
Abstract
The health of people in a nation is a potential indicator of its development. Over and above that, the job performance of people involved in the delivery and facilitation of health care services within a nation reflects the actual health conditions in it. In developing countries, where a large chunk of the population lives in rural areas, the job performance of grass-roots health care workers gains significant importance in order to ensure effective and efficient delivery of health care services to the masses and marginalized communities. The present study takes the case of Accredited Social Health Activists (ASHAs) in difficult rural areas of India to identify factors that affect their job performance and suggests interventions through which it could be enhanced. Fifty-five ASHAs were interviewed and five focused group discussions (FGDs) were conducted. Additionally, triangulation was done by interviewing other stakeholders, while studying relevant documents. Through content analysis of these interviews and documents, this study identifies the demands, resources and stressors that affect the job performance of these important intermediaries in the health care supply chain (in the Indian context). The study also suggests policy-level decisions that could help in enhancing job performance of ASHAs by managing demands, increasing resources and reducing stressors.
Key Messages
We have developed a model that delineates the demands, resources and stressors that affect job performance of women workers in rural India.
We have studied Accredited Social Health Activists (ASHAs) who are part of community health care sector. However, our findings are applicable to a wider set of similar job roles.
We have studied the nuances of factors affecting job performance for a category of community health care workers who are not full-time employees, have received minimal training and work in close proximity of their residence in a closely knit society.
We have looked at job performance of ASHAs who are women community health workers, with low educational qualifications, based in rural setting of a developing country.
We have recommended policy implications that would aid in enhancing the performance of ASHAs and thus improve the health care situation in rural India.
Introduction
India is a country with varied geographical topologies, ranging from the Himalayas in the north to the Indian Ocean in the south. Its diversity in terms of climatic conditions also makes it unique; while on the one hand, it has regions with the highest rainfall in the world, on the other, it has one of the largest deserts too. In fact, this unique diversity at times poses a big challenge in making any unified approach to delivery of government services, especially as regards delivery of health care services. Then, there is the rural–urban divide, skewed in favour of urban-centric developments, which makes rural areas especially in difficult geographies a neglected phenomenon (Pandey, Singh, & Sohani, 2018). Difficult geographies are characterized by complex land terrains that are prone to natural calamities and have low access and visibility (Pandey & Singh, 2015). These peculiar coordinates collectively make delivery of any service in these areas a challenge. For instance, in Uttarakhand, which is a hilly Indian state (Ghanshala, Pant, & Pandey, 2013), delivery of health care services becomes very complex—be it in terms of resource availability (both human and infrastructure), their usage and/or their maintenance. As per the 2011 census, Uttarakhand had a rural population of 7,036,954 (69.77%); according to the State of Forest Report 2015, all 13 districts of the state are hill districts with 61.43% forest cover. Scarcity of resource is such that until the end of 2015 as many as 76 villages in the state had no electricity since 1947 (Yogesh, 2016). What is even more amazing is that for the first time in 69 years, a bus rolled into the Salpata village of Uttarakhand (Darshan, 2016). Moreover, given the hilly nature of the state, climatic disasters are frequent, causing immense damage to both health care personnel and infrastructure. The other difficult topologies in India include some other northern and northeastern states. Studies have shown, for instance, that the hilly terrains of Himachal Pradesh also prove to be an impediment in accessing primary health care (Goel & Mazta, 2006).
Localization of health care is therefore a requirement of utmost importance in these difficult geographies. It is in regions and topologies such as these that Accredited Social Health Activists (ASHAs) are key stakeholders of public health, having their presence even in the remotest of villages. Their job performance thereby is of utmost importance as it has implications at all three levels, namely individuals (ASHAs) at the micro level, their families at the meso level and the overall health care status of the village at the macro level. Interestingly, a comprehensive generic model was evolved from Pandey’s (2019a) integrative literature review, wherein job demands, resources and stressors have been identified, which go on to affect job performance in general. In the specific case of ASHAs, it has been observed that there is a need for proper contextualization with respect to addition, deletion and contextualization of these factors (Pandey, 2017, 2019a). The Job Demands-Resources (JD-R) model has been used in this study to identify and classify the factors that impact the job performance of ASHAs.
Job Demands-Resources Model
The JD-R model (Demerouti, Bakker, Nachreiner, & Schaufeli, 2001) segregates any working conditions into two distinct categories, namely job demands and job resources. Higher demands with low resources lead to a rise in stressors. The model is extended by studying the implications of the three on job performance. While ‘job demands’ refer to ‘those physical, psychological, social, or organizational aspects of the job that require sustained physical and/or psychological (cognitive and emotional) effort or skills and are therefore associated with certain physiological and/or psychological costs’, ‘job resources’, on the other hand, refer to ‘those physical, psychological, social, or organizational aspects of the job that are either/or functional in achieving work goals, reduce job demands and the associated physiological and psychological costs, stimulate personal growth, learning, and development’ (Bakker & Demerouti, 2007, p. 312). ‘Stressors’ are those that are neither demands nor resources, but factors that impede job performance.
Although extant studies have analysed job performance of community health care workers in the past (Naimoli, Perry, Townsend, Frymus, & McCaffery, 2015), a comprehensive study specific to lay health care workers serving in difficult rural geographies has been missing. It should also be noted that apart from explicit task performance, there are many latent and implicit contextual performance parameters (Motowidlo & van Scotter, 1994), which have not been looked into. Recent studies have started giving attention to the case of ASHA workers (Sarin, Lunsford, Sooden, Rai, & Livesley, 2016; Sarin, Sooden, Kole, & Lunsford, 2016); however, a comprehensive study on their job performance is still missing. This study tries to fill this lacuna; it attempts to identify latent factors that influence the job performance of lay health care workers and also suggests how their performances could possibly be enhanced through policy interventions, given the difficult terrains within which they work.
The next section introduces ASHAs in detail, followed by the method, analyses results, discussion and policy implications of this research study.
Accredited Social Health Activists (ASHAs)
Community healthcare takes health care services from classes to masses. India, a vibrant economy with more than a billion people has ‘health care for all’ as one of its major objectives, a herculean task in itself given its manifold diversities. Introducing health care to rural areas, leave alone to the difficult terrains, is a big challenge in terms of human as well as infrastructural resources (Rao, Rao, Kumar, Chatterjee, & Sundararaman, 2011). However, reaching out to the rural areas was an essential need, especially at the village level; hence, in 2005, the ASHAs, or ASHA workers as they are called in India, were formally institutionalized.
ASHAs are community health workers coming under the ambit of the Ministry of Health and Family Welfare (MoHFW), Government of India, as part of the National Rural Health Mission (NRHM). The Indian MoHFW describes them as ‘health activist(s) in the community who will create awareness on health and its social determinants and mobilize the community towards local health planning and increased utilization and accountability of the existing health services’. According to the July 2017 update on ASHA programme, there were about 8,77,535 ASHA workers (Update on ASHA Programme, 2017), representing an enormous pool of personnel warranting proper HR management systems and processes to be in place in order for them to work effectively and efficiently.
