
Abstract
Purpose:
We examined smoking and smoking cessation by sex assigned at birth and sexual orientation and gender identity (SOGI) among Hispanic/Latino adults.
Methods:
We used data from visit 1 (2008–2011), visit 2 (2014–2017), and visit 3 (2020–2024) of the Hispanic Community Health Study/Study of Latinos (HCHS/SOL). Our analysis focused on participants (N = 8847) who responded to SOGI questions at visit 3 and provided data on smoking measures at visits 1–3. Accounting for survey design and weights, we estimated logistic regression models of associations between SOGI status and current smoking at visit 1. We also estimated discrete time models of associations between SOGI status and smoking cessation by visit 3.
Results:
In analyses adjusted for sociodemographic covariates, male sexual and gender minority (SGM) participants had 40% reduced odds of smoking compared with male cisgender heterosexual participants (95% confidence interval [CI]: 0.36–1.00). However, female SGM participants had 2.72 (95% CI: 1.92–3.86) times the odds of smoking compared with female cisgender heterosexual participants. In contrast, we found no significant differences in smoking cessation between male SGM and cisgender heterosexual participants or between female SGM and cisgender heterosexual participants. For all HCHS/SOL participants, the likelihood of cessation increased over time and increased the most for those with more than a high school education.
Conclusion:
SGM females had high rates of current smoking and were as unlikely to quit as other participants. Thus, prevention of smoking initiation is critical. Programs to prevent smoking among Hispanic/Latino individuals should be designed with consideration of differences by sex and SOGI status.
Introduction
According to the Surgeon General, one-fifth of annual deaths in the United States are attributable to cigarette smoking or secondhand exposure. 1 Many studies have found that sexual and gender minority (SGM) individuals exhibit a higher prevalence of tobacco use compared with their heterosexual and cisgender counterparts.1–8 SGM populations are exposed to more targeted tobacco advertising and are more likely to use tobacco products, begin smoking at younger ages, and smoke more heavily than cisgender heterosexual populations.1,2,9–11 SGM individuals are also less likely than cisgender heterosexual individuals to quit smoking.5–7,11 As a result, they face an elevated risk of developing cardiovascular disease and smoking-related cancers.1,12 Smoking cessation is key to reducing tobacco-related health harms.
The minority stress model links elevated health risk behaviors in SGM populations to chronic stress from stigma and discrimination.8,9,13–17 These stressors intersect with other axes of inequality, such as race, ethnicity, and socioeconomic status. 16 A growing body of research has examined tobacco use patterns at the intersection of sexual orientation, assigned sex at birth (hereafter, sex), and race/ethnicity.8,18–20 Evidence consistently shows greater tobacco use among sexual minority women compared with their heterosexual counterparts, with pronounced disparities between sexual minority and heterosexual women within the same racial and ethnic minority groups.18,19 In contrast, differences in tobacco use by sexual orientation and ethnoracial groups are less pronounced among men.2,8,18–20
Past research on smoking among Hispanic/Latino SGM populations often overlooked the importance of heterogeneity within these communities. 21 Well-established factors, such as nativity and Hispanic background, significantly influence patterns of tobacco use among Hispanic/Latino populations.22–27 For example, US-born Hispanic/Latina women who are more acculturated are more likely to smoke and less likely to quit compared with women born abroad.22–27 Individuals with Cuban or Puerto Rican backgrounds are more likely to smoke and less likely to quit than individuals with other Hispanic/Latino backgrounds. 25 Likewise, heterogeneity in sexual orientation and gender identity (SOGI) is important for understanding smoking behaviors.2,8
In sum, smoking is a major cause of death, with notable disparities by SOGI, ethnicity, nativity, and Hispanic background. Given the importance of preventing tobacco-related harms, it is essential to understand smoking behaviors across intersections of these identities to develop appropriate interventions. However, we found no studies examining smoking cessation among Hispanic/Latino populations by SOGI status. In this longitudinal cohort study, we examined smoking prevalence and cessation over time by sex and SOGI status among Hispanic/Latino adults, accounting for nativity and background.
Methods
We used data from the Hispanic Community Health Study/Study of Latinos (HCHS/SOL), a longitudinal cohort study of Hispanic/Latino adults residing in four US metropolitan areas—Bronx, NY; Chicago, IL; Miami, FL; and San Diego, CA. Across three in-person clinic visits—visit 1 (V1; 2008–2011), visit 2 (V2; 2014–2017), and visit 3 (V3; 2020–2024)—HCHS/SOL collected detailed data about health and behaviors among Hispanic/Latino adults who spanned ages 18–76 at enrollment (N = 16,415).1,2 Details about the study design, sampling method, eligibility, and examination procedures have been published previously.28,29
Ethical review
The study was approved by the University of North Carolina Institutional Review Board in Chapel Hill, North Carolina, on July 22, 2020 (Study #: 20-1496). All participants completed written informed consent to participate in the study and for the use of their data by study investigators and their collaborators. All data used for this analysis were deidentified. This research study was completed in accordance with the Declaration of Helsinki as revised in 2013.
Analytic sample
This analysis used data from all three visits of HCHS/SOL. At V3, the ancillary study of Stress, Gender, and Minority status in the Study of Latinos (SGM SOL) collected additional SOGI data among those participants who completed the in-person exam (N = 9090). 30 This sample included individuals who responded to SOGI questions and provided data on smoking measures. We excluded 215 participants due to incomplete SOGI responses and an additional 28 participants because of missing data on dependent variables. The final analytic sample consisted of 8847 participants.
Measures
Current smoking at V1 classified respondents as current smokers (1 = yes) if they endorsed having ever smoked at least 100 cigarettes in their life and reported currently smoking “daily” or “not daily” at visit 1. The reference group (0 = no) included individuals who had never smoked 100 or more cigarettes or were former smokers at visit 1. Because we were interested in the likelihood of smoking cessation by visit 3, we also defined current smokers at V2 and V3. Respondents were also asked if they lived with someone who smokes.
Cessation status was a time-varying variable that identified whether individuals who were current smokers at V1 or V2 reported being former smokers at a subsequent visit (=1). Specifically, participants who were current smokers at V1 and reported being former smokers at both V2 and V3 were classified as having quit by V2. Similarly, those who were current smokers at V1 or V2 and reported being former smokers by V3 were classified as having quit by V3. The reference group (=0) for cessation analyses included individuals who remained current smokers across all three visits.
