
Abstract
Health care organizations around the world are recognizing the benefits of maintaining electronic medical records for patients with improved quality of service, free flow of information (across multiple locations), reduced cost of operations resulting in cost efficiencies, better health and efficient utilization of resources. Recognizing these benefits as opportunities, health care providers have or are in the process of migrating from paper-based health care records to electronic medical systems. This transition is not always free from challenges. This study presents recommendations for managing challenges with data conversion from paper form to electronic database based on a case study done by students from Colorado Technical University, Colorado Springs, CO, USA, for a prominent eye hospital in Jalna, India, using appreciative inquiry. The Culture, Administrative, Geographic and Economic (CAGE) framework at the industrial level is applied to evaluate the options considered for data conversion and transition.
Introduction
An electronic medical record (EMR), also known as electronic health care record, is a computerized medical record rendered or created in a medical institution that provides systematic processing of files and proper organization of timed data for future use (Davis & Garets, 2005). Hospitals generate large amounts of paper-based data which result in growing cost of printing and publication, besides making it difficult to retrieve information. Hospitals embraced EMRs to address this problem, which would improve the data organization, communication, recording, retrieval and modification of medical records. In India, the importance of maintaining medical records and following the process and documenting the processes is at a nascent stage which requires a careful analysis of options available to meet the strategic goals of the hospitals considering EMR.
The success of EMR relies largely on how correctly and effectively the paper-based data are converted to an electronic database. This adoption requires a thorough analysis of data conversion to prevent data loss and interchange and also to maintain data security during and after conversion. While bigger institutions and hospitals are adopting procedures to follow documentation and record maintenance, smaller clinics and hospitals are yet to follow suit (Thomas, 2009), thus leaving a minimum to no medical records for the patients. EMRs would help small and bigger clinics and hospitals in India to fill the void in maintenance of medical records and also reduce the vulnerability of unauthorized access or getting destroyed due to improper storage (Godbole, 2009).
This case will show the processes involved in data adoption from about 500,000 paper-based data files to EMRs for an eye hospital in Jalna, Maharashtra (India). The study evaluates the methods of data conversion based on the CAGE framework (Ghemawat, 2007) and makes recommendations in context of the resources available with the eye hospital. Appreciative Inquiry (Whitney & Cooperrider, 1998) is used for determining the expectations from the EMR in general, desired goals and strengths of resources available with the eye hospital.
Background of the Study
The success of implementing EMR at the eye hospital depends on how paper-based data are converted to electronic database within a reasonable amount of time and cost. The effectiveness of this data conversion also determines whether the converted data is searchable and meets the requirements of the EMR being developed. The amount and type of data to be transferred would require significant resources that need to be managed following a process in order to meet the goals. Apart from financial investments, this initiative by the eye hospital would require time to carry out the project, information technology (IT) infrastructure which includes servers, user workstations, IT personnel and data security have to be revisited considering the sensitivity of EMR. The proposed EMR should be able to secure the data by providing authorized access through the interfaces for the users (Marcus, Lubrano & Murray, 2009), to protect confidential files such as DNA tests and HIV test results. The eye hospital estimates that the financial investment made will benefit the organization by reducing the operating cost such as reduced paperwork, data transfers, meals, test results and physical storage.
Statement of the Problem
At the eye hospital, patient records are maintained manually in a paper-based
record system. As a result of several years of operations, the number of records
has become huge which is posing difficulties in maintaining and retrieving
patient records. The eye hospital is considering EMR to make medical records
management more efficient. The implementation of an EMR system offers several
advantages which outweigh the challenges posed by the adoption. For a project of
this size and complexity, it is important for any organization to evaluate the
challenges and risks associated with the implementation of EMR and data
conversion. This study seeks to examine the implementation and data conversion
challenges; to offer recommendations and guidelines for implementation
processes; to evaluate the methods of data conversion and make
recommendations.
Purpose of the Study
The general purpose of the study is to evaluate the methods of converting paper-based data into an electronic database after considering the type, volume, quality and form of data to be converted. This study also aims to provide general guidelines for implementing a software system in an organization. The recommendations made by this study would benefit health care organizations considering transitioning to EMR. It would also benefit managers who can adopt the process guidelines from this study in situations involving system implementation in general.
Moving to EMRs has several benefits, including value added service to the patients while keeping costs down. However, a discussion of these benefits and the pros and cons of moving to EMR is not within the scope of this study. This study is focused on comparing the methods of converting data from a paper-based system to an electronic system and how this conversion can best be achieved without exceeding the available resources and meeting the eye hospital’s goals of being able to query patient history and medical records without needing to mine the data through a large number of paper documents.
