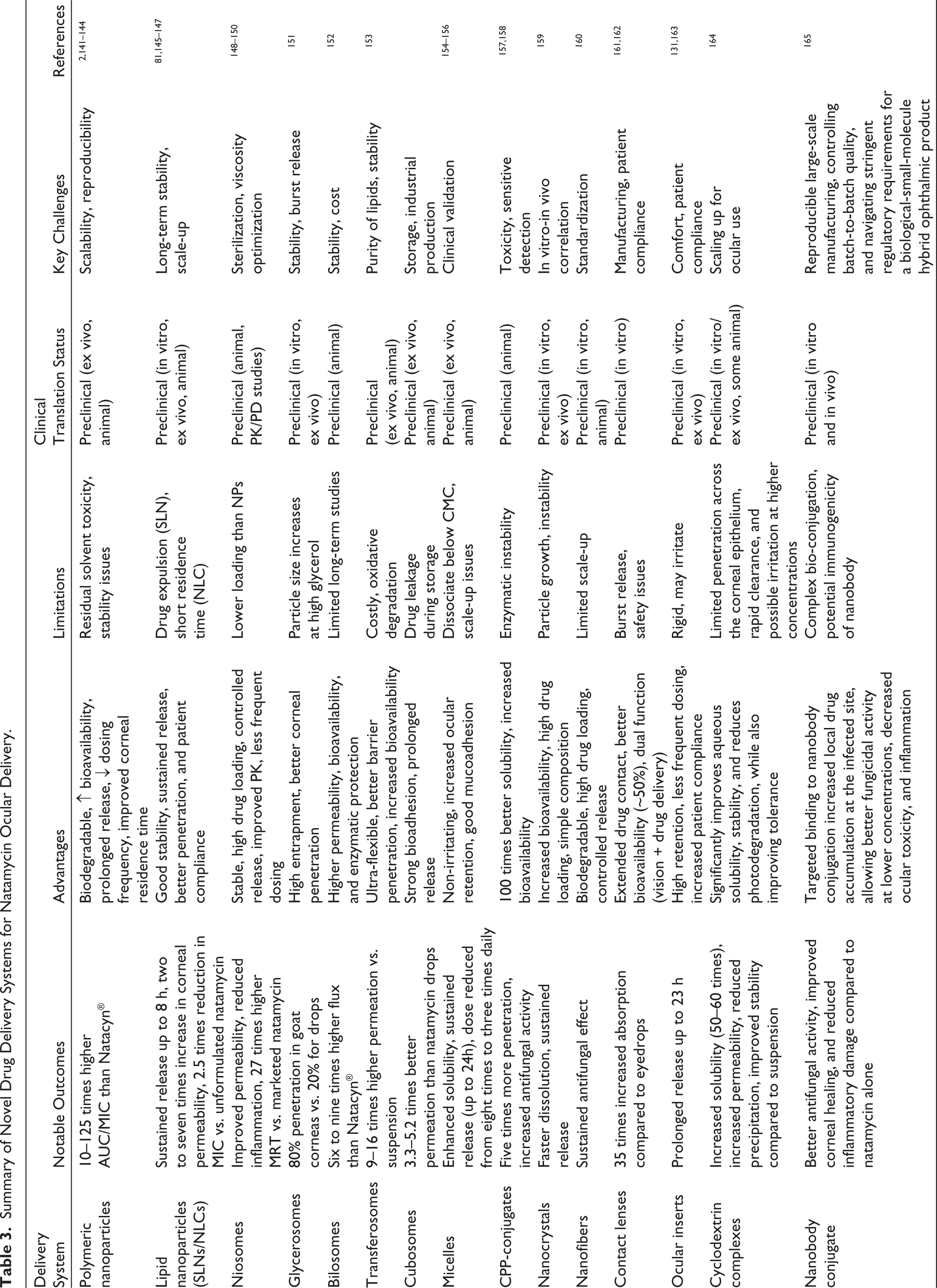
To address the physicochemical and ocular barriers discussed in the previous sections, several polymer-based and nanotechnology-driven strategies have been developed to enhance the ocular delivery of natamycin. These delivery methods can enhance corneal penetration and ocular retention, thereby preserving the natamycin MIC in the lacrimal fluid and facilitating disease treatment with minimal risk of resistance development and infection recurrence. 136 Table 3 summarizes the novel drug delivery systems developed for natamycin, highlighting their composition, findings, and therapeutic advantages.
