
Abstract
Background:
Keratin hair treatments are widely used in salons due to their ability to straighten hair. However, these treatments often contain formaldehyde, a known volatile organic compound (VOC) associated with adverse respiratory effects. Salon workers performing keratin treatments may be at increased risk of respiratory impairment due to occupational exposure to formaldehyde. This study aimed to assess the impact of formaldehyde exposure during keratin hair treatments on lung function among salon workers.
Design and methods:
This cross-sectional study included 41 female salon workers who regularly perform keratin treatments. Spirometry was conducted to measure FEV1 (forced expiratory volume in the first second), FVC (forced vital capacity), and the FEV1/FVC ratio. Values were compared with predicted norms, and associations with exposure-related variables were analyzed using independent t-tests and Spearman correlation analysis.
Results:
Participants showed significantly lower mean values for FEV1, FVC, and FEV1/FVC ratios than predicted norms (p < 0.001).
Conclusion:
These findings underscore the need for improved protective protocols in salons to safeguard workers’ respiratory health.
Introduction
Keratin hair treatments have become increasingly popular in recent years due to their effectiveness in straightening hair and reducing frizz, resulting in growing demand in hair salons worldwide. 1 However, these treatments often involve the use of products containing formaldehyde or formaldehyde-releasing agents, which are known to have adverse health effects, particularly on the respiratory system. 2 Volatile organic compounds (VOCs) are carbon-based chemical compounds characterized by their high vapor pressure at room temperature, and are commonly found in various products, including but not limited to household products, paints, and hair smoothing products. Exposure to inhalable VOCs can cause adverse respiratory effects. Paint workers, for example, were found to have a significant reduction in pulmonary function, as measured by spirometric parameters, including forced expiratory volume in one second (FEV1) and the FEV1/forced vital capacity ratio (FEV1/FVC). 3 Formaldehyde (CH2O), also known as HCHO, is an important member of the VOC family and is present in various natural and anthropogenic sources. It occurs naturally from biomass combustion, such as forest and bush fires, and is also found in urban environments due to automobile exhaust and industrial emissions. Additionally, formaldehyde is produced on a large scale for industrial use, particularly in the manufacture of resins, plastics, and cosmetic products, including keratin hair treatments. Inhalation exposure to formaldehyde has been linked to several health risks, including irritation of the eyes, nose, mouth, and throat, as well as headache and dizziness. Keratin treatment is a semi-permanent hair-straightening product that contains formaldehyde and, despite its proven risk, is still widely used in hair salons. During both the application and heating phases of keratin treatments, formaldehyde can be released into the air, posing a risk to salon workers and clients. 4 Exposure to formaldehyde in hair salons has been documented to cause respiratory symptoms such as coughing, wheezing, and shortness of breath, as well as more severe effects such as asthma and reduced lung function.2,5,6
Hair salon workers, particularly those who frequently perform keratin treatments, are at elevated risk for adverse health effects due to repeated and prolonged exposure to formaldehyde and other VOCs. 2 Studies have shown that occupational exposure to formaldehyde is associated with a range of respiratory issues, including upper airway irritation, bronchial hyperreactivity, and long-term declines in pulmonary function.7,8 Furthermore, formaldehyde concentrations in hair salons can exceed occupational safety limits, especially in poorly ventilated environments. 9 Chronic inhalation of formaldehyde and other harmful substances in these settings may contribute to the development of persistent respiratory conditions,7,8 highlighting the importance of implementing protective measures and monitoring of air quality in salons.
Given the widespread use of keratin hair treatments and the associated exposure of salon workers to formaldehyde and other volatile chemicals, there is a critical need to understand the potential respiratory health risks in this occupational setting. This study aims to examine the impact of working as a keratin treatment specialist on lung function, with a focus on the risk of developing respiratory conditions resulting from prolonged formaldehyde exposure in hair salons.
