
Abstract
The aim of this narrative review was to summarize the current evidence on the safety of systemic antifungal agents during pregnancy and to provide a state-of-the-art overview of their rational use in this setting. A comprehensive literature search was conducted to identify articles published between January 1, 2016, and December 31, 2025, including newly approved agents. We concluded that most available data focus on first trimester exposure, whereas evidence for second- and third-trimester use remains limited. Amphotericin B remains the first-line agent for many invasive fungal infections during pregnancy, owing to decades of clinical experience and the absence of consistent evidence of teratogenicity. In contrast, systemic azoles, particularly fluconazole at higher doses and during early pregnancy, have been associated with increased risks of miscarriage and congenital anomalies. Echinocandins and newer antifungal agents, including oteseconazole, ibrexafungerp, and rezafungin, are not recommended during pregnancy because of limited human data and evidence of teratogenicity from animal studies. Overall, the use of systemic antifungal therapy during pregnancy requires an individualized, risk–benefit approach, with careful consideration of gestational age, infection severity, and available safety data. Ongoing post-marketing surveillance and prospective studies are needed to better guide evidence-based management of fungal infections in pregnant patients.
Introduction
Managing fungal infections is challenging due to the varying spectrum of coverage among drug classes, their pharmacokinetic and pharmacodynamic properties, concentrations at the site of infection, and safety considerations. Furthermore, managing pregnant women poses additional challenges, as the safety and efficacy of use need to be thoroughly reviewed. It is essential to evaluate both the agent’s safety for the fetus and whether the antifungal’s pharmacokinetic parameters are affected by pregnancy. 1
Candidiasis in pregnancy is estimated to affect around 10%–20% of pregnant women. The most common form of candidiasis during pregnancy is vulvovaginal candidiasis (VVC), which may cause complications to both the mother and the fetus, such as premature membrane rupture, preterm delivery, and neonatal candidiasis. 2 Furthermore, the American Pregnancy Association states that Candida infections are more common during pregnancy, especially during the second trimester, than at any other time in a woman’s life. 3 Other common fungal infections during pregnancy are cutaneous candidiasis, oral candidiasis (thrush), cutaneous dermatophytosis (tinea infections), and onychomycosis. These mucocutaneous fungal infections can still occur during pregnancy and may persist longer because of limited systemic treatment options available during this period. 4 On the other hand, endemic mycoses such as coccidioidomycosis, histoplasmosis, and blastomycosis are considered rare during pregnancy. However, they may still be more severe due to immune changes during pregnancy. 5 Other invasive fungal infections, such as aspergillosis and mucormycosis, are less commonly seen in pregnant women as they affect mainly immunocompromised hosts such as bone marrow transplant patients and HIV/AIDS patients. 6 Many systemic antifungals are prescribed during pregnancy, of which there have been reports of fetal congenital abnormalities and spontaneous abortions. Furthermore, many physiological changes during pregnancy may lead to changes in drug exposure and side effect profile. This includes an increase in plasma volume/total body water, changes in protein binding, including a reduction in albumin, increased renal clearance, and altered hepatic enzyme activity. 7 These changes can affect the distribution, metabolism, and elimination of antifungal agents, and therefore, prescribing antifungal drugs in pregnancy needs a tailored approach. 2
In the past few years, new antifungal agents have been approved to combat fungal resistance and to provide treatment options with a better safety profile. 8 Oteseconazole received Food and Drug Administration (FDA) approval in 2022 for the reduction of recurrent vulvovaginal candidiasis (RVVC) in females who are not of reproductive potential. It is notable as the first orally available selective CYP51 (an enzyme in the synthetic pathway from squalene to ergosterol) inhibitor approved for the management of RVVC). 9 Another recently approved agent is rezafungin, a second-generation echinocandin that was found to be non-inferior to caspofungin for treating patients with candidemia and was accordingly approved by the FDA for this indication in 2023. 10 Additionally, ibrexafungerp, approved by the FDA in 2021, is the first oral non-azole agent for the treatment of VVC. This novel oral glucan synthase inhibitor exhibits broad-spectrum antifungal activity. It is currently the only oral antifungal indicated for the treatment of VVC and RVVC. 11 Given recent advances and growing evidence for the use of systemic antifungal agents, including newly approved ones, this narrative review has two objectives: (a) To summarize the current evidence on the safety of these agents during pregnancy and (b) to provide a state-of-the-art overview to guide healthcare providers in the systemic treatment of fungal infections during pregnancy.
Methodology
Search Strategy
A comprehensive literature search was conducted to identify articles published within the last decade related to systemic antifungals (updated list presented in Table 1), with a defined publication window from January 1, 2016, to December 31, 2025. The search was performed across PubMed/MEDLINE, Embase, and Scopus to ensure broad coverage of the medical literature.