Sex and SOGI. Participants were categorized as assigned female (hereafter, female) or male (hereafter, male) at birth. They were categorized as SGM individuals if they reported same sex attraction; identified their sexual orientation identity as gay/lesbian, bisexual, or some other identity; reported having had a same-sex romantic or sexual partner; or were transgender or gender diverse (TGD). Individuals who were TGD included participants whose sex differed from their gender identity; who were intersex or had a difference of sex development; or who identified as transgender or gender nonbinary.
People who selected “some other identity” for their gender identity were included in the TGD group since write-in responses indicated that they were gender diverse. All participants were asked the age at which they first identified with their current gender. Participants who reported being same-sex attracted were asked the age at which they first felt attraction to someone of the same sex. All except 2 SGM participants met our definitions for SGM prior to visit 1 data collection.
For multivariable analyses, we created a four-category variable classifying participants by both sex assigned at birth and SOGI status (SGM male, cisgender heterosexual male, SGM female, cisgender heterosexual female). Sexual orientation identity was a variable indicating whether individuals identified as straight/heterosexual, gay/lesbian, bisexual, or some other identity. The complete set of SOGI questions is available in the Appendix.31,32
Control variables. Adjusted analyses accounted for covariates known to be associated with tobacco use and cessation. These covariates included age assessed in years and nativity (i.e., born in US 50 states/DC or a US territory, hereafter US- vs. foreign-born), and the following variables are categorized as presented in Table 1: Hispanic background, study site, educational attainment, household income, number of household members, health insurance coverage, and marital status.
Demographic Characteristics at Visit 1 by Sex and Sexual Orientation and Gender Identity, Among Visit 3 In-Person Exam Participants in the Hispanic Community Health Study/Study of Latinos
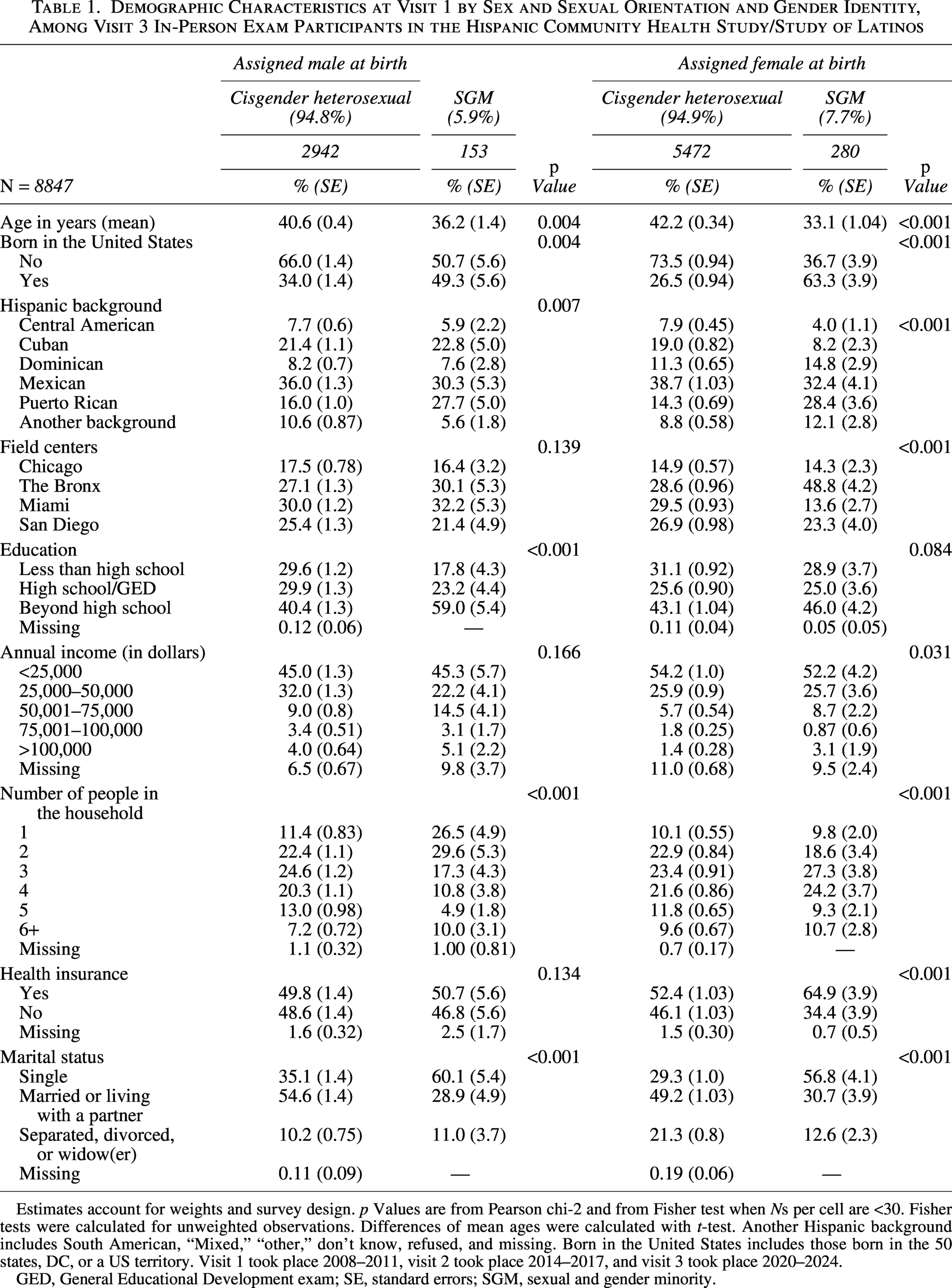
Estimates account for weights and survey design. p Values are from Pearson chi-2 and from Fisher test when Ns per cell are <30. Fisher tests were calculated for unweighted observations. Differences of mean ages were calculated with t-test. Another Hispanic background includes South American, “Mixed,” “other,” don’t know, refused, and missing. Born in the United States includes those born in the 50 states, DC, or a US territory. Visit 1 took place 2008–2011, visit 2 took place 2014–2017, and visit 3 took place 2020–2024.
GED, General Educational Development exam; SE, standard errors; SGM, sexual and gender minority.
