
Abstract
Background
Injuries are significant public health concern, contributing to substantial morbidity and mortality among adults worldwide. In Ghana, limited studies have examined injuries among adults, with existing studies predominantly focusing on a single injury mechanism within a single health facility setting.
Objective
This study aimed to describe the distrubution of hospital based reported injuries among adults in Ghana and to identify associations of injury-related mortality.
Methods
A cross-sectional study was conducted using data from four regional teaching hospitals in Ghana between January 2017 and December 2020. Descriptive statistics were used to summarize demographic characteristics, injury mechanisms and outcomes. Least Absolute Shrinkage and Selection Operator (LASSO) regression was used for variable selection, followed by survey-weighted logistic regression to estimate factors associated with mortality, accounting for facility-level effects and population structure using R statistical software.
Results
A total of 6,662 adult injury cases were included (mean age 41 ± 18 years), of which 4,702/6,662 (70.6%) were males. Road traffic injuries (4,371/6,662; 66%) and falls (1,909/6,662; 29%) were the leading injury mechanisms. The overall in-hospital mortality rate was 113/6,662 (1.7%). In multivariable analysis, educational attainment was a significant protective factor: junior high school (adjusted OR: 0.24; 95% CI: 0.13–0.45), senior high school (adjusted OR: 0.45; 95% CI: 0.23–0.85), and tertiary education (adjusted OR: 0.23; 95% CI: 0.12–0.45), compared to no formal education. Urban residence (3,814/6,662; 57.3%) was associated with lower odds of mortality (adjusted OR: 0.57; 95% CI: 0.33–0.98) relative to peri-urban areas (970/6,662; 14.6%). Age, sex, injury mechanism, and weekend occurrence were not significantly associated with mortality after adjustment.
Conclusion
Injuries among adults in Ghana are predominantly due to road traffic incidents and falls, with relatively low in-hospital mortality. Mortality is more strongly associated with socioeconomic and geographic factors than with injury mechanism or demographic characteristics. Strengthening trauma health systems, addressing social determinants such as education, and improving road safety measures in high-risk environments is recommended.
Background
Injuries encompass a spectrum of incidents including accidents, falls, burns, and poisonings, among others.1–3 These events represent a substantial global public health challenge, contributing to significant rates of morbidity and mortality among adults across all age groups.1,3,4 The World Health Organization (WHO) reports that approximately 3.9 million lives are lost annually due to unintentional injuries, with countless more individuals experiencing non-fatal injuries that can result in long-term disability, functional impairment, or compromised quality of life.1,5 The burden of injuries is disproportionately concentrated in low- and middle-income countries (LMICs), where 90% of injury-related deaths occur, reflecting disparities in infrastructure, healthcare access, and preventive resources.1–3 Shared structural determinants such as informal housing, the proliferation of commercial motorcycle use, and inadequate pedestrian infrastructure shape injury profiles Sub-Saharan Africa. 3 Additionally, household energy transition and alcohol environments intersecting with weekend travel behaviors also influence burn and road traffic injuries (RTIs) patterns to exacerbate mortality.
In Ghana, specifically, the epidemiological landscape is defined by a high prevalence of road traffic injuries (RTIs) and falls. 2 Ghana faces complex challenges in addressing injuries, particularly amid rapid urbanization and transport system transitions.4,6 The epidemiology of injuries is influenced by structural determinants, including the proliferation of motorcycle use in peri-urban corridors and disparities in healthcare access. In Ghana, it further varies across factors such as age, gender, geographic location, educational attainment, and socioeconomic status.7–9 The consequences of these injuries extend far beyond immediate physical trauma, encompassing long-term physical disabilities, psychological distress, social stigma, and substantial financial hardship for affected individuals and their families.5,7,10 Moreover, the productive capacity of adults in their prime working years can be severely compromised, with cascading effects on household income, family wellbeing, and ultimately, national economic development. 11 The healthcare system also bears a considerable burden from unintentional injuries, with substantial costs associated with emergency care, hospitalization, surgical interventions, rehabilitation services, and long-term disability management.7,12
Despite the recognized importance of this public health issue, research on unintentional injuries in Ghana has been limited in scope and methodology. Existing studies have predominantly focused on road traffic crashes as a single injury mechanism,7–9 with most investigations conducted within single-facility settings. 13 This narrow focus has left significant gaps in understanding the full spectrum of unintentional injuries, their distribution across different demographic groups, comparative mortality risks across injury types, and the complex interplay of factors that influence injury outcomes. Furthermore, single-facility studies may not capture the geographic and demographic diversity of the adult population in Ghana, potentially limiting the generalizability of findings and the development of evidence-based prevention strategies. This study aims to address the gap by providing a broader analysis on the distribution and mortality risk of unintentional injuries among Ghanaian adults using multi-facility data. This is essential for informing targeted prevention programs, optimizing trauma care systems, allocating healthcare resources effectively, and ultimately improving outcomes for affected adults.