Objectives of the Study
From the interviews and group discussions with the Human Resource Director and Hospital Director, this study has found that the eye hospital is expanding its operations by developing five new regional centres. Their goal is to meet or exceed the patient expectations by providing excellent services. Converting to an EMR system is one of the several initiatives being undertaken by the eye hospital to meet these goals.
EMR has gained popularity in the health care industry globally not only because of the cost savings which is estimated around $81 billion annually but also due to the improved efficiency in health care and safety, prevention and management of chronic diseases and other health and social benefits (Hillestad et al., 2005). Despite its usefulness, various challenges have marred the implementation of EMR by health care providers. In the developing world, scarcity of resources has placed a limit on the implementation of EMR systems (Fraser et al., 2005). In addition, prioritization of needs and environmental conditions has made EMR implementation lag in some countries (Fraser et al., 2005; Sood et al., 2008). More precisely, lack of developed infrastructure, workforce turnover, incompatibility and limited training continue to curtail EMR adoption (Williams & Boren, 2008; Ferreira et al., 2004).
In order to be prepared to face the challenges posed by converting to EMR, the
Colorado Technical University (CTU) team was asked to gather information and
provide guidance on converting the eye hospital’s paper-based medical
records to EMR. The purpose of this study was to help the eye hospital identify
the processes involved to successfully implement the EMR system and also to
identify the methods of converting paper-based data into a searchable electronic
database. The CTU team carried out the study with the following objectives to
meet the purpose of the study: Gather information about the present and future state of the
operations. Recommend general guidelines on system
implementation. Recommend methods of data conversion from paper-based records
to the electronic database.
Assumptions and Limitations
This study assumes that the participants have provided accurate information about the estimated amount of data to be converted. It is also assumed that the eye hospital has done a feasibility study for the implementation of EMR and that the needs of the hospital and patient care have been incorporated into the system. It is also assumed that the proposed system will support a bulk data entry feature. While evaluating the challenges and limitations of data conversion methods, this study was limited due to the limited availability of English-speaking participants. Due to time constraints, the research team could not evaluate the reporting needs in detail from the EMR that would have provided for a more accurate analysis of methods of data conversion to be used.
Literature Review
Introduction to EMR
An electronic medical record (EMR) is a computerized medical record rendered or created in a medical institution that provides systematic processing of files and proper organization of timed data for future use (Davis & Garets, 2005). Medical institutions have been working with a combination of manual and electronic systems to reduce the net operating costs for the hospitals (Garets & Davis, 2006).The EMR stands as the legal record created for hospitals and ambulatory environments thus being a source of statutory reporting for an inpatient’s or outpatient’s needs. These gathered data can be used for the transferring of information to other medical entities so as to build a medical record exchange improving the delivery of solutions which include medicine, workforce, machines and other medical needs (Garets & Davis, 2006). EMR has made significant inroads in various health facilities. An EMR refers to an automated environment that manages function such as order entry, clinical documentation and clinical support roles (Garets & Davis, 2006). Others define EMR as electronic records containing the patient’s information captured during medical visits.
Role of EMR
The primary role of EMR is to provide and maintain patients’ medical records. Scholars argue that EMR is also useful in reducing errors in health care services and promoting cost reduction strategies essential in limiting exhaustion of health care resources (Fraser et al., 2005). EMR is also vital in promoting the exchange of information that can allow evaluation of care in remote sites. Furthermore, EMR can also streamline the management of drugs and other communication needed within a health care environment (Fraser et al., 2005). These roles situate the need of EMRs in health care facilities such as hospitals.
Implementation of EMR
EMR implementation consists of modules such as patient health care records including laboratory reporting that provide reporting services to clinicians (Hersh, 1995). In addition, EMR can be implemented to combine data from various services such as radiology and pharmacy into usable services. This model of EMR implementation allows the integration of administrative, radiology, laboratory services, pharmacy, clinical documentation and computerized physician order entry. The modules work together as a single EMR system.
Benefits of EMR
Literature on EMR indicates that EMRs have many significant incentives. EMR allows sharing of patient’s records and their use for research work, unlike paper records (Hersh, 1995). EMR also streamlines management of hospital functions and processes, for example inventory of resources such as drugs (Fraser et al., 2005). Other benefits of EMR include reduced errors and improvement in the quality of service in health centres (MacKinnon & Wasserman, 2009). Improved patient participation is also another incentive of EMR use in health care centres (Ved, Agarwal & Pandya, 2011).
