
Abstract
Background
Despite growing concerns, limited research has demonstrated how psychological factors influence substance use in people with HIV (PWH). Therefore, we examined the association between heightened vigilance and substance use outcomes in people with (PWH) and without HIV (PWoH), while accounting for key risk factors.
Methods
Participants (n = 138) were recruited from an HIV clinic and the surrounding community, completing a urine drug screener (UDS) and questionnaires.
Results
PWH reported greater insomnia (P < .001), self-reported substance use (P < .001), and tested positive for more substances (P < .001) compared to PWoH. Self-reported use was associated with identifying as a man (P = .04) and higher vigilance (P = .02). Furthermore, having HIV (P < .001), being African American (P = .03), and greater depressive symptoms (P = .04) predicted greater UDS substance use.
Discussion
Future research should center stress-induced vigilance, mental health, and substance use among PWH.
Plain Language Summary
Substance use is a major concern for people with HIV and affects 65% of the population. Despite growing research, minimal work has aimed to understand how demographic, psychological, and clinical factors influence substance use patterns in this group. Therefore, our study aimed to understand whether heightened vigilance was a stronger contributor to substance use in people with and without HIV. Using a urine drug screener and questionnaires, we found that PWH reported greater demographic (ie, African American, older adults), clinical (ie, insomnia), and psychological risk factors compared to people without HIV. Identifying as a man and having higher vigilance was associated with greater self-report use, and identifying as African American and having greater depressive symptoms predicted greater use on the urine drug screener. These findings represent the need for more research centered around stress-induced vigilance, mental health, and coping patterns in PWH.
Keywords
Substance use is a significant public health concern among people with HIV (PWH), with prevalence rates ranging from 21% to 65% in this population. 1 While these rates vary based on the type of substance used and geographic region, PWH in the Deep South (ie, nine Southern U.S. states including Alabama, Mississippi, Louisiana, Georgia, South Carolina, Arkansas, Texas, Florida, Tennessee) bear an unequal burden.2,3 These populations are historically underserved and disproportionately affected by HIV diagnoses and treatment barriers. 4 Prior research has identified several demographic (ie, age, race, gender, lower socioeconomic status), psychological (ie, depression), and clinical (ie, insomnia, chronic pain) risk factors that are associated with substance use in PWH1,5–8 For instance, evidence highlights sociodemographic disparities, with African Americans, older adults, women, and individuals of lower socioeconomic status at greater risk4,9–15 In African American women, studies report high rates of alcohol use, as well as associations between heavy drinking and the prevalence of mental health conditions (ie, depression and post-traumatic stress). 12 Additionally, longitudinal data show that PWH use more substances than people without HIV (PWoH), with poverty further increasing the likelihood of using methamphetamine, hallucinogens, tobacco, and other illicit drugs. 16
In addition to demographic risk factors, the use of alcohol, cannabis, cocaine, stimulants, and other substances has been linked to greater pain severity and disability, as well as greater symptoms of depression and insomnia17–23 Chronic pain is frequently undertreated in PWH, particularly when it lacks a clear biomedical cause, which may prompt self-medication through substance use.18,19,24 In turn, this may contribute to a detrimental cycle of increased symptom burden, reduced antiretroviral therapy (ART) adherence, and missed medical visits.25,26 Depression and insomnia are similarly prevalent, often co-occurring with pain and substance use, and each has been independently associated with poorer HIV outcomes and elevated substance use risk19,27–29 While this triad of symptoms appears to confer substantial vulnerability to substance use, relatively few studies have examined whether these factors uniquely predict substance use in PWH, relative to PWoH. Together, these findings underscore the high degree of symptom comorbidity in PWH, and the complex, intersecting relationships among clinical health conditions, demographics, and substance use outcomes25,26,30–32