Summary of Novel Drug Delivery Systems for Natamycin Ocular Delivery.
Nanoparticles
Nanoparticles are desirable delivery systems due to their better permeability and lower ocular irritation. They act as a reservoir that helps to lower the dosage and frequency of administration.138,139
Polymeric Nanoparticles
Natamycin encapsulated polycaprolactone (PCL) nanoparticles functionalized with 5% and 1% poly-D-glucosamine (PDG) were studied. It improved the drug’s precorneal residence time and paracellular transport. The drug release followed the Korsmeyer-Peppas model. Cmax/MIC90 and AUC(0–10)/MIC were 10 and 125 times greater than standard. These nanoparticles demonstrated superior colloidal stability with no discernible particle aggregation or precipitation. Ocular tolerance studies showed no signs of irritation. 140
Compared with Natamet, the conventional eye-drop, natamycin encapsulated lecithin/chitin nanoparticles demonstrated sustained drug release for up to 7 hours. The area under the curve (AUC) increased 1.47-fold, whereas clearance decreased 7.4-fold. Chitosan provided greater retention, better mucoadhesion, biocompatibility, non-toxicity, and biodegradability. 2 Lecithin improves sustained drug release and lipophilic drug-loading. 141 Shah et al. studied a thermosensitive natamycin-loaded triblock copolymer nanoparticle and poloxamer gel complex, which improved drug-loading, penetration, and stability. The natamycin nanoparticles showed a lower MIC than the natamycin solution. The cytotoxicity assay using Human Corneal Epithelial (HCE-T) cells showed that the polymer block inhibited cell proliferation rather than killing cells. However, in an in vivo transcorneal penetration study in male New Zealand rabbits, the formulation effectively increased the amount of natamycin in the eye without causing epithelial damage or inflammatory cell infiltration. It demonstrated sustained release with enhanced penetrability and longer retention time, and its therapeutic impact was equivalent to that of 50 mg/mL natamycin suspension. 142
Cui et al. developed a co-delivery system of natamycin and clotrimazole using chitosan and PLGA, prepared via coaxial electrospray. This was able to achieve a superior drug release profile by transitioning from a rapid initial burst release (33%–37% of the drug in 2 hours) to a prolonged sustained release (80%–90% of the drug over 36 hours), compared to almost complete clearance of free drugs in just 4 hours. This also showed better antifungal effects and no corneal irritation. 143 Liu et al. developed macrophage membrane-coated PLGA nanoparticles for the delivery of natamycin. This demonstrated an encapsulating efficiency of ~41%–51%, prolonged natamycin release, and significantly improved ocular retention compared to the free drug and uncoated nanoparticles. These nanoparticles demonstrated improved antifungal efficacy, reduced inflammatory effects, lower cytotoxicity, and better therapeutic effects compared to the controls. 144
Lipid Nanoparticles
Lipid nanoparticles contain an external surfactant shell and a lipid core, which entrap hydrophobic or lipophilic drugs. 139 Natamycin solid-lipid nanoparticle (SLN) was produced by Khames et al. and then optimized using a three-level, three-factor Box-Behnken statistical design. This demonstrated an initial burst release within the first 2 hours, followed by a sustained, continuous release over the next 8 hours. The nanoparticles significantly enhanced antifungal activity against A. fumigatus and C. albicans, as evidenced by a 2.5-fold decrease in the MIC against the fungal strains compared to the unformulated natamycin. The calculated Papp was 11.59 × 10–2 cm/h for ex vivo corneal permeation studies, confirming increased ocular absorption. 82 Natamycin SLNs were prepared using Pluronic F127 (5%), 1:1 mixed lipids (Compritol AT0888 and stearic acid) loaded in a 4% HPMC gel. Compared with the marketed product, this resulted in sustained in vitro natamycin release from the gel for 6 hours (depending on polymer concentration). The in vitro antifungal effect study on C. albicans showed that the nanoparticles exhibited the maximum zone of inhibition compared to other formulations and the commercial product. The developed SLN demonstrated maximum curative efficacy against Candida keratitis with a regulated release of up to 8 hours, reducing the frequency of doses. 145