Challenges of EMR Implementation
Despite its usefulness, various challenges have marred the implementation of EMR by health care providers. In the developing world, scarcity of resources has placed a limit on the implementation of EMR systems (Fraser et al., 2005). In addition, prioritization of needs and environmental conditions have made EMR implementation lag in some countries (Fraser et al., 2005; Sood et al., 2008). More precisely, lack of developed infrastructure, workforce turnover, incompatibility and limited training continue to curtail EMR adoption (Williams & Boren, 2008; Ferreira et al., 2004).
Summary
The literature about EMT leaves no doubt that EMR offers several benefits to health care providers. EMR, comprising of modules that execute various functions within health care services, allows for the automation of processes. Therefore, EMR provides exchange of information, along with promoting safety and quality of care. Various implementations of EMR combine several functions into a system that health care providers rely on to store and retrieve data. EMRs have immense benefits despite challenges such as lack of resources and training. Nonetheless, providers can address these challenges by following processes which would address these challenges, for them to enjoy the full potential of EMRs.
Appreciative Inquiry
Appreciative Inquiry (AI) is the organizational development method that searches for the qualities that enhance the functioning of an organizational system (Thatchenkery 2005; Whitney & Cooperrider, 1998). It focuses on the effects that increase the overall development in a certain project, office, systems, methods, works, publication and laws (Hall & Hammond, n.d.). Since it is focused on the positive effects, it simply focuses on the terms ‘what will be’ or ‘what could be’. This will help to determine the total effects of the system in an institution.
According to Richard Seel (2008), appreciative inquiry can be focused on four ways of reporting: Discover, Dream, Design and Deliver. Miller, Fitzgerald, Murrell, Preston and Ambedkar (2005) also advocated a variant method of Discover, Dream, Dialogue and Design to place emphasis on concrete plan when distinguishing the AI processes (Miller et al., 2005). The AI process focuses on intervention activities, which work for the betterment of the organization. It is not to forget the limitations and liabilities, rather consider them to be the opportunities of the work thereof. This is also called the opposite of problem-solving: it aims to find better ways, not the right way (Cooperrider, 1990). A polarity map comparing AI to problem-solving results in building the strengths of both methods to deal with the opportunity and the realities of the situation (Miller et al., 2005).
The AI approach recognizes the role of the entire workforce in institutions including the president down to the lowest position in the organization. The AI intervention is used to augment trust, develop organizational alignment and meet expectations of plans. The method aims to create meaning by drawing from stories of concrete successes and lends itself to cross-industrial social activities. It is enjoyable and natural to many managers, who are often sociable people (Hall & Hammond, n.d.).
Project Management
Project Management Institute (PMI) has identified initiating, planning, executing, monitoring and controlling, and closing as the main processes within a project. A set of guidelines which includes inputs and outputs of each of these processes and the relationship between these processes has been clearly described (PMI, 2004). This study has evaluated the applicability of these guidelines to develop the process guidelines for EMR implementation at the eye hospital.
Methodology
This study used Action Research (AR) and Appreciative Inquiry (AI) to understand the needs, objectives and challenges of implementing an EMR system at the eye hospital. These methods helped the research team in discovering the scope of the EMR system, user concerns and expectations from the EMR system. The AI process revolves around finding what the strengths are, dialoguing where participants may answer questions like ‘What should be?’, and innovating where the participants would try to answer, ‘What will be?’ It follows a 4D cycle comprised of Discovery, Dream, Design and Destiny (Newparadigm, 2008; Whitney & Cooperrider, 1998). A case study on building a transcultural strategic alliance between a US multinational and an Indian family business by Miller et al. (2005) has shown that AIs are uniquely suited to deal effectively with challenges in building relationships, understanding, trust and collaboration (Miller et al., 2005). Due to time limitations, this study completed the Discovery process and only conducted limited Dream and Design phases of the 4D cycle with hospital participants.
The CTU team comprised of 18 students and 2 professors. Out of these, 3 students and 2 professors were at the hospital in India for five days. The process began with interviewing the HR Manager and Director of the Hospital. They were asked to explain the vision behind converting to EMR. They were asked to identify the departments and key positions within those departments who would either be involved in this conversion or will be affected by this change. The researchers did not have any influence in picking these participants. There was no pre-determined demographic preference of these participants other than asking for people who could speak and understand English. As a result, the participants were picked due to their ability to communicate with the researchers with or without the help of an interpreter. The researchers were still able to collect rich data in spite of the language barrier between them and the participants.
After considering process consultation and Action Research, Action Research (AR) through intervention using AI was chosen as the methodology for this case study. AR was chosen because of the need for actionable knowledge, which was to develop guidelines for implementing the EMR system and recommendations for converting paper data to EMR. AI kept in mind while framing questions where the focus was more towards the strengths and positive aspects of the current and future state. Based on the assumption that an organization changes in the direction of the studies, use of positive topic for inquiry helps to construct positive social realities and collaboration. The team used group discussions, interviews, evaluation of existing processes and documentation with a goal to bring a positive change, thus, to help in preparing the concerned departments to embrace technology in carrying out their activities, which currently depended on manual and paper-based processes.