Regardless of their marital status, ASHA workers are primarily village women within the age group of 25 to 45 years. They are thoroughly trained by health care professionals deputed by the Central government. Their services are mostly sought in case of aiding in institutional childbirths in village hospitals; they are also expected to be involved in immunizing children, using first aid to treat basic illnesses and injuries, demographic record-keeping, improving village sanitation, and so on.
Method
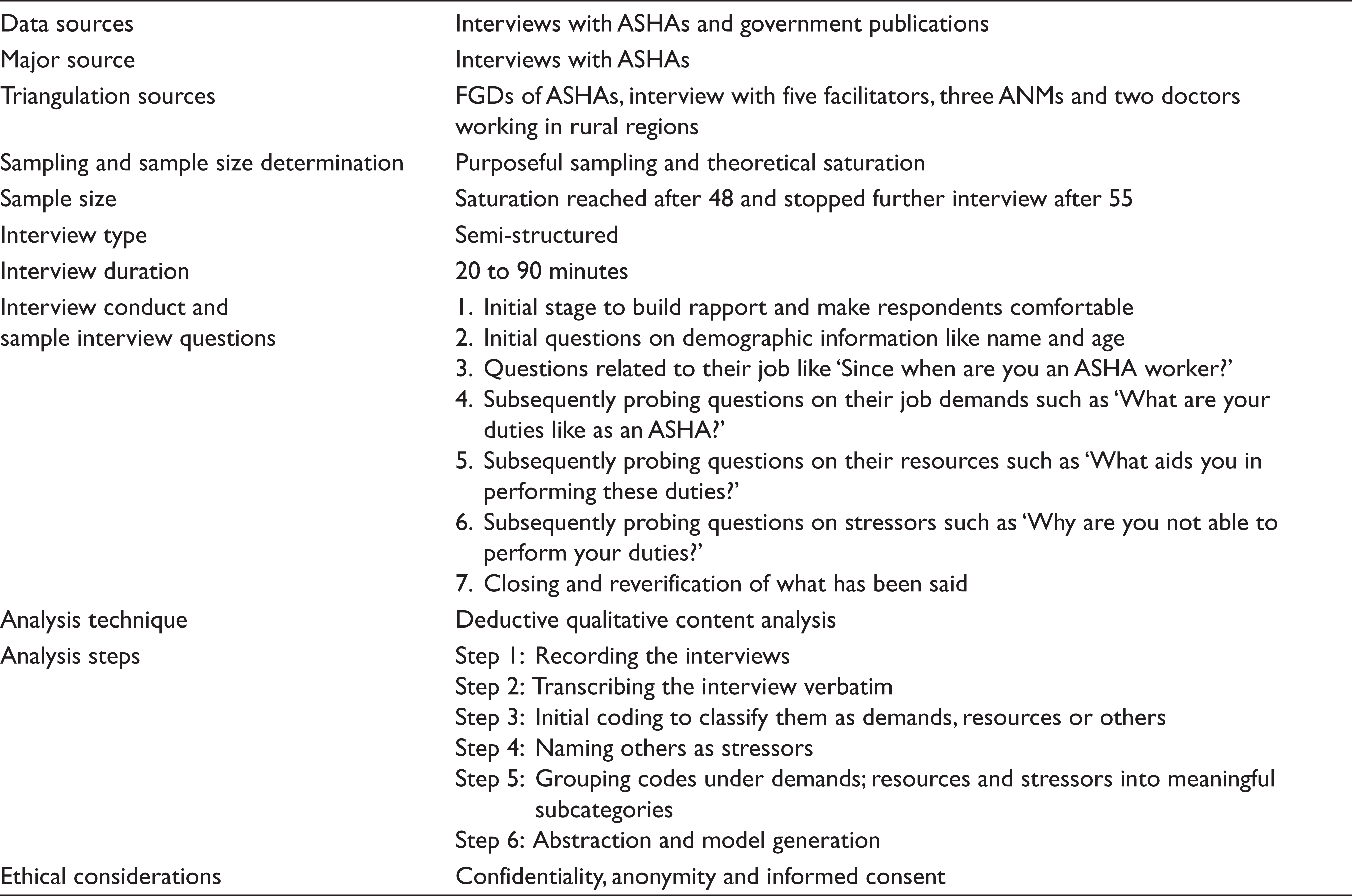
The detailed and exploratory nature of this research warrranted the use of qualitative methods (Lee, 1999; Locke, 2001). In order to understand the factors affecting the job performance of ASHA workers, it was imperative to consider their context and position in terms of socio- cultural and economic coordinates. This study thereby chose a multipronged approach wherein at first, the authors went through various documents of ASHA workers, which were available in the public domain (e.g., websites, govt. publications and newspaper articles), following which supervisors of ASHA workers along with officers from the MoHFW were interviewed. Additionally, the authors also attended multiple meetings with ASHA workers in order to develop interpersonal relationships with relevant stakeholders, these prolonged and critical for high-quality qualitative research (Lincoln & Guba, 1985). As the objectives set for the study were challenging, given the problems faced by ASHA workers, the authors preferred to verify their results and facilitate triangulation of their findings using five focus groups (Weick, 1995) for sense-making discussions. Each focus group had at least five members; such discussions assisted the authors in bringing out latent constructs. The medium of interviews was chosen as being the preferred instrument for qualitative study, as it helps in understanding motives, values, attitudes and beliefs (Richardson, Dohrenwend, & Klein, 1965); that apart, along with their congruence with observed verbal indicators (Gordon, 1975) it (i.e., the medium of interviews) also helps in blocking assistance or hindrance from others when answering (Bailey, 1987). Table 1 summarizes the method followed in the study.
Methodology
Interview Sample
Purposeful sampling (Lincoln & Guba, 1985) was the strategy followed to select respondents to get a representative sample, comprising of 55 ASHA workers and five FGDs. Additionally, in order to verify the findings gathered from the interviews and discussions, the authors also interviewed five facilitators, three auxiliary nurse midwives (ANMs) and two doctors working in rural regions.
Sample Size
Sample size in qualitative studies are generally smaller than that of quantitative studies due to the point of diminishing return of information, where additional data does not necessarily translate into additional information (Ritchie, Lewis, & Elam, 2003). A cautious approach to sample size is needed in qualitative studies, whereby the sample size must be balanced out to ensure that it is large enough to cover all important perceptions, but not too large to become repetitive and superfluous. The principle of saturation plays an important role in deciding thereby the sample size (Mason, 2010).
The selection of respondents followed a cyclic process where data was collected followed by the analysis that gave insights into selection of new respondents until saturation was reached (Glaser & Strauss, 1967) post interviewing/discussing with 48 participants and was totally stopped after 55 participants.
Data Collection
Data collection was done by using in-depth semi-structured interviews, with each interview lasting for about 20 to 90 minutes. The conversations were taped if permitted and transcribed verbatim when permission for recording was given, else it was transcribed directly during the interview. Initial questions included demographic information like name and age followed by questions related to their job—for instance, ‘Since when are you an ASHA worker?’ Subsequently, probing questions like ‘What are your duties as an ASHA worker?’ followed. The interviewer asked open-ended questions that had free-flowing answers and pointed questions that had to have a single response.