For the analysis of smoking cessation, time-varying variables were coded by visit. To account for inflation across visits, we calculated a Consumer Price Index (CPI)-adjusted income by applying the ratio of the annual CPI for the interview year to the CPI for the baseline year (2008). 33 The full set of questions for visits 1 and 2 is available on the National Heart, Lung, and Blood Institute (NHLBI) website. 31 Questions for visit 3 are available on the HCHS/SOL website. 32
Analyses
First, we estimated differences in the distribution of sociodemographic characteristics and the prevalence of current smoking and cessation by assigned sex and SOGI (SGM or cisgender heterosexual) status. Second, we estimated logistic regression models predicting current smoking status as reported in V1 and calculated adjusted odds ratios (aORs) and 95% confidence intervals (CIs) for each category of assigned sex and SOGI status. The initial analysis (Model 1) included only assigned sex-SOGI status and age as independent variables. Model 2 added nativity (US- vs. foreign-born), Hispanic background, and study site (Bronx, Chicago, Miami, San Diego). Model 3 added the remaining sociodemographic characteristics. Finally, we estimated aORs and 95% CIs for cessation among current smokers using nonparametric discrete-time logistic event history models. 34
In event history models, the unit of analysis was person-visits (N = 3007). The models included two periods, V2 and V3, and observations of those who quit by V2 were excluded for V3. As described above, three event history models were estimated, adding in each group of covariates. We also tested and found no support for a nonlinear effect of age on either outcome, current smoking, or cessation (models not shown).
In additional analyses, we described the prevalence of both outcomes stratified by SOGI status and sexual orientation identity. We examined the prevalence of ever smoking and the ratio of former smokers at V3 to ever smokers by assigned sex and SOGI status. Finally, we tested differences by assigned sex and SOGI status in two smoking-related characteristics: living with someone who smokes and, among current smokers, smoking daily or nondaily. These variables were excluded from multivariable analyses to avoid endogeneity. In all analyses, we incorporated the complex sampling design and sampling weights of the HCHS/SOL study. All analyses were conducted using Stata software, version 18 (StataCorp LLC, College Station, Texas). 35
Results
Descriptives
Participants included 6.8% who identified as SGM (n = 433); 7.7% of female and 5.9% of male participants were SGM (Table 1). Most participants were heterosexual (93.9%, n = 8444), with 2.1% (n = 140) identifying as gay/lesbian, 3.5% (n = 214) as bisexual, and 0.1% (n = 49) as “some other identity.” Thirty SGM participants were heterosexual with a gender minority identity. Among SGM males, 7.3% were heterosexual, 44.6% gay/lesbian, 42.1% bisexual, and 6.4% some other sexual orientation identity. Among SGM females, 6.6% were heterosexual, 22.0% gay/lesbian, 59.1% bisexual, and 12.2% were some other identity.
Analyses by assigned sex and SOGI status showed that SGM participants differed from their cisgender heterosexual counterparts in most sociodemographic characteristics. SGM individuals were younger (mean age male = 36.2 vs. 40.6 years; female = 33.1 vs. 42.2 years), more likely to have been born in the United States (male = 49.3% vs. 34.0%; female = 63.3% vs. 26.5%), and to be single (male = 60.1% vs. 35.1%; female = 56.8% vs. 29.3%). SGM respondents were more likely to be of Puerto Rican descent (male = 27.7% vs. 16.0% and female = 28.4% vs. 14.3%). Male SGM (vs. cisgender heterosexual) participants were more likely to have completed education beyond high school and live in households with fewer dependents. Female SGM (vs. cisgender heterosexual) participants were more likely to have a household income >$50,000, live in households with a greater number of dependents, and have health insurance.
Outcomes
A total of 1737 current smokers were identified at V1 or V2. Among current smokers, 223 were identified only at V2. Bivariate analyses (Table 2) identified differences in current smoking at V1 or V2.
Unadjusted Prevalence of Current Smoking at Visits 1 or 2 and of Cessation Status at Visits 2 or 3 Among Current Smokers Among Visit 3 In-Person Exam Participants
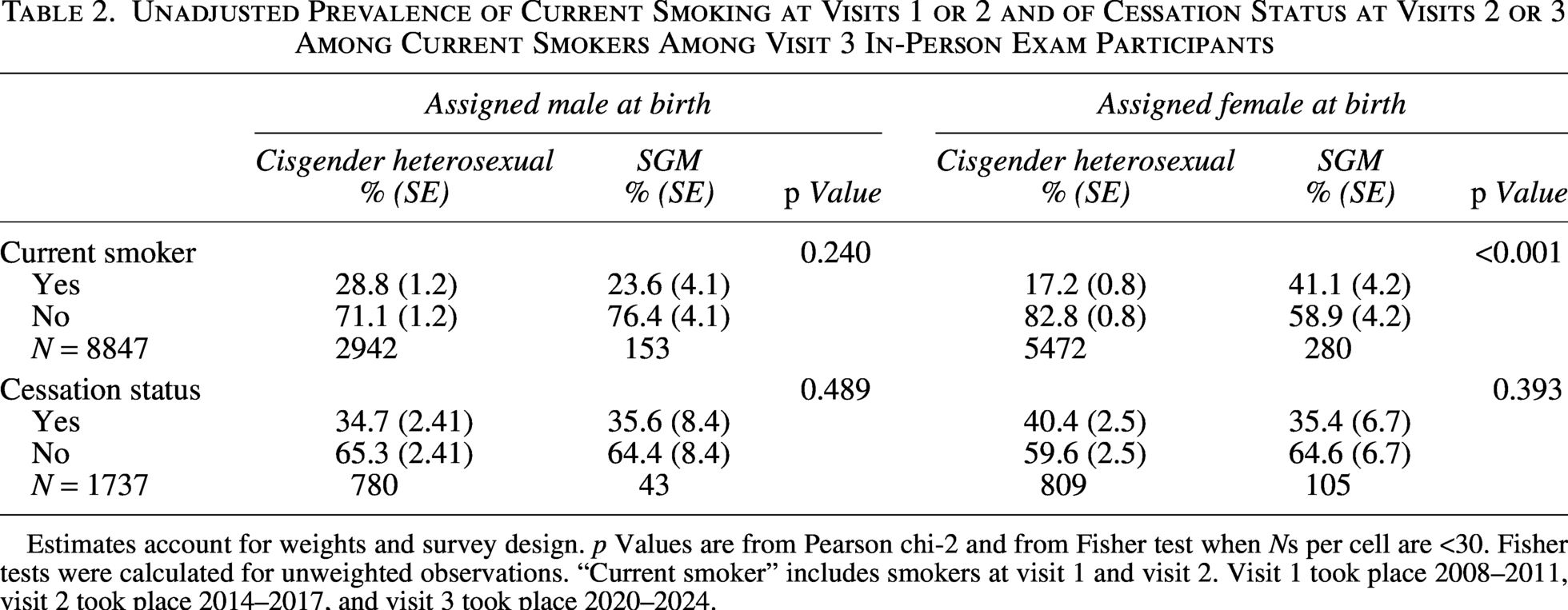
Estimates account for weights and survey design. p Values are from Pearson chi-2 and from Fisher test when Ns per cell are <30. Fisher tests were calculated for unweighted observations. “Current smoker” includes smokers at visit 1 and visit 2. Visit 1 took place 2008–2011, visit 2 took place 2014–2017, and visit 3 took place 2020–2024.
