
Abstract
Melanoma is an aggressive malignancy with a high propensity for metastasis; however, clinically apparent involvement of the gastrointestinal tract is uncommon. We report a case of metastatic melanoma involving the stomach that presented as gastrointestinal bleeding shortly after initial diagnosis. A patient with recently diagnosed melanoma with nodal metastasis presented with melena and symptomatic anemia. Esophagogastroduodenoscopy revealed multiple gastric mucosal lesions that were notably amelanotic, lacking the characteristic pigmentation typically associated with melanoma. Histopathological and immunohistochemical evaluation confirmed metastatic melanoma, and imaging findings were concerning for advanced disease. The presence of pneumatosis raised suspicion for mucosal compromise and possible early perforation, highlighting the potential severity of gastrointestinal involvement. Gastrointestinal metastases from melanoma are often clinically silent and may present with nonspecific symptoms, leading to delayed diagnosis. This case is notable for early symptomatic presentation and the presence of amelanotic lesions, which may be easily overlooked during endoscopic evaluation. The absence of pigmentation can pose a diagnostic challenge and requires a high index of suspicion in patients with a history of melanoma. Early endoscopic evaluation and tissue diagnosis are essential for timely recognition and management. Clinicians should maintain a high index of suspicion for gastrointestinal metastases in melanoma patients presenting with unexplained anemia or bleeding, even in the absence of classic endoscopic features.
Keywords
Introduction
Melanoma is an aggressive malignancy of the skin and the sixth most common cancer in the United States. 1 Although it can involve any part of the body, the most common sites of metastasis are the liver, bone, and brain. 2 Metastatic gastric involvement is relatively rare and clinically diagnosed only in 2% of patients. 3 Most gastric melanomas are asymptomatic and are detected at autopsy. 4 Amelanotic malignant melanoma contributes to less than 2% of all malignant melanomas and among them gastric metastasis is extremely rare. 5 This case is therefore notable for three distinct challenges: the early timing of symptomatic gastric metastasis, the amelanotic endoscopic appearance, and the concurrent anticoagulation-related hemorrhagic complexity in a patient with multiple comorbidities.
