
Abstract
Acute fibrinous organizing pneumonia (AFOP) is a rare form of interstitial lung disease characterized histopathologically by intra-alveolar fibrin “balls” and organizing pneumonia. AFOP is associated with infections, malignancies, and immune dysregulation, posing diagnostic and therapeutic challenges. We present the case of a 66-year-old female with rectal adenocarcinoma, chronic obstructive pulmonary disease (COPD), and a posterior mediastinal mass who was admitted with sepsis and post-obstructive pneumonia. Imaging revealed consolidations in the right middle and lower lobes with adjacent abscess formation. Lung biopsy confirmed AFOP, demonstrating intra-alveolar fibrin balls and organizing pneumonia. Cultures identified Streptococcus anginosus and Prevotella melaninogenica, indicating a polymicrobial infection. The patient was treated with antibiotics; corticosteroids were withheld due to active infection and immunosuppression from malignancy. Surgical intervention addressed the mediastinal mass and abscess. The patient recovered without AFOP recurrence. This case highlights the diagnostic complexity of AFOP, especially in patients with multiple risk factors such as malignancy, infection, and immunosuppression. The decision to withhold corticosteroids underscores the importance of individualized therapy. Clinicians should consider AFOP in the differential diagnosis of acute lung infiltrates, particularly in patients with malignancies or infections. Prompt recognition and tailored management can improve outcomes in this rare condition.
Keywords
Introduction
Acute Fibrinous Organizing pneumonia (AFOP) is a rare pneumonic process of unknown prevalence characterized by acute lung injury with histopathologic features of intra-alveolar deposition of “fibrin balls” 1 and can be idiopathic in nature or associated with infection, drugs and immunocompromised states. 2 Herein, we present a case of AFOP in a 66-year-old female.
Case Presentation
A 66-year-old female with a history of hypertension, hyperlipidemia, prediabetes, Chronic Obstructive Pulmonary Disease (COPD) on triple therapy Fluticasone/Umeclidinium/Vilanterol with a 50-pack-year smoking history, posterior mediastinal mass of unknown etiology, and rectal adenocarcinoma (previously partially resected but not currently under treatment) presented with a two-day history of cough and progressive shortness of breath. On arrival, she was hypoxic (88% on room air, improving with oxygen), tachycardic, hypotensive with systolic blood pressures in the 70s despite fluid boluses, and in moderate respiratory distress. Physical examination revealed decreased breath sounds and crackles over the right lower lung. Laboratory findings included leukocytosis (WBC 20 × 109/L) with a left shift, elevated procalcitonin (6.05 ng/mL), normocytic anemia (hemoglobin 9 g/dL), and lactic acidosis. A chest X-ray showed right lower lobe opacities, and a Computed Tomography (CT) scan revealed an 8.3 x 7 x 8 cm posterior mediastinal mass causing right lower lobe atelectasis, a moderate pleural effusion, and a moderate pericardial effusion (Figure 1). The patient was started on broad-spectrum antibiotics (meropenem, vancomycin) and admitted to the Medical Intensive Care Unit (MICU) for septic shock, likely secondary to post-obstructive pneumonia. Computed Tomography of the chest with contrast – mediastinal window (Left, coronal view & Right, axial view) shows a large heterogeneous solid mass in the mediastinum with post-obstructive pneumonia of the right lower lobe
On day two, her oxygen requirements decreased, and she was downgraded to the medical floor. A CT-guided thoracentesis drained 250 mL of serous pleural fluid, which was negative for infection or malignancy. Blood cultures grew Gemella morbillorum, which was deemed a contaminant. Sputum culture revealed Staphylococcus aureus. A septic workup was otherwise unremarkable. Echocardiography revealed an ejection fraction of 60-65%, grade 1 diastolic dysfunction, mild aortic valve sclerosis, and moderately elevated pulmonary systolic pressure.
