
Abstract
Introduction
Keloid and hypertrophic scars are products of abnormal wound healing and can cause disfigurement, discomfort, and decreased quality of life. The precise mechanisms of how these scars form remain unclear, and despite several management strategies, there is currently no definitive management approach that prevents recurrence of keloid scars. Hyaluronan (HA) is a polysaccharide with critical functions in inflammation, fibrosis, and skin health. This narrative review explores what is currently known about the role of HA and associated proteins in keloid and hypertrophic scar pathogenesis and management.
Methods
The online MEDLINE and EMBASE databases were searched for articles on keloid and hypertrophic scarring and HA from 1946 to 2026. English-language, peer-reviewed articles with empirical evidence examining human keloid scar tissue, animal models, cell-culture models, hyaluronic acid, or hyaluronome-associated genes were included. Twenty-one studies met all inclusion criteria.
Results
HA concentration was diminished in cell-based models of keloid and hypertrophic scars relative to normal skin. Observed aberrant localization of HA was likely related to the altered expression of genes encoding proteins responsible for the synthesis, degradation, binding, and signaling properties of HA. Intralesional and topical applications of HA both improve appearance and reduce recurrence rates of keloid scars in the short term.
Conclusion
Our review suggests that altered HA production, metabolism, and localization play a key role in keloid and hypertrophic scar pathogenesis. While early evidence supports the potential utility of HA in keloid scar treatment, further robust clinical validation is necessary.
Introduction
Keloid and hypertrophic scars are formed as a consequence of an abnormal response to wound healing.1,2 They are benign lesions that can cause significant symptomatic and cosmetic discomfort for patients.3,4 Keloids can form months, if not years, after an initial injury and extend beyond the site of the original wound. 2 Keloids frequently present in areas of increased skin tension, such as the back and trunk, but also form at other anatomic sites, including the ears.5–9 Most keloids are thought to have a genetic basis and are more commonly seen in patients with darker skin.3,4,10,11 Keloids are difficult to treat and have a high rate of recurrence, ranging from 45% to 100%. 7 Current treatment options for these scars include surgical removal, steroid injections, and radiation and laser therapy. 5 Steroid injections are often the first line of treatment, but have a variable response rate with 50% recurrence within 5 years posttreatment.5,6
Hypertrophic scars typically form weeks to months after an initial injury and remain confined to the original wound boundaries.8,12 Like keloids, hypertrophic scars tend to present in areas of increased skin tension. 8 Unlike keloids, they may spontaneously regress over time and have a relatively lower rate of recurrence post excision. 8 Current treatment options include silicone sheeting and gels, intralesional corticosteroid injection, pressure therapy, and excision.8,13,14
In a normal response to injury, wound healing occurs in 3 primary stages: inflammation, proliferation, and remodeling.15,16 In the inflammatory phase, granulation tissue is formed, with increased production of specific components of the extracellular matrix (ECM),17,18 including collagen and elastin, as well as proteoglycans and glycosaminoglycans such as hyaluronan (HA). 9 Granulation tissue is remodeled with the replacement of type 3 collagen by type 1 collagen. 9 Type 1 collagen is then organized into bundles to form a mature scar. 2 While the pathogenesis of keloid and hypertrophic scars has not been fully characterized; they are thought to form because of a breakdown in this temporal sequence of wound healing.