High ethical standards were maintained, whereby, right at the outset, the participants were informed about the objectives of the study and explicit verbal permission was obtained for conducting the interviews. Additionally, the authors gave assurance to the respondents that the interviews were solely for the purpose of research and not a government-sponsored exercise to evaluate them personally; anonymity was also assured and safeguarded in the analysis.
Analysis
The JD-R model (Demerouti, Bakker, Nachreiner, & Schaufeli, 2001) was used to classify the factors affecting job performance.
Content Analysis
Content analysis was used as a qualitative strategy to analyse data. This study chose to use the deductive approach to content analysis (Potter & Levine-Donnerstein, 1999), specifically with JD-R as the guiding theory as done in previous research (Pandey, 2019b).
In deductive content analysis, pre-existing models/theories aid in classifications and relationship development and thus are essential in the coding process (Hsieh & Shannon, 2005). In this study, it is the JD-R framework that aids in segregatting intial codes into demands and resources and also in the development of a new category of stressors.
Results, Discussion and Policy Implications
The ASHA programme has been well thought out in terms of its conceptualization, wherein the sociocultural coordinates of rural women are keenly looked into. For example, it is a common practice in India wherein married women live with their in-laws (usually) residing in a different village than their own. The ASHA programme acknowledges this displacement and, therefore, does not recruit unmarried women. However, there are other issues that need interventions of different magnitudes. From the JD-R model framework and stressors, three strategies may thus be adopted:
Decrease/Manage demands Increase resources Decrease/Manage stressors
The demands could either be explicit and/or implicit (i.e., hard or soft) in nature; however, these are not watertight compartments, that is, hard demands could have a component of soft demands and vice versa. Figure 1 presents this conceptualization.
Job characteristics like ‘physical effort’ have been reported to lower job performance (Kahya, 2007). The World Health Report (2000) notes, ‘performance (quality and efficiency) of a health system depends ultimately on the knowledge, skills, and motivation of the people responsible for delivering services’. So is the case with knowledge requirements (Zurn, Dal Poz, Stilwell, & Adams, 2004) and affective requirements like emotional labour (Goodwin, Groth, & Frenkel, 2011), all impacting the job performance at the end of the day. From the conservation of resource (Hobfoll & Freedy, 1993) perspective, all these demands involve the application of a specific resource, namely ‘physical demands’, which warrants the application of physical resources. ‘Cognitive demands’, on the other hand, require the application of mental resources; while ‘emotional demands’ take a toll on affective resources. Unexpected work hours make the quantum of resource applied to be higher when compared to normal settings.
Managing Demands
ASHA workers represent a very capable human resource whose presence at the village level could be harnessed to achieve many goals encompassing health care and other domains. They can be instrumental both for generating fresh data for policy formulation and for adjusting policies that have already been formed. Therefore, instead of decreasing demands, the focus should be on how these demands could be managed effectively and efficiently.
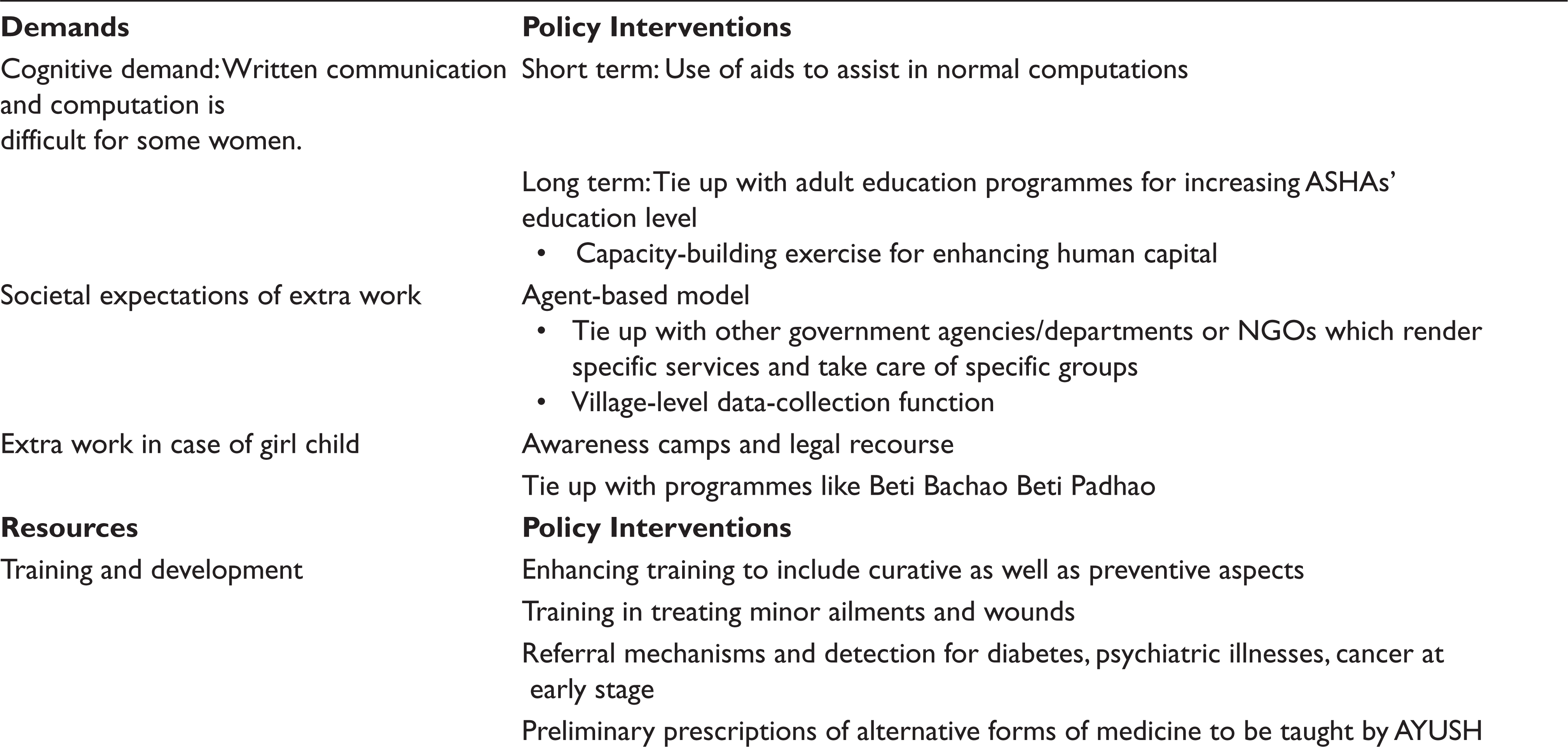
Against the given backdrop, physical and cognitive demands may be met by hiring ASHA workers who are physically fit; as regards ‘affective demands’, it may be developed through proper HR interventions (Pandey, 2018). Nevertheless, it is important to note that the ‘cognitive demands’ do require a certain level of proficiency in performing tasks like writing and counting. Though the minimum qualification for ASHA workers is 8th standard, many find it difficult to write and perform simple computation like addition or subtraction. Therefore, to deal with this demand, there could be two approaches: first, raising the entry-level educational qualification criteria for ASHA workers; second, facilitating open schooling system for ASHA workers so that they can complete higher education. This will not only raise education levels of the country at large, but also help ASHA workers perform optimally. Moreover, this could also be linked to adult education programmes like the National Institute of Open Schooling (NIOS). However, one must note that capacity building through education can be time-taking in terms of tenure, evaluation and declaration of results; job aids, which have proved to be beneficial in the past for enhancing the job performance of health care workers (Florez-Arango, Iyengar, Dunn, & Zhang, 2011; Jennings, Yebadokpo, Affo, & Agbogbe, 2010), could be used during this period. An example of job aid could be coloured chips/cards where each colour could indicate one ‘job task’, thus accounting for the number of job tasks done for different patients at the end of the month. As an ASHA worker has several ‘job tasks’ as part of his/her overall job performance, it is indeed crucial to keep a tab on how many of these tasks were actually done.

