
Abstract
The 1970s saw the establishment of University Teaching Hospital Ibadan (UTHI) as a hospital of eminence with lofty vision: ‘To be the flagship tertiary health care institution in the West African sub-region: offering world-class training, research and services and the first choice hospital’. It indeed kept its promise to emerge as the main teaching hospital of the country. The 1990s witnessed the decline. The Government of Nigeria appointed Vesta Healthcare Partners to advise on transformation and sustainability. A number of suggestions of far-reaching consequences came up. These involved restructuring and the reporting system; motivational initiatives; offer of opportunities to those who showed performance; recognition to performance; installation of performance measurement metrics; remuneration system; and more. The case study describes at length the challenges before Professor Temi, who has recently joined as the Chief Medical Director of UTHI and who has to handle the implementation of the recommendations. Simultaneously, he has to arrive at decisions in areas of conflicts.
Keywords
Introduction
It was just a month since Professor Temi resumed duties as the Chief Medical Director (CMD) 3 of University Teaching Hospital Ibadan (UTHI)—a leading teaching hospital in southern Nigeria. Departing from his new role of attending to largely administrative requirements, Dr Temi decided to operate on a patient he had booked for surgery prior to his appointment. After successfully carrying out the surgical procedure, he excused himself from the theatre and walked briskly into the consultants’ waiting room where his Executive Assistant—Taiwo—was already waiting for him with a load of files laid out on a table.
Vesta Healthcare Partners (VHP) Limited, a medical professional services (consultants) firm, had made some recommendations at the tail end of the previous UTHI administration and the onus lay on Professor Temi to decide on its implementation. It involved revamping the existing performance management systems as well as tweaking the existing organizational structure. The existing structure and reward system could not fuel the transformation of the hospital he desired. It also had adverse implications for the quality of health care delivered to patients.
Besides, performance measurement metrics under the current system were unclear and not benchmarked with international standards. Thus, it had an ineffective linkage with clinical performance outcomes and employee productivity. Remuneration was dependent on pay grades and promotions were based on years spent. As one who had risen through the ranks and was the Chairman Medical Advisory Committee (CMAC), prior to his appointment as the CMD, Professor Temi was convinced of the good intentions of the proposal. He was particularly excited about the positive impact the recommendations could have on his vision of moving UTHI from a tertiary health care facility to a quaternary health care facility.
However, VHP’s recommendations were bound to ‘rock the boat’ significantly, and, if inadequately managed, could spark off marked labour agitations. This would adversely impact on the hospital’s shaky reputation and the new future that Professor Temi envisaged for the institution. He was certain of several collateral damages, including a decline in external funding and a strain of public–private partnerships (PPPs) that the hospital had recently established.
Teaching Hospitals
Teaching hospitals provide clinical education and training to prospective and current doctors, nurses and other health care professionals, in addition to fulfilling a mandate of providing medical care to patients. They usually have a commitment to research, which undergirds their teaching and medical service mandates. UTHI is affiliated to the university as per regulatory practice in Nigeria. Most teaching hospitals in Nigeria are public institutions; however, with the advent of private universities, a few private teaching hospitals have emerged.
Public teaching hospitals are overseen by a governing board, which consists of government-appointed officials and prominent members of the community and a representative of the teaching hospital’s affiliated university. Staff recruitment, compensation, promotion and discipline are conducted within the strict ambit of national civil service rules and regulations of Nigeria.
Federal government-owned teaching hospitals are normally funded predominantly by budgetary allocations from the government; each teaching hospital is allowed to charge reasonable fees and embark on fund-raising initiatives such as grant initiatives and PPP ventures to compensate the meagre funds that come from the budgets.
UTHI: Commencement and Decline
UTHI was designed to be a centre of excellence and a reference centre for the training of indigenous doctors, nurses and other health care workers. It was established to provide teaching, research and clinical service facilities in the south-western region (refer Box 1). In the 1970s, UTHI was one of the leading teaching hospitals in Nigeria and was reputed for the calibre of its clinical staff, quality of research output and the range of services it offered. However, starting from the mid-1980s, the quality of service and infrastructure showed a decline. This decline was generally attributed to the following:
‘To be the flagship tertiary healthcare institution in the West African sub-region: offering world-class training, research and services and the first choice hospital for those seeking specialist healthcare in a conducive atmosphere; renowned for a culture of continuing and compassionate care’
‘Rendering excellent, prompt, affordable and accessible healthcare in an environment that promotes hope and dignity, irrespective of status, and developing high quality health personnel in an atmosphere that stimulates excellent and relevant research’
adverse macroeconomic environment; reduction in capital allocation from the federal government; large-scale emigration of skilled health care workers; perennial industrial crises characterized by frequent strike actions by various cadre of staff; growing inability of patients to afford the meagre hospital charges; deterioration in physical infrastructure; aging and outdated equipment prone to frequent breakdowns; deterioration of the national health system characterized by degradation of the primary and secondary tiers of health care service, which, in turn, placed an undue burden on the few tertiary health care centres; and frequent power outages and dependence on diesel-powered generators.UTHI’s Vision and Mission Statements
UTHI Vision
UTHI Mission
These interrelated factors resulted in a vicious cycle, which served to progressively demotivate the staff, resulting in a culture of apathy to work and nonchalance to customer service.
