
Abstract
Background
The hyperosmolar hyperglycemic state (HHS) is a rare but life-threatening complication of diabetes. Evidence on hyperglycemic emergencies, including HHS and their predictors in Ethiopia, is limited, and predictors specific to HHS are not well characterized. Therefore, this study aimed to determine the incidence of hyperosmolar hyperglycemic state and its predictors among adult diabetic patients in eastern Ethiopia.
Method
A retrospective cohort study was conducted among 461 adults with diabetes from January 1, 2019, to December 31, 2024. Data were collected using the Kobo Toolbox and analyzed with STATA. Survival probabilities were estimated using the Kaplan-Meier curve. Predictors of HHS were identified using the Weibull proportional hazards regression model. Hazard ratios (HR) with their respective 95% confidence intervals (CI) and p-values were computed.
Results
From the total of 452 patients included in the study, 45 (9.96%), 95% CI (7.51%-13.08%) developed hyperosmolar hyperglycemic state. The incidence rate of HHS was 5.36 cases per 100 person-years of observation, 95% CI (4.00-7.18), which was 3.89 and 5.76 per 100 person-years among T1DM and T2DM, respectively. Factors significantly associated with HHS included being rural area residents (AHR: 1.99, 95% CI: 1.01–3.92), having comorbidities (AHR: 3.01, 95% CI: 1.28–7.05), medication non-adherence (AHR: 2.14, 95% CI: 1.04–4.40), and lack of community health insurance (AHR: 2.04, 95% CI: 1.03–4.04).
Conclusion
HHS occurred more frequently among patients with T2DM. Strengthening follow-up and targeted interventions, particularly for rural residents, patients with comorbidities, those without community health insurance, and those with medication non-adherence, may reduce HHS occurrence.
Introduction
Diabetes mellitus (DM) is a chronic metabolic disorder characterized by persistent hyperglycemia. 1 As the global prevalence of diabetes continues to rise, particularly in low- and middle-income countries, the burden of its acute and chronic complications has become a significant public health concern. 2 Among the acute complications, the hyperosmolar hyperglycemic state (HHS) stands out as a rare but life-threatening emergency, predominantly affecting individuals with type 2 diabetes mellitus (T2DM).1,3 HHS is distinguished by extreme hyperglycemia, marked hyperosmolarity, and dehydration, often without significant ketoacidosis. 4 If not promptly recognized and managed, HHS carries a high risk of morbidity and mortality, with reported case fatality rates ranging from 10% to 20% in various settings.4,5
The pathophysiology of HHS involves a complex interplay of insulin deficiency and increased counter-regulatory hormones, which lead to profound hyperglycemia and osmotic diuresis. 3 Despite advances in diabetes care, HHS remains a diagnostic and therapeutic challenge, especially in resource-limited settings where delayed presentation and limited access to care may worsen outcomes. 6
Globally, the burden of hyperglycemic emergencies is shifting toward low- and middle-income countries (LMICs). In Sub-Saharan Africa and South Asia, the incidence of hyperglycemic emergencies is estimated to account for up to 30% of diabetes-related hospital admissions. 7 The hyperosmolar hyperglycemic state (HHS), in particular, has a significantly higher case fatality rate (10–50%) compared to diabetic ketoacidosis (2–5%) due to delayed clinical recognition and limited diagnostic infrastructure.8,9
A Danish nationwide cohort study found an incidence of HHS of 3.9 per 10,000 person-years in type 2 diabetes mellitus and 16.5 per 10,000 person-years in type 1 diabetes, noting that one-third of HHS cases were newly diagnosed diabetes. 10 Conversely, a previous study in Ethiopia reported an incidence of HHS of 0.9 per 100 person-years in type 1 diabetes and 2.4 per 100 person-years in type 2 diabetes. 11 Studies conducted in different parts of the world have identified several predictors of HHS, including infections, poor glycemic control (high HbA1c), use of glucocorticoids and benzodiazepines, dehydration, acute illnesses, medication non-compliance, and comorbidities.10–13 Moreover, HHS often overlaps with DKA(14), yet it disproportionately affects adults with type 2 diabetes and carries a higher mortality risk.14,15
Most studies on HHS have been conducted in high-income countries, and their findings may not be directly applicable to the Ethiopian context due to differences in healthcare infrastructure, patient demographics, and disease patterns. Even the few available studies on all hyperglycemic emergencies often lack regional specificity or comprehensive analysis. Understanding the local epidemiology of HHS is crucial for developing targeted prevention and management strategies. 3
Given these gaps, this study was designed to determine the incidence of hyperosmolar hyperglycemic state and to identify its predictors among adult diabetic patients in public hospitals in the Harari region, eastern Ethiopia. By elucidating the factors associated with the development of HHS, the findings aim to inform clinical practice and health policy, ultimately contributing to improved outcomes for diabetic patients in the region.