Expectations of villagers from ASHA workers are high and multifold; each stakeholder has some or the other requirement, (e.g., helping old people, taking people to visit hospitals, etc.). In order to meet up with these multifarious expectations, relevant ministries under the Central government could tie up with ASHA workers so that they could assist these groups in return for compensation. For instance, the National Programme for Health Care of the Elderly (NPHCE) along with the Ministry of Social Justice and Empowerment could possibly compensate ASHA workers for assisting the elderly. ASHA workers thus become relationship managers of these departments and act as bridges between these ministries and the rural populace.
‘Resources’ can be job related, work area related and related to a specific individual manifesting structurally, or perceived psychologically. Structural resources are directly job related, while psychological resources are more cognitive and/or affective in nature. However, these are not watertight compartments as stated earlier, that is to say, structural resources could possibly have a component of psychological resource and vice versa. Figure 2 shows this classification.
Training and development efforts, for instance, is a structural resource (Jha, Pandey, & Varkkey, 2018). The health department under the Central government have conducted multiple trainings and meetings to enhance job performance for ASHA workers. Past studies have shown that well-perceived training and development efforts lead to better evaluation of one’s proficiency whereby post training (Truitt, 2011) one performs better (Sparrow & Davies, 1988). The effects of training have also been observed to be enduring over time by field experiments as well (Frayne & Geringer, 2000).
Technology is another structural resource, which could revolutionize job performance, serving as an effective intervention to affect lives of both ASHA workers and villagers in difficult geographies. Take the case of mobile communication for instance; it has been a major catalyst in levelling out much of the information asymmetry in difficult geographies, especially under natural disasters. The technological acceptance model (Davis, Bagozzi, & Warshaw, 1989) thereby helps in understanding how ASHA workers accept and use technology to turn it into a valued resource for enhancing their job performance. Moreover, for the ASHA workers, mobile-based technological interventions are perceived to be user-friendly since (like everyone) they too use mobiles for communication and have no other means/resources available to them. Even if alternative resources exist, they are highly resource-intensive (in terms of both cost and time). Studies using this model on health care professionals like doctors with reference to telemedicine have shown good results (Hu, Chau, Sheng, & Tam, 1999).
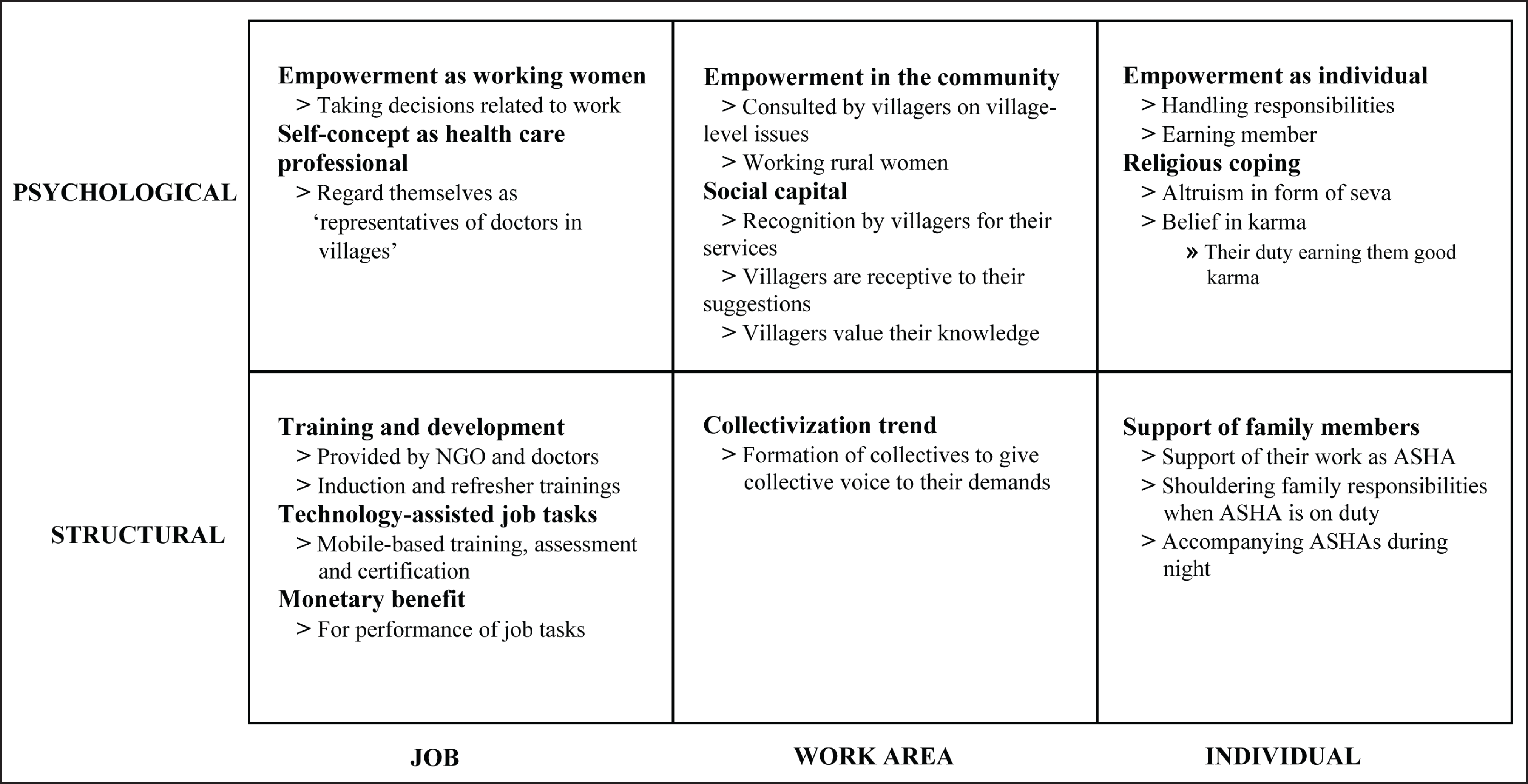
Collectivization has been a major outlet for providing a voice to the marginalized and distressed—collectivization at the workplace, houses unions and associations. The balance theory (Heider, 1958) of group formation provides insights into this trend, which primarily bases itself on the assumption that grouping tendency starts when people of similar attitudes come close to each other (Hummon & Doreian, 2003). These attitudes in terms of unionization trend could be defined as ‘work attitudes’. In the context of ASHA workers, this reflects their attitude towards their working conditions and benefits; a salient example of this is the strikes for fixed salary by groups of ASHA workers (Swathi, 2015). Collectivization also leads to empowerment like in the case of self-help groups in rural settings (Pandey & Roberts, 2012).