By addressing these issues, this study aims to provide a comprehensive understanding of the occupational hazards with keratin treatment application, thereby contributing to improved health and safety standards in the cosmetology field.
Material and methods
Study design
A cross-sectional study was conducted to achieve the study goal. This study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline. 10 The completed STROBE checklist is provided as Supplemental File 1. Ethical approval was obtained from the Research Ethics Committee at the Faculty of Allied Medical Sciences at Applied Science Private University (Reference No: AMS-2024-5).
Recruitment of participants
Participants were recruited through hair salons in Jordan. To enhance recruitment, an invitation to participate in the study was also posted on social media platforms (Facebook and Instagram). All procedures were conducted with the principles of the Declaration of Helsinki, and written informed consent was obtained from all participants. Data were collected between September 2024 and December 2024.
Inclusion and exclusion criteria
Participants were included if they were working in salons and daily performed keratin hair treatments for clients, and were above 18 years old. Participants were excluded if they had any diagnosed cardiorespiratory, musculoskeletal, or neurological conditions; or had undergone any surgeries that could limit their exercise capacity or ability to perform spirometry.
Outcome measure
Pulmonary function test
Spirometry was assessed using a spirometer (BTL Spirometry, United Kingdom) in accordance with the European Respiratory Society/American Thoracic Society (ERS/ATS) guidelines. 11 The best of three consecutive blows was used to obtain the FEV1 (forced expiratory volume in the first second), FVC (Forced vital capacity) and FEV1/FVC ratio. 11 Results were compared with norms from the Global Lung Initiative to get the predicted percent values. 12
Self-administered survey
An e-survey was administered in this study, including questions on personal and occupational information, such as the performance of keratin treatment. Supplemental File 2 presents the survey.
Statistical analysis
Descriptive statistics were used to characterize participants based on the studied variables using SPSS software. Mean and standard deviation were used to describe continuous variables, while frequency and percentage were reported for categorical data. Continuous variables included age, BMI, FEV1, FVC, the FEV1/FVC ratio, duration of working in salons/beauty centers, and duration of performing keratin hair treatments. Categorical variables included marital status, educational level, smoking status, frequency of keratin treatments per day, duration of the last keratin treatment session, use of protective measures during treatments, and the presence of health conditions.
Differences between measured and predicted values of FEV1, FVC, and the FEV1/FVC ratio based on individuals of the same age, height, weight, gender, and ethnic origin (according to the Global Lung Initiative data), were assessed using Paired t-test. In addition, Spearman correlation analysis was performed to examine associations between continuous exposure variables (years of salon work, years performing keratin treatments, daily keratin frequency, and session duration) and pulmonary function parameters (FEV1 and FVC). Spearman correlation was selected due to the non-normal distribution of some exposure variables and the relatively small sample size.
Independent t-test was conducted to assess differences in FEV1 and FVC based on various exposure-related variables: duration of working in salons/beauty centers (<15 years vs ≥15 years), duration of performing keratin hair treatments (<10 years vs ≥10 years), frequency of daily keratin treatments (1–2 times vs 3–5 times), duration of each keratin session (1–2 hours vs >2 hours), and use of protective measures (yes vs no). p-Values less than 0.001 are reported as p < 0.001 in accordance with statistical reporting standards.
Sample size
According to Skaik, 13 a minimum sample size of 40 participants is recommended for the t-test, as this number is generally sufficient to satisfy the assumption of normality. A priori power analysis assuming a medium effect size (d = 0.5), alpha = 0.05, and power = 0.80 suggested a minimum of 34 participants. We recruited 41 to account for potential dropouts.
Results
Forty-one participants were included in this study. All participants were female (41, 100%), with a mean age of 35.1 ± 10.3 years. The average duration of working in salons/beauty centers and of performing keratin hair treatments was 13.5 ± 9.1 and 7 ± 3.9 years, respectively. The mean values of FVC, FEV1, and the FVC/FEV1 ratio were 3 ± 0.64 L, 2.6 ± 0.56 L and 86.5 ± 10.2%, respectively. The characteristics of the participants are presented in Table 1.