Updated List of Systemic Antifungals.

The search strategy was two-pronged. First, a broad search was executed using a combination of Medical Subject Headings terms and keywords. The core title/abstract search was: (“Antifungal agents” OR “antifungals”) AND (“pregnancy” OR “gestation” OR “pregnant women”). Second, specific searches were conducted for each antifungal agent. These searches combined the name of each drug with the term “pregnancy.” Examples of these particular searches include:
(“Fluconazole”) AND (“pregnancy”) (“caspofungin”) AND (“pregnancy”)
The reference lists of retrieved systematic reviews and key articles were also manually screened to identify any additional relevant studies that may have been missed in the initial database search. A narrative review design was chosen for substantive reasons. Primarily, the existing body of evidence concerning systemic antifungal use during pregnancy is notably heterogeneous, encompassing case reports, series, registry-based cohort studies, meta-analyses, and animal toxicity data. Furthermore, newly approved agents are supported by limited human research, limiting the practicality of conducting a formal systematic review.
Inclusion and Exclusion Criteria
For this narrative review, we included studies that addressed the use of systemic antifungal agents during pregnancy. Evidence from a wide range of sources was considered for inclusion, including case reports, case series, observational studies, meta-analyses, and narrative or systematic reviews, as well as relevant animal data that provided safety insights. Studies were included if they reported maternal or fetal outcomes such as congenital anomalies, miscarriage, neonatal complications, or the absence of adverse effects. Only publications in English and within the period from January 1, 2016, to December 31, 2025, were reviewed. Exclusion was limited to studies that did not address antifungal exposure in pregnancy or lacked any outcomes relevant to maternal or fetal safety. Articles that focused exclusively on topical antifungals or provided insufficient information for interpretation were also excluded.
Data Extraction and Synthesis
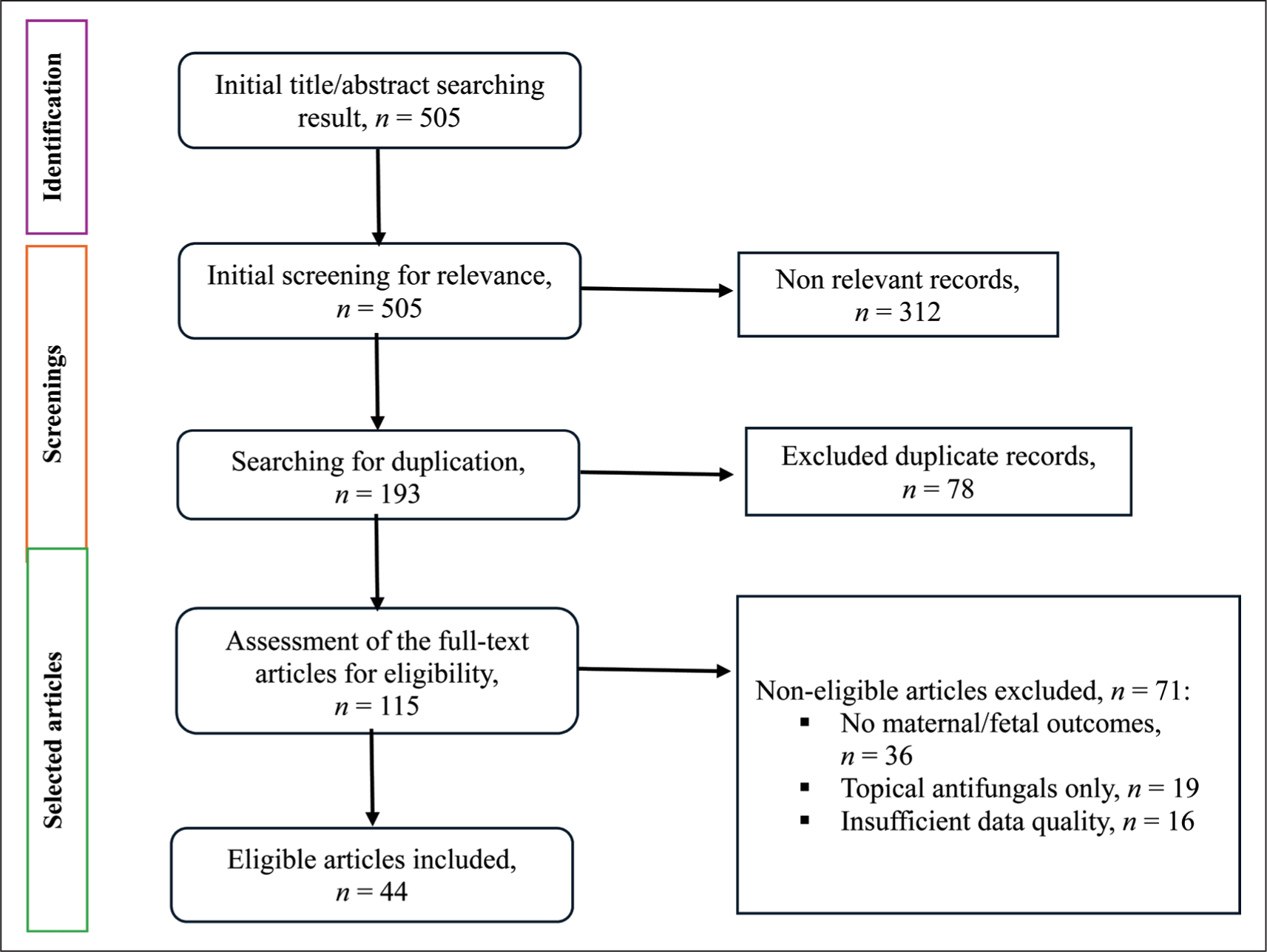
Figure 1 presents the screening, identification, and selection process of included articles. For each included study, relevant information was extracted and organized. The extracted data included: First author and year of publication; study design; population characteristics; the specific antifungal agent(s) studied (including route of administration, dosage, and timing of exposure); and the primary findings related to maternal and fetal safety. (Summary of the main human and animal developmental toxicity studies of systemic antifungals presented in Tables 2 and 3).
Flowchart of Screening, Identification, and Selection of Included Articles.
Summary of the Human Studies on the Safety of Systemic Antifungals in Pregnancy.


Summary of Animal Developmental Toxicity Studies to Systemic Antifungals.


The findings were synthesized using a narrative approach. The evidence was organized thematically by class and specific antifungal agent. Within each category, the results were discussed in relation to outcomes, such as the risk of major congenital malformations (MCMs), cardiac defects, and spontaneous abortion.
Results and Discussion
Systemic Azoles
Systemic azoles, such as fluconazole, are used to treat Candida infections, including VVC. While extended-spectrum azoles such as voriconazole and itraconazole provide additional coverage against Aspergillus. Additionally, newer azoles, including posaconazole and isavuconazole, are active against mucormycosis. 12 None of these agents is recommended for use in pregnancy. Systemic azoles act as inhibitors of fungal Cytochrome P450 (CYP450) lanosterol 14α-demethylase, which leads to impaired ergosterol synthesis and, accordingly, inhibits cell membrane formation. 12 Additionally, they inhibit multiple mammalian CYPs involved in androgen/estrogen synthesis, the glucocorticoid/mineralocorticoid pathway, and retinoic acid metabolism, which may affect endocrine-mediated developmental processes and increase the risk of teratogenicity, including craniofacial, cardiac, and skeletal anomalies. 13 However, given the limited nature of the human data, a solid conclusion requires larger prospective studies to confirm these findings and establish an association. 14 Although all azoles share the same mechanism of action, fluconazole has a unique pharmacokinetic property: It has a relatively low protein binding and readily crosses the placenta, leading to high fetal exposure with repeated dosing. Unlike other triazoles, which are more lipophilic, and highly protein-bound, they can still cross the placenta, but with likely less fetal exposure than fluconazole. 13
