
Abstract
Background
The implementation of universal screening to identify women at risk of postnatal mental disorders has been recommended. Understanding whether depressive symptoms immediately postpartum, as detected by screening tools, predict later psychiatric diagnoses is crucial for guiding timely care and optimizing healthcare resources.
Methods
All participants completed the Edinburgh Postnatal Depression Scale (EPDS) 2–5 days postpartum. Women with scores ≥ 10 were invited to the follow-up study, where psychiatric diagnoses at six weeks were assessed using the Mini-International Neuropsychiatric Interview 5 (MINI). Sensitivity, specificity, positive (PPV), and negative (NPV) predictive values were calculated. ROC analyses assessed predictive accuracy.
Results
A total of 403 women were included. EPDS scores of ≥ 16 for a major depressive episode (AUC = 0.78, sensitivity 0.71, specificity 0.84, PPV 0.14, NPV 0.99 within this high-risk sample) and ≥ 14 for any observed mental disorder (AUC = 0.69, sensitivity 0.65, specificity 0.73, PPV 0.24, NPV 0.94) were identified as optimal.
Conclusions
In women with elevated depressive symptoms shortly after delivery, the EPDS showed high NPV, supporting its usefulness for ruling out severe psychopathology at six weeks postpartum. However, the low PPV indicates that elevated scores often reflect transient postpartum distress rather than a confirmed disorder. Routine immediate-postpartum EPDS screening should therefore be approached with caution. Findings support a tiered approach—for example, brief initial inquiries followed by the EPDS and diagnostic follow-up for higher scores—and the development of screening tools better adapted to the immediate postpartum period.
Introduction
There exists global concern around postpartum mental health, as its disruption has adverse effects on women, their children, and the broader family system. 1 Anxiety and depressive disorders are the most prevalent disorders reported postpartum, with reported rates ranging from 9% to 20%, influenced by factors like country or assessment type. 2 Consistent with international data, the prevalence of postpartum mental health disorders in the Czech Republic is estimated to be 13%. 3
A comprehensive postnatal mental-healthcare pathway involves screening, assessment, triage and referral, treatment access, treatment initiation, symptom monitoring, and adapting treatment based on measurement until symptoms remit. 4 Implementing this care pathway in practice, however, faces various barriers. Over half of all postpartum mental-health cases go unrecognized and undiagnosed. 5 Increasing the number of cases identified through screening is a critical first step that needs to be followed by assessment and treatment. 4
Various guidelines and healthcare organizations recommend universal screening to identify women at risk of perinatal mental disorders. The American College of Obstetricians and Gynecologists 6 and the American Academy of Pediatrics 7 recommend repeated mental-health screening during pregnancy and postpartum at regular ob-gyn and well-child visits. Barriers, however, hinder the implementation or widespread use of screening. Patient barriers include stigma or the fear of losing one’s parental rights. Systemic barriers include limited mental-health resources, overburdened public-health clinics, the inaccessibility of screening tools, or barriers to accessing services and mental-health supports following a positive screening.8,9 Many socially disadvantaged women do not attend the recommended visits.10,11 Screening shortly after giving birth, while still in the maternity hospital, presents a unique opportunity to start the mental-healthcare pathway, especially in countries like the Czech Republic, which lacks systematic care for postpartum women in the first six weeks after delivery. This early-detection approach may serve as an early entry into the psychosocial care system for at-risk women. 12 Nevertheless, a methodological question remains whether the presence of depressive symptoms shortly after giving birth can predict the presence of a psychiatric diagnosis at six weeks postpartum.