Nanostructured lipid carriers (NLC) are a special combination of solid (fat) and liquid (oil) lipids with an irregular, formless lattice arrangement, which can exist as solid-lipid matrixes at room or body temperature.146,147 Lipid nanocarrier for dual-drug delivery of ciprofloxacin (CIP) and natamycin were embedded in an in situ gelling system. This demonstrated a continuous release of both drugs for over 24 hours. The NLC as well as the NLC gelling system showed better corneal permeability in rabbit eyes. Compared with natamycin, the permeability of NLC and the NLC gelling system was 5 and 2.5 times higher, respectively. 148 Patil et al. developed natamycin-loaded polyethylene glycosylated (PEGylated) NLCs, which exhibited transcorneal permeability (across isolated rabbit corneas) approximately seven times higher than that of Natacyn→ and approximately two times higher than that of natamycin NLC. PEGylated NLCs had approximately two times higher natamycin concentration in the cornea and iris-ciliary body than diluted Natacyn→ (0.3%), according to an in vivo distribution study, indicating enhanced corneal penetration of NLCs over natamycin solution. 149
Vesicular Systems
By imitating the biological membranes of corneal epithelium, these lipid or surfactant-based vesicles increase adhesion and transcellular diffusion. These carriers enhance the AUC on the corneal surface, prolonging the mean residence time (MRT) and decreasing tear turnover-mediated clearance.
Niosomes
Niosomes are bilayer vesicles made of non-ionic surfactants, which have better biocompatibility, fewer adverse effects, and greater permeability, stability, bioavailability, and controlled release compared to liposomes.150–152 A dual-purpose natamycin-loaded niosomal gel with ketorolac tromethamine (KT) was created by El-Nabarawi et al. to increase natamycin permeability through the cornea and reduce inflammation brought on by fungal keratitis. In contrast to Natacyn→, which demonstrated 85.52% of drug release after 8 hours, the in vitro drug release of the niosome demonstrated an initial burst release within the first 3 hours, attributed to diffusion and desorption of natamycin existing on the niosomal surface, followed by continued release (77.49% after 24 hours). Next, the optimized niosomal emulsion was added to a gel containing 0.5% KT. HPMC-E4 and sodium carboxymethyl cellulose (NaCMC)—concentration-dependent drug release was demonstrated in a natamycin niosome-loaded gel. The results showed that the MIC for the 4% NaCMC niosomal gel was 8 μg/mL, whereas the MIC for the 2% HPMC-E4 was 63 μg/mL. This difference might be due to the increased viscosity of the gel, which led to worse natamycin diffusion. The in vivo assessment had no signs of corneal irritability. Additionally, compared with the 2% HPMC-E4 niosomal gel group, histopathological investigation demonstrated a greater decrease in fungal load and corneal inflammation in the 4% NaCMC niosomal gel-treated group. The combinations enhanced ocular bioavailability and corneal permeability, thereby reducing the need for frequent dosing and minimizing systemic side effects. 152 Paradkar et al. found similar outcomes in ex vivo transcorneal permeation and ocular irritancy studies, as well as extended drug release up to 25 hours. 153 N-trimethylchitosan (TMC)-coated cationic mucoadhesive natamycin-loaded niosomes were created by Verma et al. Pharmacokinetic studies demonstrated that the TMC-coated niosomes achieved an MRT 27 times higher than the marketed suspension and a 1.5-fold higher AUC(0–12), confirming its enhanced ocular retention and increased drug exposure. The sustained release of the niosomes over 12 hours resulted in a decrease in both dosage and frequency of dosing. They also found that this formulation was able to kill Candida in both time and concentration-dependent manner. 154
Glycerosomes
Glycerosomes are liposomes modified with glycerol that have better ocular penetration due to their increased stability, fluidity, and deformability.155,156 Gupta et al. created natamycin glycerosome eye drops. This had a higher entrapment efficiency (80.84%) than liposomes (59.5%) and demonstrated improved in vitro drug penetration (93.42%). It also provided superior retention in the eye compared to liposomes (57.6%) and natamycin eye drops. The glycerosomes (approximately 80%) demonstrated comparatively better corneal penetration in ex vivo trials conducted on excised goat corneas as compared to conventional liposomes (approximately 75%) and natamycin eye drops (approximately 20%). 157