Fluconazole
Many studies have discussed the use of fluconazole in pregnancy and have stated that it should be avoided, as the risks outweigh the benefits.15,16 In a recent population-based cohort study published in 2025, using data from four nationwide Norwegian registries, including 2,119 pregnant women on fluconazole. The study showed an association with fluconazole and miscarriage (HR = 1.61; 95% CI: 1.45–1.78). However, they stated that, based on a probabilistic bias analysis, the underlying infection may affect some associations. Nevertheless, they concluded that prescribing oral fluconazole during the first trimester of pregnancy should be avoided, if possible. 17 Another population-based cohort study, drawn from national data in the United States, examined pregnant women for at least three months before their last menstrual period and for up to one month postpartum, as well as infants covered for at least three months following birth. The study population included patients who had received oral fluconazole during the first trimester of pregnancy. 18 Of the 1,969,954 pregnancies, 37,650 were exposed to oral fluconazole. They calculated the adjusted relative risk after propensity stratification for musculoskeletal malformations, conotruncal malformations, and oral clefts and concluded that the use of oral fluconazole in the first trimester was not associated with oral clefts or conotruncal malformations; however, there was a small association with musculoskeletal malformations. In a recent meta-analysis that included randomized controlled trials and nine observational studies, 116,425 pregnancies were exposed to fluconazole. The findings indicated that fluconazole use during the first trimester did not significantly increase the risk of MCMs. However, potential risks, specifically at higher cumulative doses (defined as greater than 150 mg), may be associated with MCMs and warrant caution and further confirmation. Furthermore, they reported a significant association with miscarriages. 19 A meta-analysis of nine studies evaluated the relationship between fluconazole exposure during pregnancy and the incidence of birth defects. The findings indicated that maternal use of fluconazole during the first trimester was linked to an elevated risk of fetal heart defects, regardless of dosage. 20 As a result of this growing evidence, Pfizer updated fluconazole labeling in 2024 to include a warning that it should not be used during pregnancy unless clearly necessary. Furthermore, they have stated that a woman of childbearing age is recommended to wait one week after the last dose before becoming pregnant, even with single-dose treatment. 21 Although findings vary across studies and comparators, reported birth defects include musculoskeletal anomalies (e.g., craniosynostosis, limb defects, and other skeletal malformations) as well as cardiac defects, including septal anomalies. Furthermore, the risk of spontaneous abortion was also reported, especially with early pregnancy and oral fluconazole exposure.15,23 On the other hand, a very important factor reported is the pregnancy trimester, as most of the evidence of negative outcomes and birth defects, specifically organogenesis, was reported in the first trimester,18,20,22 but the risk in the second and third trimesters cannot be excluded, specifically with high cumulative doses, as some evidence of negative outcomes is reported as well. 23 Overall, the risk profile of fluconazole is low at low doses, but the risk is not zero, and it can still adversely affect pregnancy. The risk is higher at higher doses, particularly during early pregnancy.
Itraconazole