The Edinburgh Postnatal Depression Scale (EPDS) 13 is considered the gold standard for screening depressive symptoms in the perinatal period. This self-report questionnaire may also serve to identify the presence of other mental disorders, particularly anxiety.14–16 While originally designed for use at six weeks postpartum, it has also been validated for use during pregnancy. 17 Its use shortly (within three days) after delivery is somewhat controversial. Some studies report a good correlation between EPDS scores gathered at two different time points postpartum and therefore recommend its immediate postpartum use.18,19 Other studies oppose its use, pointing out its low sensitivity in predicting future difficulties. 20
To our knowledge, only one study by Jardri et al. 21 has focused on the relationship between immediate postpartum depressive symptoms assessed with the EPDS and future diagnosis of a major depressive episode assessed with a structured diagnostic interview. They concluded that the EPDS is a valid tool for immediate screening, despite its relatively low positive predictive value. We are unaware of any research that explores the predictive value of the EPDS for other mental disorder, even though depressive symptoms and sleep disturbances can be part of the prodromal stages of various mental disorders. 22
Therefore, our study aimed to evaluate whether the presence of depressive symptoms measured by the EPDS shortly after delivery can predict the presence of a major depressive episode diagnosis or other mental disorders (hypomanic episode, anxiety disorder, panic disorder, generalized anxiety disorder, agoraphobia, social phobia, obsessive-compulsive disorder, and psychotic disorders) at six weeks postpartum in Czech women.
Methods
The study protocol was registered with the Open Science Framework (https://doi.org/10.17605/OSF.IO/B46YZ). The study was approved by the Ethics Committee of The National Institute of Mental Health (Ref No. 130/20). We used the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement as guidance for writing the current article. The STROBE statement checklist is provided as a supplemental file.
Study setting
The study was conducted in the Czech Republic, where most women give birth in maternity hospitals and stay until two to three days postpartum. Their medical care during childbirth and postpartum is fully covered by mandatory public health insurance. Participants were women who had given birth in one of six selected maternity hospitals located across three of the 14 regions in the Czech Republic. Initial screening took place in maternity hospitals, and subsequent data collection occurred remotely via telephone.
Unlike in the United States or the United Kingdom, systematic perinatal healthcare in the Czech Republic does not exist. 12 In daily practice, it usually only involves individual specialists from general psychology and psychiatry. Women in need of psychotropic medication must see a psychiatrist for a prescription, as these medications cannot be obtained without an in-person consultation. The first postnatal gynecological check-up typically occurs six weeks after delivery. Currently, no universal perinatal mental-health screening has been adopted in the Czech Republic, although the EPDS is used in multiple maternity wards and gynecology clinics. The Czech version of the EPDS has recently been assessed for its psychometric properties. 3
Participants and recruitment
Data collection took place from November 2020 to May 2023 as part of a larger project (https://ClinicalTrials.gov Identifier: NCT04639752) testing the effectiveness of remote peer support in preventing postnatal depression. Following childbirth, medical staff offered eligible women the opportunity to participate in the study. We defined women as a binary category based on sex assigned at birth. Women over 18 years of age with a valid e-mail address and who understood and spoke Czech were eligible for the study. Those who provided written informed consent for participation completed questionnaires. Only participants with a score of ≥ 10 on the EPDS were included in the study. We chose this cutoff score based on recommendations from international data 23 for selecting women with depressive symptoms. Participants who reported receiving care from a mental-health professional in the postpartum period were also excluded from the analysis. Symptom alleviation due to professional care could affect the prevalence of mental disorders six weeks postpartum and thus influence outcomes toward poorer predictability. No remuneration was provided for participation.
Measurements
The Czech version of the Edinburgh Postnatal Depression Scale (EPDS) 13 was used to assess depressive symptoms within three days after delivery. The EPDS is a 10-item self-report instrument with items rated on a four-point scale, with a summative score ranging from 0 to 30. Higher scores indicate a greater severity of depressive symptoms. Consistent with prior studies, we used a cutoff score of 10 to identify women who present depressive symptoms.3,23 The EPDS may also serve to identify the presence of other mental disorders.14–16 The Czech version has recently been psychometrically validated (Cronbach’s α = 0.863). 3
The presence of a postpartum mental disorder was assessed using the Mini-International Neuropsychiatric Interview 5 (MINI). 24 The MINI is a brief, structured diagnostic interview designed to assess psychiatric conditions in accordance with both the International Classification of Diseases, Tenth Revision (ICD-10), and the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV). In this study, diagnoses were coded according to DSM-IV criteria. The MINI is a widely recognized and psychometrically validated tool, and its use by telephone has also been validated. 25
Procedures
Within two to five days after childbirth, participants completed demographic information and the EPDS on tablets provided by the medical staff. Participants with a score of ≥ 10 on the EPDS were considered at risk of developing a postpartum mental disorder and were included in the study.