Case Presentation
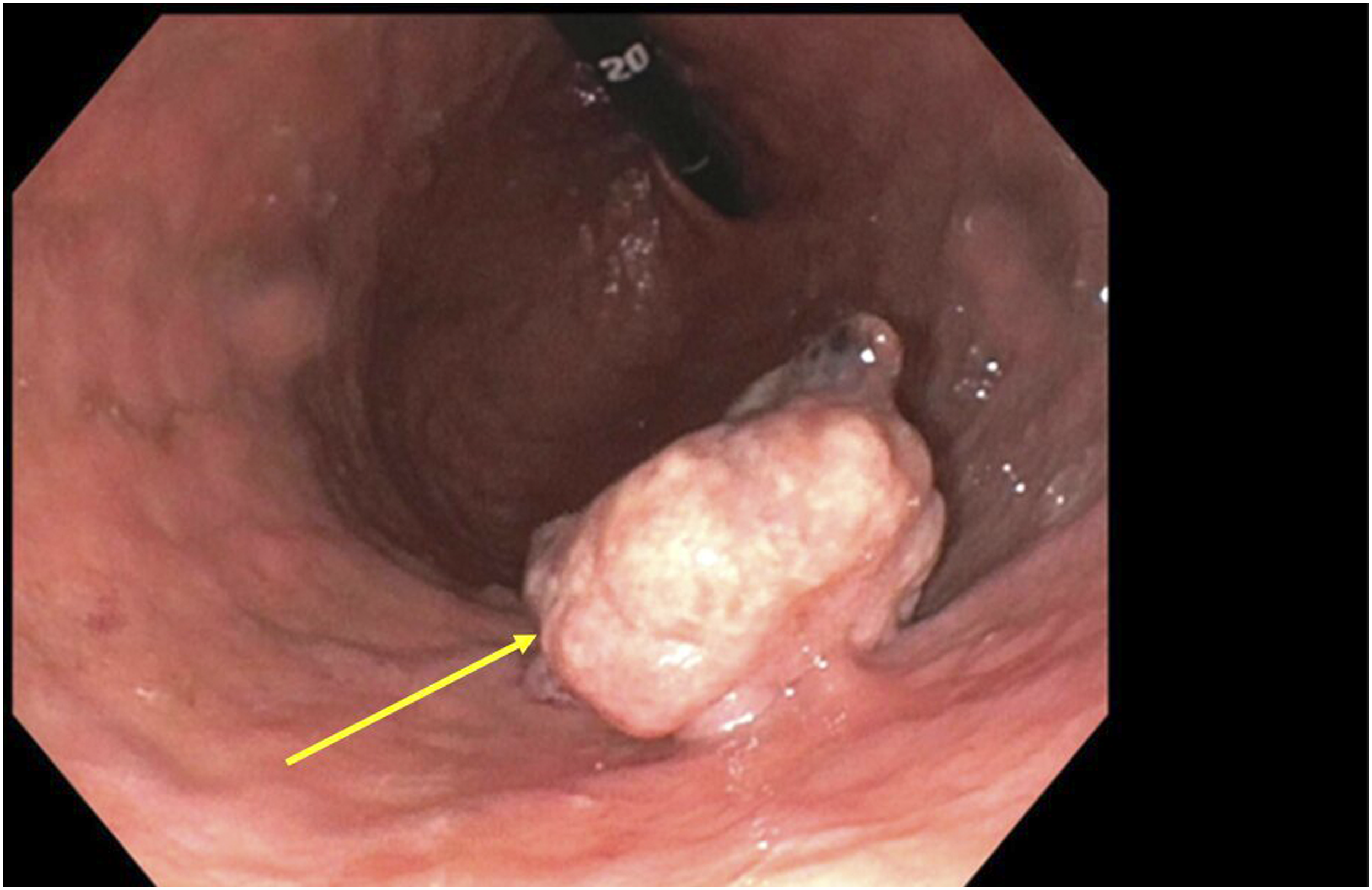
63-year-old Hispanic female with past medical history of Type 2 Diabetes mellitus, hypertension, hyperlipidemia, hypothyroidism, Stage IV metastatic malignant melanoma, bicuspid aortic valve, post mechanical valve replacement on warfarin, presented to the emergency department with complaints of nausea, and lower abdominal pain. She was diagnosed with metastatic melanoma 2 months before this current presentation during which time she was found to have a right pelvic mass which was excised, and pathology confirmed the diagnosis of metastatic melanoma with extensive necrosis. She was planned to be started on dual immune checkpoint inhibitors (Nivolumab and ipilimumab), but she never received immunotherapy before presentation. Physical examination was normal except mild tenderness in the lower abdominal quadrants. Laboratory parameters at admission were significant for moderate anemia with HbG of 7.8 and elevated INR at 2.3. Contrast-enhanced computed tomography (CT) of the abdomen and pelvis showed transition point in the small bowel with irregular intraluminal high-density material at the point of transition representing bowel contents or neoplastic intraluminal process and concerns of bowel obstruction (Figure 1), however patient had a melenic bowel movement the next day. Her hemoglobin dropped from 7.8 g/dL to 6.8 g/dL. Her INR was in the supratherapeutic range and hence Warfarin was stopped and Vitamin K was given. Gastroenterology was consulted and esophagogastroduodenoscopy showed two medium-sized, fungating, non-circumferential amelanotic mass on the anterior wall of the stomach and cardia (Figures 2 and 3) which were biopsied and hemostatic spray was applied over the lesion to stop bleeding. Once upper gastrointestinal bleed clinically resolved and hemoglobin stabilized, she was started back on therapeutic anticoagulation. Histopathology from the gastric mass biopsy showed poorly differentiated malignant neoplasm consistent with metastatic melanoma. Immunohistochemistry