Fetal outcomes associated with both itraconazole and fluconazole use during pregnancy were examined in a systematic review and meta-analysis of eight cohort studies and one case-control study. 24 The pooled estimate of the incidence of birth defects showed no difference between the populations treated with fluconazole or itraconazole and the non-exposed population. When categorizing the types of birth defects reported in the itraconazole population, the highest birth defect in the exposed group was eye defects at 0.56%. The authors concluded that this type of birth defect requires further investigation. Furthermore, animal studies have also reported embryotoxicity and malformations, especially during early pregnancy. 25 Overall, the evidence for itraconazole is lower than that for fluconazole; however, given the limited human data, primarily from observational studies, and evidence of embryotoxicity in animal studies, itraconazole should be avoided, particularly in the first trimester and when high doses or prolonged treatment are used.
Voriconazole, Posaconazole
For voriconazole and posaconazole, no human data are available, and current evidence is limited to animal studies showing teratogenicity. These agents have shown many negative signals in animal studies, including skeletal abnormalities and fatal loss, which reflected the product’s labeling. Therefore, it is recommended that pregnant women avoid both agents and that women of childbearing potential use effective contraceptive methods during the course of therapy.26,27
Isavuconazole
One case study reported the use of isavuconazole at 24 weeks of gestation in a patient with pulmonary aspergillosis proven by imaging and culture. 28 She is a 37-year-old with autosomal recessive chronic granulomatous disease and repeated fungal infections. At 21 weeks of gestation, she had three concurrent infections: Influenza A (PCR), Pneumocystis jirovecii (silver stain), and Aspergillus fumigatus (culture). The patient was started on liposomal amphotericin B, which controlled infection but caused nephrotoxicity and thrombocytopenia. At 24 weeks of gestation, amphotericin was stopped, and isavuconazole was started. The treatment continued for 12 weeks and was completed at 36 weeks of gestation. She delivered a healthy infant, and postpartum computed tomography imaging showed complete resolution of pulmonary lesions. After six months of follow-up, both the mother and the infant remained healthy. This case report is the only available human evidence and was conducted in the second trimester; accordingly, conclusions regarding safety cannot be drawn, and further studies are needed. Based on labeling information from animal studies of teratogenicity, it’s recommended to avoid during pregnancy, and women of childbearing potential should be advised to use effective contraceptive methods during the course of therapy. 29
Oteseconazole
Two key differences between this novel agent and other azoles are its exceptionally long half-life, estimated at approximately 138 days, and its lower affinity for human cytochrome P450 enzymes. This is considered an advantage, as it may be associated with a lower risk of adverse effects and drug–drug interactions. 30 It was approved to reduce the incidence of RVVC in females with a history of RVVC who are not of reproductive potential, alone, or in combination with fluconazole. It is contraindicated in pregnancy and in patients who could become pregnant, and accordingly, it is only used in postmenopausal women or those who have permanent infertility. 31 This is included in the product labeling because of ocular abnormalities that were observed in rats from day six of gestation through day 20 of lactation at a dose 3.5 times the recommended human dose. The ocular abnormalities that were documented included cataracts, opacities, exophthalmos/buphthalmos, optic nerve/retinal atrophy, lens degeneration, and hemorrhage. 32 One human study reported the use of oteseconazole in eight pregnant women without adverse outcomes. 33 A total of 13 pregnancies were reviewed (eight participants taking oteseconazole [six healthy births, one unknown outcome, and one elective termination]; five taking placebo [three healthy births, one unknown outcome, and one elective termination]). No adverse obstetrical reaction or fetal abnormality was reported. Overall, given the small number of pregnancies in this study, we cannot confirm these findings, and a larger sample is needed to confirm safety. Based on the risk reported in animal studies and product labeling, this agent should be avoided in pregnancy, and alternative agents would be considered when indicated. Figure 2 summarizes the key information for this newly approved agent.