At six weeks postpartum, these women were contacted via telephone for the MINI interview. Contact attempts were made three times. If they were unreachable or declined to answer, they were excluded from the analysis. Two psychiatrists administered the MINI to determine the presence of a major depressive episode, hypomanic episode, panic disorder, generalized anxiety disorder, agoraphobia, social phobia, obsessive-compulsive disorder, or psychotic disorders. Participants were asked whether they had received care from a mental-health professional in the postpartum period; those who had were excluded from the analysis.
Statistical analysis
Statistical analysis was conducted using STATA software (version 17.0) and IBM SPSS Statistics (version 20). Descriptive data, including the frequency count (n) of respondents with specific mental disorders and the corresponding prevalence rates (%) for each mental disorder, along with 95% confidence intervals (CI), were calculated.
Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for various EPDS cutoff scores were calculated. Sensitivity expresses the probability that the test will be positive in individuals who have the condition. Specificity expresses the probability that the test will be negative in individuals who do not have the condition. Positive predictive value (PPV) indicates the probability that an individual who receives a positive test result has the condition of interest. Negative predictive value (NPV) expresses the probability that an individual who receives a negative test result does not have the condition. 26
Receiver Operating Characteristic (ROC) curve analysis was used to evaluate the EPDS’s ability to predict mental disorders, with the Area Under the Curve (AUC) quantifying the overall ability to distinguish between groups. 27
Results
A total of 8,463 participants initially completed the demographic questionnaire and the EPDS.
After excluding 6,544 participants with EPDS scores < 10, six participants were excluded due either to incomplete EPDS responses or duplications in their responses. This resulted in 1,913 participants who were enrolled and later contacted at six weeks postpartum to complete the MINI interview. After three unsuccessful contact attempts, 1,114 participants were excluded from the study. Additionally, 78 participants provided incorrect telephone numbers, rendering them unreachable, and 257 women chose