Although prior work has documented substantial comorbidity among PWH, less is understood about the coping responses that may contribute to these associations, including heightened vigilance in response to chronic social stress. Heightened vigilance is a passive, anticipatory strategy33–35 in which individuals monitor their behavior and surroundings, often avoiding social situations or limiting interpersonal interactions, in response to perceived social threats.36,37 This coping mechanism represents the downstream effects of chronic social stress in PWH and further amplifies the risk for substance use.35,38 Although often conceptualized within the framework of discrimination-related stress, vigilance may emerge from a broader range of social or environmental stressors, particularly among PWH who often face multiple intersecting forms of marginalization35,39–41 In this regard, heightened vigilance may deter individuals from accessing HIV-related services (eg, testing and prevention, ART treatment) and reduce social engagement42–45 Additionally, the cognitive and emotional demands of sustained vigilance (ie, rumination, worry, anticipation) may negatively impact key health outcomes including sleep, mood, and physical functioning.38,46,47 These effects align with the Stress and Coping model, which posits that repeated exposure to stressors can compromise physical and mental health through the activation of stress response systems and the adoption of maladaptive health behaviors.48,49 Furthermore, this framework highlights how appraisals of threat and available coping resources shape individuals’ physiological and behavioral responses to stress, thereby offering a critical lens for exploring how heightened vigilance may contribute to adverse health outcomes in PWH. Despite its theoretical relevance, few studies have examined the role of anticipated stress, or heightened vigilance, on HIV-related health behaviors.33,34,46,50
Therefore, the primary aim of this study was to examine the association between heightened vigilance and substance use outcomes in PWH and PWoH, while accounting for key risk factors (ie, demographic characteristics, depression, insomnia, chronic pain). We hypothesized that heightened vigilance would emerge as a stronger predictor of substance use relative to these established risk factors, and that this association would be more pronounced among PWH. A secondary aim was to characterize and assess substance use patterns by HIV status. It was hypothesized that PWH would report a higher frequency of substance use compared to PWoH.
Methods
Study Design and Recruitment
This secondary data analysis was a part of a parent project that examined the impact of insomnia on pain outcomes in PWH (R01HL147603) and was conducted from August 2019 to July 2023 in Birmingham, Alabama. Prospective participants were excluded if they had any concurrent medical conditions that could confound interpretation of study outcomes, or coexisting disease that could preclude successful completion of the protocol including: (1) Systemic rheumatic disease/condition (2) uncontrolled hypertension (ie, BP > 150/95 mm Hg); (3) circulatory disorders (eg, Reynaud's disease); (4) history of heart disease or cardiac events, (5) history of cancer; (6) asthma AND use of an inhaler; (7) history of seizures; (8) history of stroke or other neurological disorder; (9) pregnancy; (10) core body temperature > 100oF as this could indicate acute infection with fever; (11) unwilling to provide a blood sample, (12) non-English speaking, and (13) recent injury or surgical procedure within past 6 months. Otherwise, individuals were included for participation if they did not meet any of the exclusion criteria and were willing to complete the study protocol.
A total of 171 participants were recruited for this study. However, 33 participants were withdrawn following the initial screening due to failure to attend the baseline assessment, unwillingness to verify HIV status or provide a urine drug screening, and having uncontrolled high blood pressure (>150/95 mm Hg). Thus, the final sample size for our study was 138 participants, with 53 people being HIV positive, and 85 people being HIV negative. PWH were recruited via an HIV clinic in Birmingham, Alabama, and HIV status was verified through electronic health records. Participants who reported a negative HIV status had their results verified using an oral HIV test (Oraquick Advance Rapid HIV ½ Swab test). Eligible participants completed two study sessions separated by 1 week. During the first session, demographic and health information were collected. Participants then returned to the laboratory 1 week later to complete a urine drug screening, questionnaires assessing psychological, and clinical risk factors (eg, sleep, depressive symptoms) for substance use, as well as a self-report substance use scale. All methods for this study were approved by the University of Alabama at Birmingham Institutional Review Board (approval no. 300003778) and were carried out with ethical research guidelines (ie, Declaration of Helsinki). All participants provided written and verbal consent to participate in this study. Participants were compensated $200 for completing the study protocol. All study reporting adheres to the guidelines for cross-sectional observational studies as determined by the EQUATOR network (Enhancing the Quality and Transparency of health Research). 51
Surveys
Heightened Vigilance Scale. The heightened vigilance scale (HVS) is a 4-item measure that assesses how often individuals prepare for experiences of overt and covert discrimination daily, with scores ranging from 4 to 24.52,53 Items were rated on a 1 to 6 Likert scale, with higher scores indicating greater vigilance. Additionally, items on this scale assess how often people prepare for possible insults, avoid social situations and places, and are careful about their words and/or appearance. For this study, the HVS demonstrated acceptable internal consistency and reliability (Cronbach's α = 0.72).