Materials and methods
Study design
This study employed a cross-sectional research design using retrospective data. The cross-sectional approach allowed for the examination of injury patterns and outcomes at a single point in time.
Study sites
The study was conducted in four purposively selected regional teaching hospitals in Ghana: Korle-Bu Teaching Hospital (Greater Accra Region), Komfo Anokye Teaching Hospital (Ashanti Region), Tamale Teaching Hospital (Northern Region), and Cape Coast Teaching Hospital (Central Region). These hospitals were selected based on several criteria: (1) their status as tertiary healthcare institutions serving as referral centers for their respective regions, (2) their trauma care facilities, (3) their established electronic medical record systems, and (4) their geographic distribution across different regions of Ghana, ensuring representation of diverse population characteristics.
Study population
The study population comprised of records of adults of 18 years and above who had sought medical care for unintentional injuries at the selected regional teaching hospitals between January 2017 and December 2020. Unintentional injuries were defined as injuries resulting from incidents occurring without deliberate intent to harm, including road traffic crashes, falls, burns, blunt trauma, and sports-related injuries.
Sampling techniques
A census sampling approach was employed, whereby all eligible cases meeting the inclusion criteria during the study period were included in the analysis.
Data collection tools and procedures
Data were extracted from the electronic medical record systems of the participating hospitals. Each hospital maintains a database of patient information, including trauma cases. Key variables extracted for this study included demographic data, injury characteristics, clinical presentation details, and outcome measures. Data quality was ensured through regular training of hospital staff on electronic medical record data entry, periodic data quality audits conducted by hospital data management teams and cross-checking of extracted data against physical records when necessary.
Definition of injury mechanisms
Injury mechanisms were classified based on electronic medical record entries using standard definitions. Road Traffic Injuries include all motorized and non-motorized collisions; Falls involve unintentional descent to a lower level; Burns encompass thermal, chemical, or electrical injuries; Blunt Trauma refers to direct impacts such as struck by objects or machinery not classified as road crashes or falls; and Sports Injuries involve organized or recreational activities. 14 Assault cases were retained as a baseline reference category for mortality risk comparison.
Data management and analysis methods
Data from all four facilities were merged into a single database, cleaned, and coded using standardized procedures. All analyses were performed using R statistical software (version 4.4.1). 15 The data management process included checking for duplicate records, identifying and handling missing data, validating data ranges and logical consistency, and creating derived variables for analysis. Descriptive statistics were computed to summarize the characteristics of the study population. Continuous variables were reported as means with standard deviations (SD), while categorical variables were presented as frequencies and percentages with 95% confidence intervals where appropriate. Chi-square tests were used to assess associations between injury mechanisms and demographic characteristics (age group, sex, settlement type) as well as temporal factors (day of week).
For the multivariable analysis, a two-stage approach was employed. First, Least Absolute Shrinkage and Selection Operator (LASSO) regression was performed using the “glmnet” package 16 to identify the most important associations of post-injury mortality from the pool of candidate variables (age, ,injury mechanism, facility, Sex, Settlement, Day Category, Educational level, year of report, time spent before reporting to the health facility). LASSO regression is particularly useful for variable selection in the presence of multiple associations, as it applies a penalty that shrinks less important variable coefficients toward zero. The optimal tuning parameter (lambda = 0.0014) was selected through 10-fold cross-validation using the minimum cross-validation error criterion. Subsequently, survey-weighted logistic regression (a “svyglm” function) analysis 17 was performed incorporating all variables identified by Least Absolute Shrinkage and Selection Operator (LASSO) regression as significant associations. To account for potential intra-cluster correlation and facility-level differences, the analysis utilized a Taylor-series linearization variance estimator. This approach accounted for the clustering of patients within facilities. Assault, an intentional injury, was used as the baseline for comparison.