A key component of the ECM, particularly in skin, is the glycosaminoglycan HA. HA is a polysaccharide that regulates inflammation and fibrosis, thus influencing wound repair. HA production, metabolism, and degradation are regulated by a network of gene products collectively referred to as the hyaluronome (Figure 1). 19 HA production is rapidly increased as an initial response to injury, and in part acts to trap fibrinogen, allowing formation of a clot that provides a suitable microenvironment for attracting and capturing inflammatory cells at the site of injury.20–22 HA, which is initially produced as a high-molecular weight, anti-inflammatory polymer (HMW-HA), rapidly degrades during tissue injury into proinflammatory fragments required for wound repair.23,24 Degradation results from reactive oxygen/nitrogen species and hyaluronidase activity that are collectively elevated during a response to injury. 25
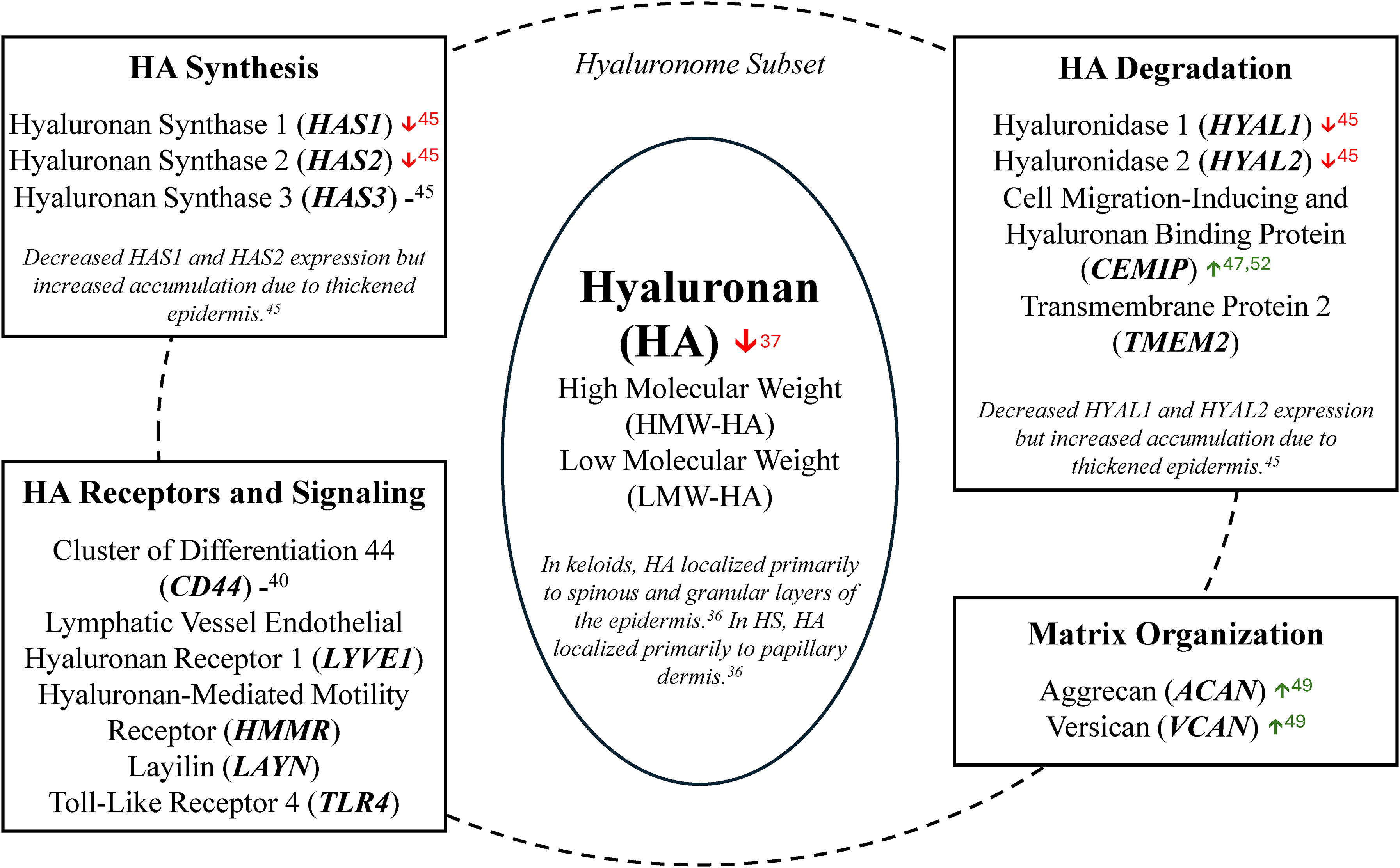
Key components of the hyaluronome relevant in cutaneous wound repair and fibrosis. The hyaluronome is a coordinated gene network governing hyaluronan (HA) synthesis, degradation, receptor-mediated signaling, and extracellular matrix organization. This schematic illustrates a subset of each functional domain and corresponding regulation patterns in keloids. Red (↓) and green (↑) arrows and horizontal dash (-) represent downregulation, upregulation, and no significant change in expression, respectively. Numbers correspond to references in the main reference list.
Recent studies suggest that replenishing HMW-HA improves the appearance of keloids.26,27 However, the underlying mechanisms for these observed benefits are poorly understood. This narrative review aims to explore what is currently known about the role of HA and the hyaluronome in keloid and hypertrophic scar pathogenesis and treatment to begin to fill this knowledge gap.
Methods
Given the heterogeneity of available literature, spanning basic science, translational, and clinical studies, a systematic review methodology was not implemented. Rather, a narrative review format was applied to provide a structured synthesis of the role of HA and associated gene products, the hyaluronome, in the pathogenesis and management of keloid and hypertrophic scars. This approach allows integration of mechanistic and clinical insights and contextualization of the hyaluronome, not readily achievable through a systematic review.