Bilosomes
Bilosomes are bile salt-containing non-ionic nanovesicles that provide high flexibility, durability, and improved corneal penetration. Bile salts and surfactants shield the drugs from enzymatic breakdown and enhance ocular permeability.158,159 Janga et al. used xanthum and gellan gum to study natamycin bilosome-loaded ion-sensitive in situ gels. Compared with xanthan gum, in situ gellan gum gel demonstrated better mucoadhesion and faster sol-gel conversion. Gellan gum was found to be non-toxic to corneal epithelial cells. Ex vivo investigation showed a 6- to 9-fold increase in transcorneal flow compared with Natacyn→. When compared to the natamycin suspension, the bilosome-loaded in situ hydrogel-treated group exhibited a higher concentration of natamycin in ocular tissues after 6 hours. The bilosome and bilosome-loaded in situ gel showed a Papp of 1.92 × 10–5 cm/s and 1.42 × 10–5 cm/s, respectively, compared to the control (0.14 × 10–5 cm/s), which could be due to improved permeability of bilosomes. 160
Transferosomes
Transferosomes are ultra-deformable liposomes with edge activators that reduce interfacial tension and adapt to epithelial pores to increase transcorneal permeability.161,162 Using gellan gum, Janga et al. created natamycin-loaded transferosomes that incorporated an ion-sensitive in situ gel. Biocompatibility has been shown in corneal histology. Compared with natamycin suspension, transferosomes and in situ gel demonstrated approximately 9- and 16-fold increases in ocular permeability, respectively. The transcorneal flow of the formulation was approximately 16 times that of the control, with a Papp of 3.9 × 10–5 cm/s. 163
Cubosomes
Cubosomes with their honeycomb-like structure, these nanovesicles can encapsulate diverse drugs and provide bioadhesion, sustained release, enzymatic biodegradability, extended corneal residence time, and a lower dosing frequency.131,164 Hosny et al. studied 1.5% Carbopol 934 loaded natamycin cubosomes loaded with a pH-sensitive in situ gel. When tested on excised rabbit corneas, the in situ gel demonstrated a 3.3-fold increase in natamycin penetration in comparison to the commercial 2% natamycin suspension and a 5.2-fold enhancement in contrast to the natamycin suspension. The Papp followed the order: cubosome dispersed in in situ gel (6.4 × 10−4 cm/min) > cubosome (4.8 × 10−4 cm/min) > natamycin suspension (1.9 × 10−4 cm/min) >commercial natamycin 2% suspension (2.5 × 10−4 cm/min). It also improved precorneal penetration. An in vivo ocular irritation test conducted on New Zealand rabbits showed that the cubosomal formulation was less irritating and safer than the commercial suspension. 137 Kazi et al. investigated the application of natamycin cubosome nanoparticles, which exhibited a two-stage drug release profile: an initial burst release followed by sustained release for up to 8 hours. Goat corneal permeation studies showed higher permeability (20.59 × 10–2 cm/h) and flux (5.46 mol/h) compared to the natamycin suspension. The Draize test showed no eye damage and a zero-irritation score. 165
Micelles
Micelles are self-assembling nanocarriers with a hydrophilic shell and lipophilic core that, by adjusting their size, composition, and structure, improve solubility, prolong stability, postpone clearance, and enable controlled drug release.166,167 Guo et al. prepared mucoadhesive poly(ethylene glycol)-block-poly(glycidyl methacrylate) (PEG-b-PGMA) micelles. The in vivo antifungal investigation found that, due to its better release profile, the number of doses may be reduced from eight to three times a day. The MTT [3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium Bromide] assay demonstrated that the natamycin micelles were non-irritating and biocompatible, and they also increased corneal permeability and natamycin solubility. Precorneal retention time was also increased. An initial burst release followed by a plateau phase was observed in in vitro release studies. 