To enhance the generalizability of findings to the broader Ghanaian adult population, survey weights based on the 2021 Ghana Population and Housing Census data 18 were applied. These weights adjusted the sample distribution to match the national age and sex distribution, thereby accounting for potential selection bias arising from the hospital-based sampling approach. Both unadjusted odds ratios (OR) and adjusted odds ratios (aOR) with 95% confidence intervals (CI) were calculated to quantify the associations between independent variables and mortality outcomes. Statistical significance was set at p < 0.05 for all analyses.
Ethical considerations
The Committee on Human Research Publications and Ethics (CHRPE) at Kwame Nkrumah University of Science and Technology granted ethical clearance for this study, under the reference number CHRPE/AP/290/19. Institutional management boards from each participating hospital in Ghana, including Korle-Bu Teaching Hospital, Komfo Anokye Teaching Hospital, Tamale Teaching Hospital, and Cape Coast Teaching Hospital, provided permissions prior to this approval.
Results
Demographic characteristics
Demographic and clinical characteristics of study participants.

Injury mechanisms
Prevalence of unintentional injuries by mechanism and temporal factors.

Distribution by demographic characteristics
The distribution of injury mechanisms differed significantly across demographic groups. Age group was strongly associated with injury mechanism (χ2 = 999.83, df = 20, p < 0.001). Falls were more prevalent among elderly individuals (above 64 years), accounting for 67.3% of injuries in this age group, while road traffic injuries predominated in younger age groups, representing 75.1% of injuries among young adults (18-25 years), 75.5% among adults (26-35 years), and 73.0% among middle-aged adults (36-45 years) (Figure 1). Burns and sports injuries showed relatively higher proportions (4.7%) in the young adult age group (18-25 years) compared to other age categories. Age – group and day category distribution of injuries.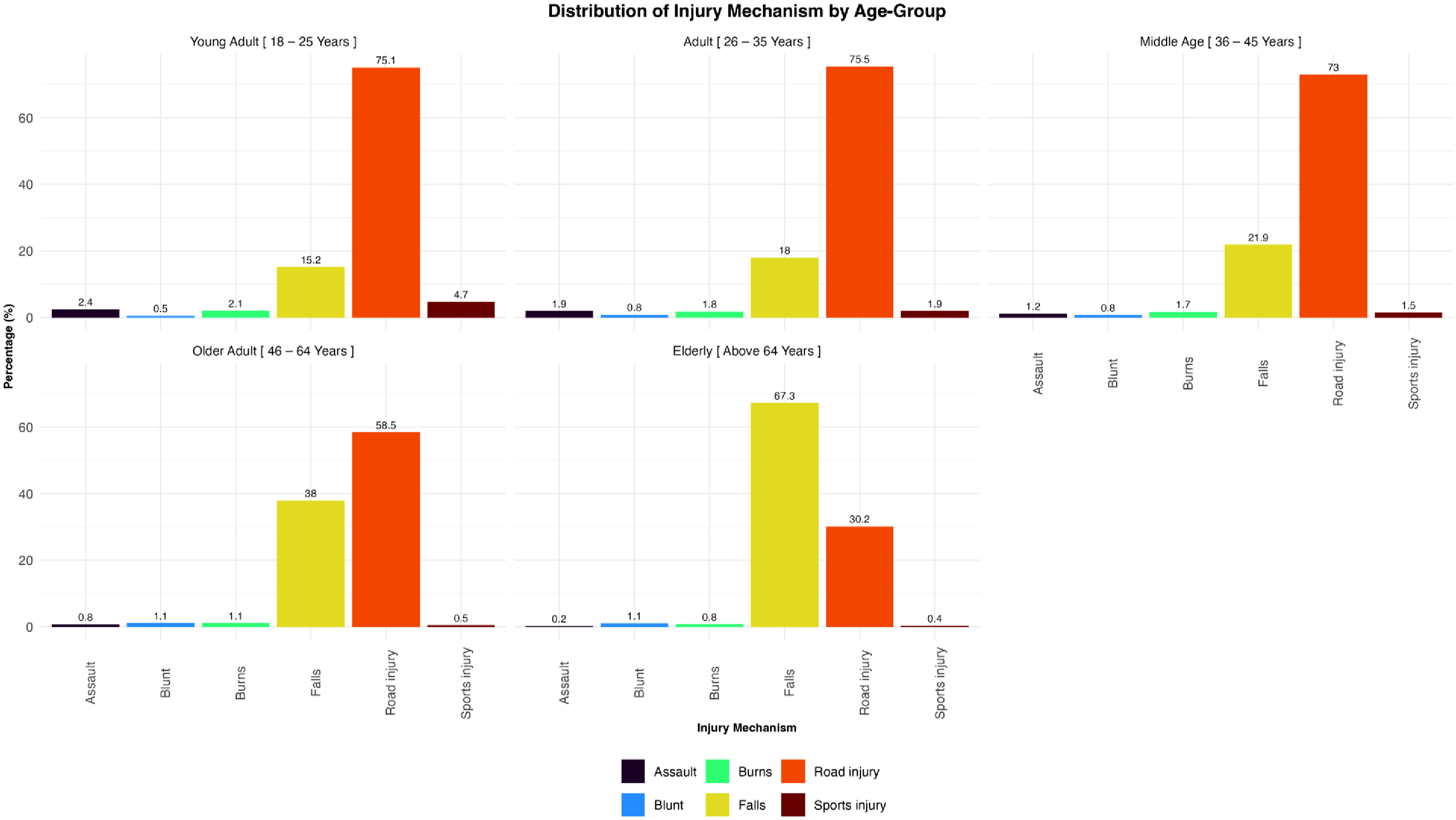