Chemical Structure and Key Features of Oteseconazole (Figure References 1).

Echinocandins
Caspofungin, Micafungin, and Anidulafungin
Echinocandins cause cell wall disruption in fungi by inhibiting β-1,3-D-glucan synthase. This target is absent in humans, which contributes to their favorable safety profile. It is highly protein-bound, consisting of large cyclic lipopeptides, available only as an intravenous product. Echinocandins are among the most widely used systemic antifungals, as they have excellent activity against yeast, including fluconazole-resistant candidiasis. 34 Their approval has changed the practice of managing systemic fungal infections by combining extended coverage with a better safety profile and fewer drug interactions.
Regarding their use in pregnancy, multiple reviews on echinocandins as a class stated that echinocandins should be avoided during pregnancy, as they have shown embryo toxicity, and their use should only be considered if the potential benefit to the mother outweighs the potential risk to the fetus.35,36 These recommendations are mainly based on animal studies. Given the absence of the molecular target ([1,3]-β-D-glucan synthase) in humans, any fetal risk is likely mediated by off-target or maternal physiological effects. However, no available data to quantify this. 27 Caspofungin, the first approved agent in the class, was studied in rats and rabbits at the recommended human dose and showed embryotoxicity and bone ossification changes.27,34 While micafungin at four times the recommended human dose showed visceral abnormalities and increased abortion.27,34 For anidulafungin, at a dose two times the recommended human dose in rodents, skeletal abnormalities, and low fetal weight were observed.27,34,36 Additionally, anidulafungin was reported to be used in a pregnant woman as documented in a case report of azole-resistant Candida esophagitis. 37 The patient had poorly controlled HIV/AIDS with a low CD4 lymphocyte count and a high viral load. She was admitted for severe odynophagia with fluconazole-resistant Candida albicans, for which she had repeated admissions in the previous 17 months of her presentation. Her most recent infections responded to voriconazole and anidulafungin in combination, and the patient was accordingly treated with this combination. She was found to be 11 weeks pregnant after starting this regimen for three days, and accordingly, voriconazole was discontinued, and they decided to continue on anidulafungin as the benefit outweighs the risk. She continued for five weeks with resolution of oral lesions after two weeks and resolution of odynophagia by five weeks. The patient had an uncomplicated pregnancy and delivery, with a follow-up after three months of delivery showing a normal baby with no reported skeletal malformation. Nevertheless, despite this case report, it is not recommended to use anidulafungin for the treatment of pregnant women with Candida infections until more evidence in humans is reported. Overall, it is not recommended to use echinocandins in pregnancy unless the risk outweighs the benefit, and no alternative safer options can be used.
Rezafungin
Rezafungin, the latest agent in the echinocandin class approved in 2023, is a semisynthetic echinocandin approved for the treatment of candidemia and invasive candidiasis in adults aged 18 years or older, where limited or no treatment options are available. It is administered once weekly due to its extended half-life, making it an excellent option for outpatient parenteral therapy (OPAT) and the discharge of stable patients. Currently, no human data are available, and animal studies did not show adverse embryofetal outcomes in rats and rabbits. 38 Clinical human data are needed to evaluate the risk during pregnancy and to provide a recommendation for use. Figure 3 summarizes the key information for this newly approved agent.
Chemical Structure and Key Features of Rezafungin (Figure References 2).