Data Collection and Analysis
CTU students worked with 10 different departments within the eye hospital to provide information on EMR and the vendor, working with the hospital to get the necessary infrastructure including hardware and software to implement the EMR system. The India-based research team gathered information about the existing manual process of collecting and maintaining patient records and designed features of the proposed system. In addition, interviews and discussions with the participants were focused on obtaining information on the plans for migrating to the EMR system, transferring data to the EMR from paper-based records, amount of paper-based records to be converted, data entry skills, quality control and other resources available with the eye hospital and/or its vendor. The options for converting the paper-based health care records to EMR were evaluated based on CAGE framework (Ghemawat, 2007), which was applied at the industrial application level to find which options of data conversion would work best in the given cultural, administrative, geographic and economic environment.
It was found that the eye hospital had an estimated number of 50 or more users who saw and/or supported the large patient volume. On a daily basis, 100 new patients and 200 returning patients were seen in the following departments: registration, clinics (glaucoma, cornea, retina and paediatrics), consultation, the ward, Operation Theatre, optical/pharmacy counters, administration, business office, purchasing and the gift shop/store.
Methodology Check
The participants were involved in making the recommendations based upon the findings of the study, thus, eliminating the bias of the researcher or any other entity towards a specific methodology. The team used triangulation to validate the data collected (Maxwell, 2005) by comparing information received from multiple people in the same position and verifying the information received by the supervisors. The study also involved interviews with multiple people within the organization using similar questions to make sure that the information collected was coherent along with studying project documentation. When contradictory statements were found, follow-up interviews were made to clarify the contradictions. Meeting notes were sent back to the team in the United States for analysis and interpretation.
Interpretation