Methods and materials
Study design, setting, and period
A retrospective cohort study was carried out among adult diabetes mellitus patients receiving follow-up care from January 01, 2019 to December 31, 2024 (cohort follow-up period) and data were abstracted retrospectively from medical records during January 01 to January 31, 2025, in public hospitals located in the Harari region, which is situated in the Harari regional state, approximately 526 kilometers from Ethiopia’s capital, Addis Ababa. The Harari region has an estimated population of 283,000, with a male-to-female ratio of 1:1. 16 The region is served by two public, two private, one police, and one non-government hospital. Additionally, there are 9 health centers, 29 private clinics, 26 health posts, and one regional laboratory serving the community. The study was conducted in two public hospitals within the region: Hiwot Fana Comprehensive Specialized University Hospital (HFCSUH) and Jugal General Hospital (JGH). HFCSUH, a large teaching hospital with 210 beds, serves as a major referral center for approximately 5.8 million people in eastern Ethiopia. 17 Jugal General Hospital, on the other hand, has 95 beds and primarily serves the population of Harar town. Currently, around 1,500 DM patients visit these two hospitals for regular follow-up care, with 852 patients at HFCSUH and 648 at JGH. 18
Populations
All adult DM patients on chronic follow-up for treatment at public hospitals in the Harari region were considered as the source population. The study population consisted of all adult DM patients on chronic follow-up between January 01, 2019, and December 31, 2024.
Eligibility criteria
Adult DM patients enrolled in the chronic follow-up care at public hospitals in the Harari region, who were diagnosed between January 1, 2019, and December 31, 2024, were included in the study. However, patients who developed HHS at the time of their initial diabetes diagnosis and those who were transferred in from other facilities were excluded.
Sample size and sampling procedures
The final sample size of 461 was determined using the Schoenfeld formula via Stata software version 17, employing power analysis for the Cox proportional hazard model. 19 This was calculated by considering a 17.7% probability of an event (cumulative incidence of HHS) and an AHR of 0.5 from a previous study. 10 We assumed a 95% confidence interval, 80% power, and 20% of withdrawal probability.
All public hospitals in the Harari region, namely Hiwot Fana Comprehensive Specialized University Hospital and Jugal General Hospital, were selected. Before sample allocation, the number of newly diagnosed DM patients who visited both hospitals for follow-up care within the study period was determined.
The total sample size of 461 was distributed proportionally between the two hospitals based on the number of diabetic patients receiving follow-up care at each facility. A list of medical record numbers for adults diagnosed with diabetes was compiled using diabetic follow-up logbooks from both hospitals. Finally, the required participants were randomly selected from the sampling frame (a list of diabetic patients enrolled between January 1, 2019, and December 31, 2024) using Excel-generated random numbers (Figure 1). Schematic presentation of the sampling procedure for DM patients at public hospitals of Harari region, Eastern Ethiopia, 2025.
Study variables
The incidence of HHS was the main outcome variable. Independent variables included socio-demographic factors (such as age, sex, residence, and community health insurance), clinical factors (including BMI, family history of diabetes, recent infections, type of diabetes, glycemic control, duration of diabetes, presence of comorbidities, systolic and diastolic blood pressure, and chronic diabetic complications), and treatment factors (such as frequency of diabetes follow-up, type of medication used, duration of treatment, and medication non-adherence).
