
Abstract
Antiphospholipid syndrome is a systemic autoimmune disorder characterized by thrombotic events in the presence of antiphospholipid antibodies including lupus anticoagulant, anticardiolipin, and anti-β2-glycoprotein I antibodies. Catastrophic antiphospholipid syndrome is a rare but life-threatening variant, accounting for less than 1% of antiphospholipid syndrome cases, and is characterized by rapid progressive microvascular thrombosis and multiorgan failure. We report the case of a middle-aged man who developed catastrophic antiphospholipid syndrome associated with systemic lupus erythematosus, presenting with diffuse alveolar hemorrhage, acute kidney injury, vasculitis skin lesions, and severe thrombocytopenia. Management requires intensive care support, immunosuppressive therapy, intravenous immunoglobulin administration, cyclophosphamide administration, and delayed plasmapheresis. Despite multi-organ involvement and guarded prognosis, the patient survived following multidisciplinary management. This case highlights the importance of early recognition, rapid therapeutic intervention, and coordinated interdisciplinary care to improve survival in patients with catastrophic antiphospholipid syndrome.
Introduction
Antiphospholipid syndrome (APS) is an autoimmune disorder characterized by persistent antiphospholipid antibodies and the occurrence of arterial, venous, or microvascular thrombotic events.1-3 Catastrophic antiphospholipid syndrome (CAPS) is a rare and fulminant variant of the antiphospholipid syndrome that has been reported since 1992. Its prevalence is less than 1% in patients with antiphospholipid syndrome and is characterized by generalized microvascular thrombosis, multiorgan failure, and high mortality rates exceeding 50% despite intensive treatment.4,5
Diffuse alveolar hemorrhage is an uncommon but potentially fatal pulmonary manifestation of catastrophic antiphospholipid syndrome associated with immune-mediated pulmonary capillaritis. Clinically, it presents with hemoptysis, acute anemia, and respiratory failure, often requiring invasive mechanical ventilation. 6 The coexistence of thrombotic and hemorrhagic events, as in catastrophic antiphospholipid syndrome, represents a significant therapeutic challenge, particularly in patients with comorbidities such as chronic kidney disease. 7
The management of catastrophic antiphospholipid syndrome is based on a combined therapeutic approach, including anticoagulation, aggressive immunosuppression with glucocorticoids, intravenous immunoglobulin, plasmapheresis, and, in refractory cases, biologic agents such as rituximab or eculizumab. 8 Early identification and rapid initiation of multidisciplinary treatment are essential for improving prognosis.
The purpose of this publication is to present a present a case of a male patient with relevant cardiovascular and renal history who developed catastrophic antiphospholipid syndrome, presenting with severe respiratory, hematologic, renal, cutaneous, and hemodynamic involvement.
Case Presentation
A male patient in his early 50s residing in a Latin American country had a medical history of long-standing hypertension, deep vein thrombosis of the left lower limb, nephrolithiasis, and stage III chronic kidney disease. He denied any allergies or prior surgery. Current medications include losartan, amlodipine, doxazosin, quetiapine, and omeprazole. Both parents had diabetes mellitus.
Two months before admission, he was treated for a hypertensive emergency with neurological symptoms, including dysarthria and severe headache. Computed tomography (CT) revealed a left parietal hemorrhage without a midline shift, aneurysms, or vascular malformations. He was managed in the intensive care unit (ICU) with hemodynamic control and neurological monitoring, evolved favorably, and was discharged with antihypertensive therapy and outpatient follow-up.
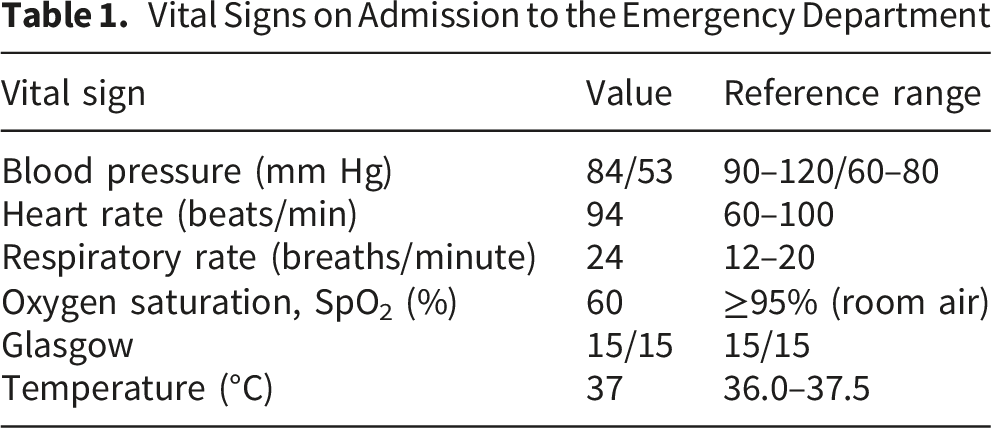
Vital Signs on Admission to the Emergency Department

Axial chest computed tomography (CT) demonstrates bilateral patchy ground-glass opacities and areas of consolidation, predominantly involving the lower lobes, with associated interlobular septal thickening and scattered nodular opacities.