Insomnia Severity Index
The insomnia severity index (ISI) is a 7-item questionnaire that assesses clinically significant symptoms of insomnia. 54 Scores on the ISI range from 0 to 28, with higher scores indicating greater symptoms of insomnia. Interpretation of scores for this measure is separated into 3 subdivisions: 0-7 (no clinically significant insomnia), 8-14 (subthreshold insomnia), 15-21 (moderate insomnia), and 22-28 (severe insomnia). For this study, the ISI was analyzed as a continuous variable. Lastly, this scale demonstrated excellent internal consistency and reliability (Cronbach's α = 0.90) and has been used to detect symptoms of insomnia in the general population. 55
Center for Epidemiological Studies Depression Scale
The Center for Epidemiological Studies Depression Scale (CES-D) is a 20-item measure that assesses the frequency of depressive symptoms within the past week. Scores on the CES-D range from 0 to 60, with responses ranging from 0 (never or rarely) to 3 (most of the time), and higher scores representing greater severity of depression. Depressive symptoms that are assessed by the CES-D include negative mood, guilt/worthlessness, helplessness/hopelessness, psychomotor retardation, loss of appetite, and sleep disturbances. Evidence of validity and reliability has been shown in the general population, as well as chronic pain and HIV populations.56,57 This scale also showed good internal consistency and reliability for the current study (Cronbach's α = 0.80).
Alcohol, Smoking and Substance Involvement Screening Test
The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) is a 10-item drug screener that assesses risky use of tobacco, alcohol, cannabis, cocaine, amphetamine-type stimulants, sedatives, hallucinogens, inhalants, opioids, and drugs labeled as “other” that do not fall into these categories. Items on this scale assess lifetime use, use in the past 3 months, and frequency of substance use. Using a 5-point Likert scale, participant responses ranged from 1 (never) to 5 (daily or almost daily). Higher scores on this scale represent a greater frequency of use; however, there are multiple scores that can derive from the ASSIST (ie, lifetime use, specific substance involvement, total substance involvement score). For this study, we focused specifically on total substance involvement within the past 3 months. 58 Final scores on the ASSIST scale ranged from 10 to 50. This measure demonstrated acceptable internal consistency and reliability (Cronbach's α = 0.68).
Urine Drug Screen
Participants completed a 5-min urine drug test (Safe cup III Multidrug 12 m, 25/cs) to assess the use of 12 substances such as cannabis/marijuana, amphetamine, benzodiazepines (when not prescribed), cocaine, ecstasy, methadone, oxycodone, barbiturates, buprenorphine, methamphetamine, morphine, and phencyclidine. This drug panel assesses recent substance use, with detection times ranging from 1 day to 1 week prior. Participants received a response of yes or no to each substance (ie, 0 or 1), and substances that were detected in the urine were summed to calculate a total score for the urine drug screener (UDS) that ranged from 0 (no current use) to 12 (use of 1/ more substances).