Sex was also significantly associated with injury mechanism (χ2 = 341.6, df = 5, p < 0.001). All injury mechanisms showed higher frequencies among males compared to females, consistent with the overall male predominance in the sample. However, when examining proportions within sex-specific groups, falls were more predominant among elderly females (77.5%) compared to elderly males (54.9%) (Figure 2). Road traffic injuries comprised a higher proportion of injuries among males (42.2 to 77.6%) compared to females (20.3 to 76.0%) across all age groups. Age – group and sex distribution of injuries.
Distribution by settlement type
The distribution of injury mechanisms by settlement type showed some variation, although the chi-square test did not indicate a statistically significant association (χ2 = 16.55, df = 10, p = 0.08). Road traffic injuries comprised 28 to 74.8% of urban injuries, 33.9 to 79.0% of rural injuries, and 32.5 to 77.3% of peri-urban injuries. Falls represented as high as 70.0% of urban injuries, 63.4% of rural injuries, and 63.2% of peri-urban injuries, showing relatively consistent proportions across settlement types (Figure 3). Age – group and settlement distribution of injuries.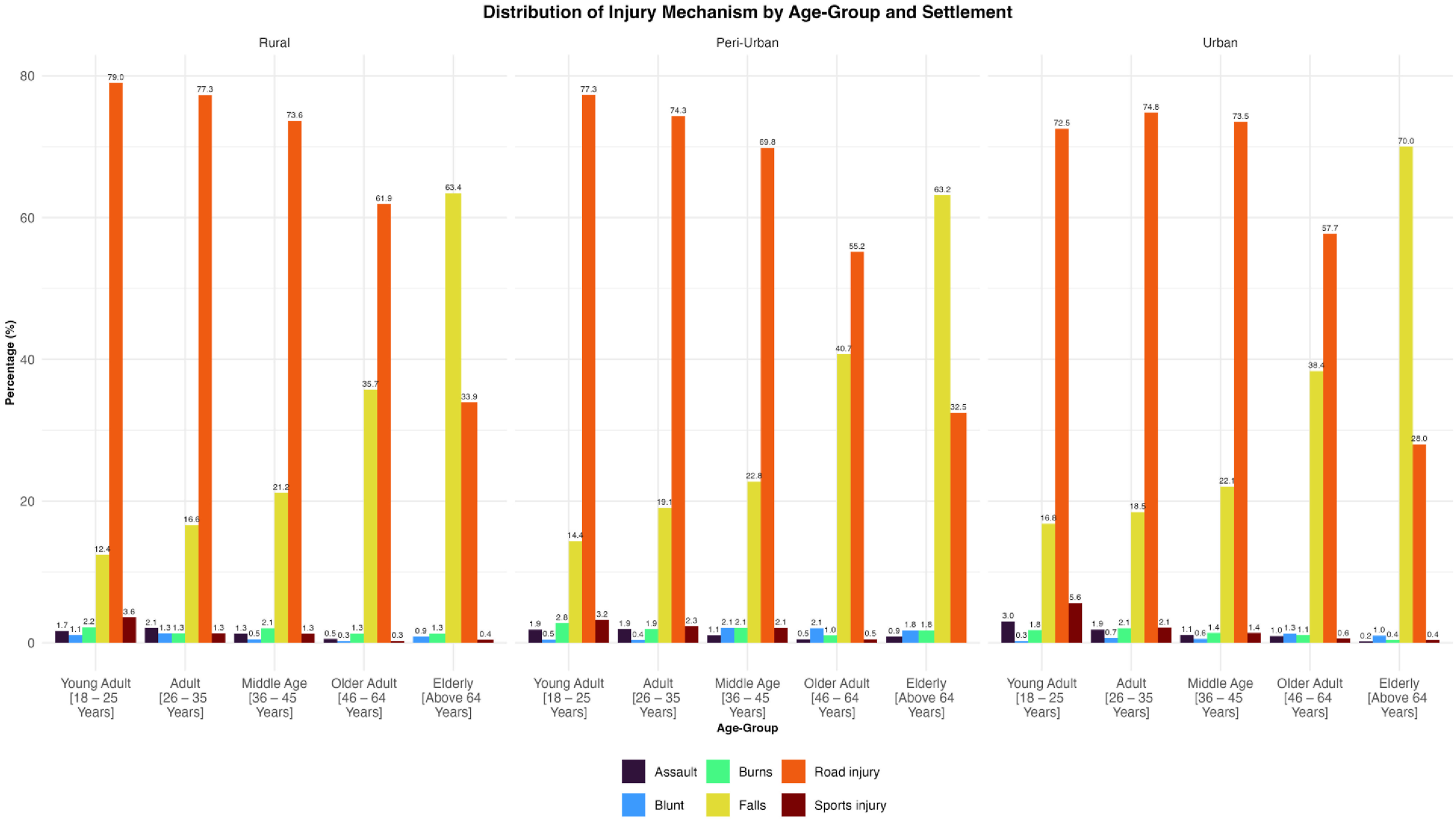
Injury mechanism by mortality and COVID season
Distribution of injury mechanism by mortality and COVID season (2017–2020).

Factors associated with mortality following injury
Risk of mortality after injury.

Discussion
This study provides a multi-facility hospital-based surveillance insights into the epidemiology of injuries among adults in Ghana, revealing important patterns in injury mechanisms, demographic distributions, and mortality association factors.1,4 The findings highlight a substantial burden of injury, with a clear predominance among males and adults aged 26-35 years, and an overall in-hospital mortality of 1.7%. The findings, excluding deaths occurring before hospital arrival and minor injuries that never presented to the helath facility for care, underscore the substantial public health burden of unintentional injuries and highlight critical areas for targeted intervention.
