
Abstract
Autoimmune pericarditis is commonly idiopathic but may represent the initial manifestation of systemic autoimmune disease. Hepatic autoimmune disorders rarely present with primary cardiac involvement, and recognition of extrahepatic presentations is essential for early diagnosis and prevention of organ damage. Autoimmune hepatitis–primary biliary cholangitis (AIH–PBC) overlap syndrome is an uncommon entity characterized by combined hepatocellular and cholestatic immune-mediated injury. A previously healthy young woman presented with progressive pleuritic chest pain and dyspnea and was found to have a large pericardial effusion causing hemodynamic compromise requiring surgical drainage. Pericardial pathology demonstrated acute and chronic fibrinous pericarditis. Initial evaluation revealed elevated inflammatory markers and mild transaminitis with positive autoimmune serologies including antinuclear antibody and anti–smooth muscle antibody. Following clinical improvement, she developed recurrent pericarditis accompanied by worsening liver enzyme abnormalities. Liver biopsy demonstrated chronic active hepatitis with bile duct injury and bridging fibrosis, consistent with autoimmune hepatitis–primary biliary cholangitis overlap syndrome. Cardiac magnetic resonance imaging confirmed active pericardial inflammation without myocarditis. Immunosuppressive therapy with corticosteroids followed by azathioprine resulted in clinical stabilization. This case highlights autoimmune pericarditis as the presenting manifestation of AIH–PBC overlap syndrome and underscores the importance of evaluating unexplained pericarditis for systemic autoimmune disease. Early recognition of cardio-hepatic autoimmune overlap allows timely immunosuppressive therapy and may prevent progression to advanced hepatic fibrosis.
Keywords
Introduction
Acute pericarditis accounts for approximately 5% of emergency presentations for chest pain, with most cases classified as idiopathic or presumed viral in origin. 1 However, autoimmune disorders represent an important but underrecognized etiology, particularly in patients with recurrent disease or systemic abnormalities. 1 Extrahepatic manifestations are well described in autoimmune liver diseases, yet cardiac involvement is rare and seldom represents the initial presentation.
Autoimmune hepatitis (AIH) and primary biliary cholangitis (PBC) are immune-mediated liver diseases with distinct pathogenic mechanisms. Overlap syndrome, characterized by features of both conditions, occurs in approximately 5–10% of autoimmune liver disease cases and is associated with more aggressive progression if untreated. 2 We report a case in which autoimmune pericarditis served as the initial clinical manifestation leading to the diagnosis of AIH–PBC overlap syndrome.
Case Presentation
A previously healthy 23-year-old woman presented with one week of worsening pleuritic chest pain and dyspnea superimposed on six months of progressive exertional symptoms. The pain was sharp, intermittent, and radiated to the back without relief with aspirin.
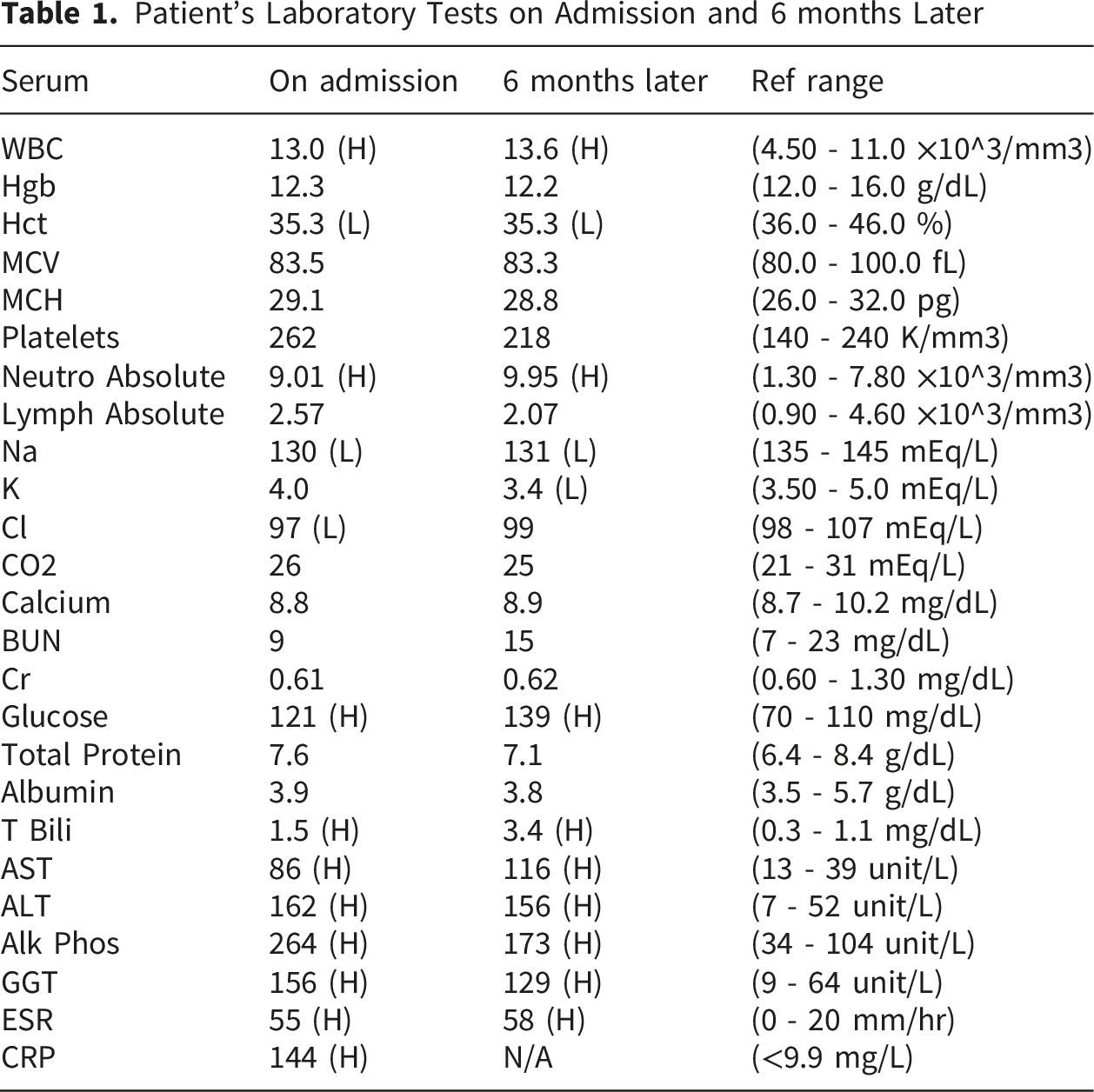
Patient’s Laboratory Tests on Admission and 6 months Later
Computed tomography excluded pulmonary embolism but confirmed a large pericardial effusion and mediastinal lymphadenopathy. Abdominal ultrasound showed mild hepatomegaly without biliary obstruction.