Statistical Analyses
Analyses were conducted using SPSS version 29. Less than 15% of participants had missing data; therefore, listwise deletion was applied across regression analyses, leaving a remaining sample size of 131 for the ASSIST, and 127 for the UDS. Multivariate analysis of variance (MANOVA) and chi-square tests were used to assess group differences in substance use, as well as demographic, psychological, and clinical risk factors. Assumptions for regression (ie, linearity, absence of multicollinearity, homoscedasticity, and normality of residuals) were met. The assumption of homogeneity of covariances was violated; therefore, Pillai's Trace was used to evaluate statistical significance. To control for Type I error across multiple comparisons, Bonferroni corrections were applied to follow-up univariate analyses. Using a nested model (ie, blockwise entry), all predictors were entered into a single hierarchical regression based upon self-reported and drug screen-detected use. Model 1 included demographic variables (ie, age, race, gender, poverty level, HIV status), Model 2 included psychological and clinical risk factors (ie, insomnia, pain status, depressive symptoms, heightened vigilance), and Model 3 included an interaction term between HIV status and heightened vigilance (for moderation analysis). The interaction term was created by mean centering the scores on the HVS and multiplying this score by dummy-coded HIV status. Covariates were selected based on prior literature reporting bidirectional relationships between one or more of the primary variables5,15,59–61 For this study, all categorical variables were dummy coded as follows: Race: 0 = White/Caucasian, Asian or Multiracial, 1 = African American; Gender: 0 = Man, 1 = Woman; Pain status: 0 = No chronic pain, 1 = Current chronic pain. To obtain effect size estimates, partial eta-squared (ηp2) was calculated (small=0.01, medium=0.06, large=0.14) for F-tests, and Cohen's f2 was calculated (small=0.02, medium=0.15, large=0.35) for linear regression analyses. Sensitivity analyses were conducted via G*Power, with findings indicating that the study was powered to detect small-to-moderate interaction effects.
Results
Participants