Family is highly important for ASHA workers and so is their work. The support provided by family members in terms of sharing family responsibilities, thereby enabling them (i.e., ASHA workers) to perform their job, indeed acts as a catalyst for fulfilling their job demands and enriching their work lives. Greenhaus and Powell (2006) defined this enrichment as ‘the extent to which experiences in one role improve the quality of life in the other role’ (p. 73). From the lens of enrichment theory (Greenhaus & Powell, 2006), the demands for the family sphere are shared by other actors in the sphere (family members), thus releasing resources that can be utilized for job performance on other domains.
Empowerment is one of the most important psychological resources (job-related) for ASHA workers, given the fact that they were previously homemakers, tied to their family and its well-being. Empowering social workers (e.g., ASHA workers) leads to gaining ‘knowledge, values and skills most likely to promote human rights and social justice’ (Turner & Maschi, 2015, p. 151). From an economic perspective, empowerment leads to a rise in economic activity rates, as well as a rise in the share of earned income, especially in the Indian context (Jayaweera, 1997). In an organizational context, studies in the past have shown ‘empowerment’ to be an important predictor of job performance (Chiang & Hsieh, 2012), which enhances job evaluation (Laschinger, Finegan, Shamian, & Wilk, 2001), especially in service settings (Hechanova, Regina, Alampay, & Franco, 2006).
Self-concept of ASHA workers as health care workers is a psychological one and originates because of their job roles and responsibilities. Moreover, self-concept is formed by ‘self-schemas’ (Markus & Wurf, 1987), which provide a basis for constructing the ‘self’ while identifying with others. The identification as ‘health care professional’ has its roots in self-schemas developed by ASHA workers as being representatives of the government health care department in villages, whereby health care professionals like doctors act as the reference group (Hyman, 1960) whom they (ASHA workers) want to emulate and in the process deal with higher demands.
Social support is another important workplace psychological resource for ASHA workers; it has been defined as ‘information leading the subject to believe that he is cared for and loved, esteemed, and a member of a network of mutual obligations’ (Cobb, 1976, p. 300). From a functional perspective, major functions of social support include providing instrumental or tangible support, emotional support, informational support, feedback support and social companionship (Cohen & Hoberman, 1983; House, 1981; Wills, 1985); these functions in turn are not mutually exclusive. The structural approach, on the other hand, looks at interpersonal relationships with relevant stakeholders within the social network (Ell, 1984; Lentjes & Jonker, 1985), e.g., friends, family, coworkers, etc. Additionally, social support provides positive experiences and helps avoid negative experiences to individuals in return for performing a few roles (Cohen & Wills, 1985). Actors in the social arena evaluate this embeddedness in roles and the support received reciprocates the quality and quantum of evaluation. Social support, thus, has also been conceptualized as a buffer for stressful events (Cohen & Wills, 1985).
Altruism refers to behaviours by an individual benefitting another who may not be closely related to her/him (Berkowitz, 1972). Psychological altruism is a type of motivatio that aims at improving others (Batson, 2010). Psychological altruism may therefore be considered as an individual psychological resource that helps ASHA workers to work for others despite other impeding factors. Further, since ASHA workers are married women, who have undergone pregnancy themselves or plan to do so, develop empathy with the beneficiaries, thus leading to the empathy–altruism hypothesis (Batson et al., 1991). The roots of altruism can also be traced in the religious beliefs of Indians (Pandey & Singh, 2016).
Increasing Resources
Training and Development Opportunities
Doctors are scarce; thus, capacity building of medical professionals is a very resource-intensive process (in terms of both time and money) requiring high levels of expertise. ASHA workers could be trained to treat minor medical needs of villagers. Moreover, as health care is not confined to curative aspects, preventive aspects are equally important and could be introduced. For instance, ASHA workers could be trained on alternative health care practices like yoga and Ayurveda, so that they could spread these health practices, thereby raising the standard of India’s rural health; the Ministry of Ayurveda, Yoga and Naturopathy, Unani, Siddha and Homoeopathy (AYUSH) would certainly have a vital role to play. Holistically speaking, ASHA workers could be introduced to two-pronged training: first, training on primary health care (e.g., treating minor wounds, administering injections, etc.); second, training on alternative ‘preventive’ practices such as yoga and Ayurveda (as discussed above). However, the flipside to this is that many of them are not so educated to understand the procedures; but this could be addressed by urging them to join the NIOS, as suggested above.
Technology-assisted Job Tasks
Technology could be leveraged upon as an important resource reducing the demands. For instance, today, to a large extent mobile phones have penetrated the rural markets; hence, mobile-based interventions could go a long way in solving problems. For example, instead of photocopying the health card of a pregnant woman, one could simply click a photo of the health card on one’s mobile—this saves both time and money. Similarly, digitization of patient records can also help ASHA workers. Hindi SMS-based reminder services about patient requirements (e.g., sonography, children’s immunization etc.) are some other avenues where technology could benefit the rural populace.
Enhancing Empowerment and Self-concept
Structural empowerment in terms of positions can lead to psychological empowerment, especially in rural settings (Pandey, 2016). ASHA programme has indeed been a major source of women empowerment, especially in rural India. Although this programme is the brainchild of NRHM, the Ministry of Women and Child Development through its programmes like National Mission for Empowerment of Women (NMEW) could serve as an additional aid. Further, the ‘self-concept’ of ASHA workers could be enhanced by positioning them as a more professional extension of health care services. The Central government could begin with small initiatives recognizing them ‘officially’ as health care professionals; for instance, giving them a uniform that would distinguish them from their friends and colleagues. Further efforts in these lines would also lead to an expansion of their psychological job resources.