Approximately two-fifths (41.1%) of female SGM participants reported smoking at V1 or V2, more than twice the smoking prevalence of female cisgender heterosexual participants (41.1% vs. 17.2%, p < 0.001) and much higher than the prevalences observed for male SGM and cisgender heterosexual participants. Although the proportion of male SGM participants who were current smokers was lower compared with male cisgender heterosexual participants, this difference was not statistically significant (23.6% vs. 28.8%; p = 0.240). Cessation prevalences were similar for SGM and cisgender heterosexual participants, whether female or male. Over one-third of current smokers at V1 or V2 had quit by V3, with the highest prevalence of cessation observed among female cisgender heterosexual participants (40.4%).
Relationship between sex and SOGI status and smoking at Visit 1
In age-adjusted analyses (Table 3, Model 1), female SGM participants had 1.66 times the odds of smoking compared with male cisgender heterosexual participants (aOR 1.66, 95% CI: 1.16–2.36). Female cisgender heterosexual participants had 47% lower odds of smoking compared with male cisgender heterosexual participants (aOR 0.53, 95% CI: 0.45–0.62). No significant differences were found by SOGI status among male participants.
Logistic Regressions of Current Smoking at Visit 1, Among Visit 3 In-Person Exam Participants in the Hispanic Community Health Study/Study of Latinos
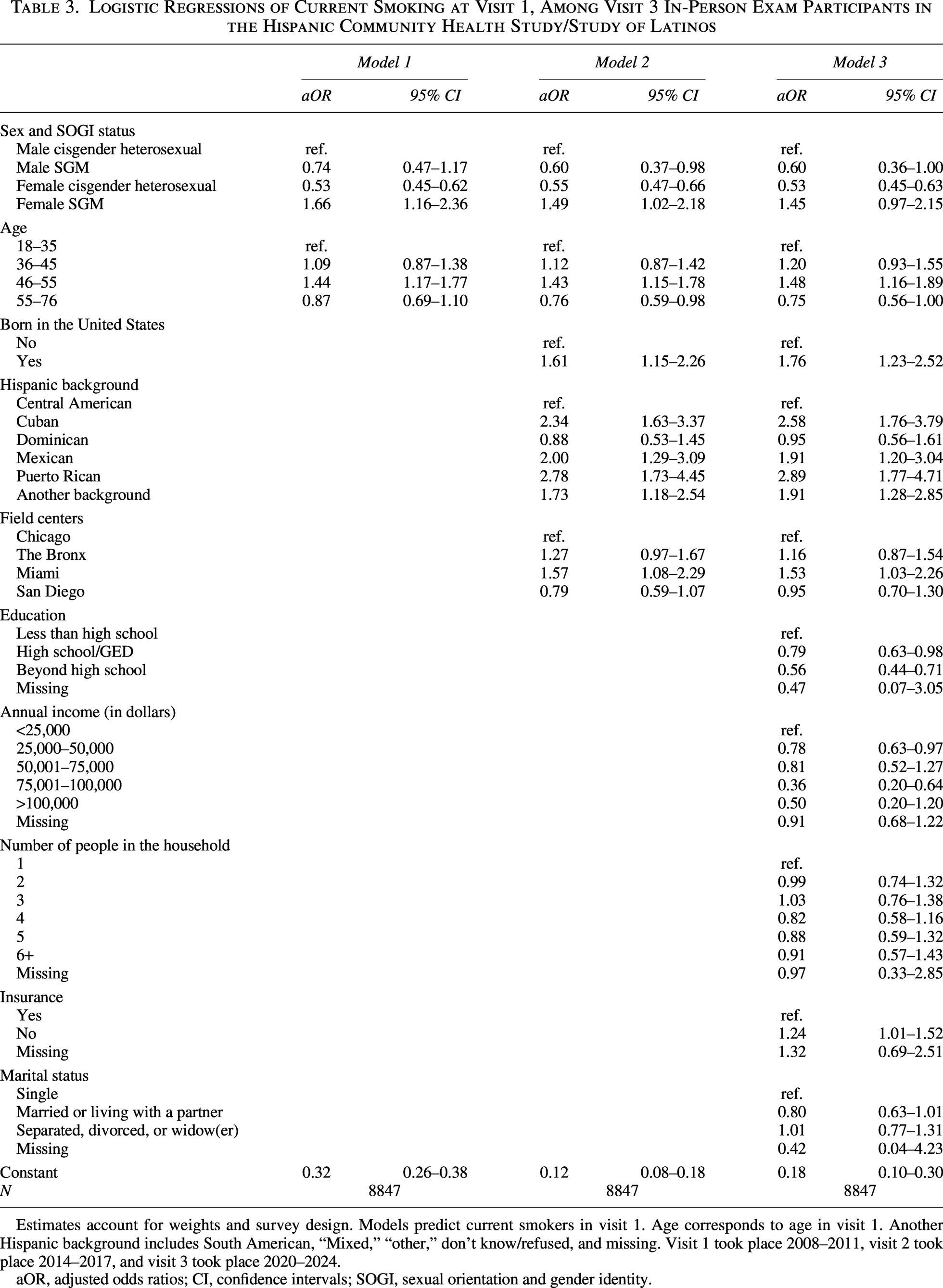
Estimates account for weights and survey design. Models predict current smokers in visit 1. Age corresponds to age in visit 1. Another Hispanic background includes South American, “Mixed,” “other,” don’t know/refused, and missing. Visit 1 took place 2008–2011, visit 2 took place 2014–2017, and visit 3 took place 2020–2024.
aOR, adjusted odds ratios; CI, confidence intervals; SOGI, sexual orientation and gender identity.