not to continue their participation. Twenty-six MINI assessments were conducted later than six weeks postpartum and had to be excluded from the analysis. Another 35 women reported receiving professional mental-healthcare during the postpartum period and were excluded from the analysis as well. Consequently, the final analyzed sample consisted of 403 women. Figure 1 provides a flowchart of the participant enrollment. Flowchart of participants abbreviations: EPDS, Edinburgh Postnatal Depression Scale; MINI, Mini-International Neuropsychiatric Interview.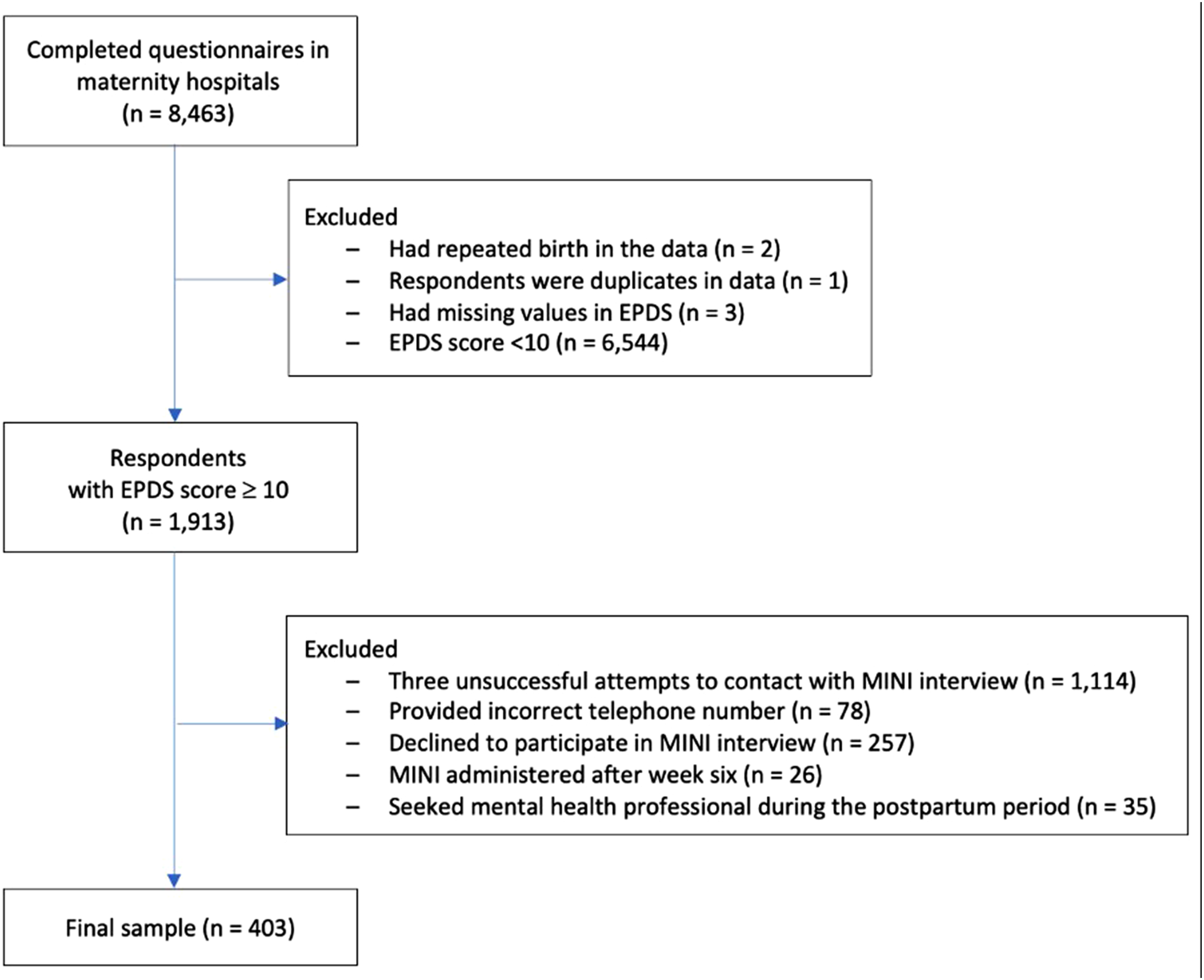
Prevalence of mental disorders six weeks postpartum assessed using the MINI.

Study sample N = 403.
Sample includes participants with EPDS score ≥ 10.
Abbreviations: MINI, Mini-International Neuropsychiatric Interview 5; 95% CI, 95% confidence interval.
A cut off score of ≥ 16 was identified as optimal for predicting a major depressive episode at six weeks postpartum. The sensitivity was 0.71, and the specificity was 0.84. The PPV of a score of ≥ 16 was 14%, and the NPV was 99%. The AUC value was 0.78 (95% CI 0.64–0.92, P < .001).
For screening for any mental disorder (including a major depressive episode), a cutoff score of ≥ 14 was optimal, with sensitivity of 0.65 and specificity of 0.73. The PPV was 24%, and the NPV was 94%. The AUC value was 0.69 (95% CI 0.60–0.77, P < .001).
Figure 2 illustrates the predictive ability of the EPDS for (A) major depressive episode and (B) any observed mental disorder using the ROC curve. ROC curve for detecting (a) a major depressive episode or (b) any observed mental disorder six weeks postpartum using the Edinburgh Postnatal Depression Scale. Abbreviations: ROC, receiver operating characteristic.
Sensitivity, specificity, and other properties of The Edinburgh Postnatal depression scale for detecting a major depressive episode or any observed mental disorder six weeks postpartum.

Abbreviations: EPDS, Edinburgh Postnatal Depression Scale; PPV, positive predictive value; NPV, negative predictive value; AUC, area under curve value; N/A, not available.
Only EPDS scores ≥ 10 were analyzed.
Discussion
The aim of this study was to determine whether the presence of depressive symptoms measured by the EPDS within three days after delivery can predict the presence of a major depressive episode and other mental disorders at six weeks postpartum among Czech women.
