
Abstract
Background
MASLD (NAFLD) is the most common chronic hepatopathy and has a rising prevalence in PLWH, with etiological factors being interplay of HIV-specific with general ones.
Methods
We conducted a cross-sectional study (n = 93). Patients were assessed in an outpatient clinic in Poland (April-October 2021) using clinical, metabolic data, irisin, CK-18, adiponectin, and leptin. Noninvasive formulas were used to assess the MASLD risk biochemically.
Results
No statistically relevant differences in MASLD-related scores among different ART regimens were found, with weak correlations were found between CD4 count and NAFLD-LFS (R < .3), and ART duration with non-HDL-C (R = −.22) and NFS (R = .23). Lifetime weight amplitude showed relationship with biochemical MASLD-related formulas and hepatitis (P = .037); among the biomarkers, leptin exhibited several correlations, strongest with HSI (R = .56) and BMI (R = .53).
Conclusions
MASLD corresponded more with general than with ART-related factors. Leptin may value when evaluating MASLD risk.
Plain Language Title
Why People Living with HIV Develop Fatty Liver Disease, and Why Body Weight Matters More Than HIV Medications
Plain Language Summary
Fatty liver disease is becoming very common, both in general society and among people living with HIV. There are some reports suggesting that HIV medication may be an issue. In our study, we wanted to take look and check what actually plays the biggest role: the treatment itself or more everyday factors like weight changes, cholesterol, or blood sugar. We worked with 93 adults living with HIV who were treated for at least 2 years. None had hepatitis B or C. We asked about their lifestyle, checked standard lab tests, and measured some newer blood markers that may tell us something about liver health. What we found was pretty simple: the type of HIV meds people in our study group were taking did not seem to make much difference. Instead, the strongest hints came from things that have nothing to do with HIV. Big changes in body weight over the years were the main factor linked to signs of fatty liver. One of the newer markers we looked at, leptin, also stood out as a useful indicator that something might be going on with the liver. Overall, it seems that for people living with HIV, everyday metabolic health—especially long-term weight patterns—matters much more for the liver than the specific HIV regimen. It is another reminder that keeping weight steady and metabolism in check can go a long way. Of course, bigger and longer studies are still needed to be sure.
Keywords
Introduction
Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) in People Living with HIV (PLWH)
MASLD, recently renamed from nonalcoholic fatty liver disease (NAFLD) to underline its connection with metabolic syndrome (MetS)1,2 is the most prevalent chronic liver disease globally. 3
MASLD prevalence in PLWH ranges from 28.8% to 48%. 4 Its pathogenesis in PLWH is more complex due to additional factors, including gut-liver axis disruptions (microbiome alterations, intestinal permeability), 5 HIV-hepatocyte interactions, 6 and notably antiretroviral therapy (ART) and its duration. 7
While ART has significantly reduced HIV-related mortality, its potential contribution to hepatic complications, particularly MASLD, is a growing concern. Older agents were primarily associated with overt metabolic disturbances like lipodystrophy and mitochondrial damage.5,8,9 Contemporary regimens, especially integrase strand transfer inhibitors (InSTIs) and tenofovir alafenamide (TAF), have shown controversial associations with steatosis progression10–13 and weight gain in some studies. Others suggest potential protective effects of InSTIs14,15 or hepatic benefits from tenofovir disoproxil fumarate (TDF). 10 This dispute highlights the demand to clarify modern ART's specific consequences for liver health in PLWH.
Data regarding the prevalence of MASLD in Poland are scarce; however, it is estimated to be about 24%. 16 To our knowledge, there are no studies comprehensively assessing the prevalence of MASLD among PLWH in Poland.
MASLD Diagnostic Methods and Novel Biomarkers
Current consensus defines MASLD as hepatic steatosis with any cardiometabolic risk factor, 1 acknowledging potential combined etiologies. While liver biopsy remains the gold standard, noninvasive methods, including imaging and biochemical markers/formulas, are widely used17,18 and some are validated in PLWH. 19
To further differentiate Metabolic Dysfunction-Associated Steatohepatitis (MASH) from simple steatosis, novel biomarkers reflecting pathways in MASH development (apoptosis, oxidative stress, inflammation) have been proposed. 20 Among these: Irisin (IRS), an adipomyokine secreted by muscle, liver, and adipose tissue, promotes white adipose tissue “browning” and potentially improves metabolic profiles by increasing thermogenesis and energy expenditure, also influencing insulin resistance.21,22 Cytokeratin-18 (CK-18) is a hepatocyte intermediate filament protein released during cell death, making it a valuable marker elevated in MASH compared to simple steatosis. 18 Adiponectin (ADPN), produced by healthy adipose tissue, exhibits anti-inflammatory properties and enhances insulin sensitivity, with its levels typically decreasing in hypertrophic white adipose tissue. 23 Conversely, Leptin (LEP), a pleiotropic hormone primarily secreted by adipose tissue, increases with adipose tissue mass, and hyperleptinemia contributes to metabolic disorders like insulin resistance and cardiovascular disease. 24 ADPN has been suggested as an inverse marker for MASLD progression and fibrosis, while LEP is implicated as a predictor of MASLD in those with weight gain. 25
Aim of the Study
This study specifically investigated the estimated biochemical prevalence and risk factors of MASLD in a cohort of HIV-positive patients treated in Wrocław, Poland. It also assessed the value of various noninvasive biochemical formulas and novel biomarkers for MASLD diagnosis and characterization, considering both HIV-related and HIV-unrelated factors, including different ART regimens.