The study discovered some of the major concerns mostly related to conversion of paper-based patient records to an electronic database. The analysis was based on the amount of data to be converted and how far back did the hospital want the records to go in the EMR. The study addressed the type of records to be converted and the basis of classifying/identifying the records which would be converted. Also reviewed was how the system could be brought online before all the paper-based data was converted.
Present State
Since the start of the eye hospital in Jalna in December 1992, patient medical records were maintained manually using a non-electronic record keeping system in the form of paper records. Many of these paper-based records are in the form of handwritten script in Devanagari, a script used by many Indian languages such as Sanskrit, Hindi and Marathi (Malik & Deshpande, 2010). Over a period of time, the size of these paper-based records have reached challenging limits, causing delays and in some cases, failure to retrieve records. This has resulted in inefficient usage of employees’ time, loss of productivity and more importantly creating a bottleneck in improving the level of service to the patients (Figure 1).
Present State at the Eye Hospital
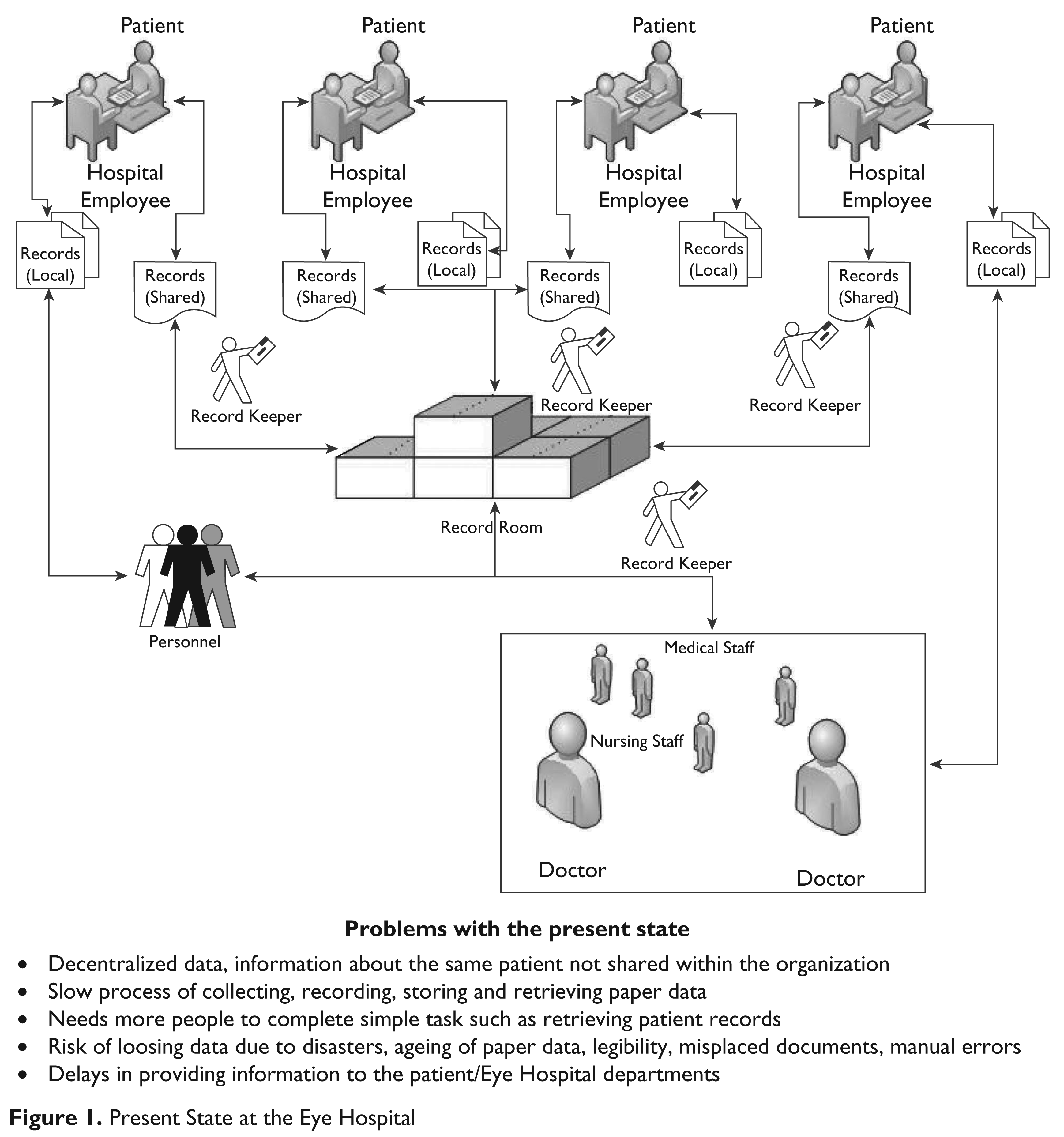
Due to lack of time, the CTU team could not gather information which would have helped the research team know if the paper-based system had any impact on the quality and cost of health care being provided to the patient.
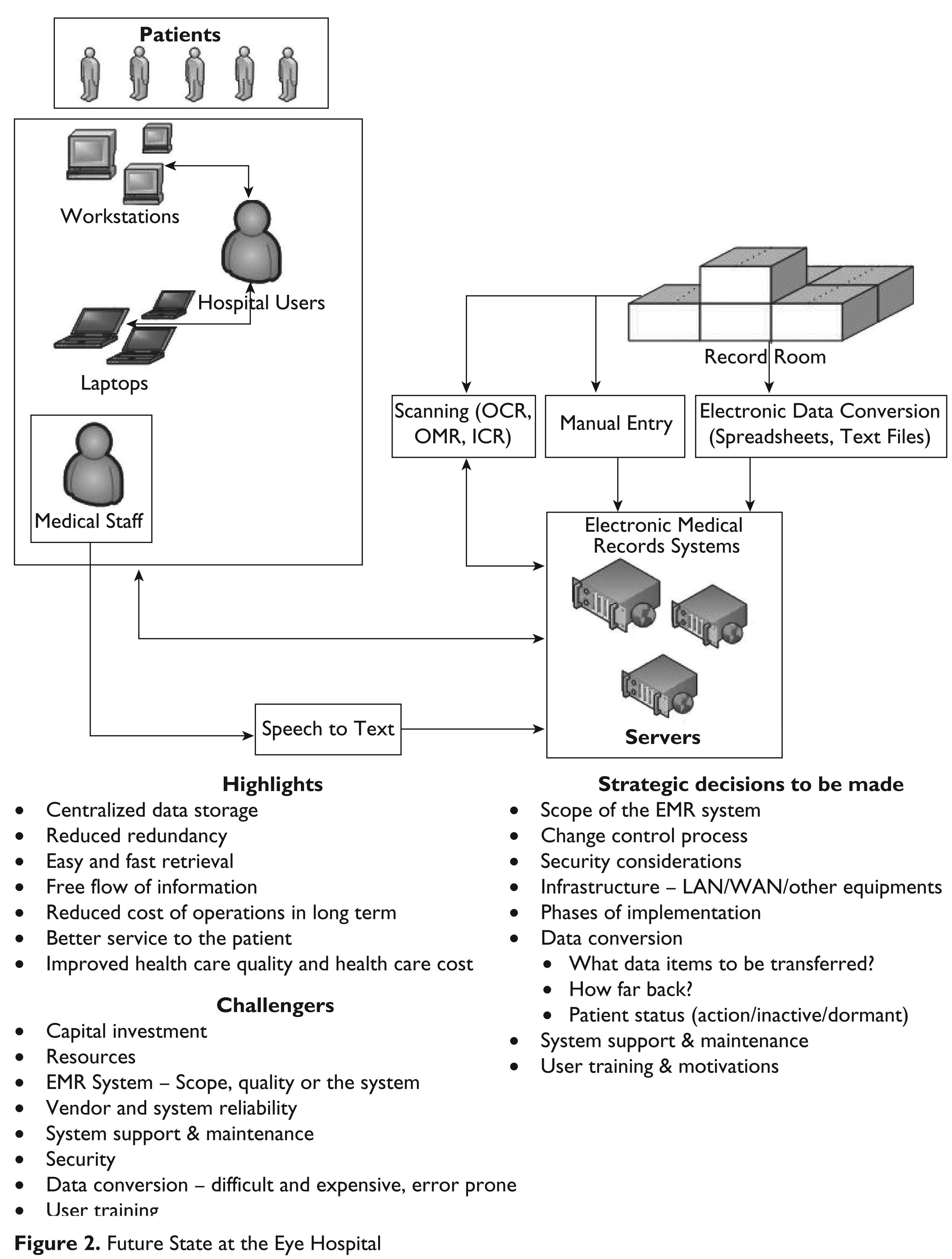
Future State
The eye hospital is acquiring an EMR system from Dewsoft Solutions (DS), which will allow the eye hospital to maintain patient records in an electronic database. The level of services provided to the patient will improve by reducing the time required to retrieve patient information and providing accurate present and historical information of the patient to the medical staff. The service to the patient is also improved by facilitating collaboration between multiple functions within the hospital (Figure 2).
Future State at the Eye Hospital
Recommendations
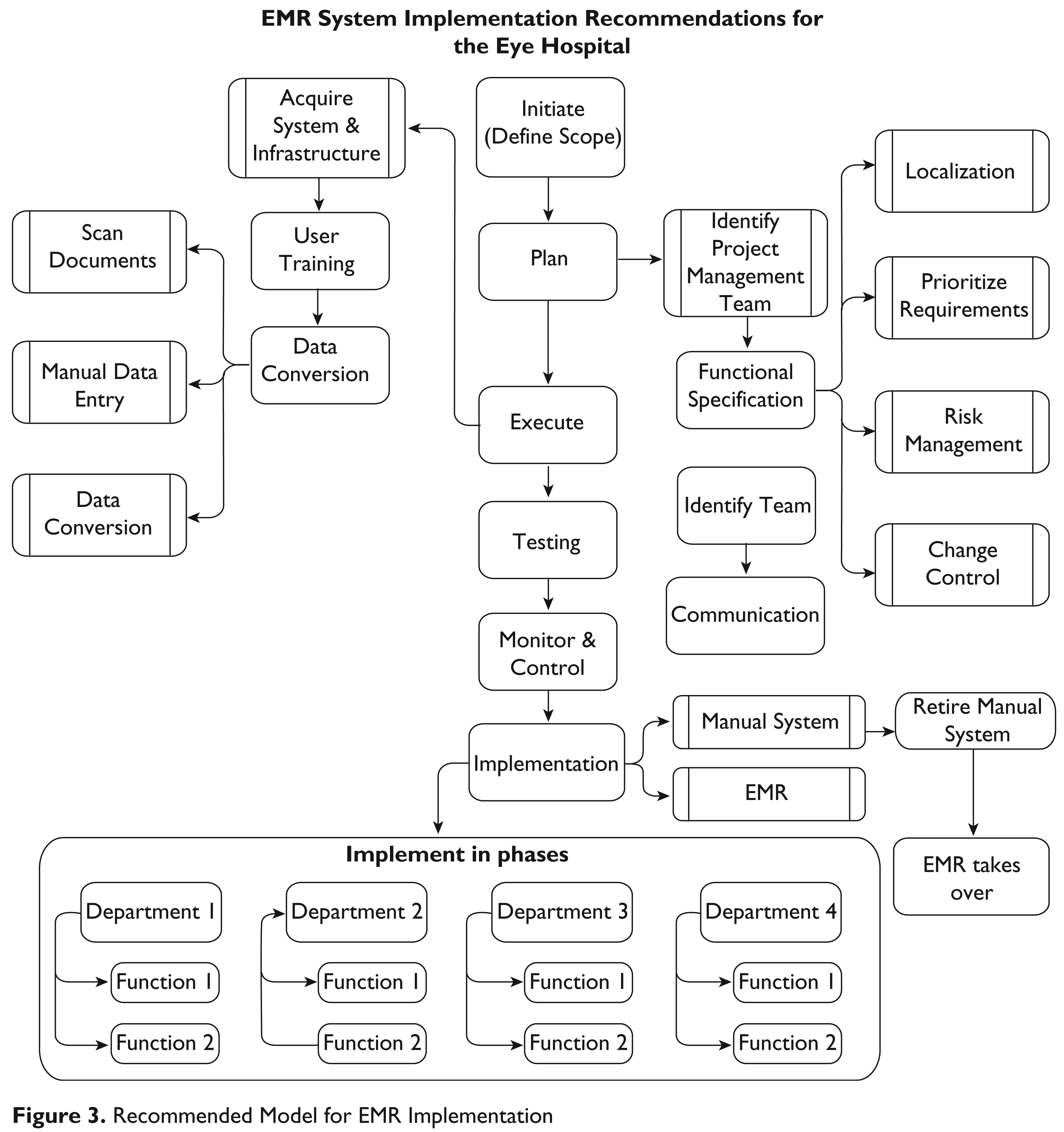