Data collection and quality control
Data were collected using a data extraction format adapted from various relevant studies.11,12,20–22 The internal consistency of the adapted tool was assessed using Cronbach’s alpha coefficient, yielding a value of 0.815, indicating good reliability. This format consisted of five sections: general information, socio-demographic characteristics, clinical characteristics, treatment-related parameters, and the follow-up form. Initially, all DM patients on chronic follow-up between January 1, 2019, and December 31, 2024, were identified from the DM registration book. Eligible adult patients were then randomly selected using Excel-generated random numbers, after excluding individuals who developed HHS at their initial DM diagnosis and those who were transferred in. Data were collected from patients’ charts using a pretested data extraction format. Medical registration numbers were used to identify reviewed records. The data collection was conducted by two BSc public health professionals experienced in data collection, supervised by a trained BSc nurse working in chronic follow-up and an MPH public health professional.
To ensure data quality, data collectors and supervisors received a one-day training session focused on the data extraction system, data collection tools, and the study’s objectives. Before the main data collection, a pretest was conducted at HFCSUH on 5% 23 of the sample size, and necessary adjustments were made to the data extraction format based on the findings. A week before data collection began, patient charts were cross-checked to confirm the adequacy of the instruments, ensure the checklist of tools was completed on time, and verify the completeness of data in the charts. Close monitoring and supervision were conducted throughout the data collection period by both the principal investigator and the supervisors. Data collectors received daily feedback to address any issues. The collected data were reviewed for completeness before analysis. To minimize misclassification bias, uniform ascertainment criteria were applied for clinical variables with multiple diagnostic criteria. Missing data were addressed using a complete case analysis.
Operational definitions
Data processing and analysis
After completing data collection, the data were exported from the Kobo Toolbox to Microsoft Excel and then imported into STATA software version 17 for further cleaning and analysis. Basic descriptive analyses were conducted. Each patient was followed until either the occurrence of HHS or one of the censoring events, whichever came first. Survival analysis was employed as the statistical model to assess the associations between HHS incidence and its predictors. The HHS-free survival probability was calculated in months, based on the time interval between diabetes mellitus (DM) diagnosis and either the date of HHS occurrence or censoring. The incidence rate of HHS was also computed. Life tables were used to estimate the survival probabilities at different time intervals following the diagnosis of DM. Kaplan-Meier survival curves and log-rank tests were performed to estimate survival probabilities and to statistically compare survival across different predictor categories, respectively.
To identify predictors of HHS, both the Cox proportional hazard (PH) model and three parametric models (Weibull, exponential, and Gompertz) were fitted. The most parsimonious model was selected based on the Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), and log-likelihood values. Based on these criteria, the Weibull PH regression model was identified as the most efficient for describing the data.
The Schoenfeld residuals test was employed to evaluate the proportional hazards assumption for individual predictors as well as for the overall model using global tests. 19 Each predictor had a P-value greater than 0.05, and the overall global test had a P-value of 0.47, confirming that the proportional hazards assumption was not violated. A log-log plot of survival was used to evaluate the predictors, and the variables in the final model yielded parallel curves, confirming the proportional hazards assumption. Multicollinearity was assessed using the variance inflation factor (VIF = 1.76), suggesting no significant multicollinearity among the independent variables.
A Weibull PH regression model was used to identify the predictors of HHS. Variables with p-values < 0.25 in the bi-variable analysis were candidates for a multivariable Weibull PH regression model. Hazard ratios (HR) with their corresponding 95% CI were used to show significance and strength of the association with the outcome variable. Variables with a p-value < 0.05 in the multivariable Weibull PH regression model were considered significant and independently associated with the outcome variable. The goodness of fit of the model was assessed by using the Cox–Snell residual technique. The cumulative hazard plot follows a straight line through the origin with slope, indicating that the model fits the data well (Figure 2). Cox–Snell residual plots for Weibull PH model of adult patients with diabetes at public hospitals of Harari region, Eastern Ethiopia, 2025. (N=452).
Ethical considerations
Ethical clearance and approval were obtained from the Institutional Health Research Ethics Review Committee (IHRERC) of Haramaya University College of Health and Medical Sciences. A cooperation letter was issued by Haramaya University College of Health and Medical Sciences to the respective hospitals. Informed, voluntary, written, and signed consent was obtained from the hospital head. After obtaining ethical approval, data were collected from patient charts using a checklist, with codes used to maintain confidentiality. The completed checklist was stored securely in a locked location. The entered data was protected with a password on the computer. The data was used solely by the principal investigator.