The online MEDLINE and EMBASE databases were searched for articles on the topic of keloid scarring and HA. MEDLINE and EMBASE were selected due to their thorough and complementary coverage of biomedical, translational, and experimental research. Together, they contain most of the literature pertaining to scarring and HA biology; and additional databases were excluded due to substantial overlap and thus incremental yield.
The MEDLINE database was originally searched from 1946 onward through to May 10, 2022. The EMBASE database was also originally searched from 1947 onward through to May 10, 2022. An updated search, conducted in March 2026, was expanded to include hypertrophic scars, burns, and other clinical contexts to identify data on HA application in scar treatment at large. The search strategies that were used can be found in the Supplemental material. English-language, peer-reviewed articles with empirical evidence that examined human scar tissue, animal models of scars, cells cultured from scar tissue, HA (in any formulation alone or in conjunction with other therapeutic modalities), or hyaluronome-associated genes (CD44, CEMIP, HAS1, HAS2, HAS3, HMMR, HYAL1, HYAL2, LAYN, LYVE1, TLR4, TNFAIP6, VCAN, TMEM2) were included. Review articles, meta-analyses, and gray literature, including conference abstracts, editorials, consensus statements, practice guidelines, working papers, policy statements, and dissertations were excluded. Additional sources were referenced through a manual search of the cited references in the identified studies.
Scope of Reviewed Literature