After carefully analyzing the information gathered at the eye hospital and understanding the resources available to the eye hospital, the needs and goals of transitioning to an EMR system and the current state of the initiative through the lens of CAGE framework, the CTU team has made the following recommendations (Figure 3). Since the focus of this study was to determine the methods of converting data from paper-based records to the electronic database, the recommendations for data conversion are elaborated, while only guidelines (PMI, 2004) are presented in other areas of system implementation. Additional site analysis is required for providing detailed recommendations on these areas.
Recommended Model for EMR Implementation
General Guidelines
Define scope—It is assumed that the eye hospital has already defined and documented the scope of the EMR system.
Determine a project manager—Experienced IT project manager with the business knowledge relevant to the needs of an eye hospital.
Define features—It is assumed that the eye hospital has defined, prioritized and documented the system features. This should include determination of how the system will be implemented and used at the new regional facilities. Determine how communication systems will be established to connect all facilities. While determining the features, the hospital should consider the economic aspects where availability of infrastructure, information, financial and human resources should be evaluated (Ghemawat, 2007).
Define phases and implementation plan—It is recommended that a system with such widespread impact should be implemented in phases. Components should be categorized under core components, add-on components (that can be added in phases) and optional (discretionary) components. The phases may also be defined based on the department priorities and needs.
This study also recommends implementing the EMR system with a parallel processing and phased cutover. During parallel processing, both the manual system and EMR system will be used for the same function. During the phased cutover, the manual system will be retired in phases and the EMR system will completely take over the function of the retiring manual system.
Identify risks and risk management plan—The eye hospital and DS should work together to identify risks associated with every stage of the implementation, categorized by the likelihood of occurrence, impact across the system and organization and any other category seen to be relevant. A risk mitigation plan should be developed for each one of the risks identified. Some of the commonly occurring risks are cost variance, time variance, vendor issues, disaster (system and data loss, connectivity losses, etc.) (Accenture, n.d.; Holbrook et al., 2003).