confirmed the melanocytic origin of the tumor cells, which were positive for SOX10 (Figure 4), S100 (Figure 5), and HMB45 (Figure 6), supporting the diagnosis of metastatic melanoma; negativity for pankeratin excluded a primary gastric adenocarcinoma or carcinoma of another origin, and negativity for CD45 excluded a hematolymphoid neoplasm such as lymphoma. BRAF mutation analysis was negative. She had recurrent melena and drop in hemoglobin. CT angiography of the abdomen showed multiple dilated small bowel loops with pneumatosis and portal venous gas with possible transition point in mid abdomen at the distal third portion of the duodenum with findings concerning for small bowel obstruction and also focal area of bowel wall thickening at duodenum/jejunal junction with adjacent mesenteric fat stranding concerning for bowel ischemia. Technetium-99m labeled RBC scan demonstrated pooling of blood in the mid-abdomen, likely from the small bowel, suggestive of hyperemia with concern for intraperitoneal bleeding, though no definite bleeding source was identified. Highlights the contrast enhanced tomography finding of small bowel obstruction with transition point (indicated by yellow arrow) Demonstrates a medium-sized, non-circumferential amelanotic mass in the subcardial region (Siewert type III location), consistent with metastatic melanoma Demonstrates a medium-sized, fungating, non-circumferential amelanotic mass on the anterior wall of the stomach, consistent with metastatic melanoma Shows the immunohistochemistry staining of gastrointestinal mass showing strong positivity for SOX10 stain, confirming melanocytes origin Demonstrates immunohistochemical staining of the gastrointestinal mass with strong positivity for S100, supporting diagnosis of metastatic melanoma Demonstrates immunohistochemical staining of the gastric mass showing cytoplasmic positivity for HMB45, confirming the diagnosis of metastatic melanoma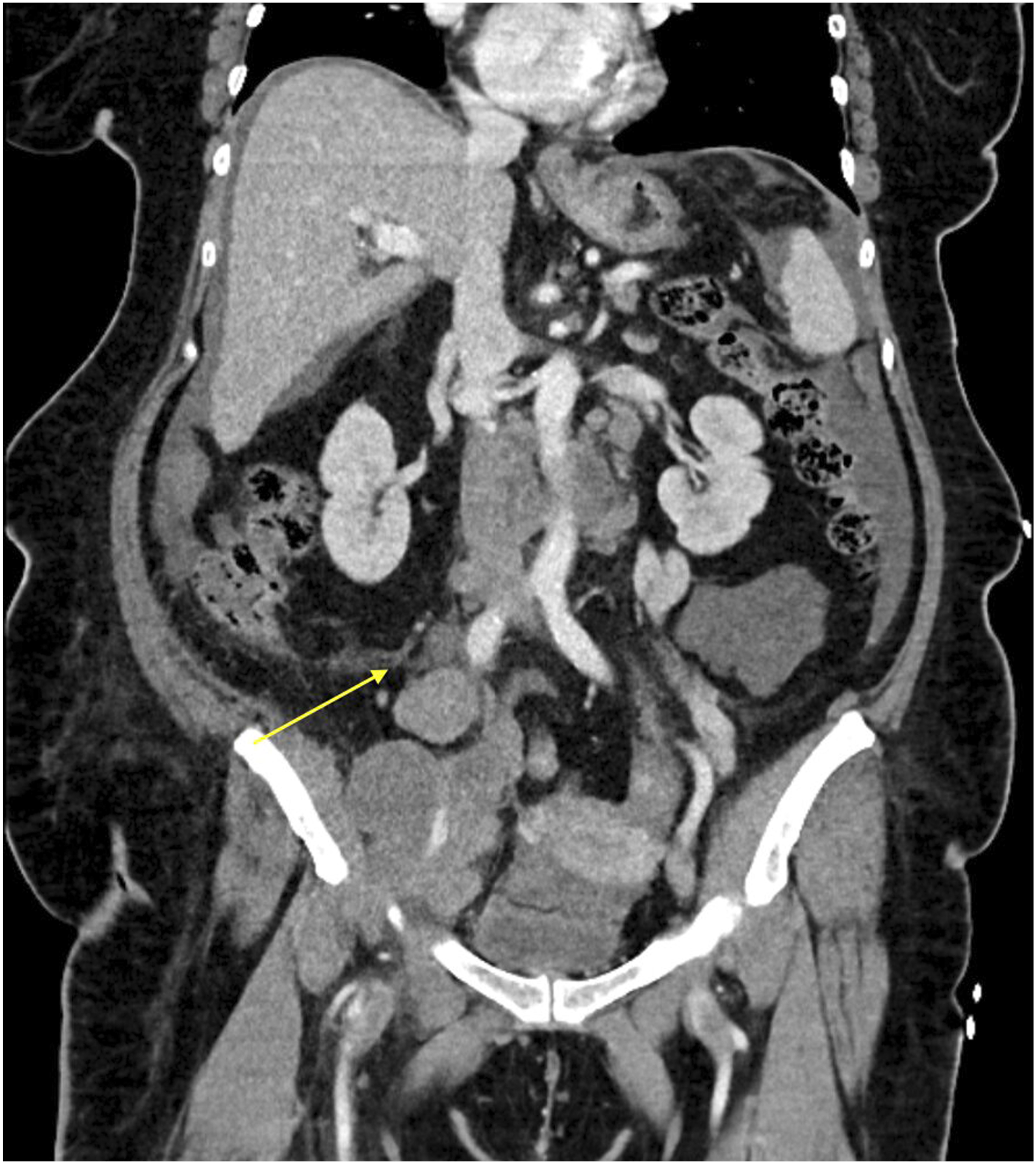




General surgery was consulted. However given the patient’s rapid progression of tumor, acute gastrointestinal bleed with SBO and bowel ischemia and her high surgical risk, after a multidisciplinary discussion, patient and her family chose hospice care and was discharged to home hospice.