Participants included 53 PWH (38.4%) and 85 PWoH (61.6%). The average age for the total sample was 44 years (age range = 18-71 years old) and was comprised 42% cis-gender men (n = 58), 55.1% cis-gender women (n = 76), 2.2% transgender women (n = 3), and 1 transgender man. To maximize inclusivity, gender was characterized as man or woman. Roughly half of our participants were living above the poverty level (n = 72), and African Americans accounted for over half (63%, n = 87) of the total sample. A full breakdown of demographics and clinical characteristics is shown in Table 1.
Participant Demographics and Clinical Characteristics (N = 138).
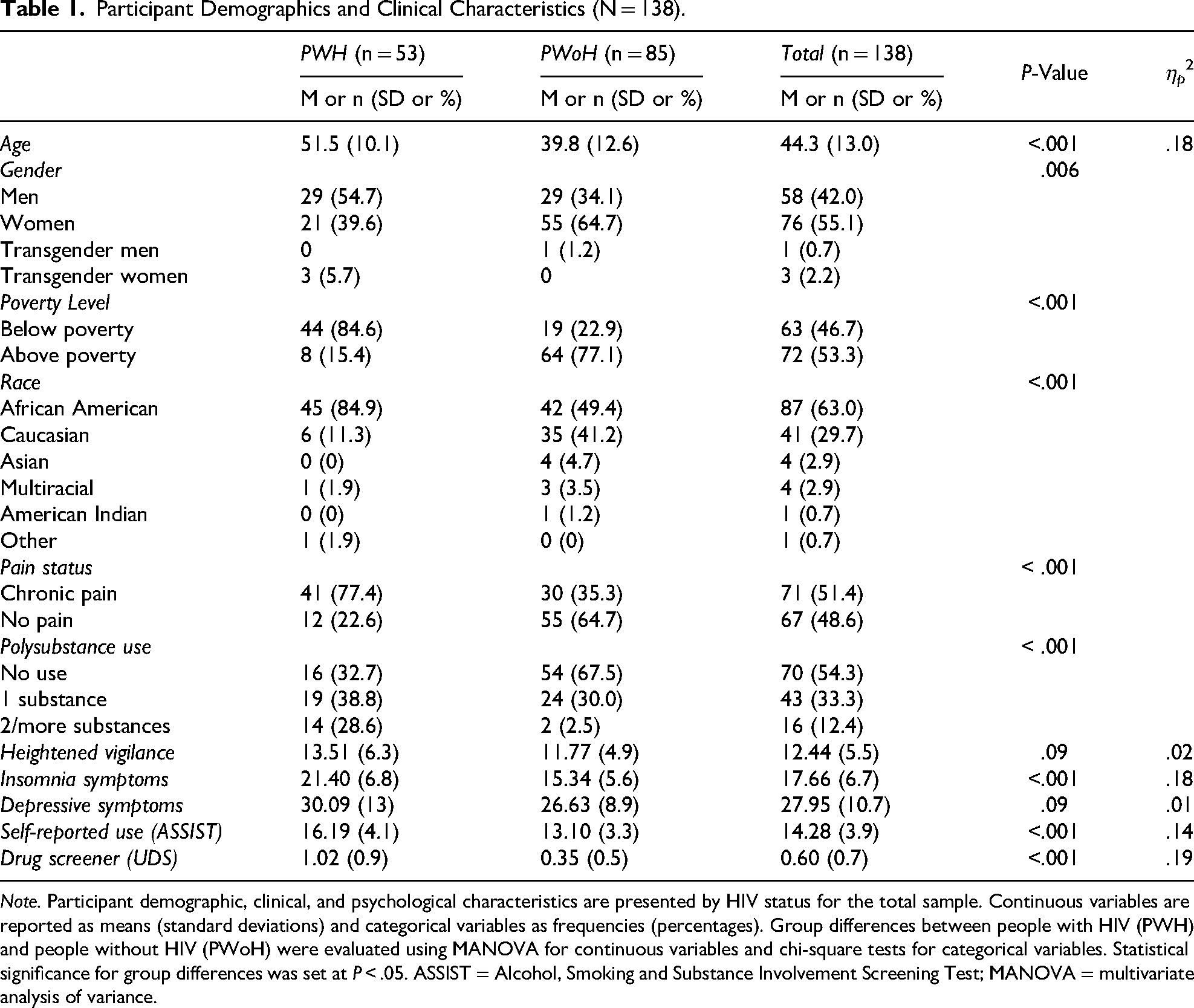
Note. Participant demographic, clinical, and psychological characteristics are presented by HIV status for the total sample. Continuous variables are reported as means (standard deviations) and categorical variables as frequencies (percentages). Group differences between people with HIV (PWH) and people without HIV (PWoH) were evaluated using MANOVA for continuous variables and chi-square tests for categorical variables. Statistical significance for group differences was set at P < .05. ASSIST = Alcohol, Smoking and Substance Involvement Screening Test; MANOVA = multivariate analysis of variance.
Group Differences in Demographic, Clinical, and Psychological Risk Factors
MANOVA and chi-square analyses were conducted to assess differences in demographic, clinical, and psychological risk factors based on HIV status (Table 1). Compared to PWoH, PWH were significantly older (P < .001), men (P = .006), living below the poverty level (P < .001), and African American (P < .001). There were no group differences in depressive symptoms (P = .14) or heightened vigilance (P = .06), but PWH had a greater prevalence of chronic pain (P < .001) and insomnia symptoms (P < .001).
Substance use frequencies (via the ASSIST) were also evaluated, along with substances detected on the urine drug screen (Figures 1 and 2). ASSIST scores indicated that PWH used significantly greater tobacco (P < .001) and cocaine (P < .001), compared to PWoH (Figure 1). PWH were more likely to use 2 or more substances (P < .001) as detected via the UDS and used significantly greater cocaine (P < .001), marijuana (P = .01), methadone (P = .02), and morphine (P = .02), compared to PWoH (Figure 2).