We hypothesized that MASLD risk in PLWH in a setting of guaranteed access to publicly funded, modern antiretroviral therapy and regular medical monitoring in a high-income country is primarily driven by traditional metabolic factors rather than ART-related characteristics, and that novel biomarkers, particularly leptin, are positively associated with noninvasive steatosis indices.
Methods
Study Design and Participants
This cross-sectional study was conducted at the Outpatient Clinic of the Department of Infectious Diseases, Liver Diseases and Acquired Immune Deficiencies at Wroclaw Medical University, which serves as a regional reference center for Lower Silesia. It investigated the prevalence, associated risk factors, and novel biomarkers of MASLD within a cohort of PLWH.
The cohort represents HIV-positive patients living in an urban population in a large (over 800,000 inhabitants) and well-developed metropolitan area with guaranteed access to publicly funded, modern antiretroviral therapy and regular medical monitoring.
This publication derives from a broader project examining metabolic aspects in PLWH, focusing exclusively on MASLD and its noninvasive biochemical assessment. Other metabolic outcomes and comparisons to healthy controls are reported elsewhere. The detailed methodology, including study design, patient recruitment, data collection, and statistical analysis, largely parallels with another publications deriving from this cohort and focusing on other aspects (MetS in PLWH, comparison with healthy controls).
We included confirmed HIV-infected patients, aged 18 to 65 years, treated with ART for at least 2 years, with no co-infection with hepatitis B or C virus (HBV/HCV). Patients were excluded if they had uncontrolled endocrine disorders, histologically confirmed chronic liver diseases (eg, alcoholic liver disease, autoimmune hepatitis), their complications (eg, decompensated liver failure), malignant tumors, pregnancy, or type 1 diabetes.
Patients with excessive alcohol consumption (>30 g/day for men and >20 g/day for women) were excluded. Moderate alcohol consumption below these thresholds was permitted. Competing causes of chronic liver disease were ruled out based on comprehensive longitudinal medical records. Specifically, viral hepatitis (HBV, HCV) was excluded via routine serological screening (HBsAg, anti-HCV) performed as part of standard HIV care. Patients with a history of autoimmune liver diseases, Wilson's disease, or hemochromatosis were also excluded.
From 2061 screened patients, 608 met initial inclusion criteria, with HBV/HCV coinfection being a common reason for exclusion. After applying detailed exclusion criteria, primarily due to advanced alcoholic liver disease, 392 patients were potentially eligible. Ultimately, 93 patients provided consent and were enrolled between April and October 2021. Recruitment was impacted by the COVID-19 pandemic, leading to a smaller final cohort than initially aimed for (150 patients), as many opted for teleconsultations. The patient selection process is detailed in Figure 1.

Patient group selection.
From 2061 screened patients, 608 met initial inclusion criteria, with HBV/HCV coinfection being a common reason for exclusion. After applying detailed exclusion criteria, primarily due to advanced alcoholic liver disease, 392 patients were potentially eligible. Ultimately, 93 patients provided consent and were enrolled between April and October 2021. Recruitment was impacted by the COVID-19 pandemic, leading to a smaller final cohort than initially aimed for (150 patients), as many opted for teleconsultations. The patient selection process is detailed in Figure 1.
The reporting of this study conforms to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement for cross-sectional studies 26 (Supllementary File 2).
Clinical and Biological Parameters
Comprehensive data were collected from each patient via a detailed questionnaire (Supplementary File 3), covering demographics (age, sex), anthropometric measures (height, current weight, 2-year weight change, lifetime maximum/minimum adult weight), lifestyle factors (weekly alcohol consumption, tobacco use, recreational drug use, physical activity), medication history, and diagnoses of chronic conditions, with particular attention to metabolic and liver diseases relevant to MASLD.