Discussion
Melanoma is an aggressive skin malignancy of melanocytes. 6 According to NCI’s (National Cancer Institute) Surveillance, Epidemiology, and End Results (SEER) program, the age-adjusted incidence rate of melanoma of the skin in the United States is approximately 21.9 new cases per 100,000 persons per year, based on 2018-2022 data. The corresponding age-adjusted mortality rate is about 2.0 deaths per 100,000 persons per year, based on 2019–2023 data. 7 Melanoma is the sixth most common cancers in the U.S., with higher incidence rates observed among non-Hispanic White individuals compared with other racial and ethnic groups. 8 The incidence rate in Hispanic individuals is approximately 5 compared to 31.8 in White individuals. 9 According to American Society of Clinical Oncology (ASCO), only about 4% of melanomas present with metastasis. 10 Our patient was stage IV at the time of diagnosis, and it was initially identified in the right pelvic region which on later evaluation was found to have metastasized from skin lesion between her first and second toe.
Involvement of the gastrointestinal tract by malignant melanoma is uncommon, occurring in only approximately 1–5% of patients, despite much higher rates seen in autopsy studies (up to 60%) that reveal occult GI spread. 11 It has high affinity to small intestine followed by the stomach and colon. Gastrointestinal (GI) metastasis is most common in the small bowel (51–71%) followed by stomach (≈27%), and large bowel (≈22%). The high frequency of metastasis to GI tract is explained by strong expression of the chemokine receptor CCR9 on melanoma tumor cell surface which binds to the ligand CCL25 found predominantly on small intestine. Primary gastric melanoma is extremely rare and has very poor prognosis at the time of diagnosis. It comes under the category mucosal melanoma and constitutes 1.4% of melanomas. 12 When gastrointestinal metastases from melanoma become clinically evident, they often present with vague symptoms such as abdominal discomfort, weight loss, acute gastrointestinal bleeding or occult bleeding causing anemia.
Endoscopic evaluation is essential for the detection and characterization of gastrointestinal involvement in malignant melanoma. Reported findings demonstrate considerable heterogeneity, with lesions appearing as pigmented or nonpigmented nodules, ulcerated masses, polypoid growths, or submucosal tumors. Lesions may be solitary or multiple and are most frequently located in the gastric body or fundus.11,13 In some cases, early lesions may be small and subtle, increasing the risk of missed diagnosis. All lesions require biopsy and pathological confirmation of the tumor type. Amelanotic lesions may either represent a new metastasis of a known primary melanoma as in our case, or a new synchronous tumor. Although metastatic melanoma involving the stomach is uncommon and often diagnosed post-mortem, rare cases of synchronous gastrointestinal metastases—such as concurrent gastric and duodenal involvement—have been reported, highlighting that melanoma can disseminate simultaneously to multiple sites within the GI tract. 14 Advanced imaging techniques, including narrowband imaging and magnification endoscopy, may improve visualization of lesion margins and vascular patterns. Given the variable appearance and potential for initial nondiagnostic biopsies, repeat endoscopic assessment and close clinical follow-up are often necessary in suspected cases. 15
This case is notable for the rapid development of symptomatic gastric metastases within five months of initial diagnosis. While gastrointestinal involvement is often reported years after primary melanoma diagnosis and is frequently detected incidentally, our patient presented with overt gastrointestinal bleeding early in the disease course. An additional notable feature in our case was the presence of two distinct gastric mucosal lesions, suggesting multifocal metastatic involvement. Multiple gastrointestinal lesions are thought to reflect hematogenous dissemination and are often associated with more aggressive disease behavior. The multifocal gastric metastases presented as an unusual cause of gastrointestinal bleeding in our case.