The addition of nativity, Hispanic background, and site (Table 3, Model 2) to the model attenuated the elevated odds of smoking among female SGM individuals (aOR 1.49, 95% CI: 1.02–2.18) and did not change results for female cisgender heterosexual participants (aOR 0.55, 95% CI: 0.47–0.66). However, male SGM participants had significantly reduced odds of smoking compared with male cisgender heterosexual participants (aOR 0.60, 95% CI: 0.37–0.98) in Model 2. The fully adjusted model results (Table 3, Model 3) were similar to Model 2, with a slight attenuation of the associations for female SGM participants compared with male cisgender heterosexual participants (aOR 1.45, 95% CI: 0.97–2.15). Among females, SGM participants were 2.72 times more likely to smoke compared with cisgender heterosexual participants (aOR 2.72, 95% CI: 1.92–3.86; data not shown).
Being US-born (aOR 1.76, 95% CI: 1.23–2.52) versus foreign-born and not having health insurance coverage (aOR 1.24, 95% CI: 1.01–1.52) were associated with higher odds of smoking. Most Hispanic backgrounds were associated with higher odds of smoking than Central American (ref), with the highest odds for Cuban (aOR 2.58, 95% CI: 1.76–3.79) and Puerto Rican (aOR 2.89, 95% CI: 1.77–4.71) heritages. Higher educational attainment, living with a partner, and higher income were all associated with reduced odds of smoking.
Relationship between sex and SOGI status and smoking cessation by visit 3
Results from the discrete-time logistic regression models adjusted only for age (Table 4, Model 1) demonstrate that female cisgender heterosexual participants were more likely to quit (aOR 1.25, 95% CI: 0.98–1.59, p < 0.10) compared with male cisgender heterosexual participants. However, this trend was not statistically significant. There were no significant differences in cessation at V3 by assigned sex and SOGI status.
Odds Ratios from Discrete-Time Models of Cessation at Visits 2 or 3, Among Participants in Visit 3 in the Hispanic Community Health Study/Study of Latinos
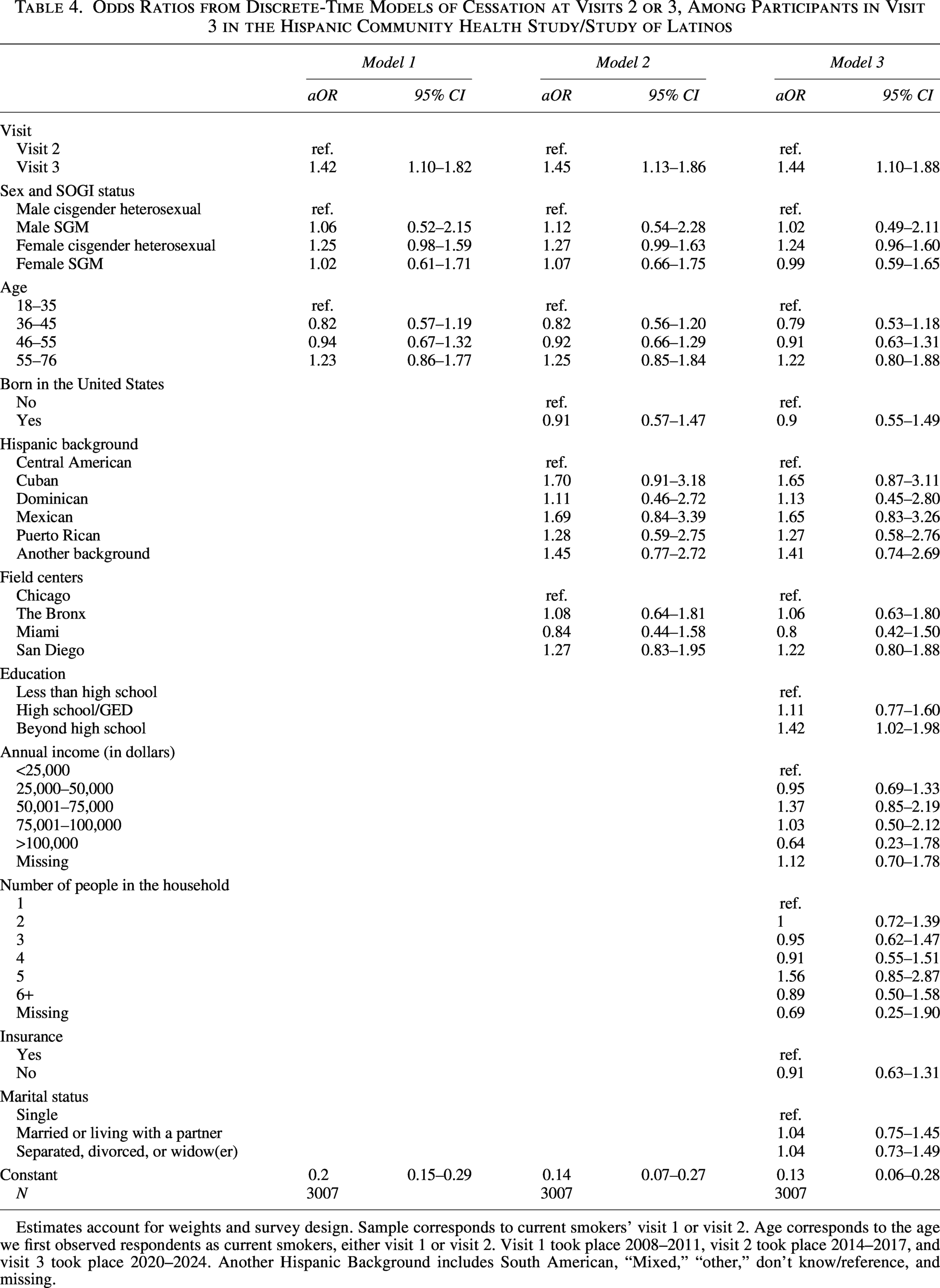
Estimates account for weights and survey design. Sample corresponds to current smokers’ visit 1 or visit 2. Age corresponds to the age we first observed respondents as current smokers, either visit 1 or visit 2. Visit 1 took place 2008–2011, visit 2 took place 2014–2017, and visit 3 took place 2020–2024. Another Hispanic Background includes South American, “Mixed,” “other,” don’t know/reference, and missing.
Results were similar in models adjusted for nativity, Hispanic background, study site (Model 2) and socioeconomic characteristics (Model 3). In Model 3, female SGM participants were less likely to quit compared with female cisgender heterosexual participants. However, the difference was not significant (aOR 0.69, 95% CI: 0.41–1.14; data not shown). In Model 3, the odds of quitting were significantly higher at V3 than V2 (aOR 1.44, 95% CI: 1.10–1.88). Participants who completed education beyond high school had higher odds of quitting than those with less than a high school education (aOR 1.42, 95% CI: 1.02–1.98). No other covariates were significantly associated with cessation.