Physical activity was quantified based on patient reports, using an exploratory, internal scoring system. We assigned coefficients to different intensity levels: 0.25 for light activities (eg, strolling), 0.5 for moderate-intensity (eg, Nordic walking), 1 for more intense activities (eg, jogging, gym exercises), and 1.5 for high-intensity activities (eg, running, weight training, interval training). This simplified (non-validated) method was used to estimate relative physical activity intensity rather than precise metabolic equivalents (METs). Alcohol consumption was quantified by converting reported beverage types and volumes into standard drinks (10 g of pure ethanol). 27
Fasting venous blood samples (8-12 h fasting) were collected for a comprehensive laboratory analysis. Key parameters assessed included: HIV viremia, CD4 lymphocyte count, complete blood count with white blood cell differential, C-reactive protein (CRP), a full lipid panel (total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), non-high-density lipoprotein cholesterol (non-HDL-C), low-density lipoprotein cholesterol (LDL-C), triglycerides (TG)), carbohydrate metabolism markers (glycemia, glycated hemoglobin (HbA1c), insulin, homeostatic model assessment for insulin resistance (HOMA-IR)), liver function enzymes (alanine aminotransferase (ALT), aspartate transaminase (AST), gamma-glutamyltransferase (GGTP), alkaline phosphatase (ALP)), total protein, albumin, and total bilirubin. Additionally, novel biomarkers central to MASLD pathogenesis were measured: IRS, CK-18, ADPN, and LEP. These parameters were obtained with proper laboratory techniques.
Commercially available parameters were analyzed in a Polish Centre for Accreditation-accredited laboratory. Parameters not available through commercial laboratories in Poland were processed at Wroclaw Medical University Laboratory. The HIV viremia was measured with HIV-1 quantitative real-time nucleic acid test performed on a cobas® 4800 System (Roche Diagnostics GmbH, Mannheim, Germany). The CD4 cell count was measured using a Navios EX flow cytometer (Beckman Coulter). Adiponectin, leptin, and irisin were 2measured using enzyme-linked immunosorbent assay (ELISA) kits (BioVendor—Laboratorni medicina a.s., Brno, Czech Republic) according to the manufacturer's instructions. CK-18 was measured using an ELISA kit (Thermo Fisher Scientific Inc., Carlsbad, CA, USA). The complete blood count with a white blood smear was analysed using a Sysmex Analyzer (Sysmex Corporation, Japan). The CRP was measured with immunoturbidimetry using a cobas® analytical unit (Roche Diagnostics). The TC, HDL, LDL, TG, ALT, AST, GGTP, ALP, total protein, albumin, total bilirubin, glycemia and insulin were measures with spectrophotometry using a cobas® analytical unit (Roche Diagnostics).
Insulin resistance (IR) was calculated using the homeostatic model assessment (HOMA)-IR formula: ((fasting plasma insulin in mU/L) × (fasting plasma glucose in mmol/L)/22.5). 28
Information regarding HIV infection duration, nadir CD4 count, and past/current antiretroviral treatment regimens was meticulously extracted from patient medical records.
Crucially for MASLD assessment, several noninvasive biochemical formulas for steatosis and fibrosis were calculated based on collected survey and laboratory data. These included: Hepatic Steatosis Index (HSI), 29 Triglyceride and Glucose Index (TyG), 30 NAFLD-Liver Fat Score (NAFLD-LFS), 31 Fibrosis-4 Index (FIB-4), 32 and NAFLD Fibrosis Score (NFS). 33 The MACK-3 score (a blood test used to assess the risk of fibrotic MASH, integrating AST, glycemia, insulin, and CK-18) was computed via an online calculator, 34 as its full formula is not publicly available.
Specific cut-off values indicating high risk of steatosis were applied according to original validation studies. For the assessment of relationships between risk factors and liver health, we utilized continuous variables (Spearman's rank correlation) rather than categorical stratification to maximize statistical power in this sample size. Since these formulas were primarily validated in the general population, their application in PLWH serves as a surrogate marker for metabolic liver risk rather than a definitive diagnosis, and their performance in PLWH may differ due to HIV-related inflammation and ART effects.
We relied exclusively on these noninvasive biochemical scores, as access to advanced imaging (eg, elastography, MRI-PDFF) was severely restricted during the COVID-19 pandemic. Furthermore, performing invasive liver biopsy on asymptomatic patients for screening purposes was not ethically justified.
Consequently, the terms “MASLD” or “MASH” in this study refer to the high probability of the disease based on biochemical risk stratification.
Statistical Analysis
Continuous variables are summarized as median ± quartile deviation, and categorical variables as number and percentage. Statistical significance was set at P < .05, with marginal significance noted for .05 < P <.1.
Differences between groups were assessed using the U Mann-Whitney test (for 2 groups), the Kruskal-Wallis test (for more than 2 groups), or the chi-square test (for categorical variables), as appropriate. The relation between 2 parameters was assessed using correlation analysis, and Spearman correlation coefficients (R) were calculated.
For the specific objectives of this study, MASLD prevalence was determined based on the calculated noninvasive formulas (HSI, TyG, NAFLD-LFS). Associations between HIV-related (ART regimen, duration, Nadir CD4) and HIV-unrelated factors (clinico-anthropometric data, lifestyle) with MASLD diagnosis and severity, as indicated by biochemical formulas, were assessed using a Spearman rank correlation. The diagnostic utility and interrelationships of novel biomarkers (IRS, CK-18, ADPN, LEP) with established MASLD formulas and liver enzymes were also analyzed using a Spearman rank correlation.