We found that while the EPDS administered shortly after delivery showed high negative predictive values (NPV) within our high-risk sample, its positive predictive value (PPV) for diagnosing specific psychiatric disorders was relatively low. These findings suggest that immediate postpartum negative screening is particularly useful for ruling out future severe psychopathology in symptomatic women, but positive screening is not a precise indicator of development of major depressive episode at six weeks postpartum.
Limited data exist on the predictive power of the presence of depressive symptoms assessed with screening tools shortly postpartum for psychiatric diagnoses assessed with a structured diagnostic interview. Previous research has focused mainly on the ability of the EPDS to detect current symptoms of depression. 23 Other studies compared EPDS scores collected at two different time points: within three days and several weeks postpartum.18–20,28 Overall, they found a good correlation between scores, indicating stability of (especially low) scores over time, but not necessarily the presence of an actual mental disorder. Nevertheless, authors of those studies 28 concluded that immediate screening in maternity hospitals is effective and can help redirect the limited available resources toward follow-up focused exclusively on the women at risk.
Universal screening for early detection of mental-health symptoms, followed by the subsequent specification of a diagnosis and the severity of symptoms, constitute the initial steps in the pathway of postnatal mental healthcare. 4 Screening in maternity hospitals presents a unique opportunity to reach a large population of women at risk who could otherwise be lost in the system.8–10 At the same time, precise identification of a woman’s symptoms and their severity and appropriate referral to the most suitable form of care are essential to the effective distribution of available care options, which are limited in many countries, including the Czech Republic.29–31 However, the timing and interpretation of such screening require careful consideration.
If our goal is to implement screening that culminates in referrals to professional care, it is crucial to achieve a high NPV to ensure that we do not miss individuals who may develop mental disorders later. Our results indicate that this is achievable in the setting of maternity hospitals, but it is crucial to interpret this finding strictly within the context of our study design, which specifically selected women with elevated depressive symptoms (EPDS ≥ 10). Within this symptomatic population, the EPDS proved effective for ruling out severe pathology. On the other hand, the relatively low Positive Predictive Value (PPV) indicates that many women with high initial EPDS scores did not meet the diagnostic criteria for a mental disorder at six weeks postpartum.
The low PPV raises important clinical and ethical questions. It is important not to interpret these “false positives” simply as an error of the instrument or a waste of healthcare resources. Perinatal mental health exists along a continuum rather than as a binary distinction between “disorder” and “no disorder.” Women with elevated scores who do not meet the criteria for a formal diagnosis often experience subthreshold depressive or anxiety symptoms that can be functionally impairing. Framing screening outcomes solely in terms of diagnostic thresholds risks overlooking this clinically meaningful group who, while not necessarily requiring specialized psychiatric treatment, may still benefit from psychosocial support.
Furthermore, administering the EPDS within the first days after childbirth also presents ethical challenges. On one hand, the maternity hospital setting offers a unique and critical window of opportunity to engage with women who might otherwise be lost to follow-up. This is particularly relevant in healthcare systems like the Czech Republic, where postpartum care such as routine home visits by midwives is not part of standard practice. Consequently, discharge from the maternity hospital often marks the beginning of a “care gap” lasting until the six-week gynecological check-up. For many women, the screening in the maternity hospital may be the only contact with healthcare professionals focused on their well-being before the potential onset of severe symptoms. On the other hand, the immediate postpartum period is characterized by substantial emotional, physical, and hormonal fluctuations (often referred to as “baby blues”), which can transiently inflate EPDS scores without indicating a lasting disorder. This raises valid concerns about the timing of screening. Implementing a formal screening tool during this particularly vulnerable period carries the risk of over-identification, pathologizing normal postpartum adjustment, and placing an emotional burden on new mothers.32,33