The original search identified 475 studies, of which 107 were duplicates. Of the 368 unique abstracts, 44 studies met the inclusion criteria, as outlined in the Methods, for full-text review. An additional 28 studies were excluded at the full-text review stage. Ultimately, 16 studies met all inclusion criteria and are included in this review (Table 1). In March 2026, the expanded search identified 1892 unique abstracts, of which 884 duplicates were identified and excluded. Of the 1008 screened studies, 5 were ultimately included in this review (Table 1). Rationale for studies excluded across both screening rounds is provided in Figure 2. The included studies were published between 1976 and 2024 from 9 different countries, including the United States (n = 6), China (n = 5), Japan (n = 3), and the United Kingdom (n = 2). Single papers originated from Korea, Sweden, the Netherlands, Thailand, and Turkey. The studies included in this review derived their scar and normal skin (NS) samples from frozen cell stock as well as excised keloid and hypertrophic scar tissue from patients. The average patient age, duration of keloid, and patient ethnicity were variable across these studies (Table 2).
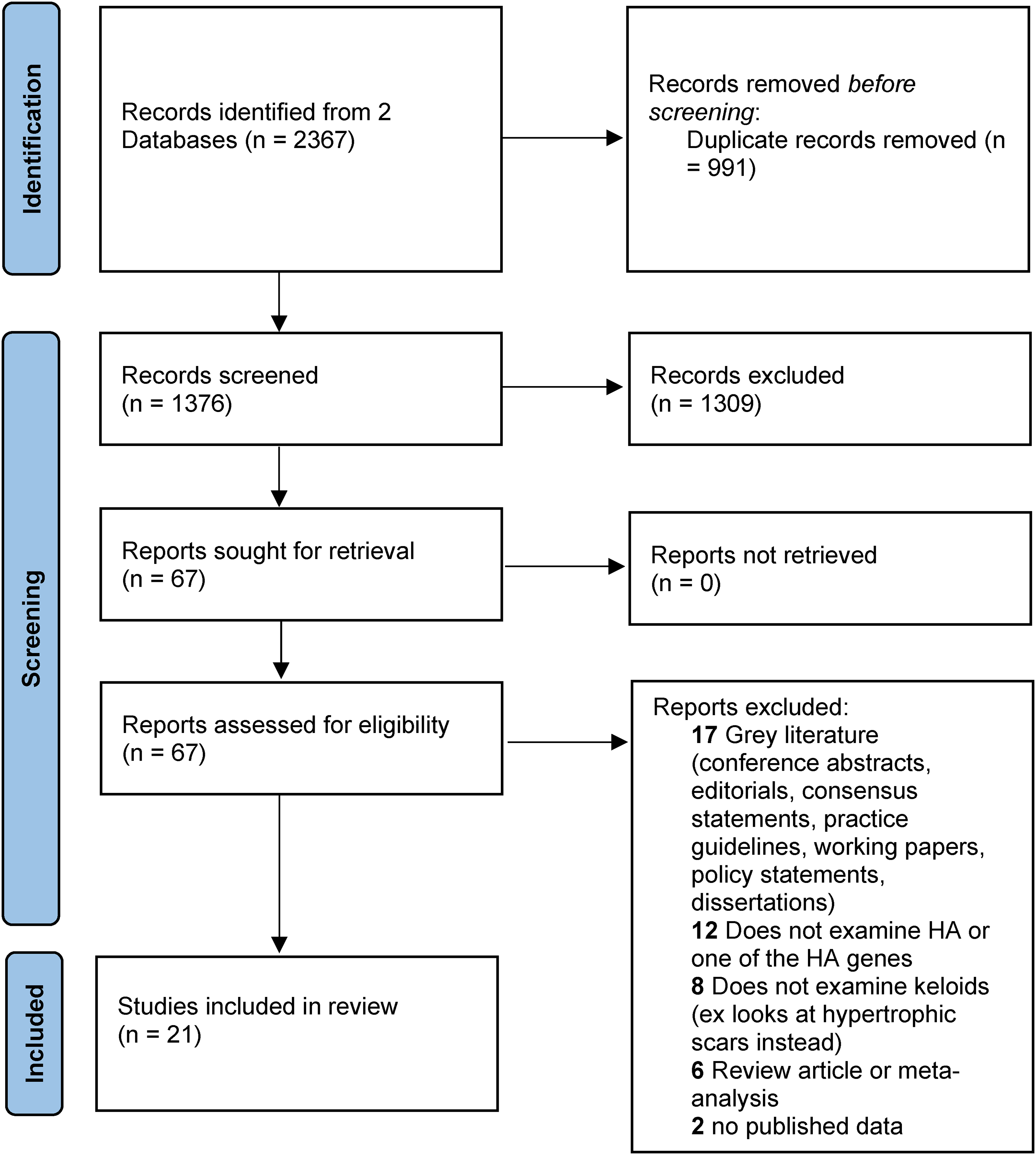
PRISMA flow diagram of study selection. Flow diagram illustrating the process through which the number of studies initially identified through the database search was filtered to the final number of the included studies. Studies were retrieved from MEDLINE and EMBASE, and duplicates were removed using Covidence. Titles and abstracts were screened, followed by a full-text review based on the described inclusion criteria.
Overview of Studies Included in this Review.
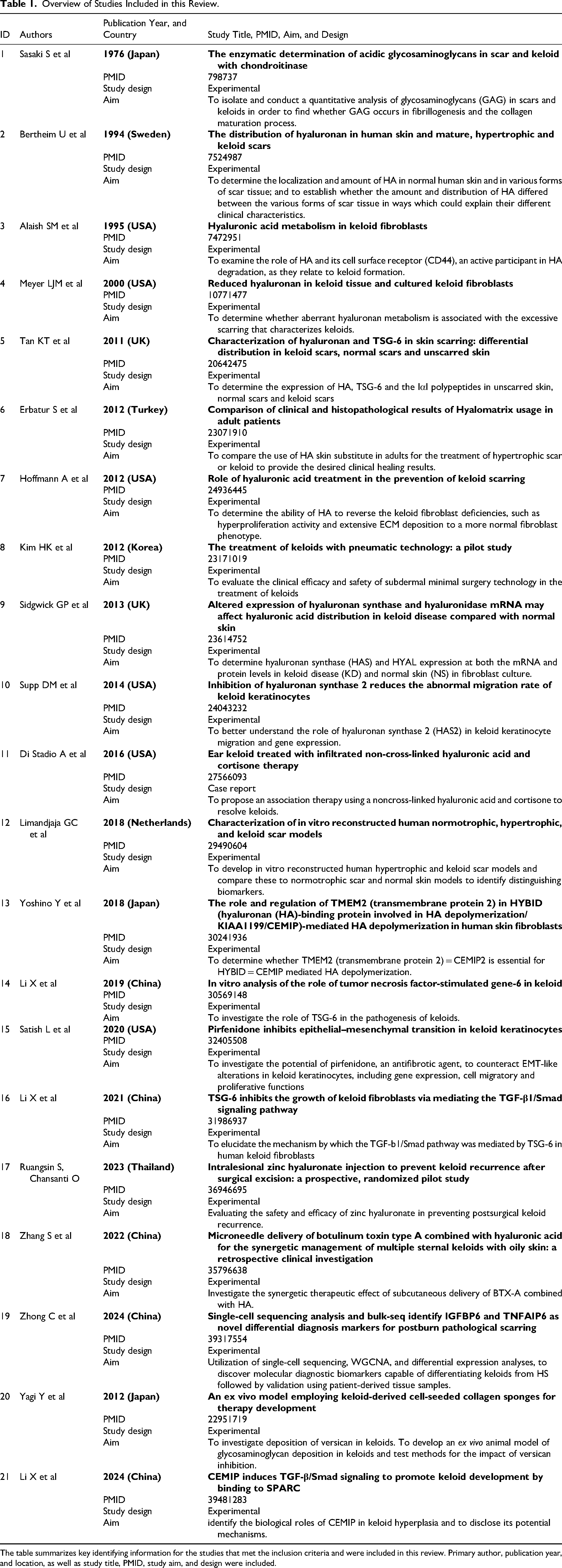
The table summarizes key identifying information for the studies that met the inclusion criteria and were included in this review. Primary author, publication year, and location, as well as study title, PMID, study aim, and design were included.