6Statistical analysis was performed using the computer statistical software package Statistica Ver. 13.3. (TIBCO Software Inc.).
ART Regimen Grouping
For improved readability, abbreviations which occur for the first time in this paragraph are explained here:
PI—protease inhibitors; NNRTI—Non-Nucleoside Reverse Transcriptase Inhibitors; ABC—Abacavir; /r—Ritonavir (used as a booster); ELV—Elvitegravir; DTG—Dolutegravir.
Of the 93 enrolled patients, a diverse range of ART regimens were observed: InSTI/TAF (n = 50); InSTI/TDF (n = 4); PI/TAF (n = 28); PI/TDF (n = 1); NNRTI/TAF (n = 3); NNRTI/TDF (n = 5); InSTI/ABC (n = 1); and PI/r (n = 1).
Given the heterogeneous and uneven distribution of patients across these specific regimens, the cohort was subsequently categorized into broader groups for robust statistical analysis, particularly for evaluating their association with MASLD:
Comparison between Group 1: InSTI/TAF (n = 50) and Group 2: PI/TAF (n = 28). Comparison between particular regimens: Group 3: ELV/cob/FTC/TAF [InSTI/TAF] (n = 28) (termed “ELV/TAF”) versus Group 4: DTG/FTC/TAF [InSTI/TAF] (n = 15) (termed “DTG/TAF”) versus Group 5: DRV/cob/FTC/TAF [PI/TAF] (n = 28) (termed “DRV/TAF”). This comparison will be names also as “ELV-DTG-DRV” in further parts.
It is important to note that Group 2 (PI/TAF) and Group 5 (DRV/cob/FTC/TAF) are composed of the same individuals, as all patients in the PI/TAF category were specifically treated with DRV/cob/FTC/TAF.
Results
Cohort Characteristics and ART Regimen Groupings
The study cohort consisted of 93 patients and reflected HIV epidemiology of our region,35,36 typical for Central Europe. All patients were Caucasian, predominantly male (83%), and most infections were sexually acquired, mainly among men having sex with men. Age and gender distribution were generally comparable across the analyzed ART regimen groups. General cohort characteristics, including BMI, prevalence of MetS, smoking, and alcohol consumption, were largely consistent across groups. It is important to note that Lifetime Weight Amplitude (LWA) data were available for 76 out of 93 patients due to self-recall limitations.
Virological control was excellent, with only 1 patient showing significant viremia (and CD4 level of 388 cells/µL), while 14 had low-level viremia.37,38 Both nadir and current CD4 cell levels, along with total ART treatment duration, showed no significant differences across regimens.
A significant difference was observed only in the duration of the current regimen, with the PI/TAF group treated longer than the InSTI/TAF group (median 4.27 vs 3.92 years, P = .0187). Within ELV-DTG-DRV comparison, the ELV/TAF group had a significantly shorter current treatment duration compared to DTG/TAF and DRV/TAF (P < .02 for both).
Detailed characteristics are presented in Table 1.
Cohort and Groups Characteristics.
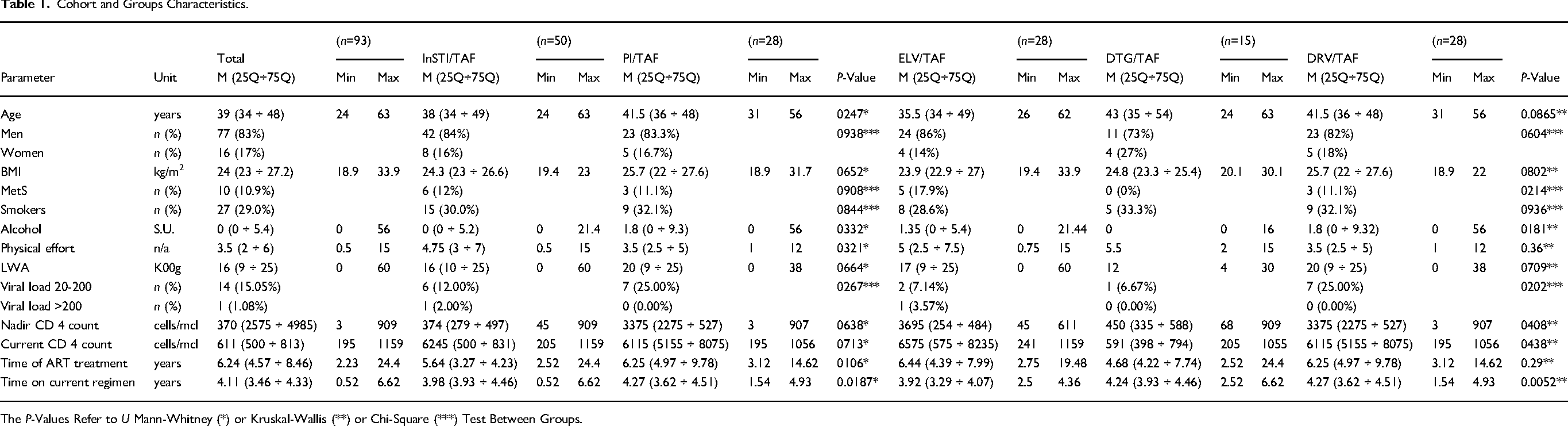
The P-Values Refer to U Mann-Whitney (*) or Kruskal-Wallis (**) or Chi-Square (***) Test Between Groups.