UTHI Renaissance
From 1999 onwards, the federal government of Nigeria began to progressively focus on transforming the national health system with concomitant initiatives directed at primary and tertiary health centres. The federal government invested in infrastructural rehabilitation of the teaching hospitals, including refurbishment and upgrade of equipment. Modern diagnostic and therapeutic equipments such as magnetic resonance imaging (MRI), computerized tomography (CT) scan, mammography machines and endoscopes were purchased and distributed to the federal government-owned teaching hospitals. End users of these equipments were trained in the use of the procured equipment. Steps were taken for proper maintenance and upkeep of the medical equipment.
At UTHI, this period coincided with the leadership of Professor Temi’s predecessor, Professor Ile. He was CMD from 2001 to 2011. He complemented the federal government’s infrastructure and equipment upgrade with PPPs, notably in diagnostics, environmental sanitation, catering and information technology. Professor Ile also made an attempt to improve the attitude of the workforce towards customer service. Numerous customer service seminars were implemented for all cadres of health care workers. Plaques heralding the customer service paradigm were fixed at prominent places within UTHI. These plaques bore messages such as: ‘UTHI is wearing a new look and new equipment are being put in place. Now let us improve our attitude to work and make UTHI the envy of the health care delivery sector.’
‘You have no right whatsoever under whatever circumstances to shout at or insult your patients. They are the reason you have a job.’
These admonitions complemented other customer service initiatives to reorient the staff of UTHI to become more patient sensitive and focused.
In 2008, Professor Ile’s initiatives resulted in the resuscitation of several hitherto abandoned specialist procedures, which had been last performed in the 1970s. These procedures included corneal transplant (last done in 1972), open-heart surgery (last done in 1978) and renal transplant (never done previously). With these achievements, staff, students and patients began to speak of the restoration of the lost glory of UTHI. Staff morale improved and patient confidence in the institution rose.
Keeping the Momentum
In spite of these notable achievements, Professor Ile felt that without an institutionalized framework, these achievements would be degraded in the near future and UTHI’s restored glory would be a flash in the pan. Following extensive consultation with his senior management team and the governing board of UTHI, it was decided that a critical review of the existing clinical performance and quality assurance system be carried out.
In 2009, after a competitive bid in compliance with public sector procurement regulations, a private sector health care consultancy firm, VHP, was contracted to design a framework for UTHI which would support sustained growth and development critical to the evolution of UTHI as a quaternary or super-specialty health care provider. Professor Ile considered that quaternary health care services would attract a fair share of the foreign exchange spent on medical tourism by Nigerians in India, the United Kingdom (UK), Egypt, Germany, South Africa, etc. He also considered that this would raise the profile of UTHI within the local and international medical community and attract staff and patients to the institution. Professor Ile anticipated that successful quaternary health care services would attract government funding to the institution.
Extensive hospital-wide consultations and systems reviews followed. The external consultants surmised that the extant organizational structure and the absence of an explicit performance measurement system at UTHI could neither maintain nor sustain the vision of transforming UTHI into a quaternary health care establishment. They, therefore, recommended a restructuring of the hospital’s organizational structure and a reworking of its performance management system—particularly as it related to job planning, objective setting and performance appraisal.
Organizational Restructuring: Clinical Leadership
Traditionally, the academic heads of departments at the College of Medicine become the de facto heads of clinical service departments at UTHI. These academics are affiliated to the College of Medicine and their primary interests are teaching and research. These academics are, in turn, conferred with the status of honorary consultants by the teaching hospital. To augment the services of these honorary consultants, the hospital employs another category of similarly qualified medical professionals referred to as hospital consultants. The primary responsibility of these hospital consultants is patient care. However, they are also involved in teaching and research activities for which they are neither remunerated nor appraised. The College of Medicine remunerates honorary consultants, while UTHI augments with a variable call duty allowance. Hospital consultants are entirely remunerated by the UTHI. The teaching hospital pays both their basic salary and call duty allowance.