Characteristics of Keloid Tissue Samples.
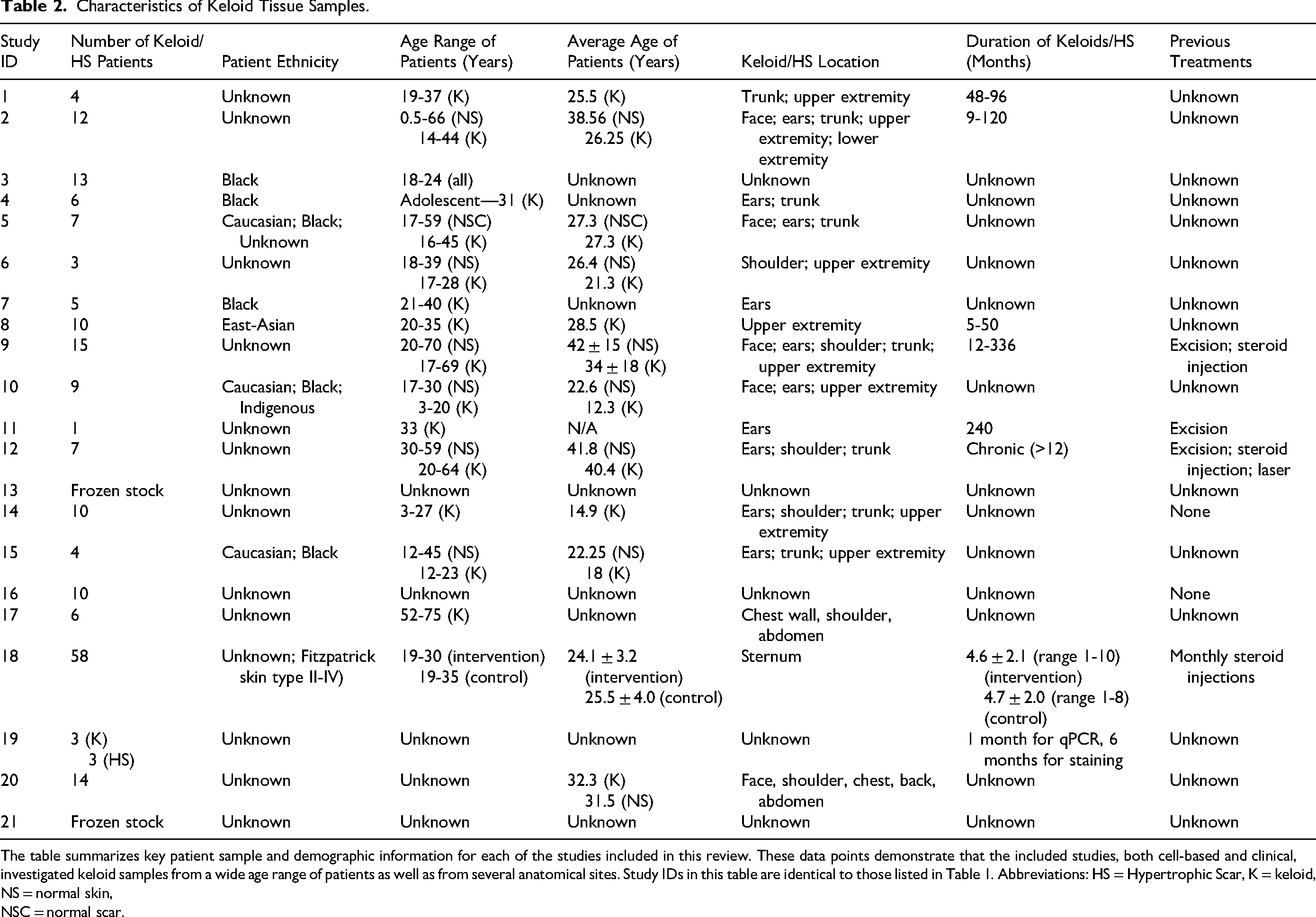
The table summarizes key patient sample and demographic information for each of the studies included in this review. These data points demonstrate that the included studies, both cell-based and clinical, investigated keloid samples from a wide age range of patients as well as from several anatomical sites. Study IDs in this table are identical to those listed in Table 1. Abbreviations: HS = Hypertrophic Scar, K = keloid, NS = normal skin, NSC = normal scar.