Baseline characteristics of participants.

BMI: body mass index; FEV1: forced expiratory volume in the first second; FVC: forced vital capacity; N: number; SD: standard deviation.
The paired t-test showed that the mean values of FEV1, FVC and FEV1/FVC were significantly lower than their predicted values; t(40) = −31.38, p < 0.001; t(40) = −30.42, p < 0.001; and t(40) = −27.60, p < 0.001, respectively (Table 2).
Spirometry results compared to their predicted values according to the Global Lung Initiative data (using paired sample test).
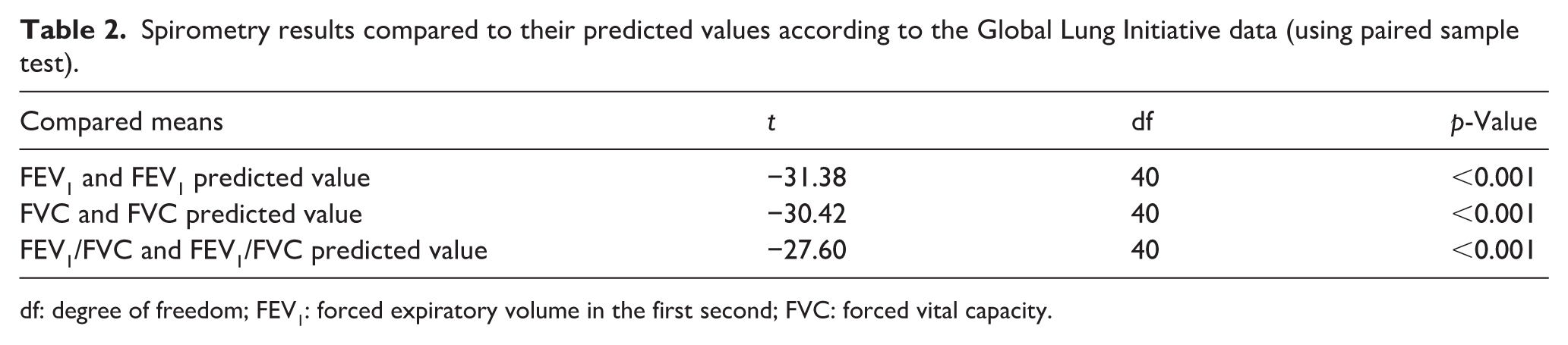
df: degree of freedom; FEV1: forced expiratory volume in the first second; FVC: forced vital capacity.
Independent t-test indicated that there were no statistically significant differences in the mean values of FVC (Table 3) and FEV1 (Table 4) across the studied variables; duration of working in salons/beauty centers, duration of performing keratin hair treatments, frequency of daily keratin treatments, duration of each keratin session, and use of protective measures.
Spirometry results (FVC) based on various exposure-related variables (using independent t-test).