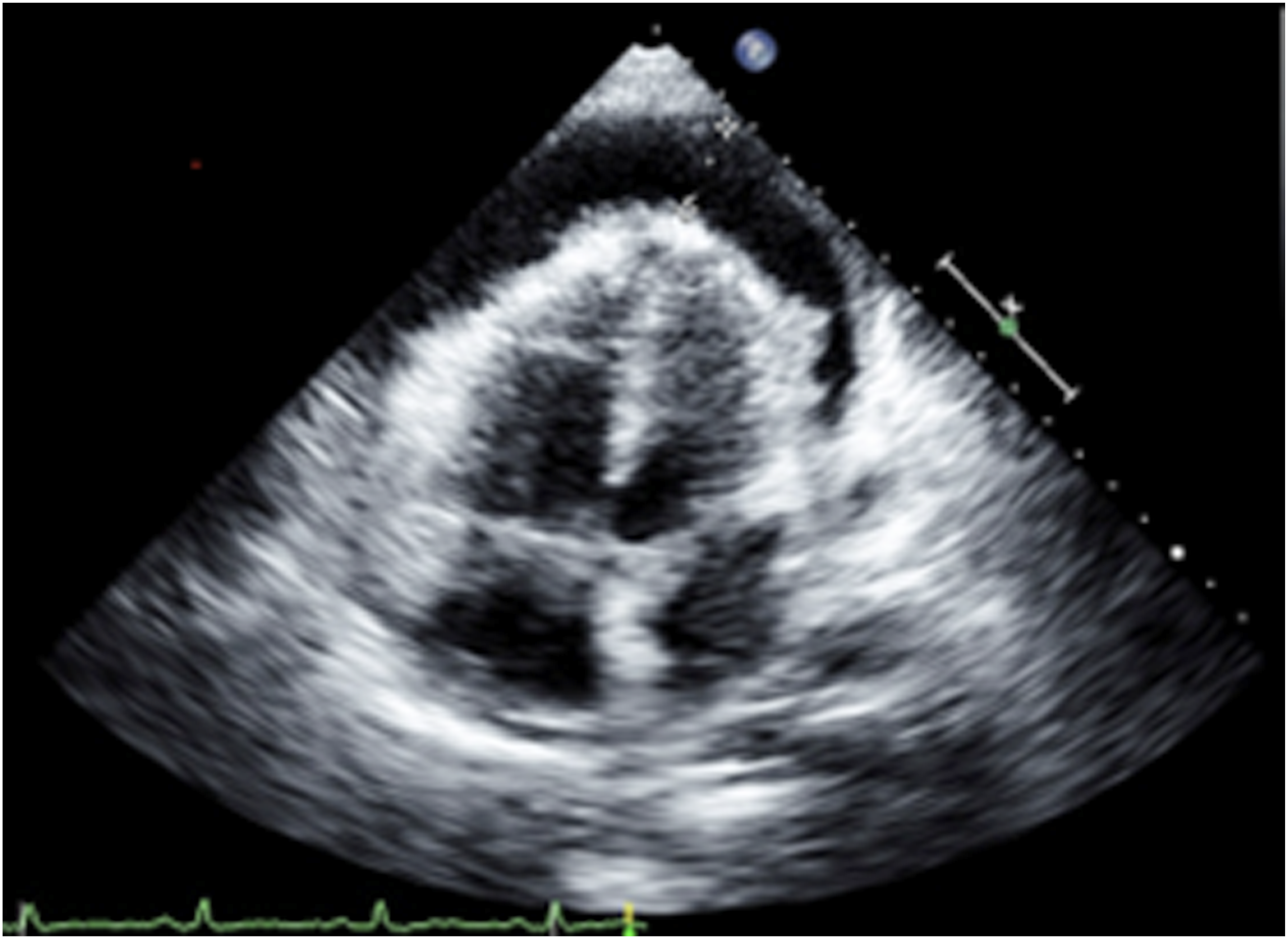
Transthoracic echocardiography revealed preserved left ventricular function with a large pericardial effusion and features of hemodynamic compromise (Figures 1 and 2). The patient underwent surgical pericardial window with drainage of serous fluid. Transthoracic echocardiography demonstrates large circumferential pericardial effusion on short axis view Transthoracic echocardiography demonstrates large circumferential pericardial effusion on apical view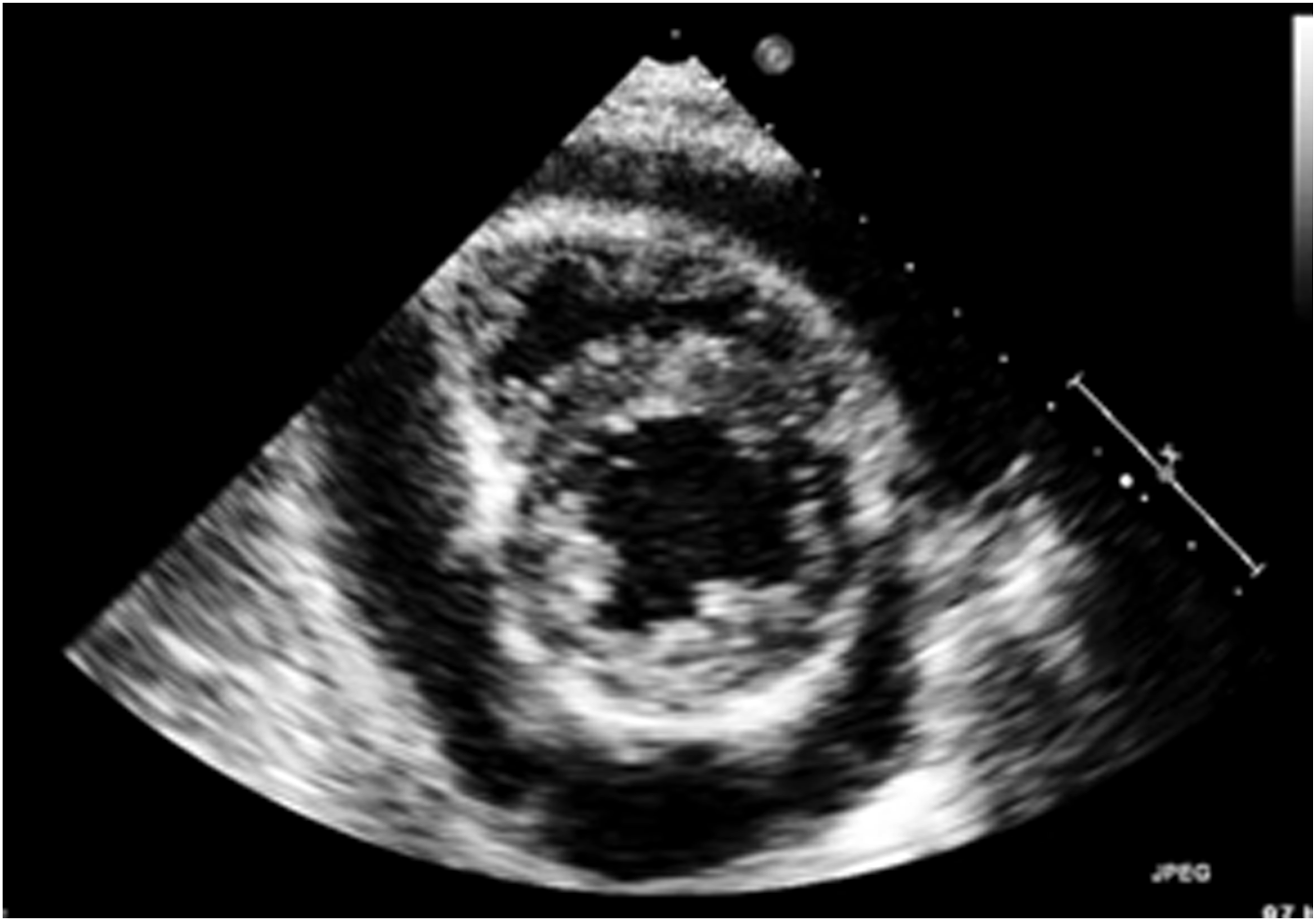
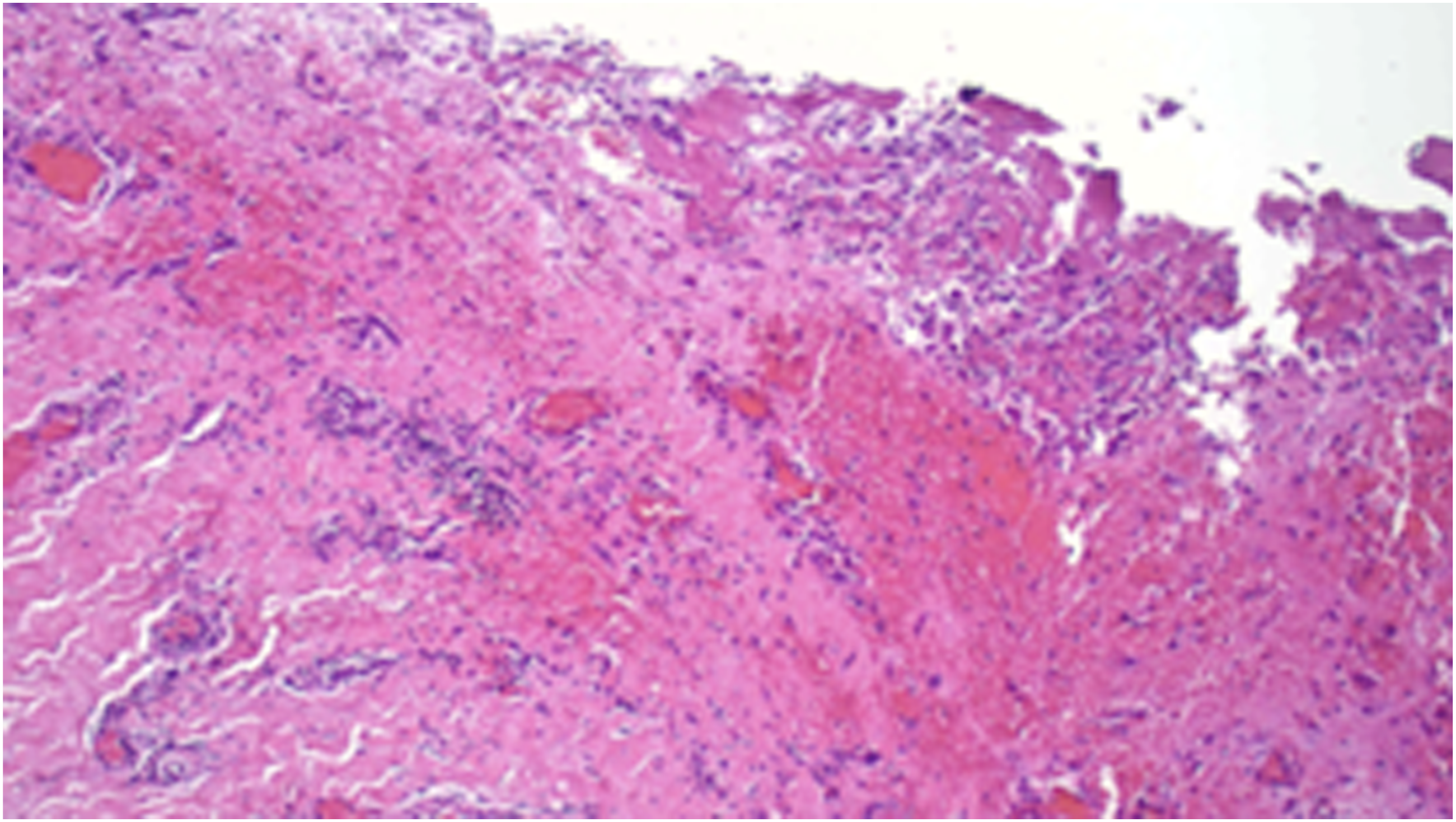
Pericardial fluid gram stain showed no organisms, and bacterial cultures were negative. Acid-fast bacilli smear and mycobacterial cultures of pericardial fluid and tissue were similarly unrevealing. Fungal