Review of Clinical Evidence for Therapeutic HA Administration
Several studies have reported the therapeutic potential of HA in treating keloid scars. Subdermal minimal surgery, wherein a pneumatically accelerated jet of HA penetrates the epidermis and extends laterally along the dermis, was utilized in a pilot study with 10 patients. 26 HMW-HA was administered to all patients’ upper arm keloid scars in this manner 3 times at 3-week intervals. 26 The study showed significant improvement in 3 month posttreatment Vancouver Scar Scale (VSS) scores compared to pretreatment, with average scores of 5.8 and 8.8 (P < .001), respectively, as well as subjective physician-reported improvements in scar appearance. 26 While this study only included 10 participants, limiting generalizability, similar levels of clinical improvement were reported in a case report of a 33-year-old patient who underwent concurrent treatment with cortisone and HMW-HA, 20 years following the onset of a keloid scar on his left ear. 27 Over 60 days, the keloid scar was treated with alternating infiltrations of cortisone and Restylane Vital (HA), with 4 and 3 treatments total, respectively. 27 Subsequently, the scar underwent another round of alternating treatments, comprised of 3 cortisone and 2 Restylane Vital infiltrations. 27 The keloid was completely resorbed at 15 days following the second round of treatment and had not recurred in the following 12 months, which was the end of the study period. 27
Intralesional injection was also the treatment modality used in another study investigating botulinum toxin type A (BTX-A) and hyaluronic acid as combined therapy for sternal keloids in 58 patients with oily skin. 28 The 26 patients in the control group received intralesional steroid injections every 4 weeks for 24 weeks, while the 32 patients in the intervention group received both the steroid treatment as well as subcutaneous microneedle delivery of BTX-A combined with HA (BioHyalux®) on the same day every 4 weeks for 24 weeks. 28 At 24 weeks, patients in the intervention group noted higher satisfaction, significant improvements in pain and itching per visual analog scale scores, and significant improvements on the VSS, with total scores of 11.04 ± 0.14 and 8.93 ± 0.26 (P < .001) in the control group and intervention group, respectively. 28 Sternal keloid relapse was noted in 88.5% of patients in the control group, and no patients in the intervention group. 28 While the absence of keloid recurrence in the treatment group is promising, the lack of long-term follow-up and limited scar anatomic location variation restricts generalizability.
Longer-term follow-up was implemented in a prospective double-blinded randomized controlled trial evaluating zinc hyaluronate (ZH) in preventing postsurgical keloid recurrence. 29 A single dose of intralesional ZH or placebo gel was applied following keloid excision, prior to primary closure, in 4 and 2 patients, respectively. 29 Patients received no further keloid treatments and were followed postoperatively for 5 years. 29 Recurrence was diagnosed in year 3 for all patients in the placebo group and 3 of 4 patients in the intervention group. 29 Studies discussed thus far employed either intralesional HA injection or topical application. One study looked at the application of Hyalomatrix PA membrane following surgical excision of hypertrophic/keloid scars in 10 patients for 4 weeks. 30 Another 10 patients were treated with 4 consecutive weekly HA injections into hypertrophic/keloid scars without excision. 30 The scars did not recur over the next 12 months in the Hyalomatrix PA membrane group, and the amount of vascularization and collagenization in the region also decreased. 30
When considering evidence for using HA in treating hypertrophic scars, current studies employ HA as a component of drug delivery systems rather than as a standalone treatment. Specifically, HA-based microneedle platforms have been used to deliver protocatechuic aldehyde, salvianolic acid B, 5-fluorouracil, and asiaticoside into hypertrophic scar tissue animal models.31–33 These studies suggest a role for HA in facilitating targeted therapies, and demonstrate improved drug penetration, reduced scar elevation index 32 and downregulation of fibrotic markers like collagen I and transforming growth factor-β1 expression.31,32
Taken together, despite promising early findings, the current body of clinical evidence remains limited. The reviewed studies are constrained by small sample sizes, heterogeneous scar anatomical locations, variable HA formulations, and short follow-up durations. Nevertheless, these studies suggest that when HMW-HA is introduced into keloid tissue, the size of the scar decreases, the appearance improves, and postexcision recurrence rates decrease in the short term.26,27,30 These clinical findings are underpinned by in vitro results demonstrating that HA plays a prominent role in keloid and hypertrophic scar pathogenesis.