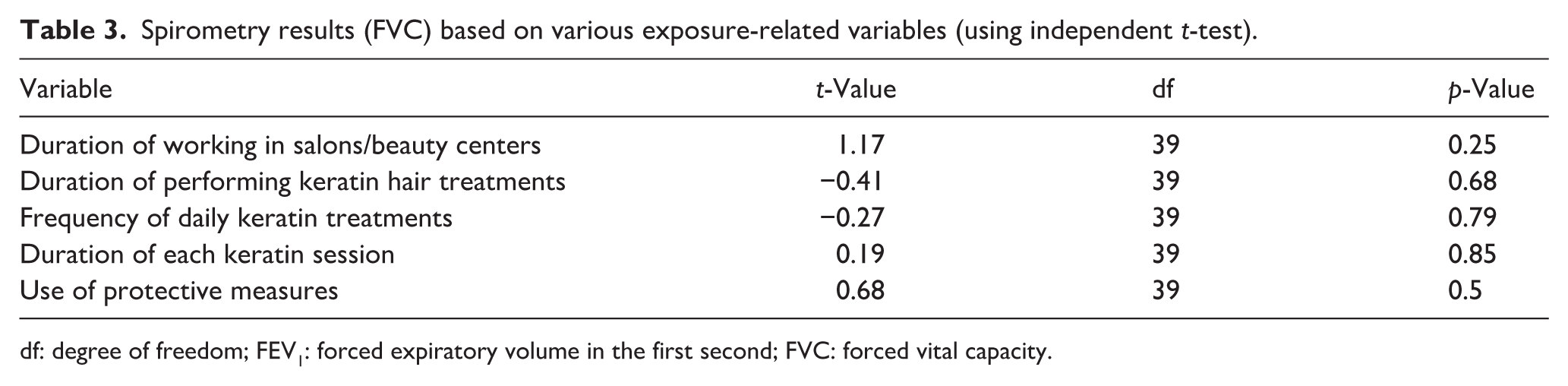
df: degree of freedom; FEV1: forced expiratory volume in the first second; FVC: forced vital capacity.
Spirometry results (FEV1) based on various exposure-related variables (using independent t-test).

df: degree of freedom; FEV1: forced expiratory volume in the first second; FVC: forced vital capacity.
Spearman correlation analysis did not demonstrate any statistically significant associations between continuous exposure variables and pulmonary function outcomes (all p > 0.05). Weak inverse correlations were observed between years of salon work and both FEV1 (ρ = −0.203, p = 0.202) and FVC (ρ = −0.202, p = 0.206); however, these associations were not statistically significant (Table 5).
Spearman correlation between continuous exposure variables and pulmonary function parameters.

ρ: Spearman correlation coefficient.
Discussion
This study examined the impact of occupational exposure to formaldehyde from keratin hair treatments on lung function among hair salon workers in Jordan. Our findings revealed significant reductions in lung function parameters of FEV1, FVC, and FEV1/FVC ratio compared to predicted values for healthy individuals of similar age, height, ethnic origin and gender. These findings are consistent with previous literature demonstrating the adverse respiratory effects of formaldehyde exposure.2,5,6 The observed decline in pulmonary function among participants highlights the occupational health risks associated with repeated exposure to formaldehyde-containing products in the salon environment, underscoring the need for protective measures and improved regulations in the cosmetology industry.
The findings of this study also indicated that the duration of exposure to keratin treatments was not significantly associated with reduced pulmonary function. Regardless of the duration of performing keratin hair treatments, the frequency of daily treatments, and the length of each session, participants exhibited reduced lung function. This contrasts with previous studies,14,15 which reported that a longer duration of work as a hairdresser was associated with greater declines in pulmonary function. A possible explanation for this discrepancy is that approximately 83% and 78% of participants in the present study had been working as hairdressers and performing keratin treatments, respectively, for more than 5 years. Additionally, all participants reported performing this type of work for at least 1 h per day. Our study specifically examined exposure related to Formaldehyde associated with keratin treatment rather than cumulative occupational exposure over total years of hairdressing practice. This may suggest that keratin treatment might be considered as a potential respiratory irritant even from relatively early exposure. However, it should be mentioned that the larger sample sizes in the referenced studies may have provided greater statistical power to detect the association between exposure duration and pulmonary function decline, which may explain this discrepancy between their findings and ours.