Road traffic injuries emerged as the leading cause, accounting for two-thirds of all reported injuries and 1.4% mortality. This was more common among males and those aged below 65 years compared to females and the elderly respectively. This finding is consistent with the high burden of road traffic injuries reported in Ghana and other low- and middle-income settings, where rapid urbanization, increasing motorization, and limited enforcement of road safety regulations contribute to a high burden of road traffic injuries.7,11 The strong age gradient observed where road traffic injuries predominated among younger adults 13 while falls were concentrated among the elderly reflects differing exposure patterns and vulnerability across the life course.19,20 This is consistent with findings from other low- and middle-income countries. 21 This further reflects the reduced physiological reserve and higher frailty in older populations,4,7 even though the study may have been underpowered to detect a definitive effect. Similarly, while males accounted for the majority of injuries, their mortality risk did not differ significantly from females after adjustment, indicating that exposure rather than case fatality may explain observed sex differences.4,7 In the environmental scope, the level of rainfall and temperature also influence road traffic crashes 22 and injuries 23 in Ghana. Additionally, injuries and its associated mortality are heat related.24,25
The multivariable analysis also showed no statistically significant differences in mortality risk across injury mechanisms, with wide confidence intervals suggesting sparse data and limited precision for less common injury categories. This finding contrasts with some prior studies and suggests that, within this study, factors beyond injury type such as access to care, injury severity, or pre-hospital delays may play a more critical role in determining survival outcomes.