Altered Production of HA in Keloid and Hypertrophic Scars
Several cell-based studies demonstrated that production of HA was disturbed in keloid and hypertrophic scar tissue.30,34–39 Alaish et al used radiolabeled precursor assays that showed HA synthesis was higher in cultured keloid fibroblasts than in normal comparators. 40 Alaish et al used Alcian blue dye to stain for HA, which is a nonspecific measure of HA in tissues.40,41 A newer study by Meyer et al, which used biotinylated HA binding protein that specifically detects HA, demonstrated decreased HA staining intensity in histological analyses of keloids compared to normal scar, and further reduction when compared to NS. 37 Additional studies echo this reduction in HA in keloid-derived fibroblasts (KDFs) compared to normal scars and normal scar fibroblasts.36,38,42
HA synthesis is driven by the HA synthase family of genes, namely HAS1, HAS2, and HAS3. Limandjaja et al found that HAS1 mRNA expression was decreased in the dermis of cocultured 3-D keloid and hypertrophic scar models constructed of KDFs, keloid-derived keratinocytes (KDKs), and hypertrophic scar-derived fibroblasts and keratinocytes. 43 However, Supp et al reported no significant difference in HAS1 mRNA expression in KDKs, using a 2-D monolayer culture model. 44 These discrepancies may reflect confounding factors relevant to culture systems, as 3-D cocultures better replicate fibroblast–keratinocyte interactions, ECM signaling, and intercellular spatial architecture absent in 2-D monolayer models. Sidgwick et al reported very low, but significantly increased HAS1 expression in NS compared to keloid scar tissue. 45 They also demonstrated a greater abundance of HAS1 protein, through immunohistological analysis, in keloid tissue compared to NS. 45 This was attributed to the thicker epidermis identified in keloid tissue. 45 Overall, the observed decrease in HAS1 expression in 3D scar models by Limandjaja et al and in scar tissue by Sidgwick et al best reflects in vivo regulation within the scar microenvironment.
KDKs had increased expression of HAS2 mRNA when compared with NS samples. 44 When HAS2 was inhibited, there was decreased migration of KDKs, a key step in keloid pathogenesis. 39 Contrarily, HAS2 mRNA expression was shown to be increased in NS compared to keloid tissue in the study by Sidgwick et al. 45 HAS3 mRNA expression was similar between KDKs and NS cells isolated from 2-D monolayer cultures. 44 A comparable trend was also seen at the protein level between KDFs and NS cells under the same culture conditions. 45 These studies suggest that there is variability in HA synthase mRNA expression in keloid tissue. However, while HAS1 and HAS2 mRNA expression were decreased in keloid tissue relative to NS, at the protein level, expression of all markers was weak, and no significant differences were observed. 45 Notably, accumulation of HAS protein in keloid tissue was greater than that in NS, presumably due to the thicker epidermis. 45 The functional implications of low transcript levels but increased protein abundance remain unclear.
Aberrant HA Levels Explained by Metabolic Variation
The decreased HA levels seen in the cell models of keloids may be attributed to increased turnover and metabolic dysregulation-associated degradation. Specifically, this could be due to altered expression and activity of genes associated with HA binding, like VCAN, TSG6, HMMR, LYVE1, LAYN, CD44, and TLR4, and genes associated with HA processing, like CEMIP, HYAL1, HYAL2, and TMEM2.39,42–44,46–48 There was no reported significant difference in the expression of CD44 or VCAN in KDFs when compared with NS.40,43 However, microarray analysis and immunohistochemistry demonstrated increased mRNA expression of VCAN and protein deposition of VCAN in keloid tissue relative to NS, respectively.49,50 VCAN is thought to contribute to keloid pathology through its role in excessive proteoglycan deposition and subsequent increase in keloid volume. 49 Reduced expression of TSG6 was observed in keloid tissue. 42 This reduction suggests that resultant impaired HA cross-linkage, a principal function of TSG6, may contribute to aberrant ECM formation in keloids, in turn facilitating their progression. Notably, in a study of postburn injury patients, expression of TSG6, assessed by immunohistochemistry and quantitative polymerase chain reaction (qPCR), was significantly lower in keloids compared to hypertrophic scars. 51 This difference may reflect differences in ECM organization, with hypertrophic scars demonstrating more organized collagen networking relative to keloids. 51
Decreased mRNA expression of hyaluronidases HYAL1 and HYAL2 has been demonstrated in KDFs relative to NS. 45 However, immunohistological analysis of keloid tissue demonstrates an increased abundance of HYAL in keloid tissue relative to NS, attributed to a thickened epidermis. 45 Expression of CEMIP, a hyaluronidase, was elevated in KF compared to normal fibroblasts. 52 In knockout studies of hyaluronidase CEMIP, HMW-HA depolymerization was fully suppressed, and KF proliferation and ECM deposition were impaired.47,52 Inversely, in knockout studies of hyaluronidase TMEM2, HA depolymerization was enhanced. 47 Although expression levels of CEMIP and TMEM2 have not been reported in whole keloid tissue, potential aberrant expression of these genes may affect HA turnover in keloids.