Our study marked that the early screening is feasible, but its clinical utility depends on how the results are communicated and managed. A possible approach is the integration of the EPDS into broader, tiered screening frameworks. Existing guidelines, such as those by the National Institute for Health and Care Excellence (NICE), 34 advocate for a stepped approach beginning with ultra-brief instruments, such as the two-item Whooley questions, where the EPDS serves as a secondary assessment tool reserved for women who screen positive on initial inquiries. Recent studies also concluded that the stepped approach was cost effective compared to standard care or the use of a single screening tool administered at a single time point.35,36
Given the fact that the original development of the EPDS did not consider immediate postpartum use, the EPDS alone may not be the optimal standalone instrument for this timeframe. Future research could focus on developing a new screening instrument adapted to this specific period. Such a tool could consider various psychosocial and medical factors, including a history of mental disorders, domestic violence, substance misuse, adverse childhood experiences, deprived socioeconomic background, or high-risk pregnancies or deliveries.37,38
Tiered screening models and referral pathways need to be adapted to the local cultural and healthcare context, as studies in several low- and middle-income countries have shown that local language versions of the EPDS often have lower precision for identifying true cases of perinatal mental disorders than the original English version. 39
Limitations
The results of our study should be interpreted in the context of its limitations. First, this study included only women with depressive symptoms at the time of screening (EPDS ≥10). This cutoff was selected based on international recommendations to specifically evaluate the predictive value of early symptomatic distress. However, by excluding women with lower EPDS scores, the study may have missed important information about symptom distribution and the tool’s ability to identify both low- and moderate-risk women. Consequently, key screening properties—such as sensitivity, specificity, and negative predictive value in a universal screening context—cannot be fully assessed.
Additionally, excluding women who reported receiving mental health care in the postpartum period may further limit the representativeness of the sample. While this was done to evaluate the predictive validity of the EPDS on the natural course of symptoms without intervention, we acknowledge that this could bias the results toward a “healthier” or less complex subgroup, as women who sought help may represent the true positive cases with the most severe needs.
The MINI was not conducted immediately postpartum, preventing a direct comparison of changes in the prevalence of mental-health disorders assessed with the diagnostic interview at two time points. Therefore, we cannot definitively say whether the results were influenced by changes in the prevalence of disorders or whether the predictive ability of the EPDS was insufficient at any time point.
We acknowledge the substantial loss to follow-up in our study, as well as the limited number of participants diagnosed with mental disorders, both of which could influence the predictive values calculated from the completer sample. This study is a secondary analysis of data collected within a larger randomized controlled trial. As such, no a priori sample size calculation specific to this analysis was performed. Recruitment procedures and sample size were determined by the parent project, which limits the statistical power for predictive validity analyses. Demographic and psychosocial characteristics were not comprehensively collected, preventing formal comparisons between women who completed follow-up and those who were lost. This limitation makes it difficult to determine whether selection bias influenced our results. Certain subgroups—such as women from lower socioeconomic backgrounds—may have been underrepresented, while women with better mental health could have been more likely to continue participation due to greater capacity or motivation, potentially affecting the generalizability of our findings. Nevertheless, our study aimed to maintain a naturalistic design with minimal exclusion criteria, reflecting the real-world distribution of EPDS scores and postpartum mental health. Finally, the study was conducted on a population of Czech women, limiting its generalization to entire populations outside of the Czech Republic.
Strengths
This study also has notable strengths. One key strength is its use of standardized and well-validated tools for both the initial screening and diagnostic follow-up. In many cases, only a screening tool like the EPDS is used to determine the prevalence of postpartum depression. In our study, the MINI was administered by psychiatrists to assess psychiatric diagnoses. The use of this established instrument ensures the reliability and validity of the data collected.
The study leverages the national system of maternity hospitals covered by the Czech Republic’s public health insurance. This integration underscores the feasibility of implementing similar screening and follow-up protocols within existing healthcare infrastructures.