Result
Socio-demographic characteristics
Incidence of HHS and socio-demographic characteristics of diabetes patients at public hospitals of Harari region, Eastern Ethiopia. (N=452).

CBHI, community-based health insurance.
Clinical and treatment characteristics of patients with diabetes mellitus
Clinical and treatment-related results of adult patients with diabetes at public hospitals of Harari region, Eastern Ethiopia. (N=452).
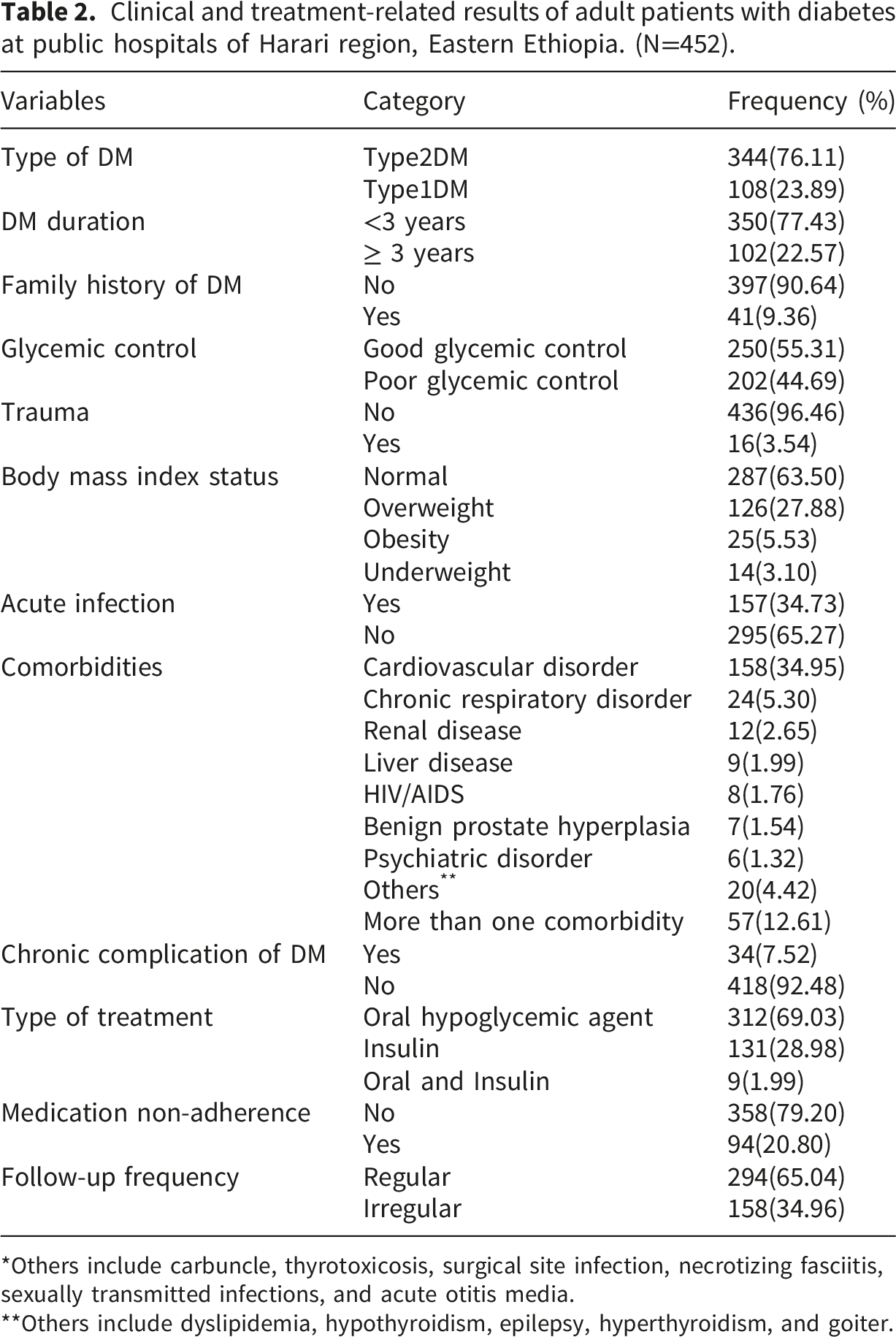
*Others include carbuncle, thyrotoxicosis, surgical site infection, necrotizing fasciitis, sexually transmitted infections, and acute otitis media.