Formaldehyde exposure limit and regulatory actions vary across countries. In Jordan, formaldehyde-containing cosmetic products are not completely banned; however, it does follow strict regulations by the Jordan Food and Drug Administration (JFDA). 16 The JFDA requires prior approval before marketing and closely monitors cosmetic safety; yet, the limit concentration is not explicitly defined in publicly accessible regulatory texts. In comparison, jurisdictions such as those in the United States have established defined workplace formaldehyde exposure limits. According to the Occupational Safety and Health Administration (OSHA) in the United States, the permissible exposure limits of formaldehyde are 0.75 ppm as an 8-h time-weighted average and a short-term exposure limit of 2 ppm. 17 Given the known respiratory effects of formaldehyde, there is a national need to clearly define exposure limits and increase awareness of preventive measures and safer product alternatives. In addition to differences in sample size and years of occupational exposure, other environmental and occupational factors may partly explain discrepancies between our findings and previous studies. Detailed information regarding weekly working schedules was not collected in the present study; therefore, variations in the number of working days per week or the distribution and clustering of keratin sessions may have influenced cumulative exposure patterns. Differences in temporal exposure dynamics could result in heterogeneity in formaldehyde dose-response relationships across studies.
Furthermore, indoor formaldehyde concentrations are not static and may fluctuate according to environmental and photochemical processes. Formaldehyde can interact with atmospheric oxidants such as ozone (O3) and nitrogen oxides (NOₓ), which follow diurnal patterns influenced by sunlight intensity and urban traffic emissions. These interactions may modify indoor concentration dynamics, particularly in urban salons with variable ventilation rates and proximity to outdoor pollution sources.
Additionally, structural and environmental differences between salons, including floor level, building design, ventilation systems, air exchange rates, and geographic location, may substantially influence airborne accumulation of volatile compounds. Such contextual variability may limit direct comparability between studies conducted in different environmental and regulatory settings.
A simulation-based study was conducted to directly measure airborne formaldehyde during keratin sessions. 18 Formaldehyde concentrations were detected at levels approaching or exceeding OSHA’s exposure limit during both blow-drying and flat ironing phases in the breathing zone of stylists and clients, even in products marketed as “formaldehyde-free.” The present study differs by assessing exposure indirectly by examining lung function in salon workers and using exposure proxies such as treatment duration and session length. Together, these complementary approaches provide both mechanistic evidence of exposure and associated physiological changes.
In the current study, we examined whether the use of protective measures may reduce the impact of Keratin exposure on lung function. The results showed no statistically significant differences in pulmonary function between individuals who used protective equipment (gloves or/and mask) and those who did not. One possible explanation is that prior COVID-19 infection, which was reported in a substantial proportion of participants, may have influenced pulmonary function independently of occupational exposure. 19
Several limitations should be acknowledged. First, the cross-sectional design of this study restricts the ability to infer causality between formaldehyde exposure and lung function decline. Longitudinal studies are needed to better understand the cumulative effects of chronic exposure to formaldehyde over time. Second, formaldehyde exposure from keratin hair treatments was not objectively measured, which may affect the accuracy of exposure assessment and weaken the ability to establish a clear relationship between exposure and its respiratory effects. Third, the study sample was limited to female salon workers, which may limit the generalizability of the findings to male workers who may have different occupational exposure levels or health conditions. In addition, characteristics of salons such as location, floor level, ventilation, building structure, were not collected. These characteristics may influence air circulation and the accumulation of airborne contaminants, potentially affecting exposure levels among workers. Additionally, baseline/background indoor formaldehyde levels from sources such as furniture, building materials, and outdoor pollution were not measured, which limits the ability to isolate keratin-related exposure from other environmental contributors. Lastly, the relatively small sample size limits the statistical power and generalizability. A major limitation is the lack of direct measurement of airborne formaldehyde or formaldehyde biomarkers. Future studies should employ personal air sampling or passive dosimeters to better quantify individual exposure.
Conclusion
In conclusion, this study adds to the growing body of evidence indicating that occupational exposure to formaldehyde from keratin hair treatments poses significant respiratory health risks for salon workers. Given the increasing prevalence of keratin treatments, there is a pressing need for regulatory bodies and salon employers to implement and enforce protective measures aimed at safeguarding workers’ respiratory health. Future research should prioritize longitudinal studies to monitor lung function changes over time, explore safer alternatives to formaldehyde-based products in order to reduce occupational hazards in the cosmetology industry and incorporate direct environmental monitoring of formaldehyde concentrations to improve exposure characterization.