Polyenes
Conventional Amphotericin B, Liposomal Amphotericin B, and Lipid Complex Amphotericin B
Amphotericin B causes pore formation in the fungal cell membrane by binding to ergosterol, ultimately leading to cell death. It is highly protein-bound and extensively distributed into tissues. Amphotericin B has broad-spectrum coverage against many fungi, including Candida (except Candida lusitaniae), Cryptococcus, Aspergillus species (except Aspergillus terreus), Mucorales, and dimorphic fungi. 39 Amphotericin B is available in three formulations: Conventional, lipid complex, and liposomal amphotericin, with the latter two having less nephrotoxicity and infusion reactions than conventional. For many years before the introduction of echinocandins, amphotericin B was used as a first-line treatment for various invasive fungal infections. With the introduction of echinocandins and extended-spectrum azoles, which provided broad coverage and a better safety profile, the use of amphotericin B was limited to Central Nervous System (CNS) infections and to cases resistant or refractory to other agents. However, in the case of pregnancy, amphotericin B remains the first-line for many serious systemic fungal infections. 39 This safety may be attributed to two factors: Limited placental transfer, resulting in low direct fetal exposure, and a mechanism of action that does not inherently target mammalian developmental pathways. 40 Despite this safety profile, a question remains about the dose recommended during pregnancy, as it is based on body weight. O’Grady et al. reported a case of mucocutaneous leishmaniasis in a pregnant patient treated with 5 mg/kg/day (ideal body weight) for the first week, followed by weekly 4 mg/kg (adjusted body weight) and concluded that using this approach of perfect body weight deserves and adjusted body weight to be further studies in large patient population in pregnant women to confirm a solid recommendation. 41 Further, the use of amphotericin B during pregnancy and the postpartum period was reported for the treatment of cryptococcal infection in HIV-infected women. 42 They identified 19 women, including 13 pregnant women, one who was breastfeeding, two with recent miscarriages, and three within 14 days postpartum. Twelve women had cryptococcal meningitis and received amphotericin B deoxycholate at a dose of 0.7–1.0 mg/kg. The maternal survival rate was 75%, whereas the neonatal/fetal survival rate was 44% among surviving mothers. In addition, miscarriages and stillbirths were common, indicating good maternal outcomes but poor fetal outcomes for cryptococcal meningitis treated with amphotericin B. However, a significant limitation of this case study series is the lack of complete clinical information on treatment and maternal/fetal outcomes. The decision to use amphotericin B during pregnancy is based on the patient’s type of infection, severity, and the need for systemic antifungal therapy. Similar to non-pregnant patients, amphotericin B requires careful monitoring of side effects and electrolyte abnormalities and correction whenever necessary. In a recently published case report of intra-amniotic Candida infection treated with high-dose liposomal amphotericin B, they measured maternal and cord blood concentrations and reported cord levels >30-fold lower than maternal plasma levels. The mother delivered a healthy preterm neonate, which confirms previously published evidence. 40 Overall, amphotericin B is considered the standard of therapy when treating invasive fungal infection in pregnant women, as we have decades of use without reported malformation patterns. The main fetal risk is indirect, via maternal nephrotoxicity and metabolic derangements, and not structural malformation.
Allylamines
Terbinafine
Terbinafine’s mechanism of action involves inhibiting squalene epoxidase, leading to squalene accumulation and ergosterol depletion. It is highly lipophilic, with a high volume of distribution and a long terminal half-life. Terbinafine is used to treat onychomycosis and tinea infections. This agent is associated with multiple drug–drug interactions that should be carefully reviewed before initiation of therapy. 43 Published human data on the use of terbinafine during pregnancy are limited; however, no evidence of toxicity has been observed in animal studies. 44 A registry-based cohort study published in 2020 explored the safety of oral terbinafine in 891 exposed cases among 1,650,649 pregnancies. 45 They evaluated the risk of major malformations and spontaneous abortion and concluded that oral terbinafine use during pregnancy showed no increased risk of either. Nevertheless, systemic therapy for onychomycosis and tinea infections is generally not considered first-line during pregnancy, which limits the clinical use of this agent because these conditions are its only two approved indications.
Antimitotic Antifungals
Griseofulvin
Griseofulvin inhibits fungal cell mitosis at metaphase by binding to human keratin, making cells resistant to fungal invasion. It is used to treat onychomycosis and tinea infection. Most reviews recommend avoiding griseofulvin during pregnancy, especially in the first trimester. This recommendation is based on evidence of teratogenicity from animal studies showing growth restriction and on a population-based case-control study that found a strong signal for overall major malformations. 1 Therefore, it is recommended to avoid it during pregnancy, especially in the first trimester. Similar to our recommendation against systemic terbinafine for onychomycosis and tinea infections, which is generally not first-line during pregnancy, this limits the clinical use of the agent because these conditions are its two approved indications.