**Others include dyslipidemia, hypothyroidism, epilepsy, hyperthyroidism, and goiter.
Incidence of hyperosmolar hyperglycemic state
Out of 452 patients followed over five years, 45 developed HHS (9.96%; 95% CI: 7.51%–13.08%), while the majority (90%) were censored (Figure 3). The overall incidence rate was 5.36 cases per 100 person-years (95% CI: 4.00–7.18). Specifically, the rate was higher among patients with T2DM (5.76) than those with T1DM (3.89) per 100 person-years. Incidence was notably higher in rural residents (8.28; 95% CI: 5.71–11.99) and older individuals aged ≥ 65 years (6.18; 95% CI: 2.78–13.76) per 100 person-years. Throughout the follow-up period, the highest incidence of HHS was recorded between the 12-to-18-month follow-up intervals (Table 3). HHS-free survival probability declined over time, reaching 82.11% by the end of the follow-up period. The median HHS-free survival time for the entire cohort was undefined, as the survival curve did not cross the 50% threshold, indicating that more than half of the cohort remained HHS-free at the last recorded time point. (Figure 4). Bar graph showing the status of HHS among adult patients with diabetes at public hospitals of Harari region, Eastern Ethiopia. (N=452). Life table showing the survival to develop HHS among adult diabetic patients at public hospitals of Harari region, Eastern Ethiopia. (N=452). Kaplan–Meier survival curve of HHS-free survival estimate of adult patients with diabetes at public hospitals of Harari region, Eastern Ethiopia. (N=452).


Predictors of hyperosmolar hyperglycemic state
Bivariate and multivariate Weibull proportional hazards regression of predictors of HHS among DM patients at public hospitals in the Harari region, East Ethiopia.

CBHI, community-based health insurance.
Accordingly, patients from rural areas had a 99% higher hazard of developing HHS compared to those from urban areas (AHR: 1.99, 95% CI: 1.01, 3.92). Diabetes mellitus patients without CBHI had a two-fold higher probability of HHS than those with CBHI (AHR: 2.04, 95% CI: 1.03, 4.04). Regarding treatment adherence, the risk of HHS was 2.14 times higher among patients with medication non-adherence compared to those who were adherent (AHR: 2.14; 95% CI: 1.04, 4.40). Similarly, the hazard of HHS was three times higher in patients with comorbidities than in those without (AHR: 3.01; 95% CI: 1.28, 7.05) (Table 4).
Discussion
This study investigated the incidence and predictors of HHS among diabetic patients in Eastern Ethiopia. The incidence rate of HHS in this study was much higher than the national reports from the United States (0.9 per 1000 person-years) 26 and Denmark (20.4 per 10,000 person-years(16.5 and 3.9 among people with known type 1 and type 2 DM, respectively)), 10 and higher than study conducted Bahar Dar, Ethiopia (2.1 per 100 person-years (0.9 and 2.4 among T1DM and T2DM, respectively)). 11 The higher incidence rates of HHS in this study may be attributed to its institution-based design, in contrast to nationwide studies. The incidence rate of HHS in this study was higher among individuals with type 2 diabetes mellitus, in contrast to a study conducted in Denmark, which reported a higher incidence rate among individuals with type 1 diabetes mellitus. 10 This discrepancy highlights the importance of considering specific population characteristics and regional factors when assessing the risk and incidence of HHS. The cumulative incidence in this study was lower than reported rates in China (46.8%), 11 Atlanta (35%), 27 and Nigeria (58.3%). 13 These discrepancies may be attributed to differences in study populations, socioeconomic status, culture, lifestyles, and environmental factors, all of which influence glycemic control and diabetes management. 28
This study identified a significant link between rural residence and HHS, which is consistent with a study conducted in Iraq. 29 The association could be due to limited access to healthcare, poorer glycemic control, and socioeconomic issues, all of which contribute to poor diabetes management and its complications. 30 This aligns with findings from other Ethiopian contexts, where the ‘distance decay’ effect is interpreted through Andersen’s Behavioral Model. Service utility decreases as distance increases, which often leads to delayed presentation of hyperglycemic emergencies. 31
The incidence of HHS was greater among DM patients with comorbidities in comparison to those without comorbidities. This finding is consistent with studies conducted in Bahar Dar, Ethiopia 11 and in Sidama, Ethiopia. 32 This may be due to comorbidities and their associated medications, which can disrupt the normal functions of insulin and other counter-regulatory hormones, either directly or indirectly. Furthermore, diabetic patients with chronic medical comorbidities often experience poor glycemic control. 33