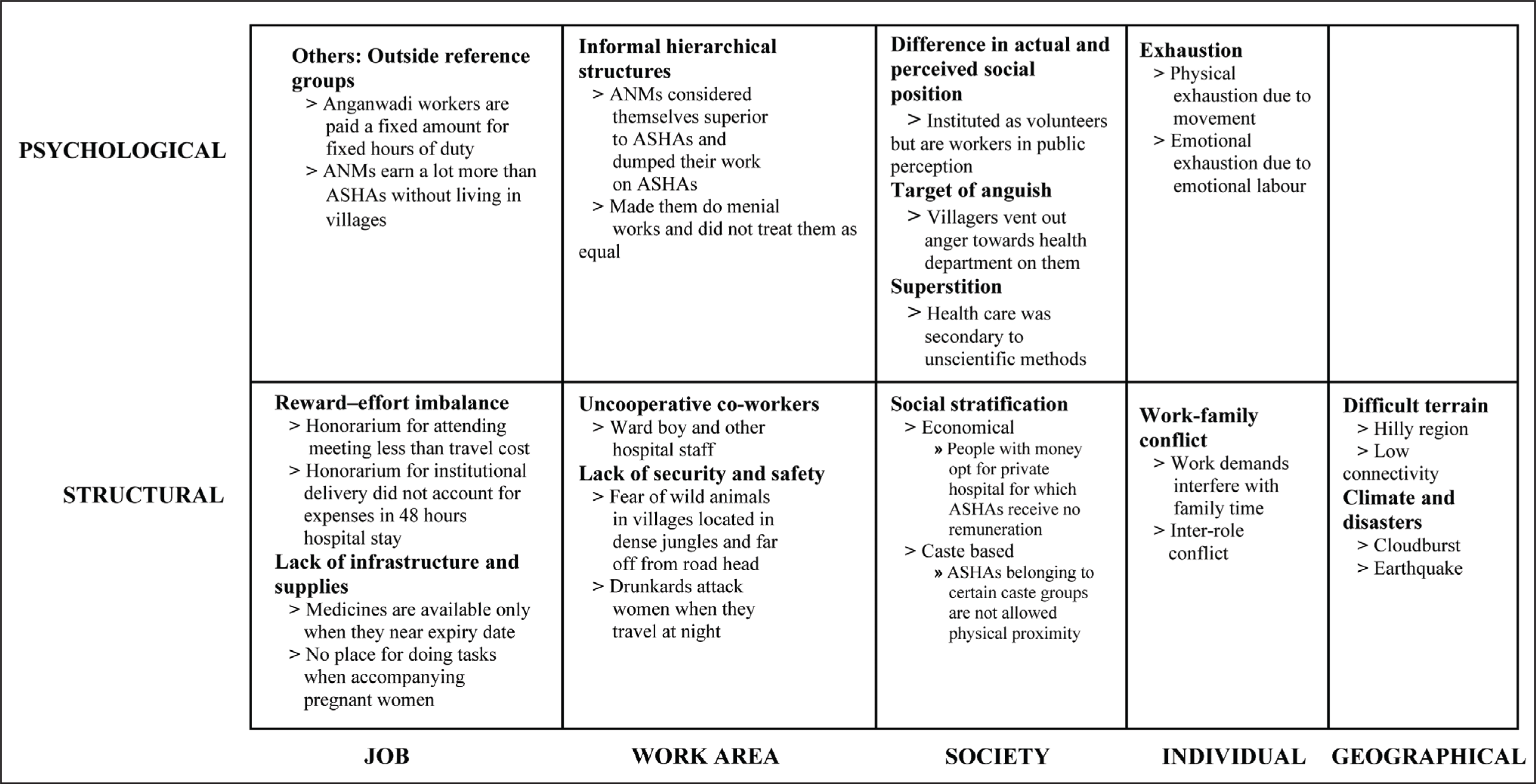
Stressors are manifold; they can be related to job, work area, society and/or geography. Stressors thereby affect individuals or groups and could be manifested structurally or could even be perceived psychologically. However, as mentioned earlier, these are not watertight compartments, that is to say, structural stressors, for instance, may have a component of psychological stressor and vice versa. Figure 3 shows this classification.
Individual-related structural and psychological stressors are work-family conflicts and exhaustion. Work and family are two major areas that any employee juggles through in her/his lifetime, whereby an individual needs to perform different sets of roles. Individuals are involved in many sets of ‘transitions’: physical transitions or ‘planned transitions’ (e.g., movement to the place of work); psychological transitions or ‘interposed transition’ (e.g., employee thinking about problems at work while in home) (Carlson, Kacmar, Zivnuska, & Ferguson, 2015) and transitions everyday between work and family domains (Hall & Richter, 1988). There are role boundaries, which act as conceptual delineations that help individuals manage expectations from each role (Ashforth, Kreiner, & Fugate, 2000).
An inter-role conflict between work and family spheres occurs when two roles are incompatible and/or one role influences the other. Work-family conflict is one such major inter-role conflict (Kahn, Wolfe, Quinn, Snoek, & Rosenthal, 1964) and has been defined as ‘a form of inter-role conflict in which the role pressures from the work and family domains are mutually incompatible in some respect’ (Greenhaus & Beutell, 1985, p. 77). Work-family conflict is studied as an employee-focused variable (Glaveli, Karassavidou, & Zafiropoulos, 2013) and draws upon the perception of an employee’s evaluation of the incompatibility of work and family demands, which in turn compete for the limited resources of an individual in terms of his/her cognitive, affective and physical resources (Greenhaus & Beutell, 1985). Work-family conflicts can arise due to time, strain and behaviours invested in one role that impede the performance of another role (Greenhaus & Beutell, 1985).
Studies in the past have demarcated the effect of family on work and vice versa, bringing out the direction of conflict to be a major factor. These two forms of conflict, namely work interference with family and family interference with work, are opposite in direction and are different from each other. Transitions from work to family and vice versa are thereby a prime source of stress. The transition of family to work occurs when an individual in his/her family time meets a work demand (Matthews, Barnes-Farrell, & Bulger, 2010); similarly, the transition to meet family demands during work time is referred to as work-to-family transition.
These variables are important as they are related to many work and health outcomes such as burnout (Brauchli, Bauer, & Hämmig, 2011), health satisfaction (Knecht, Bauer, Gutzwiller, & Hämmig, 2011) and life satisfaction (Glaveli et al., 2013; Rupert, Stevanovic, Hartman, Bryant, & Miller, 2012) to name a few. It has been studied as an important work-related stressor (ten Brummelhuis & Bakker, 2012).
The women who participated in our study were not trained professionals and, for many of them, this was their first job. Their work and family lives are not insulated; there is permeability of one role behaviour into another. Generally, women primarily handle household responsibilities (Pleck, 1985) and this phenomenon is more prevalent in India; thus their lives are anchored at their homes. Traditional expectations from Indian women are that they would take care of the family; therefore, causes for work-family conflicts seem to be more pronounced in the case of Indian women (Eby, Casper, Lockwood, Bordeaux, & Brinley, 2005; Grandey & Cropanzano, 1999). For working women, the work and family demands become incompatible, thus leading to work-family conflict (Tone Innstrand, Melbye Langballe, Falkum, Espnes, & Aasland, 2009).
Exhaustion is linked to professions that involve caring, teaching, nursing, etc. ASHA workers, like nurses, work in close proximity to people who are in need of health care services and are, thus, more exposed to stress. Researchers in the past have tried to refine and adapt the definition of burnout to ‘a debilitating process that robs individuals of their enthusiasm, destroying initiative and motivation, and ultimately depriving the organization of the full contributions of a valuable employee by consuming physical and psychological energy that is now unavailable for other uses’ (Stevenson, 1994, p. 350). Some others have defined burnout to a ‘degree of physical and psychological fatigue and exhaustion experienced by the person’ (Kristensen, Borritz, Villadsen, & Christensen, 2005, p. 197). The emphasis on ‘degree’ exists because it is tough to distinguish between people with burnout and people without (Shaughnessy & Moore, 2010).