stains and cultures were negative. Cytology was negative for malignancy. Pericardial tissue pathology demonstrated acute and chronic fibrinous pericarditis without granulomatous inflammation (Figures 3 and 4). Serologic evaluation, including HIV antibody, hepatitis B and C serologies, and respiratory viral panel, were negative. Viral nucleic acid amplification testing of pericardial fluid was not performed, as routine viral PCR is not standard practice given its limited impact on management. Renal and thyroid function were normal. Pericardium1 (100x): Thickened pleura showing marked fibrinous pericarditis with abundant fibrin, neutrophils and histiocytes Pericardium2 (200x): Focal small amount of perivascular lymphocytic infiltrates also noted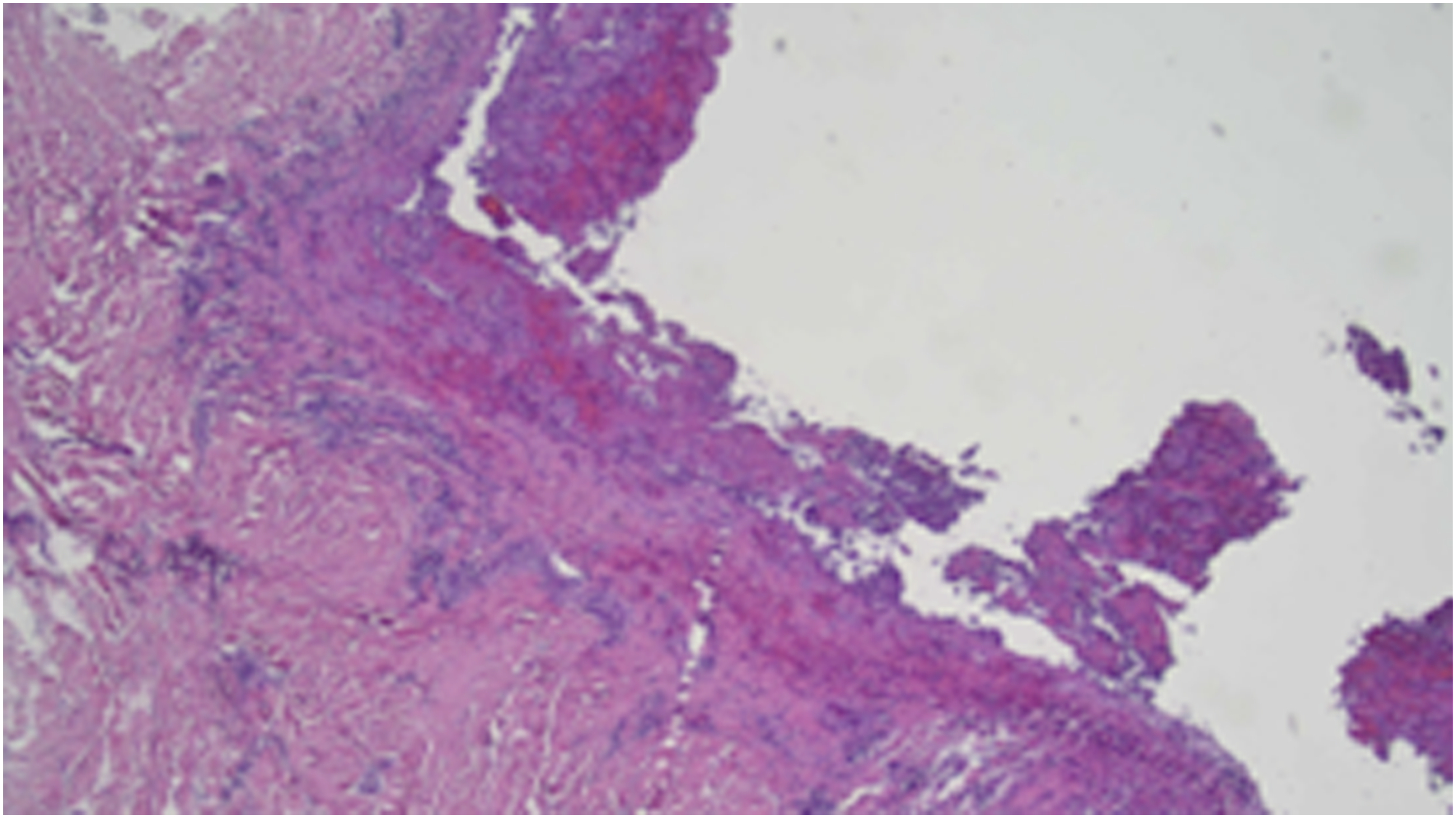
Given the negative infectious workup, autoimmune evaluation was pursued, which demonstrated elevated inflammatory markers, positive anti–smooth muscle antibody and initially negative ANA that converted to high-titer homogeneous pattern on subsequent clinic follow up (1:640).
Symptoms improved following drainage and anti-inflammatory therapy, and she was discharged with colchicine and nonsteroidal therapy.
Approximately one month later, follow-up imaging showed resolution of the pericardial effusion and improvement in mediastinal lymphadenopathy. However, she returned several weeks later with recurrent chest pain after discontinuation of anti-inflammatory therapy. Laboratory evaluation demonstrated leukocytosis and worsening liver biochemical abnormalities.