In this study, patients without community health insurance were positively associated with HHS. This agrees with a study conducted in Bahar Dar, Ethiopia 11 and South Africa. 34 The reason might be that patients without community health insurance are less likely to afford regular self-blood glucose monitoring, and the costs of follow-up examinations. 35 Furthermore, the lack of CBHI acts as a financial barrier to secondary prevention, such as routine blood glucose monitoring. In Ethiopia, CBHI membership has been shown to increase outpatient department visits by up to 43%, suggesting that those without insurance are more likely to delay care until an acute crisis like HHS occurs. 36
Medication non-compliance was positively associated with HHS in this study. This finding aligns with a previous study conducted in China, 37 in Nigeria, 13 and in Bahar Dar, Ethiopia. 11 This may be due to medication non-compliance, which disrupts the management of diabetes, leading to increased risks for severe complications like HHS. 38 This also aligns with the Health Belief Model. Previous evidence from the Harari region, Ethiopia, indicates that diabetic patients often have low perceived severity regarding complications and low self-efficacy for self-care practices. When patients do not perceive the immediate threat of asymptomatic hyperglycemia, adherence to daily regimens drops. 31
Strengths and limitations of this study
A key strength is the utilization of five years of follow-up data, which allows for the assessment of hyperglycemic hyperosmolar state (HHS) incidence over time and offers a comprehensive understanding of the condition. However, the retrospective design limits the inclusion of all potential factors influencing HHS, and the possibility of misclassification bias may affect the validity of the results. Specifically, because the HHS diagnosis relied on clinical records, some cases may have been miscoded as DKA or mixed states. This likely resulted in an underestimation of the true HHS incidence rate. Additionally, reliance on physicians’ clinical judgments for defining and diagnosing HHS may introduce inconsistency or unreliability. Other limitations include the inability to assess time-varying exposures and limited generalizability beyond public hospital attendees.
Conclusion
In this study, 10% of diabetes patients developed a hyperosmolar hyperglycemic state. The incidence rate of hyperosmolar hyperglycemic state was found to be higher among patients with T2DM compared to T1DM. Diabetes programs should adopt a T2DM-targeted HHS prevention and early-detection policy. Rural residence, comorbidities, medication non-adherence, and lack of community health insurance were found to be significantly associated with the hazard of HHS. To mitigate these risks, the Harari Regional Health Bureau should prioritize the expansion of CBHI enrollment specifically for chronic disease patients to remove financial barriers to monitoring. Furthermore, decentralizing diabetes follow-up care to rural health centers could reduce the distance decay effect identified in this study. Clinical practice should incorporate targeted patient education to improve medication adherence and early symptom recognition. Finally, we recommend that future prospective follow-up studies incorporate time-dependent covariates to account for variables that change over time and to address the missed variables.
Footnotes
Acknowledgments
We would like to thank institutional health research ethics review Committee of Haramaya University College of Health and Medical Sciences for its ethical approval. We would also like to thank the Harari region public hospital administrative bodies and card room workers for their cooperation. Finally, we would like to thank data collectors and supervisors for their commitment during data collection.
Ethical considerations
The studies involving humans were approved by the Institutional Health Research Ethics Review Committee of the Haramaya University College of Health and Medical Sciences (IHRERC/149/2024). The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin due to retrospective nature of the study.
Author contributions
BS, AG, and AT were involved in the conception and design, acquisition of data, analysis, and interpretation of data. DF and SD were involved in data curation, software used, and revising contents until the final version was prepared for publication. Finally, all the authors read and approved the final version and agreed on all aspects of this work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors upon request and without undue reservation.
Patient and public involvement
Patients and/or the public were not involved in the design, conduct, reporting, or dissemination plans of this research.