168 Polymeric nano micelles developed by Lorenzo-Veiga et al. using Pluronic P103 and Soluplus dispersions with or without cyclodextrin (10% w/v). This increased natamycin solubility. The in vitro release studies demonstrated that Pluronic P103 micelles released the drug fastest within 6 hours, with more rapid diffusion and greater permeability (Papp increased up to 1.67 × 10 6 cm/s), which was attributed to their small size and less compact structure. According to Hen’s egg test- chorio-allantoic membrane (HET-CAM) assay, the micellar formulations did not cause any irritation. 169 Sathe et al. developed a 1% natamycin nano-micelle formulation with D-α-tocopheryl polyethylene glycol 1000 succinate. This demonstrated significantly improved corneal penetration, provided sustained drug release for up to 24 hours, longer ocular retention, and enhanced biocompatibility. 170
Cell-penetrating Peptide (CPP)
CPPs are shorter amino acid sequences that can pass through different cell membranes without interacting with receptors. Jain et al. developed the first conjugate of natamycin with the Tat dimer (Tat2 and MTat2), a CPP that demonstrated improved cellular penetration and up to a 100-fold increase in natamycin solubility in water. The two-fold micro broth dilution assay showed that a low concentration (10 μM) of natamycin conjugated to CPPs demonstrated complete inhibition of F. solani, indicating a two-fold increase in antifungal activity compared to unconjugated natamycin. 171
In comparison with the commercially available natamycin suspension, Rohira et al. assessed the tissue penetration and antifungal activity of natamycin conjugated to Tat2. This showed a fivefold increase in ocular penetration and accumulation in the aqueous and vitreous humor, indicating better natamycin bioavailability. Cytokine analysis revealed that natamycin-Tat2 conjugation significantly decreased IL-6 levels, whereas Tat2 alone decreased both IL-6 and IL-1β levels. It also considerably reduced the natamycin concentration required for an in vivo antifungal effect against the Fusarium species. 172
Nanocrystals
Nanocrystals are pure drug particles with a high drug-loading capacity, providing better solubility, quicker dissolution, increased mucoadhesion, and extended ocular surface retention, all of which contribute to effective drug delivery.173,174 Das et al. manufactured pH-sensitive in situ gels loaded with natamycin nanocrystals using Carbopol 940P and HPMC EL 50 V. According to an in vitro release investigation, the drug released from nanocrystals was 87.56% faster after 2 hours than from the pure drug. The gel enhanced ocular bioavailability, as evidenced by the sustained in vitro release compared to the marketed suspension. Ex vivo investigations demonstrated increased corneal penetration of the in situ gel, attributed to its prolonged dissolution. 175
Nanofibers
Nanofibers are large-surface, biodegradable polymeric drug carriers made by sol-gel or electrospinning techniques.176,177 Veras et al. created PCL-natamycin nanofibers through electrospinning. Nanofibers exhibited better antifungal activity with formulations containing THF (tetrahydrofuran): N, N-dimethyl formamide (DMF) (4:1, v/v), PEG 4000, and medium chain triglycerides dissolved in THF: Chloroform (3:1 v/v). These formulations were effective against eight distinct yeast and filamentous fungal isolates. 178
Contact Lens
These are ocular prosthetics that can be used to deliver drugs and correct vision. By extending the corneal contact period, the drug absorption into the cornea increases by up to 50%, making CLs 35 times more effective than eye drops. 179 The in vitro absorption and release kinetics of natamycin from various commercial silicone hydrogel lenses (SiHL) and conventional hydrogel lenses (CHL) were investigated by Phan et al. Even though SiHL and CHL both released a clinically significant amount of drug, their burst release indicated that they were unsuitable for commercial application for fungal keratitis. 180 Phan et al. investigated CD-functionalized CL materials for silicone-based and traditional hydrogel lenses to overcome the challenges. The results of the investigation indicated that the functionalized methylacrylated β-CD and methylacrylated hydroxypropyl (HP)-β-CD CL materials on CDs exhibited better drug-loading and release properties, particularly at higher concentrations. 181
Ocular Inserts