Lipid, Carbohydrate, and Liver Parameters by ART Regimen
The analysis of multiple parameters across different ART regimens groups revealed no significant differences in any of the calculated MASLD-related formulas (steatosic and fibrotic). This suggests that the type of current ART regimen did not have relevant impact MASLD prevalence or severity in this cohort. Albeit some minor or marginal differences were noted in isolated parameters (eg, (1) TC between DTG/TAF and DRV/TAF, P = .074; (2) higher GGTP in DRV/TAF versus DTG/TAF, P = .036; (3) marginal ADPN difference between InSTI/TAF and PI/TAF, P =.072), these were not indicative of broad regimen-specific effects on MASLD. Comprehensive data for lipid, carbohydrate, and liver parameters are provided in Tables 2 and 3 in the Supplemental Materials.
HIV-Related and HIV-Unrelated Factors—Associations With Hepatic Parameters and MASLD Formulas
We investigated the influence of HIV-related (nadir CD4 count, total ART treatment duration, current drug regimen treatment duration) and HIV-unrelated factors (BMI, carbohydrate/lipid parameters, LWA, smoking status) on 6 MASLD-related biochemical formulas: NAFLD-LFS, HSI, and TyG for steatosis; and FIB-4, NFS, and MACK-3 for fibrosis.
Overall, no single HIV-related factor demonstrated a significant impact on these MASLD formulas. Only a weak correlation was observed between nadir CD4 count and NAFLD-LFS (R < .3). Total ART duration showed only weak correlations with non-HDL-C (R = –.22) and NFS (R = .23). The current ART regimen duration did not significantly correlate with any metabolic parameters in the full cohort. Detailed correlation data for HIV-specific parameters are presented in Tables 4 and 5 in the Supplemental Materials.
Conversely, several HIV-unrelated factors showed significant correlations with MASLD formulas (Tables 6 and 7 in the Supplemental Materials). Notably, the TyG index correlated with all measured lipid parameters. An unexpected finding was a negative correlation between non-HDL-C levels and both FIB-4 and NFS scores. A combined quantitative analysis (summarized in Table 2) suggests that HIV-unrelated factors exert a more pronounced influence on MASLD development within this patient cohort. For this table, to minimize redundancy, only non-HDL-C was included from the lipid parameters (selected for its relevance to overall lipid-related health risk), while both HOMA-IR and HbA1c were retained to represent distinct facets of carbohydrate metabolism. The significant correlations are visually represented in Supplementary Figures 2 and 3 as scatter plots.
Impact of HIV-Related and HIV-Unrelated Factors on MASLD-Related Biochemical Formulas (P values in brackets).
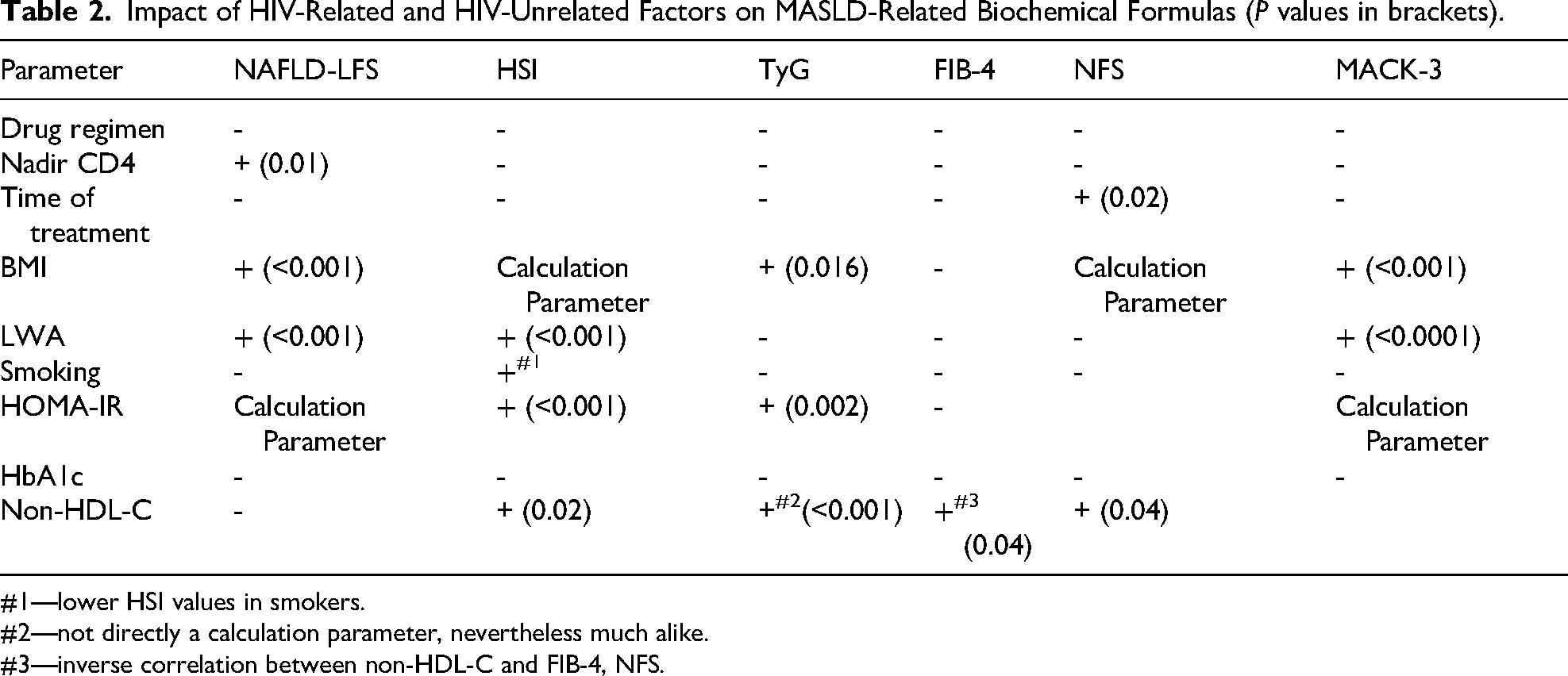
#1—lower HSI values in smokers.
#2—not directly a calculation parameter, nevertheless much alike.
#3—inverse correlation between non-HDL-C and FIB-4, NFS.
Factors Associated with Biochemical Hepatitis
Biochemical hepatitis (ALT or AST > 35 U/L) was significantly associated with LWA (P = .0375), which was the only statistically significant factor identified. Patients with hepatitis exhibited a higher median LWA (24.5 kg) compared to those without (14.5 kg). BMI and HbA1c showed only marginal associations (P = .079 and P = .065, respectively). Neither ART regimen nor smoking status was significantly associated. Detailed results are presented in Tables 9 to 11 (Supplemental Materials).