Repeat echocardiography revealed a small recurrent pericardial effusion without tamponade physiology. Given persistent elevated liver enzymes and autoimmune serologies, a percutaneous liver biopsy was performed.
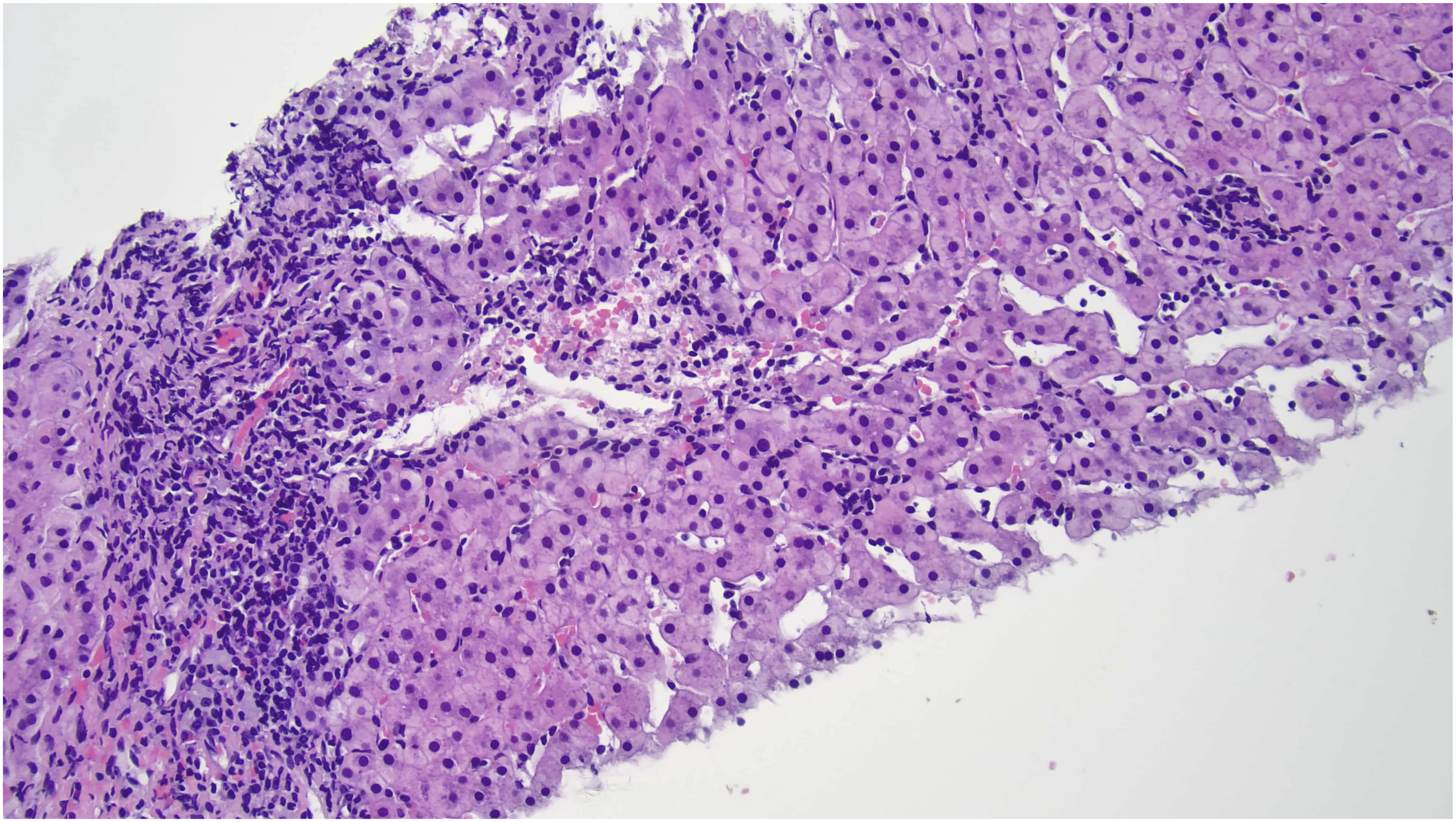
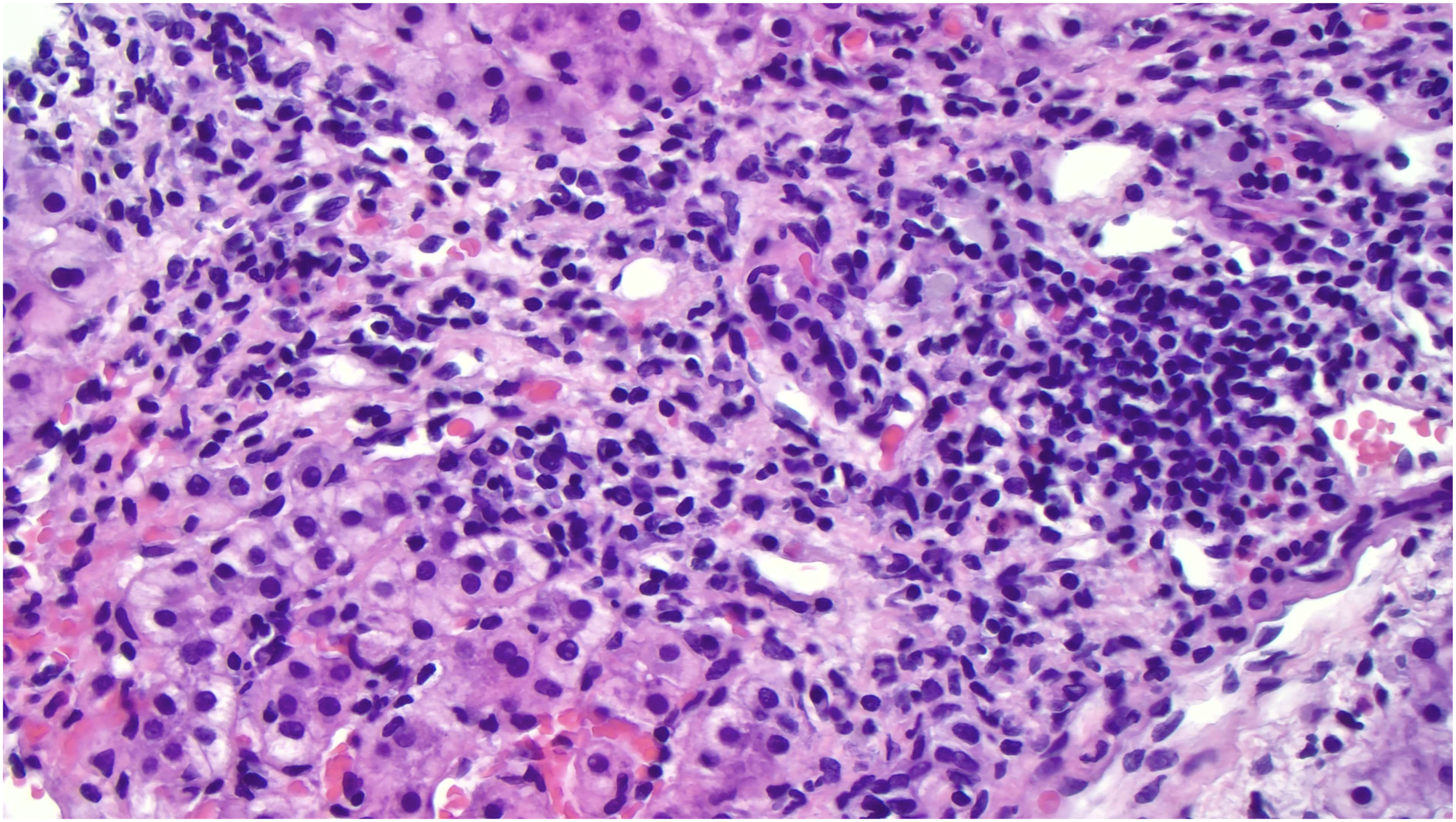
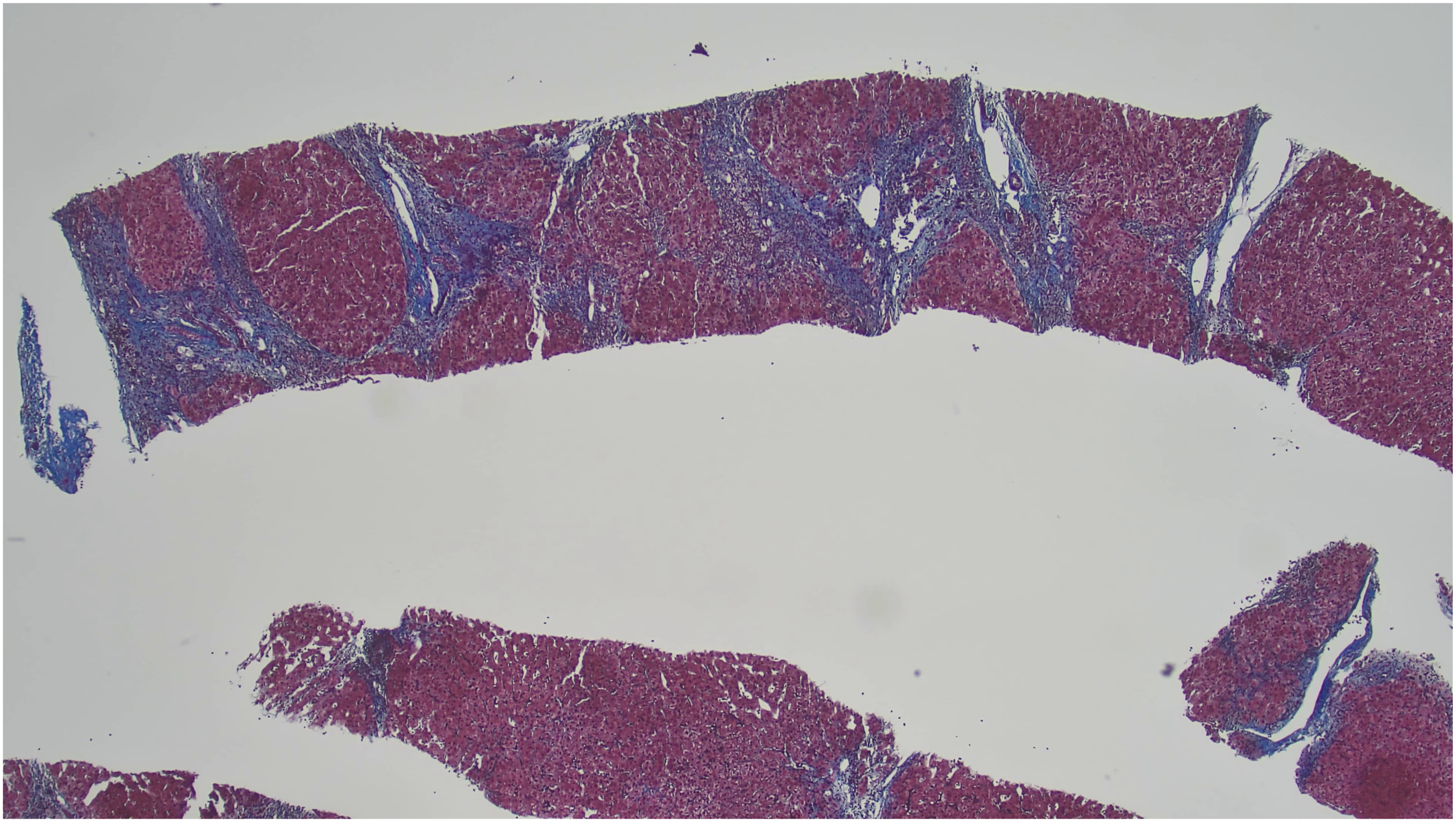
Histopathology demonstrated chronic active hepatitis with portal and interface inflammation, bile duct injury, and portal-to-portal bridging fibrosis (Figures 5-8), consistent with autoimmune hepatitis–primary biliary cholangitis overlap syndrome. Liver bx1 (100x): Low power view showing extensive portal chronic inflammation and interface hepatitis Liver bx2 (200x): Showing scattered lobular activities with hepatocyte damage (spotty necrosis) Liver bx3 (400x): High power view showing abundant lymphocytes and focal scattered plasma cells in the portal tract and interface Liver bx4 (20x): Trichrome stain highlighting the portal-to-portal and focal portal-to-central bridging fibrosis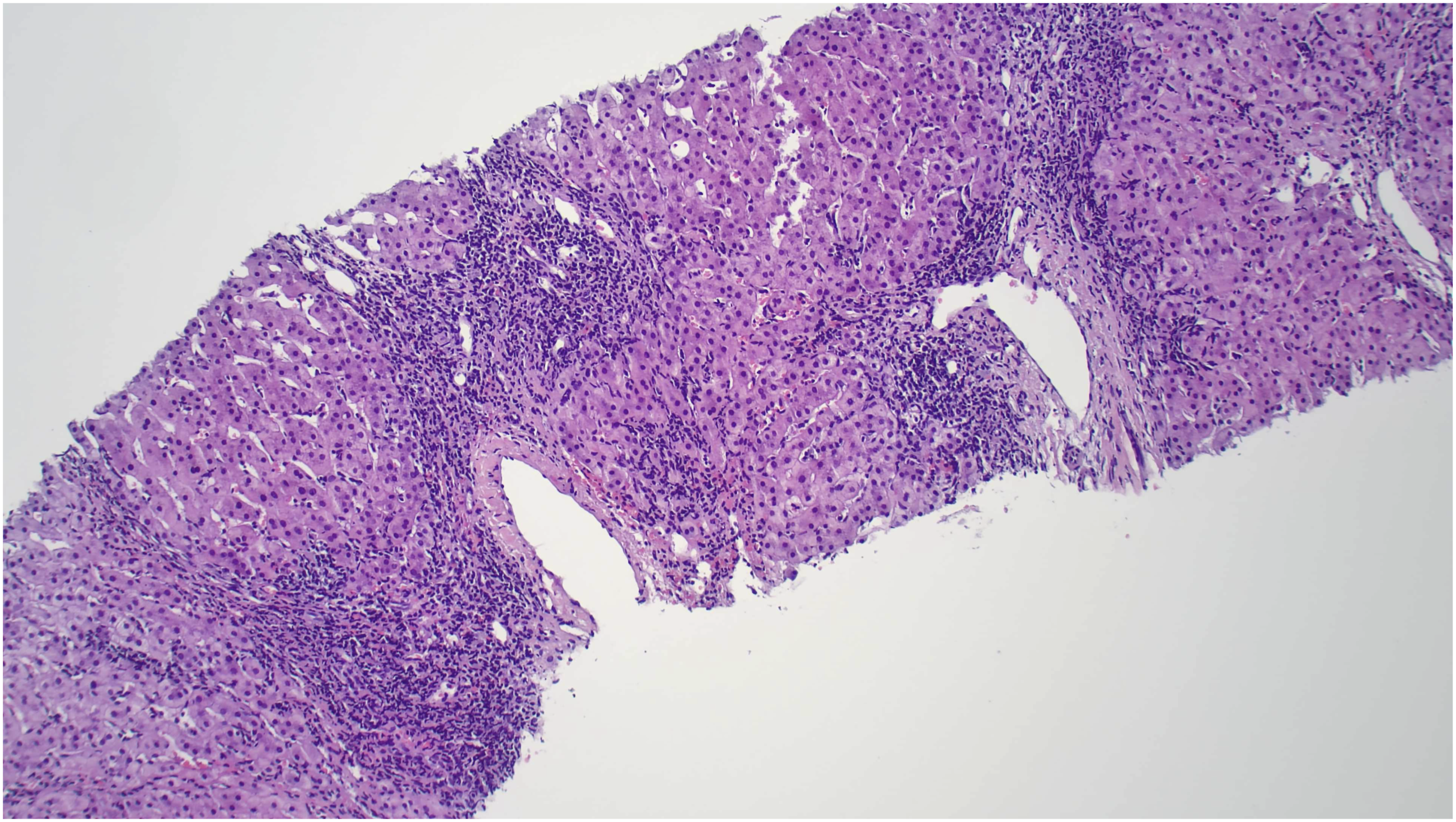
Cardiac magnetic resonance imaging demonstrated diffuse pericardial enhancement consistent with active pericarditis without myocarditis.