Gastrointestinal metastases from melanoma also have a propensity to develop complications such as perforation. Pneumatosis identified in our case may represent an early sign of impending or contained perforation. Goodman and Karakousis described 22 cases of symptomatic gastrointestinal metastases from melanoma, reporting a median survival of 2.2 months. Among the six patients who were not candidates for surgery, two died due to perforation. In contrast, the 13 patients who underwent surgical intervention had a median survival of 4.5 months. 16
Over the past decade, the management of melanoma has been substantially transformed by the introduction of molecularly targeted therapies and immune checkpoint inhibitors, leading to significant improvements in treatment outcomes for many patients. 17
For BRAF-mutant melanoma, targeted therapy with combination of BRAF/MEK inhibitors (Vemurafenib, Dabrafenib and Trametinib) is the standard of care. Many patients show rapid response to the therapy but acquired resistance is common. It is seen in almost 50% of treated patients within 1 year of treatment. 18
The introduction of immune checkpoint inhibitors [ICI] has significantly improved outcomes for patients with advanced metastatic melanoma. Ipilimumab, an anti– cytotoxic T-lymphocyte associated protein 4 (Anti-CTLA-4) antibody, approved by the U.S. Food and Drug Administration (FDA) in 2011 was the first immune checkpoint inhibitor, for use in patients with metastatic melanoma. 19 It demonstrated objective response rates of approximately 11–15% and produced durable survival in a subset of patients, with pooled analyses showing a plateau in long-term survival at around 21% after three years. 20 Programmed cell death protein 1 (PD-1) inhibitors, including nivolumab and pembrolizumab, approved in 2014, further improved response rates to approximately 30–45% and were associated with superior overall survival and more favorable toxicity profiles.21,22 However, immune-related adverse events such as colitis, dermatitis, endocrinopathies, hepatitis, and myocarditis remain important limitations, particularly with combination therapy. 23 Perforation secondary to colitis is also reported in literature. 24 Despite durable responses in some patients, a substantial proportion exhibit primary or acquired resistance, highlighting the need for improved biomarkers and novel combination strategies to enhance long-term efficacy.25,26 ICIs are used for BRAF mutant melanoma as well and the choice of treatment depends on disease setting and goals. They have slower but sustained response. BRAF inhibitors combined with MEK inhibitors achieve rapid, high response rates (≈70%) in BRAF-mutant melanoma, which can be especially valuable for patients with high tumor burden. 27 Intralesional therapy with Talimogene laherparepvec (T-VEC) was approved by FDA in 2015 for unresectable, cutaneous, subcutaneous and nodal melanomas. It is a herpes simplex virus-1 based oncolytic immunotherapy. It has not been studied for visceral organ metastasis. 28 Trials are ongoing for newer agents and newer modalities of treatment.
Prognosis of metastatic malignant melanoma is poor. 5-Year survival rate is reported to be <10%. Mean survival is 6 to 8 months. 29
The diagnosis of gastric metastasis in our patient had important implications for clinical management and prognostic assessment. Identification of gastrointestinal involvement prompted reassessment of disease burden and therapeutic strategy, particularly in the context of BRAF-negative status and limited targeted treatment options. The presence of symptomatic visceral metastases is associated with poorer outcomes and often necessitates a multidisciplinary approach, including systemic therapy, supportive care, and close monitoring for complications such as gastrointestinal bleeding.
Conclusion
This case highlights an uncommon presentation of metastatic melanoma involving the stomach manifesting as gastrointestinal bleeding within a short interval after initial diagnosis. Gastrointestinal metastasis from melanoma is usually clinically silent and are more frequently detected at autopsy than in symptomatic patients. In our patient, endoscopic evaluation revealed amelanotic gastric lesions, which can pose a diagnostic challenge because they lack the characteristic pigmentation typically associated with melanoma. This case underscores the importance of maintaining a high index of suspicion and considering metastatic melanoma in the differential diagnosis of unexplained gastrointestinal bleeding in patients with a history of melanoma, even when endoscopic lesions appear nonpigmented. It also emphasizes the potential role of early endoscopic evaluation in patients with advanced melanoma, particularly when associated with iron deficiency anemia.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for Publication
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
AI Usage Statement
Generative AI was used to assist in language editing and clarity of this manuscript. The authors reviewed and took full responsibility for the final content.