Correlation Between Metabolic Parameters, MASLD Formulas, and Novel Biomarkers
Correlation analyses were performed between metabolic parameters, MASLD formulas, and novel biomarkers (IRS, CK-18, ADPN, and LEP).
IRS and CK-18 generally showed weak correlations (IRS with HOMA-IR: R = .21; CK-18 with LWA and NAFLD-LFS: R = .27). In contrast, LEP demonstrated stronger and more widespread correlations with several key metabolic and MASLD-related parameters, including BMI, LWA, TC, HOMA-IR, HbA1c, NAFLD-LFS, and HSI. Its strongest correlations were with HSI (R = .56) and BMI (R = .53). ADPN showed a mix of positive and negative correlations with metabolic parameters and MASLD formulas. It correlated positively with HDL-C (R = .47) but negatively with triglycerides (R = −.24), HSI (R = −.21), and TyG (R = −.24). Its strongest positive association was with HDL-C (R = .47), while its strongest negative associations were with TG and TyG. All correlation coefficients are detailed in Supplementary Table 12.
Additional Analyses
A history of intravenous drug use showed only a marginal, nonclinically significant association with NFS (Supplementary Table 13). Given the study's predominantly male composition (83%), analysis of sex-related bias in MASLD parameters revealed significant differences in LEP and ADPN levels by sex (P ≤ .001 for both) (Supplementary Table 14).
Discussion
The emerging prevalence of MASLD and other metabolic complications among PLWH is a significant concern, however the exact pathophysiology remains complex and partially obscure. 39 A central part of the debate addresses the relative impact of HIV-related versus HIV-unrelated factors to MASLD development in this population.
Our study aimed to investigate this issue by comparing liver function, MASLD-related biochemical parameters, and key metabolic indicators across PLWH on various ART regimens. A key finding was the lack of significant association between most HIV-related factors and MASLD development, with only a weak correlation between nadir CD4 count and the NAFLD-LFS. This result offers a individual perspective—many data on ART's direct role in MASLD often reports associations with HIV-related factors, yet these findings are inconsistent. For instance, 1 meta-analysis indicated ART duration as the sole HIV-related MASLD risk factor, 7 while another suggested the involvement of both HIV-related and traditional factors. 40 A recent expert consensus also emphasized traditional risk factors like T2DM, male sex, and higher BMI without specifically implicating ART. 39
The “annual change” in BMI and weight, particularly Lifetime Weight Amplitude (LWA), emerged as a crucial factor, significantly associated with biochemical hepatitis in our cohort. This aligns with the understanding that PLWH, similar to the general population, are susceptible to the global MetS, with studies indicating differences in annual BMI gain between PLWH and uninfected individuals, though not consistently between specific ART regimens. 41 While several studies have highlighted the impact of newer ART agents, particularly TAF and INSTIs, on weight gain and hepatic steatosis,10–13,42 our findings suggest that HIV-unrelated metabolic factors exert a more pronounced influence on MASLD development than current ART regimen in this cohort. This underscores the importance of managing traditional metabolic risk factors in PLWH.