In the opinion of VHP consultants, the undeclared allegiance of the academic honorary consultants is to their primary employer—the College of Medicine—and consequently, these individuals would invest more passionately in traditional measures of advancing their careers—research and academic publications—rather than the unmeasured and unrewarded volition of clinical service at UTHI. Consequently, VHP consultants recommended the institution of a clinical leadership system, described as leadership by clinicians of clinicians, with only hospital consultants appointed as heads of departments.
Organizational Restructuring—Clinical Divisions
Traditionally, heads of departments have the responsibility for accomplishing clinical departmental goals and objectives but do not control financial, budgetary or administrative resources that are required for the efficient accomplishments of these obligations. UTHI’s 24 heads of departments report to the CMAC. This results in excessive administrative burdening of the CMAC who, in addition to his administrative role, still maintains teaching and research obligations to the College of Medicine (see Figure 1). This also stifled innovation and prompt service delivery within the hospital.
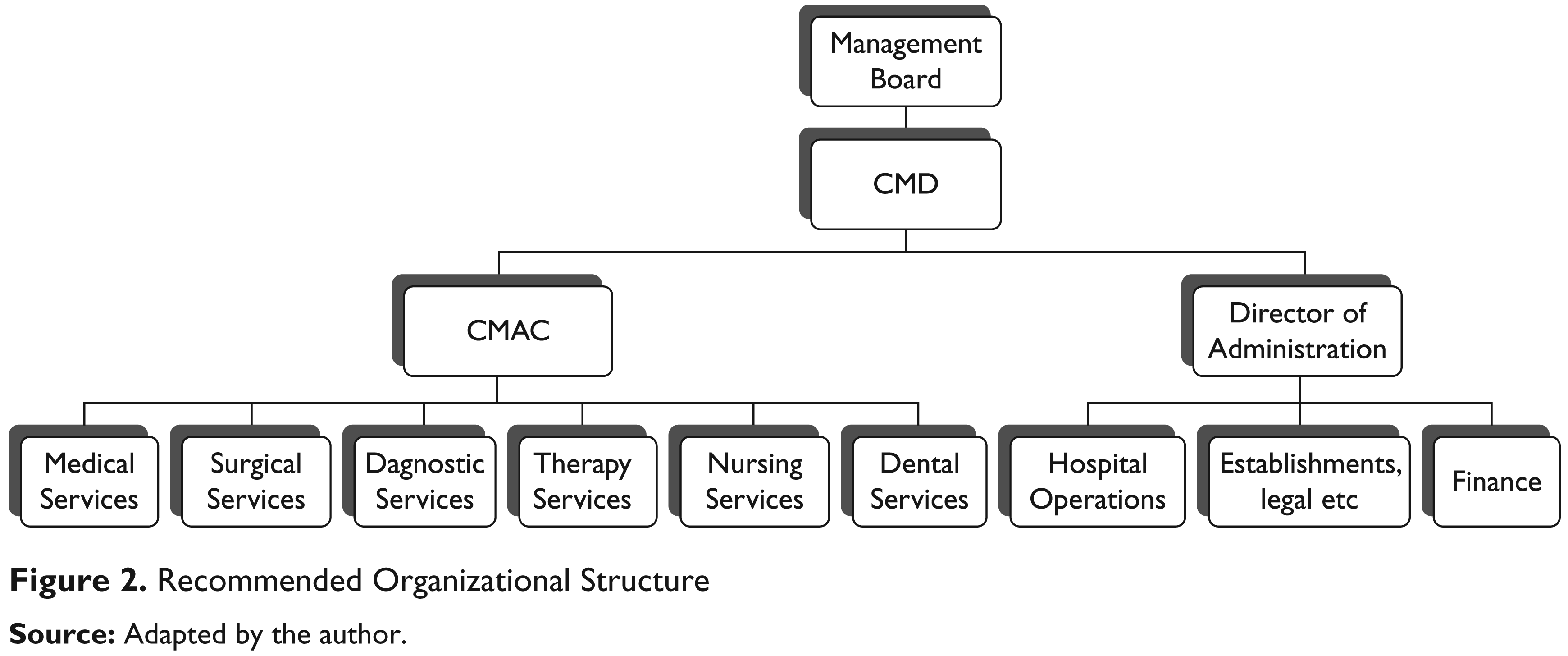
The VHP consultants proposed that six new clinical divisions (medical services, surgical services, dental services, therapy services, diagnostic services and nursing services) should replace the existing 24 heads of departments. The existing departments would be subsumed within related clinical divisions and reconfigured as service lines within the divisions. The clinical division heads shall be senior hospital consultants who shall have full clinical, managerial and budgetary control with overall responsibility and accountability for the performance of their divisions. The six clinical division heads will report to the CMAC who, in turn, reports to the CMD.