Additional analysis
In additional analyses, SGM respondents were more likely to be current smokers (33.8% vs. 22.9%) and equally likely to quit compared with cisgender heterosexual respondents (35.5% vs. 36.9%) (Table 5). Small sample sizes limited our ability to conduct analyses by sex and sexual orientation identity. However, analyses by sexual orientation identity alone revealed a higher prevalence of current smoking among gay/lesbian respondents compared with heterosexual respondents (37.9% vs. 22.9%) and bisexual respondents (34.1%). We found no differences in cessation prevalences by sexual orientation identity.
Unadjusted Prevalence of Current Smoking at Visits 1 or 2 and of Cessation Status at Visits 2 or 3 Among Current Smokers Among Visit 3 In-Person Exam Participants
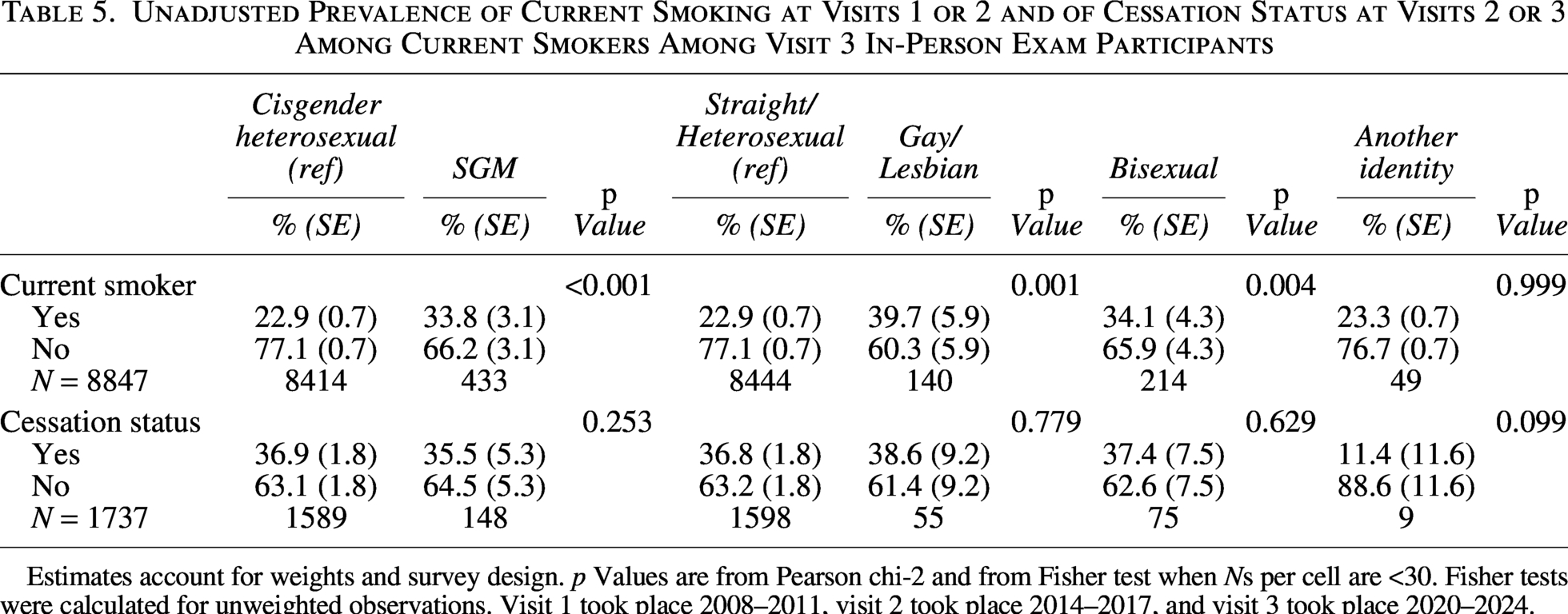
Estimates account for weights and survey design. p Values are from Pearson chi-2 and from Fisher test when Ns per cell are <30. Fisher tests were calculated for unweighted observations. Visit 1 took place 2008–2011, visit 2 took place 2014–2017, and visit 3 took place 2020–2024.
Female SGM participants were more likely to have ever smoked compared with female cisgender heterosexual participants (58.6% vs. 32.7%) (Table 6). We observed no differences in ever smoking by SOGI status among male participants nor in cessation status across groups. Among female participants, we found that SGM respondents were more likely to live with someone who smokes compared with cisgender heterosexual respondents (36.7% vs. 20.3%) (Table 7). Female cisgender heterosexual participants were more likely to be daily smokers (59.2% vs. 52.8%) than female SGM participants, although the difference did not reach statistical significance. Among male respondents, prevalence of daily smoking or living with someone who smokes did not differ significantly by SOGI status.
Unadjusted Prevalence of Ever Smoker and Rates of Cessation by Visit 3
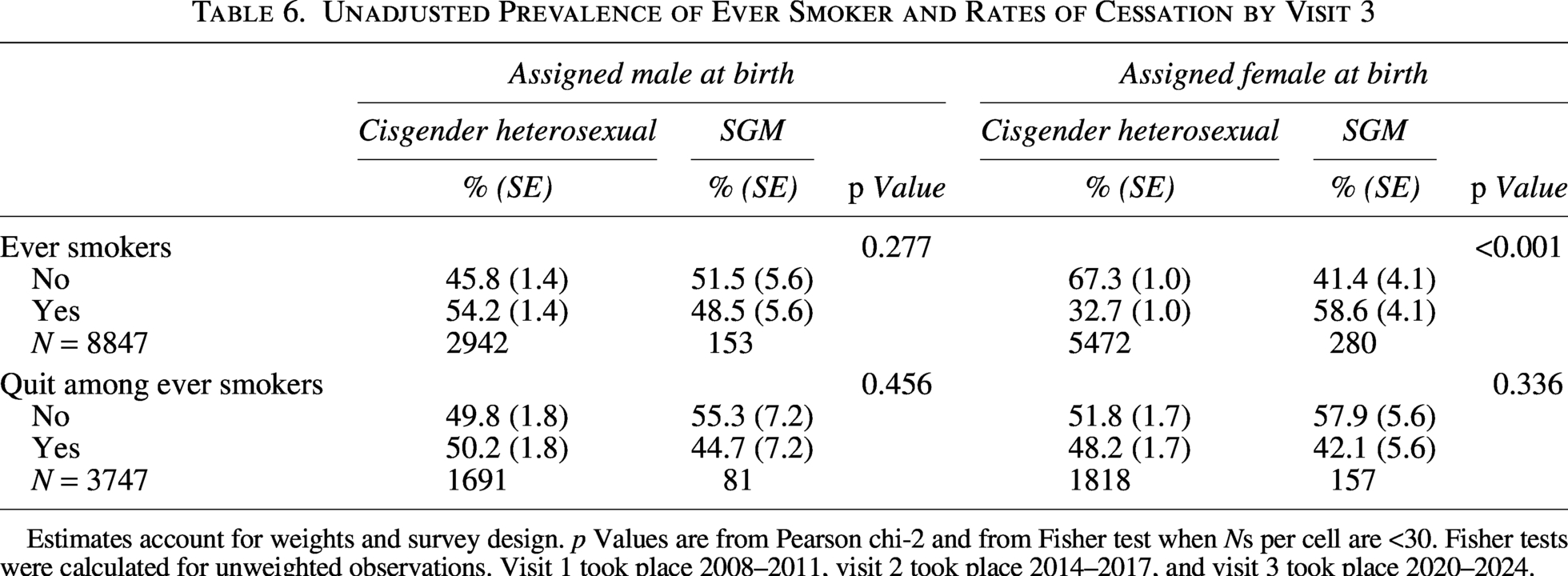
Estimates account for weights and survey design. p Values are from Pearson chi-2 and from Fisher test when Ns per cell are <30. Fisher tests were calculated for unweighted observations. Visit 1 took place 2008–2011, visit 2 took place 2014–2017, and visit 3 took place 2020–2024.