Furthermore, educational level emerged as a significant factor, with individuals with junior high, senior high, and tertiary education had substantially lower odds of mortality compared to those with no formal education. This findings reflects differences in health literacy, socioeconomic status, risk awareness, and healthcare-seeking behavior, reinforcing the broader role of social determinants in injury outcomes. 26
Settlement type also demonstrated an important association with mortality. Urban residents had significantly lower odds of death compared to peri-urban residents. Urbans have controlled traffic matched by pedestrian safety measures and closer to referral centers for early intervention. 23 Unlike established urban centers, peri-urban zones in Ghana often serve as ribbon developments along high-speed trunk roads. 23 The elevated risk in peri-urban areas may reflect a convergence of risk factors, including high-speed road networks, inadequate pedestrian infrastructure, and limited access to timely emergency care. 2 These transitional environments often lack the structured safety systems of urban centers while experiencing higher traffic volumes than rural areas, increasing exposure to severe injuries.
Temporal factors showed limited influence on mortality. Although injury mechanisms differed significantly across the pre-COVID and COVID periods possibly due to the lockdown measures, these shifts did not translate into measurable differences in mortality risk after adjustment. Similarly, weekend injuries were not associated with increased mortality, suggesting that behavioral risks such as increased nighttime travel and alcohol use during funeral activities on the weekends8,9,13 may influence injury occurrence more than survival outcomes, particularly for motorcyclists who may lack proper protective gear. 27
Strengths and limitation
This study has several notable strengths. The multi-facility design across four regional teaching hospitals enhances generalizability compared to previous single-facility studies. The large sample size (n = 6,662) provides adequate statistical power to detect meaningful associations and examine subgroup patterns. The application of population-based weights adjusts for sampling bias and improves external validity. However, some limitations warrant consideration. First, the cross-sectional design precludes causal inference. Second, the hospital-based sampling may introduce selection bias, as the most severely injured patients who die before reaching the hospital or those with minor injuries who do not seek hospital care are not represented. This likely results in underestimation of the true burden of injury mortality and morbidity. Third, the study lacked detailed information on injury severity scores, pre-hospital care, specific treatment interventions, road user type classification and post-discharge outcomes. These variables could provide additional insights into mortality determinants and opportunities for intervention.
Future research directions
Future research should include prospective cohort studies with detailed injury severity scoring and longitudinal follow-up would provide deeper insights into recovery trajectories and long-term outcomes. Community-based studies are needed to capture the full spectrum of injuries, including those not presenting to hospitals. Investigation of pre-hospital care systems, emergency response times, and their impact on outcomes would inform system-level improvements. Studies examining facility-level factors (staffing patterns, resource availability, treatment protocols) and their influence on outcomes would support quality improvement initiatives. Finally, implementation research on injury prevention strategies tailored to the Ghanaian context is needed to translate epidemiological findings into effective action.
Conclusion
In this multi-facility study, injury-related mortality was associated with socioeconomic and geographic factors, with higher education and resisdents of urban areas showing a protective effect. These findings underscore the need for targeted prevention strategies and strengthened trauma care systems. Efforts should focus on improving road safety through enhanced infrastructure, law enforcement, and public education.
Footnotes
Ethical considerations
Ethical approval was obtained from the Committee on Human Research Publications and Ethics (CHRPE), of Kwame Nkrumah University of Science and Technology with reference number: CHRPE/AP/290/19. Prior to approval, permission was sought from institutional management boards of each of the participating hospitals in Ghana namely Korle-Bu Teaching Hospital, Komfo Anokye Teaching Hospital, Tamale Teaching Hospital and Cape Coast Teaching Hospital. Participants’ privacy and confidentiality were rigorously maintained throughout the study.
Author contributions
Conceptualization, J.S.I and E.N.; Methodology, E.N. and J.S.I.; Validation, J.S.I., J.S.S. and S.M.; Formal Analysis, J.S.I.; Data Curation, J.S.I., J.S.S. and S.M.; Writing – Original Draft Preparation, J.S.I.; Writing – Review & Editing, E.N, J.S.S. and S.M.; Visualization, J.S.I.; Supervision, E.N.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are available through the corresponding author on reasonable request. However, sample data may be shared for verification of results.