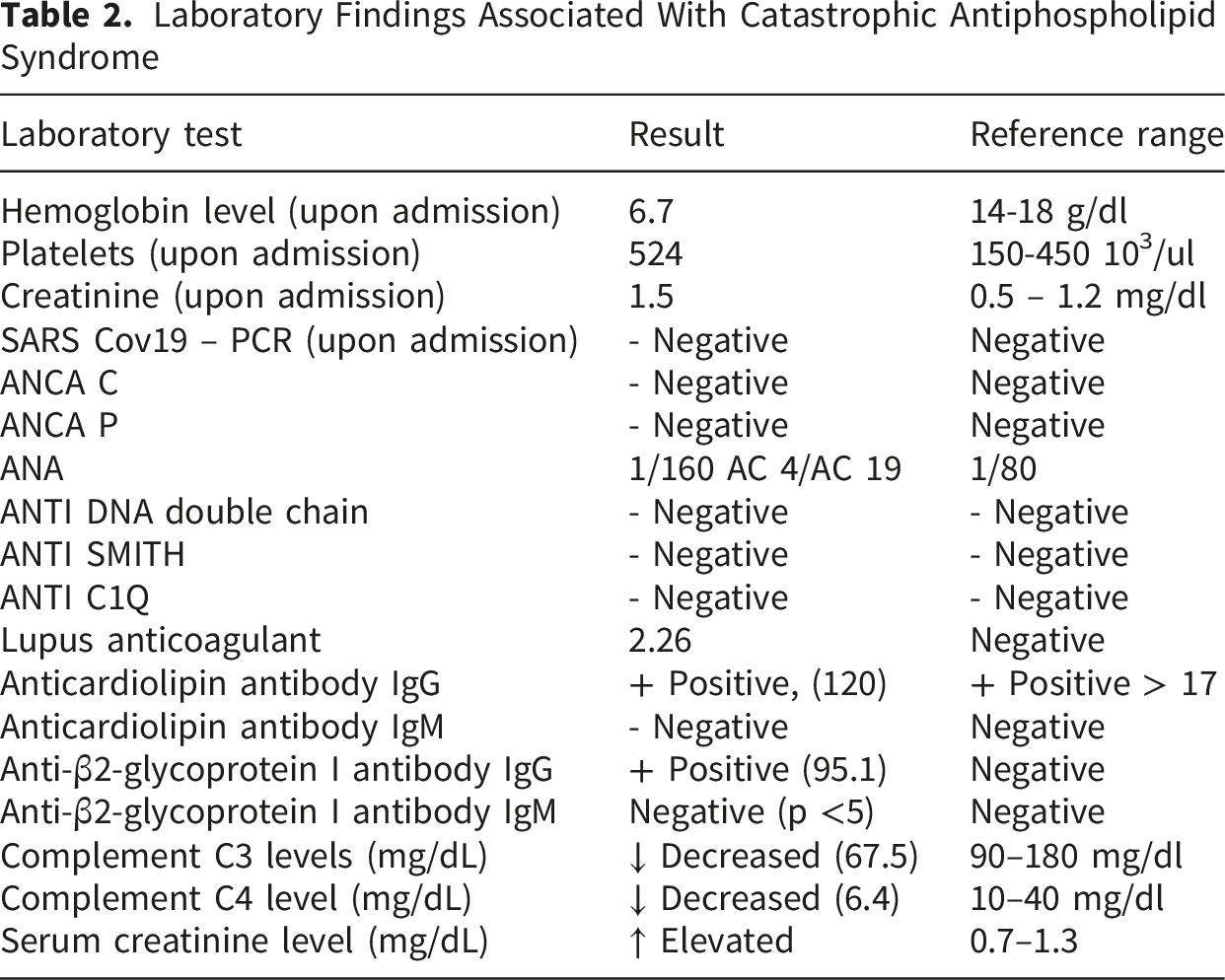
Laboratory Findings Associated With Catastrophic Antiphospholipid Syndrome
The patient received immunosuppressive and immunomodulatory therapy including pulse methylprednisolone (3 g over 3 days), intravenous immunoglobulin (0.4 g/kg/day for 5 days), a single intravenous dose of cyclophosphamide (1 g), and Pneumocystis jirovecii prophylaxis with trimethoprim-sulfamethoxazole until hospital discharge. Plasmapheresis was initially proposed as a rescue therapy due to a poor response to corticosteroids and immunoglobulin; however, it was deferred because of hemodynamic instability. After achieving stabilization, in coordination with nephrology, plasmapheresis was performed for five consecutive days, leading to clinical improvement.