Sterile, multilayered, drug-loaded devices called ocular inserts are made to fit into the cornea or lower or upper fornix.182,183 They can be dissolvable or mucoadhesive and are composed of soluble or insoluble polymers.184,185 Their main benefit is extended precorneal residence, which allows for less frequent dosing, enhanced bioavailability, reduced systemic absorption, and controlled drug release. However, discomfort and application difficulty may lead to decreased patient compliance. 186 Bhandari et al. combined a solid natamycin dispersion with a polymeric ophthalmic film comprising polyvinyl alcohol (PVA), chitosan, and ethyl cellulose. Studies on in vitro permeation have shown that natamycin release decreases with increasing polymer concentration; this may be due to the drug’s extended diffusion pathway. The drug permeability in the ex vivo trial was lower than in the in vitro study, possibly due to the presence of fatty tissues and the cornea’s different pore sizes, which block drug permeation. The Draize eye irritation test indicated that the formulation was non-irritating, and the antimicrobial test showed an inhibitory zone that persisted for 24 hours and remained for up to 15 days. 187
Rajasekaran et al. developed polymeric controlled-release ocular inserts for natamycin delivery using different ratios of cellulose acetate phthalate, hydroxypropyl cellulose phthalate, and Eudragit, with PEG-400 as a plasticizer. A formulation comprising 3% Eudragit L-100 and 1% Eudragit L-100 exhibited minimal moisture absorption and zero-order drug release, with a prolonged natamycin release of 23 hours, attributed to the hydrophobic molecular substitutions of Eudragit L-100. 188
Cyclodextrin Inclusion Complexes
To improve natamycin’s solubility, a 2-hydroxypropyl-ß-cyclodextrin (HPßCD) based formulation was prepared by Díaz-Tomé et al. They also formulated hydrogels based on hyaluronic acid (HA) and PVA. This improved its corneal permeability and antifungal efficacy, while also showing good ocular tolerance. 189 Cai et al. developed randomly methylated β-cyclodextrin (RMβCD) and HPβCD, which increased the solubility of natamycin by 66-fold and 54-fold, respectively. There was an 8.5-fold improvement in transcorneal permeability compared to Natacyn→. 190
Nanobody Conjugate
Liu et al. recently prepared a nanobody specific to ß-glucan in the fungal cell wall and then conjugated it with natamycin. This nanobody suppressed fungal growth by interfering with the production of fungal cell walls and biofilms. Compared to natamycin, this compound exhibited superior antifungal activity, lower cytotoxicity, and reduced ocular surface irritation.
Patents
Two patents now cover the commercial manufacture of natamycin (Table 4). The US Patent and Trademark Office awarded a patent for a stable natamycin suspension (patent number US5552151), filed on April 11, 1995, by inventors Bertus Noordam, Jacob Stark, Ben R. De Haan, and Hong Sheng Tan. The patent was granted on September 3, 1996. These natamycin suspensions are concentrated and exhibit good microbiological, chemical, and physical stability. Another patent has been filed for Natasol, a sterile, water-soluble intrastromal natamycin developed by the Ocular Pharmacology and Pharmacy Division at AIIMS, New Delhi, India, highlighting ongoing efforts to improve natamycin’s solubility and stromal delivery.86,87
Summary of Patents on Natamycin Formulations.

Clinical Relevance and Translational Challenges
The synthesis of novel formulation strategies reveals an astonishing range of technological progress but shows a remarkable lack of actual clinical translation. When compared to standard suspension, natamycin-loaded nanoparticles, SLN, NLC, niosomes, cubosomes, and nano micelles have all shown enhanced corneal penetration, prolonged ocular retention, and superior antifungal activity in rabbit keratitis or biodistribution models, with short-term safety supported by Draize tests, ocular surface grading, and corneal histology. However, translation into real-world therapeutic use faces several barriers. Many delivery systems like nanofibers, drug-eluting CL, ocular inserts, and some vesicular platforms (like glycerosomes, bilosomes, and CPP) are mostly limited to in vitro or ex vivo studies, with little or no data on in vivo ocular infection and virtually no chronic toxicity evaluation, including immunogenicity and retinal safety.