In the context of health care exhaustion, ‘burnout’ thereby becomes a very important variable; it impacts the quality of service and care provided, the level of job performance, turnover, absenteeism and the overall well-being of employees (Cherniss, 1980). Non-involvement in work and fatigue are products of exhaustion, which leads to a dip in effectiveness (Leiter, 2010). While studying Australian midwives, researchers found moderate to high burnout levels in 30 per cent of the sample, whereas the ‘personal’ aspect of burnout was reported high for 50 per cent of the sample (Jordan, Fenwick, Slavin, Sidebotham, & Gamble, 2013). The burnout rate for orthopaedic surgeons in Australia is seen to be in the range of 50–60 per cent higher than general surgeons. The source of their burnout was a combination of both subjective and objective factors; the latter consisted of caseload, practice setting, while the former included perceptions that career was unrewarding, lacked autonomy, etc. (Arora, Diwan, & Harris, 2013). These subjective and objective factors also exist for ASHAs as per our findings.
Every job has certain demands for which the performer is required to put in some effort for which s/he is rewarded. The effort–reward imbalance model (Siegrist, 1996) provides insight into a situation of imbalance. Efforts represent job demands, whereas rewards, given by an employer (and by society at large), encompass monetary as well as non-monetary (esteem and job security) benefits (van Vegchel, de Jonge, Bosma, & Schaufeli, 2005). A job that includes high efforts coupled with low rewards is said to be one with ‘reciprocity deficit’ and would lead to stress (de Jonge, Bosma, Peter, & Siegrist, 2000). In the specific case of ASHA workers, there is certainly an imbalance of the effort required to perform various job demands vis–à-vis the meagre monetary benefits in doing them.
Proper infrastructure and supplies are essential for effective job performance. Performance in itself has been studied earlier, whereby it was found to be impacted by the availability of infrastructure, equipment and support systems (Zurn et al., 2004). The World Health Organization’s (WHO) report on improving performance of health care workers also identified the availability of infrastructure, medications, supplies as part of positive working conditions, while their deficiency was related to poor performance of health care workers (Marjolein & Harnmeijer, 2006). This scarcity of infrastructure and supplies is prevalent even for ASHA workers, especially in difficult geographies.
Reference group comparisons are common in jobs, they dictate ‘how’ we evaluate employees based on their work outputs and inputs. The equity theory (Adams, 1963a) provides an insight into this phenomenon, especially inequity in terms of wages (Adams, 1963b). The theory posits that people compare their inputs in terms of efforts and outputs in terms of rewards in a job with those of others called reference groups. The four reference groups are her/his position in a different job within the same organization, that is, self-inside; her/his own position in the same job in a different organization, that is, self-outside; other person’s positions within her/his organization, that is, others-inside; and finally, other person’s job in an outside organization, that is, others-outside. A comparison, which indicates that inequity leads to stress, which in turn leads to lower productivity and quality of work (Lawler, 1968). For ASHA workers, Anganwadi workers are an others-outside reference group with which they can identify with. Anganwadi workers are isomorphic to ASHA workers in terms of socio-economic and cultural coordinates and, hence, the comparison is more pronounced. The predictable work hours coupled with fixed remuneration of Anganwadi workers as ASHAs in the same village is a source of stress for ASHA workers.
Social stratification leads to the creation of groups in society that are evaluated based on their positioning in the social hierarchy. One such schema for classification that is widely prevalent in rural India is the caste system (Pandey & Varkkey, 2017). Each caste in this schema is evaluated differently and, thus, the society dictates the planned behaviours with these groups. In the case of ASHA workers, who belong to the lower strata of the society, there are these beliefs about them in the minds of beneficiaries, which lead to behaviours that hinder their performance; for instance, not allowing them inside our homes and still soliciting their services. Similar is the case with superstitions, which are beliefs that have been formulated since time immemorial; this too impedes the performance of ASHA workers by soliciting non-scientific management of diseases.
The social position of an individual determines how others treat him/her for which his/her occupation/profession is a vital determinant; it has associated rewards (monetary as well as non-monetary) and expectations too (Macintyre, 1986). Given this backdrop, studies have shown that social position thereby often becomes a source of stress (Moore & Cunningham, 2012). For example, a government officer in India has a high social standing and enjoys high social security and benefits thereof; thus, people instinctively expect such an individual to perform according to his position. In the case of ASHA workers, though they are volunteers, they are perceived to be government employees enjoying various government benefits (as mentioned above); thus, there are high expectations from them, which involve tasks beyond their explicit requirements. These differing perceptions lead to dissonance among ASHA workers, leading thereby to intra-role conflicts (Katz & Kahn, 1978) in their jobs. Role conflict in itself is believed to be promoting stress and negatively affecting job satisfaction and job performance (Miles & Perreault, 1976; Mohr & Puck, 2007). The differing demands for a volunteer and paid worker are a source of this stress and thus impede job performance.
Difficult terrains have been acknowledged to be a major impediment in the delivery of health care (Spencer, 1999), as hilly and difficult terrains lead to unequal distribution of health care services in these areas when compared to plains (Coady, Clements, & Gupta, 2012).
Decreasing/Managing Stressors
Diminishing the Reward–Effort Imbalance and Others-Outside Comparison
A related issue is that of rewards and effort imbalance; though ASHA workers perceive the work as a ‘voluntary service’, their rewards in terms of monetary compensation is certainly not commensurate with their efforts. This not only leads to dissatisfaction with the service but also sets a negative evaluation of the work done by ASHA workers by their own family members. Reward in terms of monetary compensation is way below what they would earn if they were to engage in other productive works, for example, working in fields, taking care of livestock, etc. The rewards therefore must be adjusted to their effort; for instance, the remuneration paid to them for attending monthly meetings is ₹150/-. While it is true that those ASHA workers living close to the meeting venue have no travel expense, the ones who live in the peripheries effectively pay up more than they actually earn.
Recognizing ASHA workers as ‘formal employees’ would help them in getting a salary and, in the process, would lead to the strengthening of the marginalized section of society. A compensation structure similar to Anganwadi workers would also bring in acceptability of the job with both the family members and villagers alike, reducing thereby work-family conflicts and increasing family support. It would also bring down the others-outside comparison and clarify their perceived social position with villagers in conjunction with other health care workers. However, here too there are concerns of a few ASHA workers being free riders; nevertheless, proper checks and balances through facilitators could curb this problem. A principal agent-based model could be developed, where a part of the payment is fixed and another part is dependent on performance. ASHA workers in West Bengal, for example, get a fixed salary per month borne by the state government (PTI, 2013). The Centre and state’s partnership in this regard would certainly be a good way forward.
There are also other difficulties, which specifically ASHA workers under rugged geographies face; these have not been thought of by policymakers, neither have they been highlighted before the policymakers and thus have not been compensated by the government. As a solution, ‘zoning’ could be done to account for specific difficulties that ASHA workers of a particular zone face, e.g., difficult terrains, fear of wild animals, etc., wherein they could be compensated accordingly.