Thoracic surgery was consulted for evaluation of the mediastinal mass, and on day 7, she underwent video-assisted thoracoscopic surgery (VATS), converted to a mini-thoracotomy. The procedure included right lung and chest wall decortication, lysis of dense intrapleural adhesions, drainage of a walled-off right lung abscess, wedge resection of the right lung, and biopsy of the posterior mediastinal mass. Pathology of the lung wedge revealed acute organizing pneumonia with extensive intra-alveolar fibrin balls, type 2 pneumocyte hyperplasia, and acute fibrinous pleuritis without evidence of malignancy (Figure 2). The mediastinal mass demonstrated fibrinopurulent exudate and fibroblastic proliferation with no malignancy. Cultures of the lung abscess grew Streptococcus anginosus and Prevotella melaninogenica, prompting continuation of antibiotics (meropenem and levofloxacin). Hematoxylin & Eosin stain of right lung resection at 40x (Left) & 10x (Right) showing intra-alveolar fibrin balls (black arrows) and type 2 pneumocyte hyperplasia (red arrow)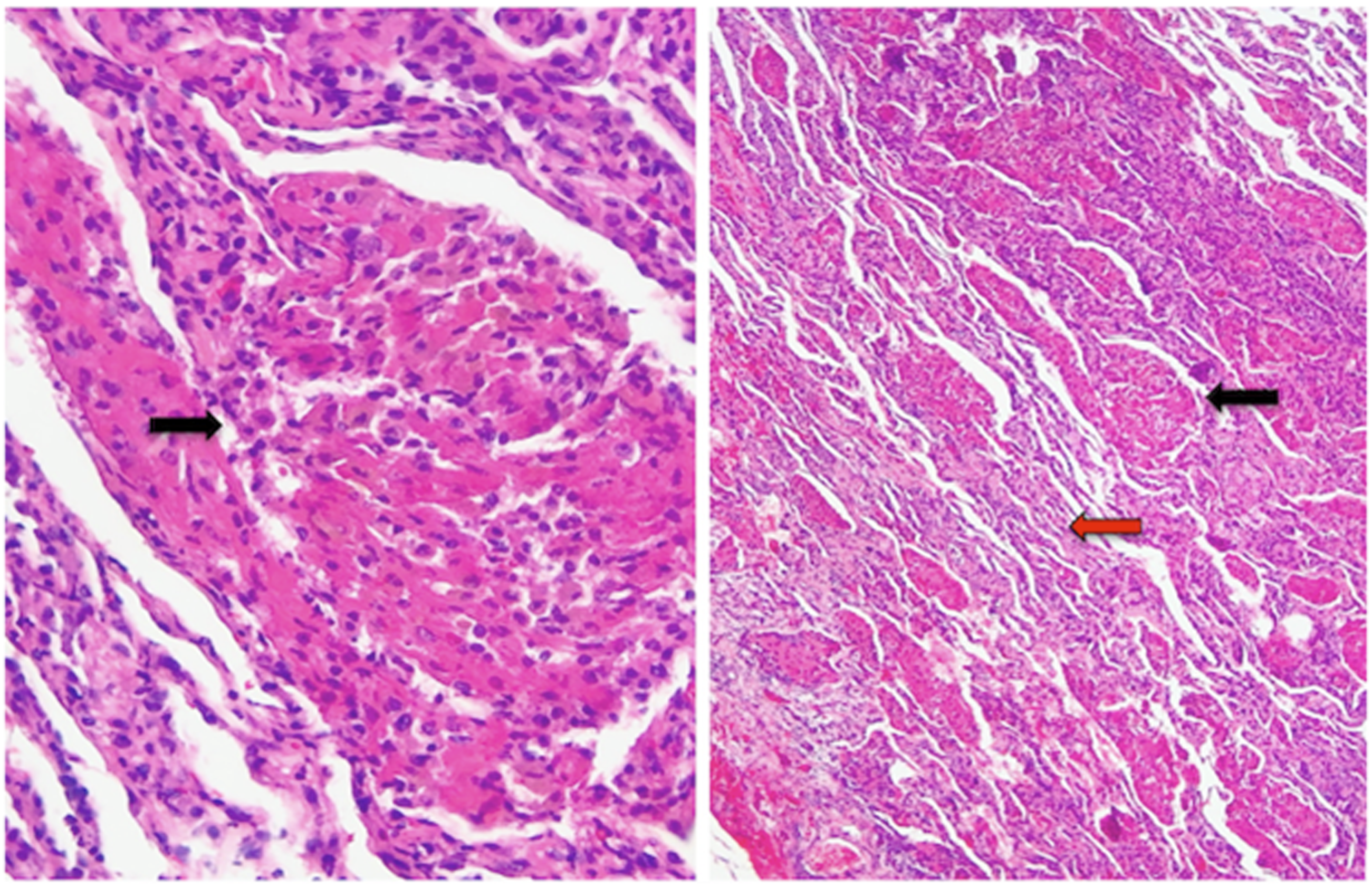
Postoperatively, the patient initially required ICU-level care with intubation and vasopressor support but was subsequently extubated and transitioned to the medical floor. After stabilization, she was discharged to rehabilitation on day 18 with supplemental oxygen and a two-week course of antibiotics. A follow-up was planned for ongoing management of her mediastinal mass and COPD.