The patient was initiated on prednisone followed by azathioprine for maintenance immunosuppression, resulting in clinical improvement. She continues multidisciplinary follow-up with cardiology, rheumatology, and hepatology.
Discussion
Autoimmune liver diseases (AILDs), including autoimmune hepatitis (AIH) and primary biliary cholangitis (PBC), are chronic inflammatory disorders characterized by immune-mediated hepatic injury. Extrahepatic autoimmune manifestations are well described in AILDs, occurring in approximately 30–44% of patients with AIH and 42% of patients with PBC.3-5 The most commonly associated extrahepatic conditions include autoimmune thyroid disease, Sjögren syndrome, celiac disease, and various rheumatologic disorders.3-5 In AIH-PBC overlap syndrome, in which patients simultaneously exhibit features of both autoimmune hepatitis and primary biliary cholangitis, up to 44% of patients have concurrent extrahepatic autoimmune diseases, with autoimmune thyroid disease (18%), Sjögren syndrome (8%), and rheumatoid arthritis (4%) being most prevalent. 6
Cardiac manifestations in the context of autoimmune diseases extend across the entire spectrum of cardiac pathology and are increasingly recognized, with patients having 1.4-3.6 times higher risk of cardiovascular disease compared to those without autoimmune disorders. 7 Most common cardiac manifestations include atherosclerotic disease, inflammatory cardiac diseases (including pericarditis and myocarditis), infection-related heart disease, and venous thromboembolism. 7 Systemic autoimmune diseases contribute to approximately 22% of pericarditis cases with a known etiology with SLE being fairly most common autoimmune disease causing pericarditis with incidence around 20-50%, typically during disease flares and usually accompanied by other systemic features such as rash, arthritis, or pleuritis.8,9 In rheumatoid arthritis and systemic sclerosis pericardial involvement usually occurs as asymptomatic pericardial effusion rather than active pericarditis.8,9
However, pericarditis as an isolated presenting manifestation of autoimmune liver disease in the absence of systemic rheumatic disease is exceedingly rare and poorly characterized in the literature. The pathophysiology of pericarditis in autoimmune conditions involves dysregulation of both innate and adaptive immune responses, with pericardial inflammation triggered by activation of the inflammatory cytokines such as interleukin-1β.8,9 The present case suggests that similar immune dysregulation may have precipitated pericarditis in the setting of undiagnosed AIH/PBC overlap syndrome, though this association remains poorly characterized in the literature.