Overall, these studies suggest that altered expression and activity of genes associated with HA binding, processing, and depolymerization led to dysregulated HA metabolism in scar tissue. This provides insight into the mechanisms underpinning the decreased levels of HA in scar tissue relative to NS.
Production and Localization of HA
The functional consequence of HA depends upon its production and localization, both of which are aberrant in keloid and hypertrophic scar tissue models.36–40,42 In keloids, HA was shown to be primarily located in the spinous and granular layers of the epidermis, while in NS, HA was located primarily in the dermis.36,37,42 In hypertrophic scars, HA was found in a narrow distribution within the papillary dermis. 36 Within keloids, an abnormal dense reticular pattern of HA staining has been observed. 42
These abnormalities are functionally significant because HA influences fibroblast phenotype and ECM organization.37,48,53 Dermal HA reduction impairs cell migration, matrix remodeling, and tissue hydration.37,48,53 Elevated epidermal HA impacts epidermal–dermal barrier function and signaling.37,48,53 Overall, the resulting microenvironment affected by altered HA metabolism is one that promotes keloid and hypertrophic scar pathogenesis through increased fibroproliferation and excess collagen deposition.37,48,53
Next Steps
While preclinical and clinical studies connect HA to keloid and hypertrophic scar pathogenesis and treatment, key gaps in the literature warrant further investigation. As characterized in Figure 1, the regulation of LYVE1, HMMR, LAYN, and TLR4 has not been fully demonstrated in existing literature pertaining to keloid and hypertrophic scar pathogenesis. With regard to TMEM2, 1 study demonstrated increased HA degradation in KDF following knockdown of TMEM2. Further validation of the whole keloid tissue is necessary to ascertain the role of TMEM2 as a relevant hyaluronidase. As such, further studies would benefit from a unified approach evaluating both mRNA and protein level expression of all the genes outlined in this narrative review, the hyaluronome, across keloid tissue, KDFs, hypertrophic scar tissue, hypertrophic scar-derived fibroblasts, and NS. Such an approach may provide a direct comparison of expression levels and comprehensive insight into HA regulation across scar tissue types and its potential role in pathogenesis. From a clinical standpoint, future trials should consider comparing intralesional injection versus topical application of HA with larger sample sizes, longer-term posttreatment follow-up, and heterogenous scar anatomical locations. Similarly, an important future direction expanding upon this narrative synthesis is a systematic review evaluating the effects of different methods of HA-based therapies (topical formulations vs intralesional) on keloid recurrence following excision.
Conclusions
Overall, this narrative review investigates the available experimental and clinical data connecting HA with keloid and hypertrophic scars. The reviewed cell-based studies suggest that altered production and turnover, and changes in the spatial distribution of HA in tissue are associated with keloid and hypertrophic scar pathogenesis. The reviewed clinical studies present early evidence supporting a role for HA as a treatment for keloid scars in humans. While these results show promise, more clinical and mechanistic studies will be necessary before clinical recommendations involving HA application for keloid and hypertrophic scar treatment can be made.
Supplemental Material
sj-docx-1-psg-10.1177_22925503261457127 - Supplemental material for The Role of Hyaluronan in Keloid and Hypertrophic Scar Pathogenesis and Treatment
Supplemental material, sj-docx-1-psg-10.1177_22925503261457127 for The Role of Hyaluronan in Keloid and Hypertrophic Scar Pathogenesis and Treatment by Jay Shah, Ayushi Bhatt, Sammie Yu, Kathleen A. Hill, Eva Turley and Caitlin J. Symonette in Plastic Surgery
Supplemental Material
sj-docx-2-psg-10.1177_22925503261457127 - Supplemental material for The Role of Hyaluronan in Keloid and Hypertrophic Scar Pathogenesis and Treatment
Supplemental material, sj-docx-2-psg-10.1177_22925503261457127 for The Role of Hyaluronan in Keloid and Hypertrophic Scar Pathogenesis and Treatment by Jay Shah, Ayushi Bhatt, Sammie Yu, Kathleen A. Hill, Eva Turley and Caitlin J. Symonette in Plastic Surgery
Footnotes
Author Contributions
AB conceptualized the project and developed the search parameters. AB and SY conducted the original search. JS conducted the secondary search, and expanded upon drafts prepared by AB, to prepare the final manuscript. KAH, ET, and CJS supervised the project. All authors provided feedback and contributed to revisions and the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.