Discussion
Acute fibrinous and organizing pneumonia (AFOP) was first described by Beasley et al. in 2002 as a distinct histological pattern associated with acute or subacute lung injury. 1 Since then, over 100 cases have been reported in the literature, providing additional, but still limited insight into the disease. 2 Due to its extreme rarity and different presentations, the clinical manifestations and long-term prognosis of AFOP remain poorly understood.
AFOP is still considered a subcategory of rare histologic patterns of ILD and was not included as a new idiopathic interstitial pneumonia (IIP) entity according to the last update of the International multidisciplinary classification of the idiopathic interstitial pneumonias by the ATS/ERS published in 2013, 3 because it was not clear whether it represents a unique, standalone IIP entity or a variant of existing IIPs or exists only in association with other conditions such as hypersensitivity pneumonitis (HP) 4 or collagen vascular disease (CVD). 5 Further published cases during the last 12 years supported that it may be idiopathic in nature or can be associated with underlying conditions like connective tissue diseases, infections, drug reactions, environmental exposures, and recent lung transplantation. 2 AFOP was also reported in some cases as a paraneoplastic syndrome, especially in association with hematological neoplasia like lymphoma.6,7 Solid tumors were rarely reported and it is unclear if the cancer itself or treatment might be linked to the disease. 8
The histopathologic pattern of AFOP is intra-alveolar fibrin deposition described as “fibrin balls” along with organizing pneumonia. A Classic hyaline membrane of diffuse alveolar damage is absent. Another important consideration is to rule out eosinophilic pneumonia by the absence of tissue and peripheral eosinophilia, as this histopathologic pattern can be seen in eosinophilic pneumonia, this diagnosis should be excluded. 3
The diagnosis of AFOP is likely obscured in many cases, particularly when it presents as secondary to infection, such as pneumonia or lung abscess. There are no specific radiologic findings that definitively point to AFOP, as the imaging typically shows consolidations, ground-glass opacities, or nodules that are indistinguishable from infectious pneumonia or other acute lung processes.2,9,10 Pleural involvement is uncommon. Most likely reported as an uncomplicated pleural effusion. 2 Furthermore, there are no early clinical signs to guide the need for lung biopsy in these patients, especially when cultures are positive and the patient is already being treated for confirmed pneumonia with appropriate clinical response. In such scenarios, clinicians have little reason to pursue invasive tissue diagnosis, as the working diagnosis of bacterial pneumonia appears sufficient to explain the clinical picture. This diagnostic challenge is compounded by the fact that AFOP often mimics treatment-resistant pneumonia, and patients may initially improve with antibiotics if there is a concurrent infectious component, further obscuring the underlying histopathologic pattern.10-12 As a result, AFOP may be significantly underdiagnosed in clinical practice, with many cases going unrecognized unless tissue is obtained for other indications.13,14
In our patient, the diagnosis of AFOP was made incidentally during a surgical procedure performed for therapeutic purposes rather than for diagnostic purposes. The indication for video-assisted thoracoscopic surgery (VATS) was therapeutic—to drain the abscess, perform decortication, and biopsy the mediastinal mass—not to investigate an unexplained pneumonia. Had the patient not required surgical intervention for these complications, the AFOP would likely have remained undiagnosed, as she was already receiving appropriate antibiotic therapy for her polymicrobial infection with clinical improvement. The true incidence of AFOP in the setting of severe bacterial pneumonia may therefore be substantially higher than currently recognized in the literature.