Triterpenoid Antifungals
Ibrexafungerp
It is a first-in-class triterpenoid antifungal that inhibits the enzyme β-(1,3)-D-glucan synthase, leading to increased permeability of the fungal cell wall and cell lysis. It was approved in 2021 for VVC and in 2022 for RVVC. 46 Although the mechanism of action is similar to that of echinocandins, they do not share the same binding site, which is considered an advantage because it leads to limited cross-resistance. It is active against Candida albicans and other Candida species, including C. krusei, C. glabrata, and C. auris (Candidozyma auris). Ibrexafungerp is contraindicated in pregnancy with an FDA black box warning due to the risk of teratogenicity that was reported in preclinical animal studies. Accordingly, it is recommended to use effective contraception when a woman of childbearing potential is on treatment and for at least four days after the last dose. 47 There have been two phase III clinical trials comparing ibrexafungerp versus placebo. Among these trials, three pregnancies were reported, two resulted in live births with no teratogenicity or complications, and one was electively terminated at 12 weeks of gestation. Nevertheless, given the lack of human data and the teratogenicity observed in animal studies, the FDA has required a postmarketing study of the effects of ibrexafungerp on pregnancy and fetal development, which is expected to be completed in 2029.47,48 Figure 4 summarizes the key information for this newly approved agent.
Chemical Structure and Key Features of Ibrexafungerp (Figure References 3).
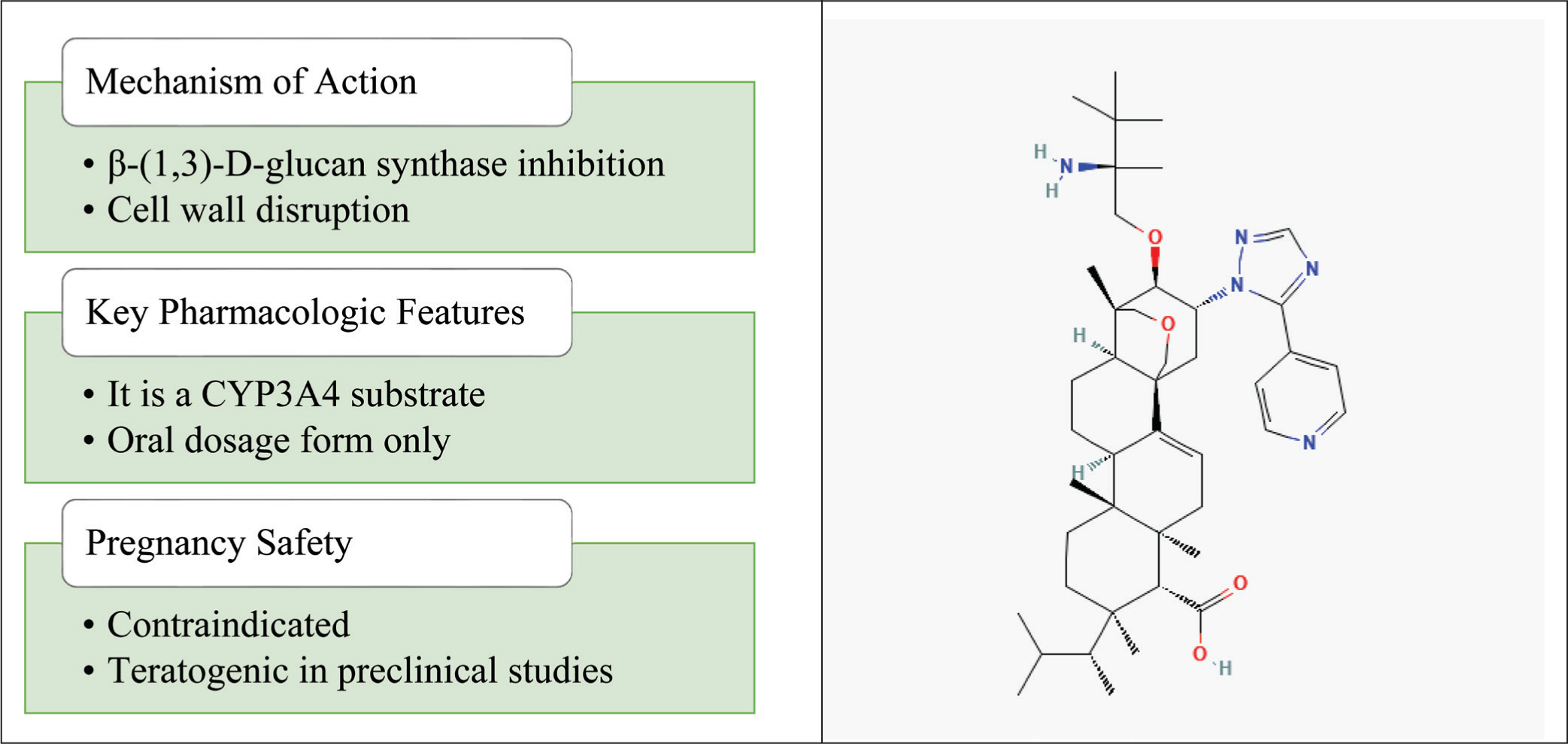
Figure 2. Chemical structure reference of oteseconazole: National Center for Biotechnology Information (2026). PubChem Compound Summary for CID 77050711, Oteseconazole. Retrieved January 17, 2026 from Figure 3. Chemical structure reference of rezafungin: National Center for Biotechnology Information (2026). PubChem Compound Summary for CID 78318119, Rezafungin. Retrieved January 17, 2026 from Figure 4. Chemical structure reference of ibrexafungerp: National Center for Biotechnology Information (2026). PubChem Compound Summary for CID 46871657, Ibrexafungerp. Retrieved January 17, 2026 from
Antimetabolite Antifungal
Flucytosine
Flucytosine is converted inside fungal cells to 5-fluorouracil, which then inhibits Deoxyribonucleic Acid (DNA) and RNA synthesis. It is active against Candida species and Cryptococcus species, but it is mainly used in combination therapy for the treatment of cryptococcal meningitis. 49 Animal studies have shown developmental toxicity when used in the first trimester, including growth retardation and congenital malformation. 49 Given the absence of human studies evaluating flucytosine exposure during pregnancy, the teratogenicity reported in animal studies, and the limited clinical indications for use, it is recommended that this agent be avoided during pregnancy.