Regarding lifestyle factors, while some research links tobacco use to MASLD progression, 43 our study found smoking to be marginally associated with a slightly reduced Hepatic Steatosis Index (HSI). This finding should be interpreted cautiously due to the relatively small sample size of smokers (n = 27) in our cohort. We also acknowledge that PLWH who acquired HIV heterosexually may be more prone to advanced HIV disease, 44 potentially influencing metabolic outcomes. Furthermore, our explicit exclusion of individuals with HBV or HCV coinfection, common in intravenous drug users (IDUs), might introduce a selection bias regarding the overall liver health profile of our cohort.
Our investigation into novel adipokines and myokines revealed no significant differences in IRS, CK-18, ADPN, or LEP levels between the various ART regimen groups, aligning with previous local research on IRS. 45 IRS and CK-18 generally showed only weak, singular correlations. While some studies have explored CK-18 as a marker for NASH diagnosis, 46 data specifically linking its correlation strength with MASLD in PLWH remains limited. 47
In contrast, LEP demonstrated a wider range of fair to strong correlations with key metabolic parameters and MASLD biochemical formulas, most notably with HSI (R = .56) and BMI (R = .53). These findings are consistent with existing literature highlighting leptin's role in adipose tissue hypertrophy, insulin resistance, and its potential involvement in hepatic steatosis progression. 25 The observed sex difference in LEP levels, with higher concentrations in females, also aligns with established research on fat tissue distribution. 48 Furthermore, ADPN correlated positively with HDL-C (R = .47) and negatively with triglycerides (R = −.24), HSI (R = −.21), and TyG (R = –.24). This pattern of correlations, particularly the inverse relationships with markers of metabolic dysfunction and hepatic steatosis, is consistent with research highlighting adiponectin's protective role in reducing body fat, increasing insulin sensitivity, and preventing hepatic lipid accumulation, suggesting its inverse relationship with MASLD development. 46
Conclusions
Our study of PLWH on various ART regimens found no significant association between most HIV-related factors and MASLD development (biochemically estimated), with the exception of a weak correlation between nadir CD4 count and NAFLD-LFS. Importantly, specific ART regimens also showed no significant correlation with MASLD-related formulas within our cohort.
This weak but significant association with nadir CD4 cell count underscores the importance of early intervention. Given that rapid ART initiation is effective in preventing individuals from becoming “late presenters,” our findings suggest this approach may also be beneficial in reducing the risk of long-term metabolic and hepatic complications like MASLD, by preventing low nadir CD4 values.
Despite these observations regarding nadir CD4 count, our findings indicate that traditional, non-HIV-related metabolic risk factors emerged as the primary drivers of MASLD and associated liver complications in this group. LWA was particularly important, significantly linked to MASLD-related formulas, and solely associated with biochemical hepatitis. BMI and HbA1c also showed several associations.
Among novel biomarkers, LEP proved promising, correlating significantly with MASLD formulas and anthropometric/metabolic parameters. Other biomarkers like ADPN, IRS, and CK-18 showed weaker or marginal associations.
To conclude, MASLD in this cohort of PLWH appears to be predominantly influenced by classic metabolic risk factors rather than HIV-specific factors or ART regimens. Furthermore, larger longitudinal studies are needed to confirm these findings and clarify the role of novel biomarkers in MASLD management among PLWH.
Strengths and Limitations
The strengths of this study include the concurrent assessment of clinical parameters and several novel biomarkers (leptin, irisin, adiponectin, CK-18) in PLWH. Strict exclusion of HBV and HCV coinfections enabled a more accurate evaluation of metabolic and ART-related factors contributing to MASLD. Furthermore, while the demographic homogeneity of the cohort (predominantly Caucasian males from a large urban center in Poland) restricts global generalizability, it minimizes ethnic and systemic confounders, providing real-world data reflecting the specific HIV epidemiological landscape in Central Europe.
This study is also a subject to several limitations. Firstly, its cross-sectional design restricts our ability to establish causality or observe changes in MASLD progression over time. Secondly, no formal a priori sample size calculation was performed; the cohort size was determined by the number of eligible and consenting patients available during the study period. This relatively small sample size, coupled with an uneven distribution of patients across different ART regimens, reduces the statistical power. Consequently, the lack of significant differences between ART regimens should be interpreted with caution due to the potential for Type II errors; our results suggest that metabolic factors are the dominant drivers of MASLD in this cohort, but do not definitively rule out drug-specific effects that might be detectable in larger populations.