Unadjusted Prevalence of Lives with Someone Who Smokes and Daily Smoker Among Current Smokers at Visits 1 or 2 by Visit 3
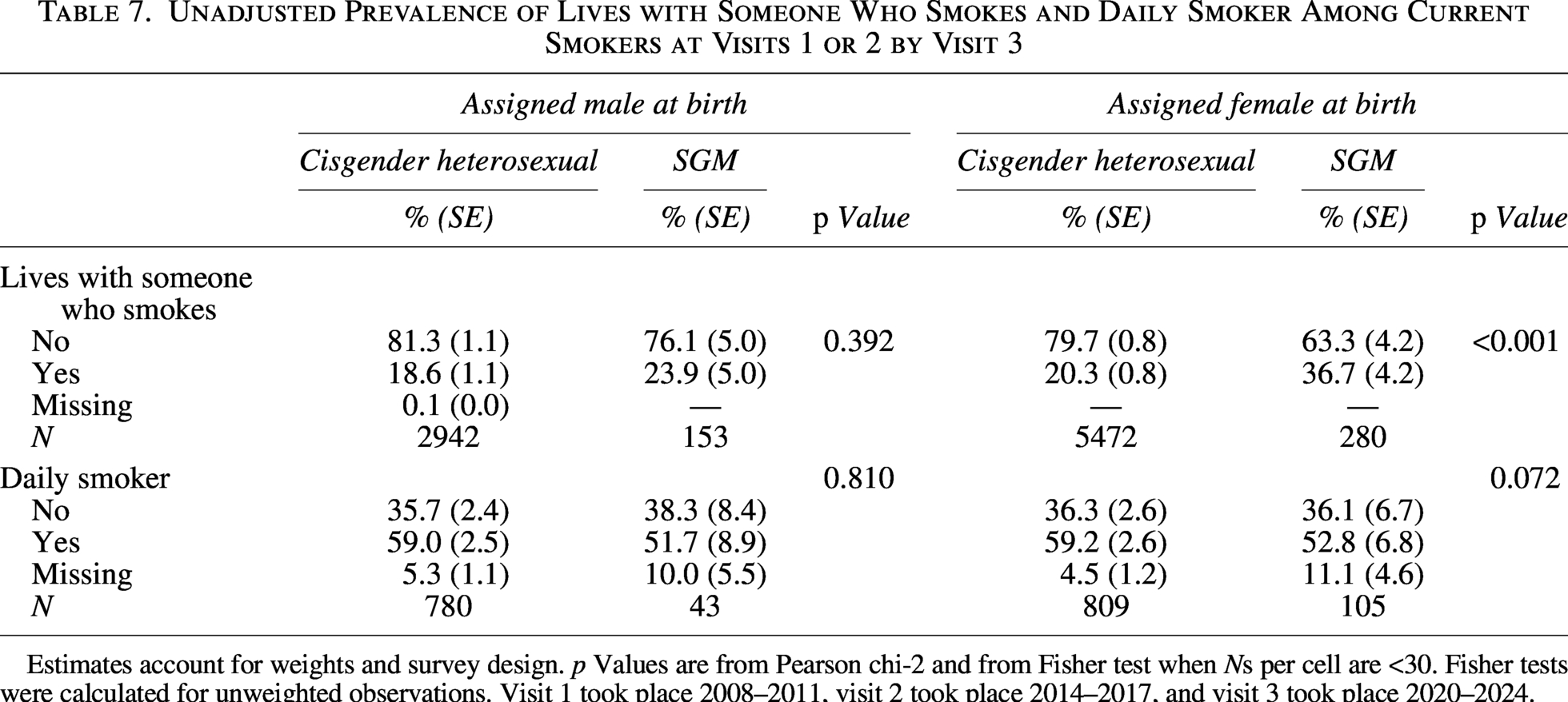
Estimates account for weights and survey design. p Values are from Pearson chi-2 and from Fisher test when Ns per cell are <30. Fisher tests were calculated for unweighted observations. Visit 1 took place 2008–2011, visit 2 took place 2014–2017, and visit 3 took place 2020–2024.
Discussion
This study of cigarette smoking and cessation examined differences by assigned sex and SOGI status among Hispanic/Latino adults. Female SGM participants were more likely to be current smokers than their cisgender heterosexual counterparts and both SGM and cisgender heterosexual male participants. Notably, female SGM (vs. cisgender heterosexual) participants were also more likely to live with someone who smokes.
Analyses adjusting for potential confounders identified a nuanced pattern in which female SGM participants were more likely, but male SGM participants were less likely, than male cisgender heterosexual participants to be current smokers. Adjusted models found a lower likelihood of smoking among SGM (vs. cisgender heterosexual) male participants. The lower odds of smoking observed among male SGM participants in fully adjusted models may reflect underlying differences in smoking behaviors and SGM identity by nativity and Hispanic background. Nativity and Hispanic/Latino background remained significant in all adjusted models. We found no differences in smoking cessation over time by assigned sex and SOGI status.