Structuring of Work and Resources
Structuring of duties of ASHA workers is equally important to eliminate jobs that can be effectively done by others. For example, a hospital stay for 48 hours after child birth leads to detrimental performance of ASHA workers and also creates a clutter in the hospital. Rather, there could be a centralized approach where a single individual could possibly be delegated to perform these duties; thus, instead of multiple ASHA workers staying in the hospital, only one stays and offers these services.
The ‘Yashoda’ programme in Rajasthan 1 nd ‘Mamta’ in Bihar prove to be good models for structuring such a programme. ‘Yashodas’ are primarily placed at district hospitals, where the footfall of pregnant women is relatively higher and in their job roles they deliver care and support to newborns and their mothers during their stay at these facilities (Varghese & Beena et al. 2014). There could be a system where ASHA workers hand over the responsibility of a new born to Yashodas and take over the charge after discharge from the hospital.
Shortage of medicines is another hurdle that ASHA workers face; therefore, inventory management practices need to be improved, so that ASHA workers receive adequate medical supplies regularly as opposed to being given a stock once a year. Additionally, there is also the issue of dumping medicines nearing expiry dates, which must be checked. Structuring of roles and responsibilities with respect to other players in health care like ANMs and Anganwadi workers must be done to avoid duplication of efforts, as well as to avoid conflicts and victimization.
Dealing with Geographical Factors and Exhaustion
Difficult terrains warrant extra effort on the part of ASHA workers; this should be stated explicitly during the selection process. As their work could involve climbing mountainous regions, those with sturdy legs without any joint problems should be selected. Further, the ‘one shoe fits all’ approach in rationalizing honorarium has to be rationalized. For ASHA workers operating under extremely difficult geographies, there should be special allowances, like hill compensatory allowance. There could also be an attempt to tie up with state disaster response teams, who could also teach them the necessary skills to deal with natural disasters.
Ensuring Security and Safety at Work Area
Jobs of ASHA workers, especially at night, involve a certain level of risk; the Central government being the ‘de facto employer’ of these women is thereby obligated for arranging security measures. For example, in areas with wild animals, a ‘risk allowance’ could be instituted; additionally, a second person could be there to accompany the ASHA worker at night. Similarly, in areas with high proneness to violence and crime, ASHA workers could be provided police protection. Sexual Harassment of Women at Workplace (Prevention, Prohibition and Redressal) Act, 2013 provides for the safety of women; therefore, it should be applicable even in the case of ASHA workers.
Dealing with Societal Problems
Most of the social problems exist since long; thus, a quick fix solution is certainly not possible. One needs to have a three-pronged approach to deal with this issue: (a) train ASHA workers to deal with these problems (legally as well as through persuasion), (b) raise awareness by collaborating through existing programmes and (c) form support groups that would help ASHA workers in case of any difficulties.
Article 47 of the Indian Constitution states:
The State shall regard the raising of the level of nutrition and the standard of living of its people and the improvement of public health as among its primary duties and, in particular, the State shall endeavour to bring about prohibition of the consumption except for medicinal purposes of intoxicating drinks and of drugs, which are injurious to health.
However, alcoholism for instance, is still a peril in rural India; therefore, the scheme for Prevention of Alcoholism and Substance (Drugs) Abuse should be strengthened there.
Societal problems of caste also need to be addressed. Article 17 of the Indian Constitution seeks to abolish ‘untouchability’ and forbids all such practices; the Scheduled Caste and Scheduled Tribe (Prevention of Atrocities) Act should therefore be strengthened to curb discriminatory practices.
Article 51A(h) of the Indian Constitution states, ‘to develop the scientific temper, humanism and the spirit of inquiry and reform as a fundamental duty for every Indian citizen’. Superstition, in rural India may be curbed at the village level by conducting awareness camps and by handing out an interdict to people who promote magical remedies through Drugs and Magic Remedies (Objectionable Advertisements) Act.
As per the Census of 2011 in India, there were 940 females per 1000 of males. The girl child has been neglected in rural India due to a lack of awareness, common practice of dowry and low career prospects. However, the government’s efforts to minimize this discrimination has manifested through various programmes and policies, which in turn must be made known to the rural populace. ASHA workers could be a carrier and disseminator of such information. Beti Bachao Beti Padhao scheme is one such scheme with objectives of (a) ‘Prevention of gender biased sex selective elimination’, (b) ‘Ensuring survival & protection of the girl child’ (c) ‘Ensuring education and participation of the girl child’ (‘Beti Bachao Beti Padhao’, 2018) can go a far way in bridging this gap.
Support groups could help ASHA workers deal with these stressors, thereby building a robust system of mutual help. It could also be a place where successful management practices of handling these stressors can be shared. Peer to peer learning has immense potential for cooperative learning for ASHA workers.
These recommendations at various levels would certainly lead to better job performance of ASHA workers; in the macro sense, they did provide better health care delivery in rural areas, especially under difficult geographies.
Tables 2 present these policy implications.
Policy Recommendations for Managing Demands, Enhancing Resources and Dealing with Stressors

Conclusion
The goal of ‘health care for all’ in India needs the incorporation of many more health care professionals, especially in rural regions (Garg, Singh, & Grover, 2012). Although ASHA workers, Anganwadi workers and ANMs exist simultaneously, their work/job roles have been segregated and made mutually exclusive, whereas they could effectively be mutually inclusive. For example, Anganwadi workers are more concerned with the problem of child hunger and malnutrition; ANMs do not reside in villages where beneficiaries of this service stay. ASHA workers could thereby prove to be a health care agent who could lead to reaching the last man at the last mile.
On paper, ASHA workers have been conceptualized as honorary health care volunteers; however, in practice and in public perception, they are no less than a worker per se. Their amount of work requires them to invest a significant portion of their time to this activity; this creates a perception in their villages that they have got jobs like Anganwadi workers. Moreover, they are seen as the face of the health department in villages and are often subjected to suggestions and complaints about the department. A policy-level decision thus needs to be pondered over as to how ASHA workers could be positioned in today’s progressive society going forward. A shift from the status of a volunteer to that of worker would have implications spanning economic, social and psychological domains. The provision for ANMs initially started as a short-term programme, but later they became permanent staff in the public health system (Mavalankar & Vora, 2008); the same could also be possible for ASHA workers.
Job performance as measured by monthly progress reports (MPRs) is only a partial reflection of what ASHA workers do. A new performance matrix that takes into account contextual performance and takes input from other stakeholders must be developed. Contextual performance dealing with softer aspects of a job per se have been stressed by other researchers as well (Bajpai & Dholakia, 2011); these must include regular feedback from supervisors and self on a monthly basis; while doctors, beneficiaries and other villagers could be included on a quarterly basis. A job performance report should be generated in order to provide developmental feedback to ASHA workers, which could be used to further improve their performance.
Footnotes
Acknowledgements
This paper is based on the doctoral thesis of the first author at Indian Institute of Management Ahmedabad. Other authors have contributed to shaping this paper as part of the thesis advisory committee members.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.