From a regulatory perspective, ophthalmic nanocarriers can be categorized as either complex drug products or drug-device combination products. Therefore, extensive chemistry, manufacturing, and controls (CMC) documentation is necessary for regulatory examination by organizations such as the European Medicines Agency and the US FDA. Particle size distribution, polydispersity, surface charge, drug-loading homogeneity, residual solvent limitations in compliance with ICH (International Council for Harmonization of Technical Requirements for Pharmaceuticals for Human Use) Q3C standards, and long-term stability under ICH Q1A (R2) conditions are all strictly characterized. Validated aseptic processing (USP 71), endotoxin control (USP 85), preservative efficacy testing, and repeatable batch-to-batch production are required for sterile ophthalmic solutions. Industrial challenges, including aseptic scale-up (cGMP regulations [21 CFR Parts 210 and 211]), optimization of various formulation parameters, and toxicological profiling, further compound this preclinical-to-clinical gap. As a result, although combination therapy of natamycin with other antifungals is practiced clinically for severe or resistant cases, it has not yet been incorporated into an advanced ocular nanocarrier co-formulation, highlighting a significant opportunity for future innovation in drug delivery. Importantly, data from the clinical trial registry indicate that none of these novel natamycin formulations has yet advanced to the clinical trial stage or the commercial market, suggesting they remain at the concept or feasibility stage, underscoring the gap between laboratory invention and clinical application.
Conclusion and Future Aspects
Despite decades of clinical experience and evident therapeutic superiority over many recent agents for superficial fungal keratitis, natamycin still suffers from fundamental delivery limitations that have not yet been resolved in practice. Its relatively large molecular size, poor solubility, and suspension-only formulation limit penetration into the deeper corneal stroma and intraocular tissues, limiting its role primarily to superficial keratitis and necessitating frequent dosing due to precorneal loss and low bioavailability. However, due to its potent activity against common causative agents, good safety profile, and relatively low risk of resistance compared to widely used azoles, natamycin remains the drug of choice for filamentous fungal keratitis.
Novel delivery systems have, at the experimental level, addressed several disadvantages of traditional natamycin therapy, including reducing the need for frequent instillations, mitigating the toxicities associated with high dosing, and stabilizing fluctuations in ocular drug levels, while maintaining its broad antifungal spectrum. However, the majority of systems are still in the proof-of-concept or early preclinical stages, with none having progressed to regulatory submission. Future studies must move beyond originality in formulation to translational validation. To ascertain genuine clinical superiority in terms of stromal penetration, fungal clearance, reduced dosing frequency, and long-term ocular safety, leading delivery platforms should be compared side-by-side in a standardized fungal keratitis model. Dual-drug approaches combining natamycin and azoles should receive special consideration to improve outcomes in deep stromal infections, address resistance, and expand spectrum coverage. Translational credibility will be strengthened by establishing a predicted in vitro-in vivo correlation (IVIVC). Next, safety assessments need to go beyond ocular tolerance. Studies of chronic toxicity that evaluate cumulative exposure, inflammatory response, retinal safety, and tissue effects linked to degradation are crucial. An independent toxicological rationale is necessary for novel excipients, surface modifications, and penetration enhancers. For ophthalmic products, sterility assurance, endotoxin limitations, and preservative efficacy validation are essential and must be integrated early in the development process. Also, the design phase needs to incorporate production and regulatory readiness. Regulatory acceptability depends on thorough physicochemical characterization, control of residual solvents, stability validation under ICH Q1A, and batch-to-batch reproducibility under cGMP conditions. Early interactions with organizations like the US FDA could expedite the submission and categorization processes. If these strategies are pursued, natamycin-based nanomedicines with improved precorneal retention, higher targeted tissue levels, reduced dosing frequency, and better adherence could realistically enter clinical testing and ultimately reshape the management of fungal keratitis.
Footnotes
Acknowledgements
The authors are grateful to Dr. Sruthi Vijendran for her guidance on the review process and for her assistance with manuscript preparation.
Authors’ Contribution
Meghana Prabhu led conceptualization, literature review, original draft preparation, editing, and visualization. Mruganka Rahul Lale provided methodological support, data validation, and critical review. Sulatha V. Bhandary and Bharath Raja Guru contributed to conceptualization, editing, revision, and final approval of the manuscript. All authors agree to be accountable for all aspects of the work and ensure its accuracy and integrity.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The Manipal Academy of Higher Education (MAHE) Faculty Development Fund provided funding for the Article Processing Charges (APC) associated with this publication.
Informed Consent
Not applicable.
Use of Artificial Intelligence-assisted Tools:
AI-based language and support technologies are used to improve language and correct grammar.