Even though the infectious workup for her pericarditis was negative, viral etiology of pericarditis cannot be definitively excluded as viral pericarditis is a diagnosis of exclusion and most cases of idiopathic pericarditis are presumed to be viral in etiology, but the patient’s lack of preceding viral prodrome such as a flu-like or gastrointestinal illness, positive autoimmune serologies, and eventually response to immunosuppressive therapy favored an autoimmune rather than viral etiology.
During the patient initial presentation, her mildly elevated liver enzymes were thought to be due to congestion due to the pericardial effusion and potential tamponade versus a systemic viral infection causing both pericarditis and mild liver injury. Due to persistent elevated transaminases further infectious and autoimmune workup was ordered and the patient was found to have positive ASMA suggestive of concurrent autoimmune liver disease. Given that the patient was asymptomatic and had mild elevation of liver enzymes ASMA titer was initially also thought to be falsely positive as it could be in numerous conditions unrelated to autoimmune hepatitis including bacterial, viral, autoimmune diseases and even in healthy individuals as low titer and close monitoring was decided.
In subsequent clinic follow-ups after patient was discharged from the hospital, she continued to have mildly elevated liver enzymes with no symptoms with repeated autoimmune workup showing persistent elevated ASMA, but her repeated ANA was converted to positive at 1:640 from negative during hospitalization. The patient was referred to rheumatology, but further workup showed no evidence of any systemic rheumatic disease. During that time the patient was on treatment for idiopathic pericarditis and receiving colchicine and NSAIDs which are both well-known to cause elevated liver enzymes. A liver biopsy was later considered necessary given her persistent mild transamenitis despite completing therapy for pericarditis.
The diagnosis of AIH-PBC overlap syndrome in this patient was established as she met the Paris criteria for the diagnosis which requires two of three criteria for each disease.2,10,11 For PBC: (1) alkaline phosphatase ≥2-fold upper limit of normal (ULN) or GGT ≥5-fold ULN, (2) positive antimitochondrial antibodies (AMA), and (3) florid bile duct lesions on histology. 2 For AIH (in addition to interface hepatitis): (1) ALT ≥5-fold ULN and (2) IgG ≥2-fold ULN or positive smooth muscle antibodies.2,11 This patient demonstrated histologic features of both diseases on liver biopsy, with interface hepatitis and bile duct injury. She had elevated alkaline phosphatase at 264 U/L (reference range 34-104 U/L) and positive anti-smooth muscle antibodies at 75 and 44 units on repeat testing (reference range 0-19 units). However, she had only mild elevations in GGT, AST, ALT and IGG that did not meet the Paris criteria thresholds, and her AMA was negative. Despite not meeting all the aspects of Paris criteria, the combination of histologic findings showing features of both diseases, elevated alkaline phosphatase, and positive ASMA were enough to establish the diagnosis of overlap syndrome. This highlights important limitations of current diagnostic approaches. The Paris criteria have not been independently validated and may exclude patients with less severe biochemical abnormalities. 2
The histopathologic findings in this case—chronic active hepatitis with portal and interface inflammation, bile duct injury, and advanced fibrosis (stage III/IV)—are characteristic of overlap syndrome.12,13 The presence of both periportal lymphocytic piecemeal necrosis (typical of AIH) and bile duct injury (typical of PBC) on the same biopsy specimen is a hallmark feature. 13
The natural history of AIH-PBC overlap syndrome appears more aggressive than isolated PBC, with earlier onset of portal hypertension and increased need for liver transplantation.2,10,12 In this case, the patient presented with advanced fibrosis (stage III/IV) at diagnosis despite being only 23 years old, suggesting a prolonged subclinical phase and luckily her diagnosis was not delayed even further. However, with appropriate treatment, outcomes can be favorable and delay the development of cirrhosis. 14
The management of recurrent pericarditis in this patient required careful consideration. The 2025 ACC Expert Consensus Statement on pericarditis emphasizes the role of anti-inflammatory therapy, typically with NSAIDs and colchicine with avoiding steroids as it was associated with higher recurrence rates.15,16 However, in the context of underlying autoimmune disease, systemic immunosuppression may be necessary.8,16 The initiation of systemic corticosteroids for the overlap syndrome likely provided dual benefit for both hepatic and pericardial inflammation.
Conclusion
This case highlights autoimmune pericarditis as the presenting manifestation of AIH–PBC overlap syndrome and underscores the importance of evaluating unexplained pericarditis for systemic autoimmune disease. The presence of extrahepatic autoimmune manifestations may obscure the underlying liver disease and liver biopsy may be delayed contributing the abnormal liver enzymes to other factors like treatment side effects. Liver biopsy remains essential for establishing the diagnosis of overlap syndrome and guiding therapy, as serologic and biochemical features alone may be insufficient, as in our patient the biopsy was deferred as her AFTs were only slightly elevated.
The multidisciplinary approach employed in this case—involving cardiology, rheumatology, and hepatology—exemplifies the complexity of managing patients with overlap syndromes and extrahepatic manifestations. Long-term monitoring will be essential to assess treatment response, disease progression, and the potential for additional autoimmune complications.
Footnotes
Acknowledgements
Authors report no acknowledgements.
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for Publication
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.