These findings align with existing literature on sexual orientation-related disparities in tobacco use.8,18–20 Three recent studies based on nationally representative data reported few to no significant differences in tobacco use between Hispanic/Latino sexual minority and heterosexual men.8,19,21 These studies also found significantly elevated smoking among Hispanic/Latino sexual minority women.
Several factors may explain the higher smoking prevalence among female SGM Hispanic/Latino individuals in our study. According to the minority stress model, they may experience compounded stressors based on gender (e.g., sexism) as well as anti-SGM stigma and discrimination, which may be exacerbated by racism, xenophobia, and immigration-related stress.13,17,36–39 Extant literature suggests that male SGM Hispanic/Latino individuals may have greater access to community ties and resilience strategies that buffer the adverse health impacts of stress.37,40 In addition, female SGM participants were more likely to live with someone who smokes, which may contribute to their higher smoking prevalence, given the known relationship between living with a smoker and both greater smoking uptake and lower cessation. 41
Results of the multivariable analyses are consistent with prior research indicating that disparities in tobacco use by SOGI status are not fully explained by socioeconomic or demographic characteristics.2,4,8,18,19 However, these studies did not account for heterogeneity within Hispanic/Latino populations. The persistent significance of nativity and Hispanic/Latino background, as well as their role in attenuating the association between sex and SOGI status and smoking in our multivariable models, underscore the importance of considering the diversity within Hispanic/Latino populations when assessing and addressing tobacco use.
Likelihood of smoking cessation did not vary by assigned sex or SOGI status. This indicates that SOGI-related disparities in smoking may persist over many years. The lack of association between cessation and sociodemographic factors aligns with prior research.24,25
Other factors may shape the smoking cessation experience. For example, Hispanic/Latino individuals are more likely to attempt quitting but are less likely to receive cessation advice or use pharmacological treatments compared with non-Hispanic White individuals. 42 Similarly, SGM individuals are equally or more motivated to quit smoking but face economic, normative, and psychological barriers to accessing effective cessation treatments.7,43,44 These findings highlight the need for effective cessation interventions for Hispanic/Latino individuals, especially those who are female and SGM. Research is needed on the efficacy of standard versus culturally tailored interventions for this population.
Limitations
This study has some limitations. First, we were unable to include tobacco products beyond cigarettes, such as Electronic Nicotine Delivery Systems (i.e., e-cigarettes). Although most Hispanic/Latino tobacco users consume cigarettes exclusively, sexual minority individuals—particularly women—are more likely to use and be exposed to advertising of these products.3,5 Thus, we may have underestimated tobacco use among study participants.
Due to the limited number of SGM participants in the dataset, we also could not conduct more detailed analyses by sexual orientation or gender identity. Prior literature indicates that bisexual women face unique disparities in tobacco use. 45 Future studies with larger numbers of SGM participants are needed to advance a more nuanced understanding of smoking behaviors by sex and sexual orientation among SGM Hispanic/Latino populations. Despite limitations, this study contributes to the literature by examining smoking and cessation over a 15-year period in a large population-based sample of Hispanic/Latino adults, inclusive of specific data on nativity and Hispanic/Latino background.
Conclusion
The 2024 “Report of the Surgeon General” calls attention to persistent inequalities in tobacco use, including among SGM communities. The report notes that “Tobacco-related health disparities are a social injustice, in addition to an economic and health burden” (p. 2) and highlights the urgency to address “experiences of racism, discrimination, and targeted marketing by the tobacco industry.” 1 Programs to prevent smoking among Hispanic/Latino individuals should also be designed with consideration of differences by sex and SOGI status, as well as the heterogeneous experiences by nativity and background.
Authors’ Contributions
C.H.-A.: Methodology (lead), writing the original draft, and editing. T.C.P.: Funding acquisition and conceptualization; methodology, writing the original draft and editing; and data curation and project administration. A.H.: Data curation, project administration, reviewing, and editing. A.P.: Data curation, project administration, reviewing, and editing. A.T.: Reviewing and editing. M.D.: Data curation, project administration, reviewing, and editing. D.J.L.: Reviewing and editing. N.S.: Data curation, project administration, reviewing, and editing. K.M.P.: Funding acquisition and conceptualization; methodology, writing the original draft, and editing; data curation, and project administration.
Ethical Considerations
The study was approved by the University of North Carolina Institutional Review Board in Chapel Hill, North Carolina on July 22, 2020 (Study #: 20-1496). This research study was completed in accordance with the Declaration of Helsinki as revised in 2013.
Footnotes
Acknowledgments
Consent to Participate
All participants completed written informed consent to participate in the study and for the use of their data by study investigators and their collaborators.
Consent for Publication
Not applicable. This article does not contain any identifying data from an individual person (including individual details, images, or videos).
Data Availability
The data and computer code used for this analysis reside at the University of North Carolina—Chapel Hill. The HCHS/SOL fully supports data sharing for HCHS/SOL-approved article proposals with outside investigators. All data sharing is conducted in accordance with HCHS/SOL study and NIH policies and governed by a Data and Materials Distribution Agreement between UNC and the external institution, ensuring the confidentiality and privacy of HCHS/SOL participants and their families. Alternatively, deidentified HCHS/SOL data are publicly available at BioLINCC and dbGaP for the subset of the study cohort who authorized general use of their data at the time of informed consent. The questionnaires for each study visit in the HCHS/SOL are called “FORMS” by HCHS/SOL. All forms for visit 1 and visit 2 are publicly available at https://biolincc.nhlbi.nih.gov/studies/hchssol. They are titled (1) Forms—Baseline and (2) Forms—Visit 2. Forms for visit 3 have not yet been posted to the NHLBI data repository. However, these forms are available online by going to the HCHS/SOL website (![]() ), selecting the resources tab, then Materials/Procedures, and then the FORMS/QxQ tab. Then, indicate “data collection” in the Form type. The website is not public, but interested individuals can sign up for an account to view the forms. Codebooks with derived variables are listed under methods and guidelines.
), selecting the resources tab, then Materials/Procedures, and then the FORMS/QxQ tab. Then, indicate “data collection” in the Form type. The website is not public, but interested individuals can sign up for an account to view the forms. Codebooks with derived variables are listed under methods and guidelines.
Declaration of Conflicting Interest
T.C.P. serves on the editorial board of LGBT Health. All other authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Statement
Research reported in this publication was supported by the
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.