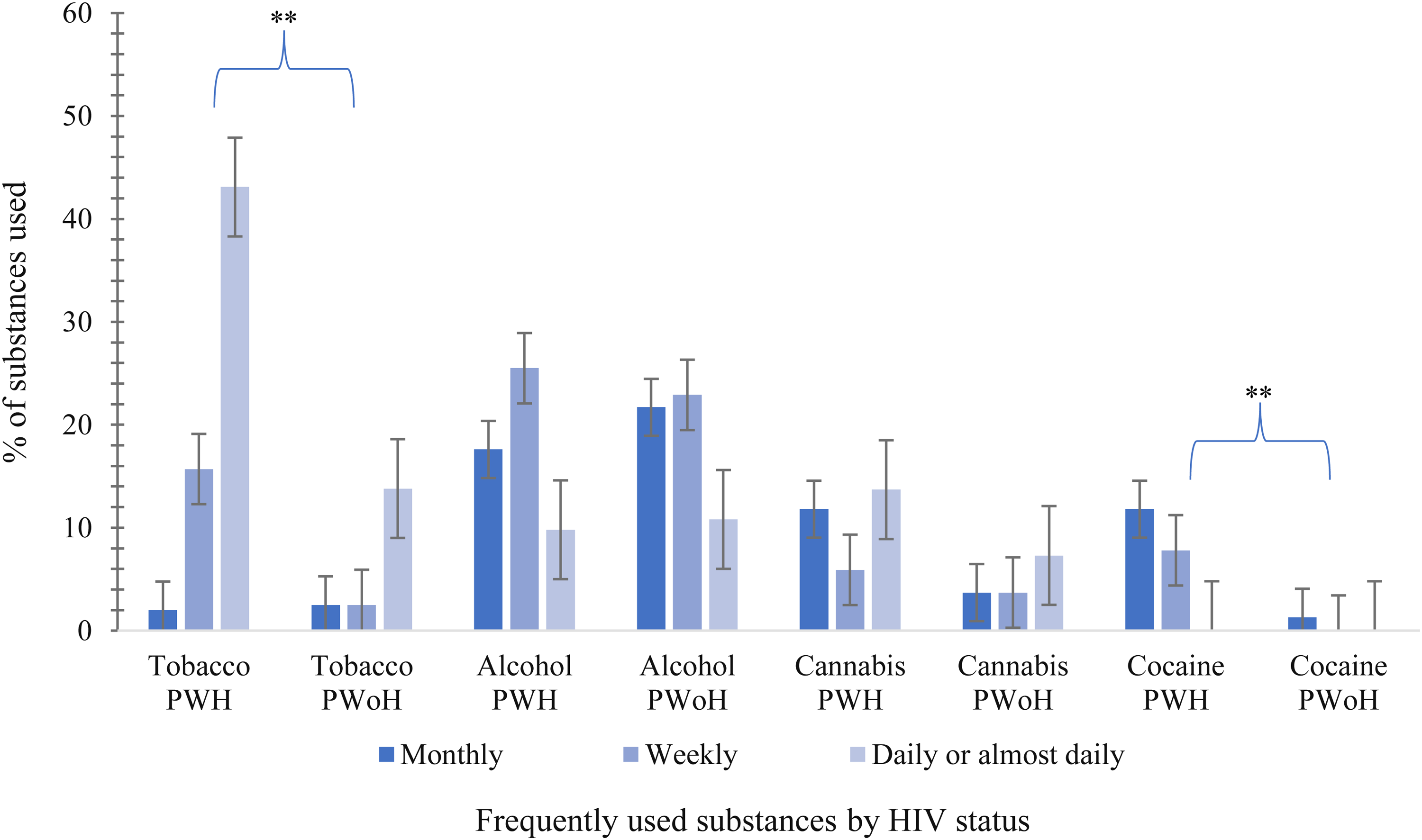
Frequency of self-reported substance use by HIV status. Note. Substance use frequency by HIV status based on ASSIST responses. Frequency was calculated as the percentage of participants reporting use on a monthly, weekly, daily, or almost daily basis within the past 3 months. Only the most commonly reported substances are displayed. PWH = people with HIV; PWoH = people without HIV. Group differences were evaluated using chi-square tests and statistical significance was set at P < .05. ** = P ≤ .01. ASSIST = Alcohol, Smoking and Substance Involvement Screening Test.