Thirdly, the study cohort was predominantly male (83%) and exclusively Caucasian, reflecting the specific epidemiological characteristics of the HIV epidemic in region (Poland and Central Europe). While this limits the generalizability of our findings to women and other ethnic groups, it provides specific data for this geographical region.
Furthermore, our assessment of liver disease, including steatosis and fibrosis, relied solely on biochemical markers and calculated noninvasive formulas, lacking radiological or histopathological confirmation, which impacts diagnostic precision.
The impact of ART duration is also potentially confounded by patients having used multiple treatment regimens over the years, making it challenging to isolate the effects of current or cumulative therapy. Additionally, the exclusion of individuals with HBV or HCV coinfection restricts the generalizability of our findings to the broader PLWH population, many of whom experience such coinfections.
Additionally, data limitations were encountered, with some variables, such as lifetime weight amplitude (LWA), having missing information due to incomplete patient responses or gaps in medical records; however, we prioritized data accuracy over completeness. We acknowledge that data regarding weight history and lifestyle factors are self-reported and subject to recall bias.
Lastly, no formal a priori sample size calculation was performed; the cohort size was determined by the number of eligible and consenting patients available during the study period. This modest sample size may limit the statistical power to detect more subtle differences between specific ART subgroups.
Supplemental Material
sj-docx-1-jia-10.1177_23259582261436955 - Supplemental material for MASLD in PLWH on ART: Predominance of Metabolic Risk Factors and Insights From Novel Biomarkers—A Cross-Sectional Study in Wrocław, Poland
Supplemental material, sj-docx-1-jia-10.1177_23259582261436955 for MASLD in PLWH on ART: Predominance of Metabolic Risk Factors and Insights From Novel Biomarkers—A Cross-Sectional Study in Wrocław, Poland by Michał Biały and Małgorzata Inglot in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-pdf-2-jia-10.1177_23259582261436955 - Supplemental material for MASLD in PLWH on ART: Predominance of Metabolic Risk Factors and Insights From Novel Biomarkers—A Cross-Sectional Study in Wrocław, Poland
Supplemental material, sj-pdf-2-jia-10.1177_23259582261436955 for MASLD in PLWH on ART: Predominance of Metabolic Risk Factors and Insights From Novel Biomarkers—A Cross-Sectional Study in Wrocław, Poland by Michał Biały and Małgorzata Inglot in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-3-jia-10.1177_23259582261436955 - Supplemental material for MASLD in PLWH on ART: Predominance of Metabolic Risk Factors and Insights From Novel Biomarkers—A Cross-Sectional Study in Wrocław, Poland
Supplemental material, sj-docx-3-jia-10.1177_23259582261436955 for MASLD in PLWH on ART: Predominance of Metabolic Risk Factors and Insights From Novel Biomarkers—A Cross-Sectional Study in Wrocław, Poland by Michał Biały and Małgorzata Inglot in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgments
The authors extend their sincere gratitude to Dr. Jacek Gąsiorowski, Head of the HIV Outpatient Clinic, for providing the clinical site essential for this research. We also thank Dr. Małgorzata Zalewska for her invaluable assistance with the selection and execution of biochemical assays at the University Laboratory, and Joanna Bortkiewicz, Nurse Coordinator at the Clinic, for her help in managing the sample collection process. Our appreciation also goes to Dr. Marcin Czarnecki for his assistance with contacts and procedures related to the Bioethics Committee, and to the physicians from the clinic who significantly aided in patient recruitment: Dr. Marzena Dawiec, MD Michał Furdal, Prof. Brygida Knysz, Dr. Weronika Rymer, Dr. Bartosz Szetela, and Dr. Aleksandra Szymczak. Finally, we are grateful to Małgorzata Rąpała for her expert assistance with the statistical analysis.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Wroclaw Medical University. Approval Code: KB-380/2021.
Consent to Participate
All patients provided their informed written consent prior to participation.
Consent for Publication
Not applicable.
Author Contributions
Conceptualization was performed by MI and MB. Methodology was developed by MI and MB. MB was responsible for the investigation, data collection, and writing the original draft. MI handled review, editing, and supervision. Formal analysis was carried out by MB and MI. Project administration and funding acquisition were managed by MB and MI. The authors confirm this is their original work. Gemini 2.5 Large Language Model was used solely for language refinement, grammatical correction, and enhancing text flow and professionalism. AI did not generate any content, interpret data, or formulate conclusions. Authors remain fully responsible for the manuscript's accuracy and integrity.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Wroclaw Medical University internal grant: UMW SUB.C170.21.027.
Declaration of Conflicting Interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MB has served as a speaker for Gilead. MI has served as a consultant for Gilead, GKS-ViiV, Janssen, and Merck, as well as a speaker for AbbVie, Gilead, GKS-ViiV, Janssen, and Merck.
Data Availability
The data supporting this research are not publicly available as they contain information that could compromise the privacy of research participants. However, anonymized data may be made available from the corresponding author upon reasonable request and with permission from the Ethics Committee of Wroclaw Medical University.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.