The patient required vasopressor support, invasive mechanical ventilation, strict hemodynamic monitoring, fluid adjustment, and blood transfusion, as needed. Nephrology did not indicate urgent renal replacement therapy, as the criteria were not met; however, renal function was closely monitored. The nephrotoxic medications were adjusted, diuretics were initiated for fluid overload, and continuous bladder irrigation was required for hematuria. Based on these clinical manifestations, catastrophic antiphospholipid syndrome with severe pulmonary, hematologic, and cutaneous involvement was suspected. However, alternative diagnoses, including ANCA-associated small-vessel vasculitis and severe systemic lupus erythematosus flare, were initially considered. These were ruled out based on specific laboratory results.
During his 43-day hospitalization, the patient experienced multi-organ complications including thrombosis, hemorrhagic episodes, ventilator-associated pneumonia, and acute respiratory failure requiring ventilatory and vasopressor support. Despite a guarded prognosis, the patient was discharged after functional recovery, requiring initial nocturnal oxygen and rehabilitation therapies. He continued multidisciplinary follow-up every three months with anticoagulation treatment with warfarin 5 mg twice a week, 2.5 mg five times a week, hydroxychloroquine 300 mg daily, prednisone 5 mg daily, and regular antihypertensive medication.
Discussion
This case represents a severe and rare form of catastrophic antiphospholipid syndrome, characterized by multiorgan involvement and simultaneous thrombotic and hemorrhagic events. A history of deep vein thrombosis, intracranial hemorrhage, and chronic kidney disease suggests an underlying prothrombotic state that contributes to the development of CAPS.3,4
Diffuse alveolar hemorrhage (DAH) is one of the most severe manifestations of CAPS and is associated with high mortality. Its pathophysiology involves immune complex-mediated pulmonary capillaritis and complement activation, which results in endothelial damage and persistent alveolar bleeding.6,9 In this patient, acute respiratory failure required prolonged invasive mechanical ventilation and was complicated by ventilator-associated pneumonia, a common occurrence in this clinical context. 10 Severe hematologic involvement with hemolytic anemia and refractory thrombocytopenia contribute to persistent bleeding and limited full anticoagulation, which is central to CAPS management. 11 Renal involvement likely reflects both lupus nephritis and catastrophic antiphospholipid syndrome-associated thrombotic microangiopathy. 12
The treatment approach is aligned with the current recommendations for catastrophic antiphospholipid syndrome, employing combined therapy with high-dose glucocorticoids, intravenous immunoglobulin, cyclophosphamide, and plasmapheresis. 8 “Triple therapy” has been associated with improved survival compared to incomplete regimens.5,13 However, the inability to administer rituximab and delayed plasmapheresis owing to hemodynamic instability and resource limitations represent significant barriers.
Multidisciplinary management, involving intensive care, rheumatology, nephrology, pulmonology, hematology, and internal medicine, is fundamental. Despite the initial severe deterioration, the patient survived, defying the high mortality described in catastrophic antiphospholipid syndrome with severe multiorgan involvement.4,14
Conclusions
Catastrophic antiphospholipid syndrome is a rare but severe condition that requires a high level of clinical suspicion and prompt initiation of combined therapy. Diffuse alveolar hemorrhage represents a life-threatening complication that significantly worsens the clinical course. In low-resource settings, limited access to advanced therapies may adversely influence patient outcomes. Early multidisciplinary management is therefore essential to optimize treatment strategies and reduce morbidity and mortality.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent to Participate
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.