Conclusion
Our study, conducted on a sample of women with elevated depressive symptoms (EPDS ≥ 10), indicates that early postpartum screening can be useful in identification of women in low risk of development of major depressive episode six weeks postpartum. However, the interpretation of these findings requires caution. While the high NPV within this symptomatic group supports the utility of the EPDS for ruling out severe pathology, the relatively low PPV suggests that elevated scores often reflect transient distress rather than a confirmed disorder. Our results underscore the need for a more suitable screening tool, which could consider other medical and psychosocial variables. Furthermore, employing a tiered or repeated screening process only for women at risk (e.g., Whooley questions followed by the EPDS) could enhance screening accuracy and minimize patient burden. Where the EPDS remains the standard method, we recommend interpreting results through a tiered management strategy based on our findings within a high-risk sample: EPDS item 10 (suicidal ideation) must prompt immediate referral; EPDS scores ≥16 have a higher probability of a disorder and should be prioritized for diagnostic follow-up; women with intermediate scores (EPDS 10–15) may not meet diagnostic criteria, but they likely require active monitoring, repeated screening, or psychosocial support to prevent symptom escalation; and although our study did not evaluate women with scores < 10, standard clinical practice suggests that routine postnatal care remains appropriate for this group.
Significance for public health
This study highlights the critical importance of early detection and intervention in postpartum mental health. By evaluating the predictive value of the Edinburgh Postnatal Depression Scale (EPDS) administered shortly after delivery, our findings underscore the potential for initiating mental health care pathways within maternity hospitals. Identifying women at risk of developing psychiatric disorders as early as two to five days postpartum allows for timely intervention, which can mitigate long-term mental health consequences for both mothers and their families. Implementing such screening in maternity hospitals could bridge existing gaps in perinatal mental health care. This approach could enhance the allocation of limited mental health resources, ensuring that at-risk women receive the necessary support and care, ultimately improving maternal and child health outcomes.
Supplemental material
Supplemental material - Immediate postpartum depressive symptoms and future psychiatric diagnoses: A predictive analysis using the EPDS
Supplemental material for Immediate postpartum depressive symptoms and future psychiatric diagnoses: A predictive analysis using the EPDS by Kristyna Hrdlickova, Marie Kuklova, Hana Nemcová, Anna Horakova, Nancy 1Byatt and Antonin Sebela in Journal of Public Health Research.
Supplemental material
Supplemental material - Immediate postpartum depressive symptoms and future psychiatric diagnoses: A predictive analysis using the EPDS
Supplemental material for Immediate postpartum depressive symptoms and future psychiatric diagnoses: A predictive analysis using the EPDS by Kristyna Hrdlickova, Marie Kuklova, Hana Nemcová, Anna Horakova, Nancy Byatt and Antonin Sebela in Journal of Public Health Research.
Footnotes
Acknowledgements
The authors wish to thank all study participants and the staff of participating maternity hospitals for their support and contribution to data collection. No additional external acknowledgements are applicable.
Ethical considerations
The study was approved by the Ethics Commission of the National Institute of Mental Health (Ref No. 130/20). All participants provided written informed consent.
Consent to participate
All participants provided written informed consent. Participants provided consent to conduct and publish the study. Participant information has been anonymized.
Author contributions
Kristyna Hrdlickova contributed to conceptualization and methodology, performed the statistical analyses, and drafted the original manuscript. Marie Kuklova assisted with statistical analyses, curated and cleaned the dataset, prepared the figures and tables, and contributed to writing the initial draft. Hana Nemcova curated the dataset, helped interpret the findings, and revised the manuscript. Anna Horakova and Nancy Byatt contributed to interpreting the results and provided critical revisions throughout the manuscript. Antonin Sebela oversaw the study as principal investigator, developed the study concept and design, supervised the analyses, managed the project, secured funding, and contributed to manuscript writing and revisions. All authors have read and approved the final version of the manuscript and take responsibility for its content.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Czech Health Research Council [grant number NU31J-09-00064] and the Cooperatio Neurosciences, Third Faculty of Medicine, Charles University. The funding source had no involvement in study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This work was supported by the Czech Health Research Council [grant number NU31J-09-00064]. KH, MK, HN, AH and AS have received salary from this grant. They have no other conflict of interest. NB has received salary and/or funding support from Massachusetts Department of Mental Health via the Massachusetts Child Psychiatry Access Program for Moms (MCPAP for Moms). She is also the Medical Director of Research and Evaluation for MCPAP for Moms and the Executive Director of the Lifeline for Families Center at U Mass Chan Medical School. NB has received honoraria from Global Learning Collaborative. She has also served as a consultant for The Kinetix Group, VentureWell, and JBS International.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.