Each clinical division head would be supported by specialty consultant leads, a clinical head of nursing and five service delivery officers. The specialty consultant leads will replace the traditional heads of departments and would have oversight over specific clinical units, while the clinical head of nursing would line manage all nurses in the division. The service delivery officers—a new cadre of managers—would have oversight over administrative and quality improvement resources. All specialty consultant leads, the clinical head of nursing and the service delivery officers would report to the clinical division head (see Figure 2).

The net impact of the proposed organizational restructuring is a strengthening of clinical leadership resulting in faster and more effective decision making.
Clinical Performance Management
The VHP consultants observed that there was no explicit performance management system at UTHI guiding administrative, financial and clinical performance at UTHI. Traditionally, staff were promoted from one step to another annually, and usually from one level to another every four years. This promotion was without recourse to the attainment of explicit corporate or departmental metrics. The promotion of academic consultants was not within the purview of the UTHI but the College of Medicine, although their clinical service privileges resided at UTHI.
To achieve more responsive patient-centred services and consistent clinical outcomes, VHP consultants recommended the introduction of a clinical performance management system, which relates indices of productivity, performance, quality and outcomes of care to individual clinicians, divisions and UTHI. These indices would be measured, actively monitored and reviewed periodically. Patient safety and well-being would be the underlying themes.
The VHP consultants recommended that patient outcomes should be evaluated through clinical outcomes benchmarking which referred to the practice of collecting, analyzing and publishing diverse outcomes data that reflect the clinical practice of consultants and comparing with those of the consultant’s peers. Measured outcomes will be case mix adjusted for age, gender and social status. Specific metrics include outpatient attendance, finished consultant’s episode, outpatient first appointment to follow up ratio, outpatient to inpatient conversion rate, mortality rate procedures, mortality rate diagnoses, length of stay procedures, length of stay diagnoses, readmissions rate procedures, readmission rate diagnosis, day case rate procedures and DNA (did not attend) rates. This practice will ensure that clinical performance management is integrated into the fabric of each clinical unit, division and the entire UTHI.
While these recommendations were certain to be embraced by consultants who devoted most of their time on patient care at UTHI, it was bound to cause some rancour among those who spent a good deal of their time in more lucrative private practice engagements. The high attrition rate of quality medical personnel was yet to fully become a thing of the past; acting on this recommendation may frustrate the progress made.
The move, if taken, may deepen the feelings of inequity that existed between the honorary and hospital consultants. Up to this point, the honorary consultant received higher emoluments than their counterparts employed by UTHI as full-time consultants. Their income came from UTHI as consultants, the College of Medicine as academics and private practice. They also were better favoured for research grants and incentives. Hospital consultants relied on private practice to make up for the comparatively low earnings that are received by medical practitioners in Nigeria generally.
Professor Temi’s Dilemmas
The VHP’s recommendations were received close to the end of Professor Ile’s tenure. In his handing over brief, he urged Professor Temi to implement those recommendations. The onus to implement, discard or modify the recommendations therefore fell on the incumbent, Professor Temi. He needed to take a definite decision over the weekend, ahead of his first management meeting with the executive management team on Monday.
Professor Temi noted that the recommendations were transformative and he wondered if less revolutionary initiatives would suffice to take UTHI to the promised land of delivering quality patient-centred quaternary care services. He also thought about the impact of the recommendations on industrial relations. He doubted that the restrictive national civil service rules and regulations would allow for innovative organizational structures and performance evaluation such as was recommended by VHP. He also considered the possible impact of these recommendations on the morale of hospital consultants. Is there something we could do to ensure performance without compromising on the commitment of our dedicated staff? Was the proposed restructuring sufficient to restore the lost glory of the teaching hospital and make it the premier health care institution in Nigeria a few years in the future?
Footnotes
Acknowledgements
The authors wish to express thanks to the UTHI management for the support in development and consent for publication of this case study.