Change control process—All changes should go through a change control process, which may determine the impact, dependencies, feasibility and risks before approving the change.
Identify project team—Resources required to support implementation, training and support should be identified. From economic component of the CAGE framework (Ghemawat, 2007), availability of skilled workers in IT is one of the strengths of India which should make it easier to create a team comprising of qualified and experienced professional to execute the needs of the project.
System testing and quality assurance—This is a vital step in the implementation of a system. A dedicated team comprised of quality assurance engineers and users should be involved in thoroughly testing the system.
System support—The system support and maintenance plan should be laid out and a contract signed with the vendor. It is recommended to have an in-house team, which should be trained to meet the support and minor needs of changes in the system.
Communicating change—The eye hospital executive leadership should clearly communicate the purpose, need and benefits of EMR systems to the eye hospital employees. This communication should include details on how it affects the employees, which departments are affected, what they should expect, timing and the direct benefits for the employees and the organization. Linguistic cultural aspects should be considered while developing a communication plan. Per CAGE framework (Ghemawat, 2007), culture influences how information is distributed and received depending on language, religion, ethnicity, trust and values.
User training—The users should be provided appropriate training and support tools such as user manuals, quick reference guides, cheat-sheets, etc. During the initial phases, having a helpline available during business hours to answer user questions would be beneficial. Considering the cultural factors and the availability of a large pool of software developers and trainers (Kazmin, 1999; Nikravan, 2012; Times, 1999), this study recommends an instructor-led training. Once the users become well versed with the system, computer-based training or system help can be used to train users on system enhancements. The training material should address the differences in national and regional languages followed by the target audience, thereby reducing the cultural distance (Ghemawat, 2007).