Significance for public health
This study demonstrates that salon workers performing keratin hair treatments are at increased risk of respiratory impairment due to occupational exposure to formaldehyde. Participants exhibited significantly lower lung function measures (FEV1, FVC, and FEV1/FVC) compared with predicted norms, highlighting a clear occupational health concern. These findings emphasize the urgent need for public health interventions, including stricter enforcement of protective protocols in salons, use of personal protective equipment, and the development of safer, formaldehyde-free alternatives. By addressing these modifiable workplace hazards, regulatory bodies and salon employers can reduce respiratory health risks and improve long-term health outcomes for cosmetology workers.
Supplemental Material
sj-docx-1-phj-10.1177_22799036261441337 – Supplemental material for Impact of occupational exposure to formaldehyde in Keratin hair treatments on lung function among salon workers: A cross-sectional study
Supplemental material, sj-docx-1-phj-10.1177_22799036261441337 for Impact of occupational exposure to formaldehyde in Keratin hair treatments on lung function among salon workers: A cross-sectional study by Mohammad Z. Darabseh, Rahaf Badran, Aseel Aburub, Ragad Alkaraki, Tarekq Gharibeh, Ala’a M. Shurrab, Anas Nizar, Owis Eilayyan, Bence L. Raposa and Pongrác Ács in Journal of Public Health Research
Supplemental Material
sj-docx-2-phj-10.1177_22799036261441337 – Supplemental material for Impact of occupational exposure to formaldehyde in Keratin hair treatments on lung function among salon workers: A cross-sectional study
Supplemental material, sj-docx-2-phj-10.1177_22799036261441337 for Impact of occupational exposure to formaldehyde in Keratin hair treatments on lung function among salon workers: A cross-sectional study by Mohammad Z. Darabseh, Rahaf Badran, Aseel Aburub, Ragad Alkaraki, Tarekq Gharibeh, Ala’a M. Shurrab, Anas Nizar, Owis Eilayyan, Bence L. Raposa and Pongrác Ács in Journal of Public Health Research
Footnotes
Acknowledgements
We would like to thank all participants for taking part in this research.
Ethical considerations
Ethical approval was obtained from the Research Ethics Committee at the Faculty of Allied Medical Sciences at Applied Science Private University (Reference No: AMS-2024-5).
Consent to participate
All procedures were conducted with the principles of the Declaration of Helsinki, and written informed consent was obtained from all participants.
Consent for publication
Not applicable.
Author contributions
Conceptualization: Mohammad Z. Darabseh, Rahaf Badran and Aseel Aburub; Data curation: Ragad Alkaraki and Anas Nizar; Formal analysis, Owis Eilayyan. Investigation: Mohammad Z. Darabseh, Rahaf Badran, Aseel Aburub, Anas Nizar, Bence Raposa and Pongrác Ács. Methodology: Mohammad Z. Darabseh, Aseel Aburub, Ragad Alkaraki and Owis Eilayyan. Project administration: Mohammad Z. Darabseh. Resources: Ragad Alkaraki and Ala’a Shurrab. Supervision: Aseel Aburub; Validation, Aseel Aburub and Tariq Gharaibeh; Writing – original draft: Mohammad Z. Darabseh, Rahaf Badran, Aseel Aburub, Ragad Alkaraki, Tariq Gharaibeh, Ala’a Shurrab, Anas Nizar, Owis Eilayyan, Bence Raposa and Pongrác Ács. Writing – review & editing: Mohammad Z. Darabseh, Rahaf Badran, Aseel Aburub, Ragad Alkaraki, Tariq Gharaibeh, Ala’a Shurrab, Anas Nizar, Owis Eilayyan, Bence Raposa and Pongrác Ács. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by Applied Science Private University (Project reference number: DRGS-2024-2).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data are fully available without restriction.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.