Current Systemic Antifungal Safety Profile and Future Directions
Given current evidence, amphotericin B is considered the first-line agent for the treatment of many invasive fungal infections, despite its associated side effects. The availability of a safety profile during pregnancy, and the absence of evidence of teratogenicity or harm to the fetus, support the use of amphotericin B. In contrast, avoiding systemic azoles in pregnancy is recommended, especially during the first trimester. In addition, although echinocandins are among the most widely used antifungals for the management of invasive candidiasis, they are not recommended during pregnancy due to limited human data and animal studies indicating teratogenicity.
The introduction of new antifungal agents has advanced the management of fungal infections by providing agents with extended coverage, new sites of action, and unique pharmacokinetic properties; however, these agents are not recommended during pregnancy. Preclinical data demonstrating the teratogenicity of oteseconazole and ibrexafungerp have prevented their use, whereas the absence of human data for rezafungin precludes definitive recommendations for use until further data are reported. The current systemic antifungal safety profile in pregnancy, identified by trimester based on available human data, animal studies, and product labels, is presented in Table 4.
Antifungal Safety in Pregnancy, Identified by Trimester Based on Available Human Data, Animal Studies, and Product Labels.

Generally considered acceptable based on available human data.
Use with caution: limited or conflicting human data; use only if the benefit outweighs risk.
Avoid/contraindicated due to evidence of teratogenicity or safety concerns.
The traditional approach, relying on the FDA adverse event reporting system, passive post-marketing surveillance, published case reports, case series, or retrospective studies, and subsequent categorization of systemic antifungal safety in pregnancy, has inherent limitations in real-world settings. Accelerating research in the field using novel methods is promising, and emulated target trials are a new epidemiological approach that uses electronic health records and registries to evaluate drug safety. It can reduce immortal-time bias and enable trimester-specific risk estimation. In addition, estimating fetal systemic antifungal exposure without fetal sampling, using placental models, and physiologically based pharmacokinetic modeling during pregnancy, will help classify maternal and fetal risk, as human outcome data are scarce, especially for evaluating the safety of new systemic antifungals. Furthermore, using accumulated data from maternal prescription records, birth defect registries, neonatal Intensive Care Unit (ICU) databases, and long-term developmental follow-up will enable cross-registry analyses to evaluate fetal structural malformations and functional outcomes. Final, synthesizing the emerging evidence beyond meta-analysis using Bayesian models can combine all available data sources to estimate the probability of specific major malformations.
Conclusion
The challenge of managing pregnant patients with systemic fungal infections remains unresolved, and newly approved antifungal agents have not yet been deemed safe during pregnancy. There is limited published information available about the safety of most systemic antifungal medications when used during pregnancy, particularly beyond the first trimester, and important developmental follow-up studies are also scarce. The paradigm for systemic antifungal use during pregnancy should be shifted from avoiding antifungal agents based on “absence of safety data” to informed use guided by updated evidence and recommendations, with the risks and benefits to the mother and fetus carefully weighed. In addition, further research and reporting are needed to advance cumulative knowledge on the safety of systemic antifungals during pregnancy.
Footnotes
Acknowledgements
Not applicable.
Author’s Contribution
The author made substantial contributions to conception and design, acquisition of data, or analysis, and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work. The author is eligible to be an author as per the International Committee of Medical Journal Editors requirements/guidelines.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Data Availability Statement
All the data is available with the author and shall be provided upon request.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study does not involve experiments on animals or human subjects.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable.
Use of Artificial Intelligence-assisted Tools
The author declares that they have not used artificial intelligence (AI) tools for writing and editing of the manuscript, and no images were manipulated using AI.