Data Conversion Recommendations for the Eye Hospital
Based on the interviews with the software vendor DS and the eye hospital’s IT staff members, this study has made some recommendations for the data conversion process. These recommendations are made such that the eye hospital can achieve its goals with minimum cost, training, support and time, but at the same time be able to feed quality data into the system.
Scoping (AHIMA, 2010)—Scoping the data to be migrated is one of the most important strategic decisions the eye hospital will need to make. The strategy should take into account the purpose of the system, feasibility of transferring data into EMR and reports required from the system. Benchmarks and criteria for the data to be included in conversion should be clearly laid down before picking the method of data conversion and estimating the efforts required. Some of the common criteria on which candidate data can be identified are patient status, the possibility of a patient returning to the eye hospital, patient’s medical condition and number of years of past data to be captured, etc.
Methods of data conversion—Manual entry, scanning, speech to text (medical transcription) and electronic conversion are the four methods of data conversion from one system to another (Medi101, n.d.).
Manual entry is more time-consuming, and costly, but the benefits of quality of data conversion considering the challenges in the automated conversion of handwritten scripts in Devanagari and availability of skilled data entry operators (Kaka & Sinha, 2005), manual entry may be justified in selective areas. The eye hospital can take the economic advantage available in India due to cheap labour for its data entry operator needs.
Scanning is easier, faster and depending on the cost of resources, sometimes cheaper (Dubiel, 1999). However, in the context of the cost of resources in India, acquiring scanning software may be more expensive, as compared to hiring temporary workers to do the data entry (Kaka & Sinha, 2005). The cost varies with the quality of the original data and language. Acquiring scanning software to scan handwritten script in Devanagari may be challenging. Considering cultural and administrative areas of the CAGE framework (Ghemawat, 2007), the administrative challenges in acquiring foreign made software for a public service system may pose difficulties to the hospital. The government policies would influence the acquisition and implementation of tools required to scan in addition to challenges in customizing the tools to work with the regional language. For the eye hospital, scanning can be used for data items, which do not require inclusion in text searches, as they can be stored as images. It may also use a combination of electronic scanning with manual review of data converted to improve accuracy of automated data conversion.
Electronic conversion (Outlook Associates, n.d.) is a preferred method of data conversion, especially when data from one system has to be transferred to another system. However, in the case of the eye hospital, since the data comes from non-electronic sources, hybrid conversion methods can be used where data from paper can be entered into easy to use electronic document management systems such as spreadsheets, text files, etc., and then imported into the new system. This will require minimal training and most of the data entry errors can be fixed by implementing data validation processes.
Medical transcription and speech-to-text (Bikman & Whiting, 2007; Hurley, 2008) is another non-traditional data conversion method, which is recommended to capture data such as medical reports by the doctors once the system goes live.
Resourcing (Brooks, 2004)—This study recommends that the eye hospital hires a vendor to provide an EMR system with the ability to import data from sources such as text files and spreadsheets, with validation routines for capturing errors in electronic and manual data entry. The data conversion process may be expedited and resource requirements can be minimized by filtering the data to be imported into the system based on patient status, location and time, then classifying the data for manual entry, scanning and electronic conversion. In order to support these efforts, it is recommended that the eye hospital hire temporary staff in combination with outsourcing data conversion to meet the strategic goals.
Conclusions
Transforming to an EMR system from a manual record keeping and processing system involves challenges due to large financial investments, scope, building or acquiring the system, implementing the system and converting the historical paper-based data to the electronic system. This study found that following defined processes minimizes these challenges. This study also concludes that depending on the quality, form and volume of data to be converted in the context of CAGE framework which considers cultural, administrative, geographic and economic factors, a combination of data conversion methods comprising of manual data entry, scanning, speech to text and electronic conversion would help in effectively converting paper-based data to the electronic database. Health care providers planning for such data conversion should consider filtering the data to be converted based on patient status, amount of historical data required and cost of manual entry versus the cost of acquiring software to scan or import data into the electronic database.
This study was carried out by a group of CTU students and faculty as part of an Action Research course. Appreciative inquiry methods helped the research team motivate participation and as a result the study was able to collect information which was used to develop recommendations. This study provides the guidelines, processes and methods of data conversion based on the information available. Due to lack of time and other resources, a cost analysis of the methods of data conversion could not be done. This study can be extended to include an empirical examination of the cost of data conversion based on the specific information about the volume of data to be converted. Also, a detailed examination of features supported by the proposed EMR system may be carried out to determine if the reporting needs are met following the recommended data conversion methods.