The clinical presentation and microbiological findings in our patient strongly suggest that infection was the primary driver of AFOP rather than malignancy. While viral infections (respiratory syncytial virus, influenza) and atypical bacteria (Legionella, Chlamydia) have been most commonly reported, bacterial pneumonia can trigger the AFOP pattern, particularly when associated with intense inflammatory responses.2,9,15 In our patient, the subsequent development of a walled-off lung abscess with dense intrapleural adhesions and empyema represents a severe, complicated bacterial infection—precisely the type of intense inflammatory process associated with AFOP. 9 Even though, Streptococcus anginosus and Prevotella melaninogenica bacteria that grew in the surgical specimen cultures were not linked to AFOP previously this association must be considered especially that Streptococcus anginosus group (SAG) bacteria are well-recognized causes of severe pulmonary infections with a propensity for abscess and empyema formation and frequently present in polymicrobial infections in synergy with oral anaerobes like Prevotella species.16,17
While AFOP has been reported as a paraneoplastic syndrome, this association is predominantly with hematological malignancies such as lymphoma and myelodysplastic syndromes.6,7 Solid tumors are rarely reported in association with AFOP, and when they occur, it remains unclear whether the cancer itself, cancer treatment, or concurrent infections are responsible for the AFOP pattern.7,8 Our patient had rectal adenocarcinoma that was not actively being treated, and the mediastinal mass—initially concerning for malignancy—was found on pathology to represent fibrinopurulent exudate and fibroblastic proliferation without evidence of malignancy. This finding further supports infection rather than malignancy as the primary etiology. Moreover, the patient’s immunosuppression from cancer-related cachexia and chronic COPD with inhaled corticosteroid use likely predisposed her to severe bacterial infection rather than directly causing AFOP. The absence of any cancer treatment (chemotherapy, radiation) eliminates drug-induced or radiation-induced AFOP from consideration.
Given the scarce cases and variable prognosis of AFOP, there is still no standard therapy for this disease and treatment methods remain controversial. While corticosteroids are effective in 94% of AFOP cases, their use must be carefully considered in the context of active infection.2,9 In our patient, treatment with antibiotics and withholding corticosteroids was deemed appropriate given the presence of active polymicrobial infection, lung abscess, empyema, and immunosuppression from malignancy-related cachexia. This decision reflects the principle that when AFOP is secondary to infection, treating the underlying infection takes priority, and corticosteroids may be contraindicated until the infection is controlled.10,15 The successful resolution of AFOP without corticosteroid therapy in our patient further supports infection as the primary etiology.
Few studies have investigated the long-term prognosis of AFOP, with significant limitations given the rarity of the disease contributing to a low study sample.7,18 The literature review published in 2021 by Chen et al., which studied all cases reported since 2002, revealed a death rate of 39% among all 150 patients. 2 Morbidity and mortality were significantly higher in patients with secondary AFOP compared to idiopathic cases.2,7 These findings highlight the need for further research to better understand the long-term outcomes of AFOP and to identify strategies for improving survival, particularly in patients with secondary AFOP who face a significantly higher risk of morbidity and mortality.
Conclusion
Given the poor prognosis associated with AFOP, clinicians should have a high index of suspicion in immunocompromised patients with multiple comorbidities presenting with pneumonic features, to ensure timely diagnosis and treatment with corticosteroids and immunosuppressants if clinically indicated.
This diagnostic challenge has important implications for understanding the true prevalence of AFOP. This case raises the possibility that AFOP goes unrecognized because tissue is not obtained when patients have culture-confirmed pneumonia with an appropriate clinical response to antibiotics. The coexistence of AFOP with severe bacterial infections may be more common than currently appreciated in literature, but the diagnosis requires histopathologic confirmation that is rarely pursued in straightforward infectious cases.9,10
Footnotes
Acknowledgements
Authors report no acknowledgements.
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent to Participate
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Prior Presentation of Abstract Statement
The case was presented as an abstract in the ATS 2023 conference, Washington D.C. May 19-24, 2023.