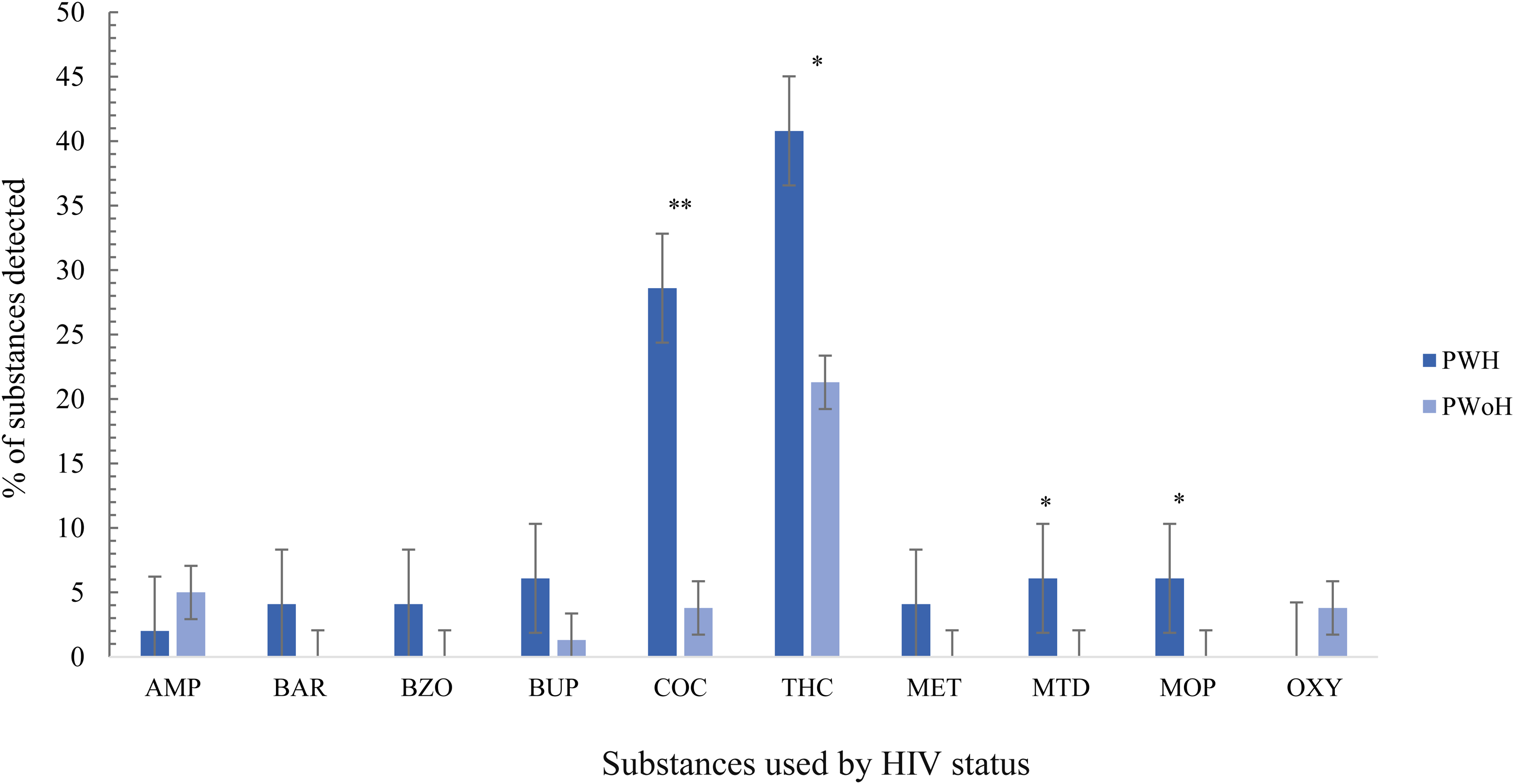
Urine drug screen characteristics based on HIV status (UDS). Note. Substance use by HIV status based on urine drug screening (UDS) results. Percentages reflect the proportion of participants with a positive test result for each substance (coded as 0 = negative, 1 = positive). AMP = amphetamine, BAR = barbiturates, BZO = benzodiazepines, BUP = buprenorphine, COC = cocaine, THC = marijuana, OXY = oxycodone, MOP = morphine, MTD = methadone, MET = methamphetamine; PWH = people with HIV, PWoH = people without HIV. Group differences were evaluated using chi-square tests and statistical significance was set at P < .05. * = P < .05, ** = P ≤ .01.
Hierarchical Regressions: Self-Reported Substance Use
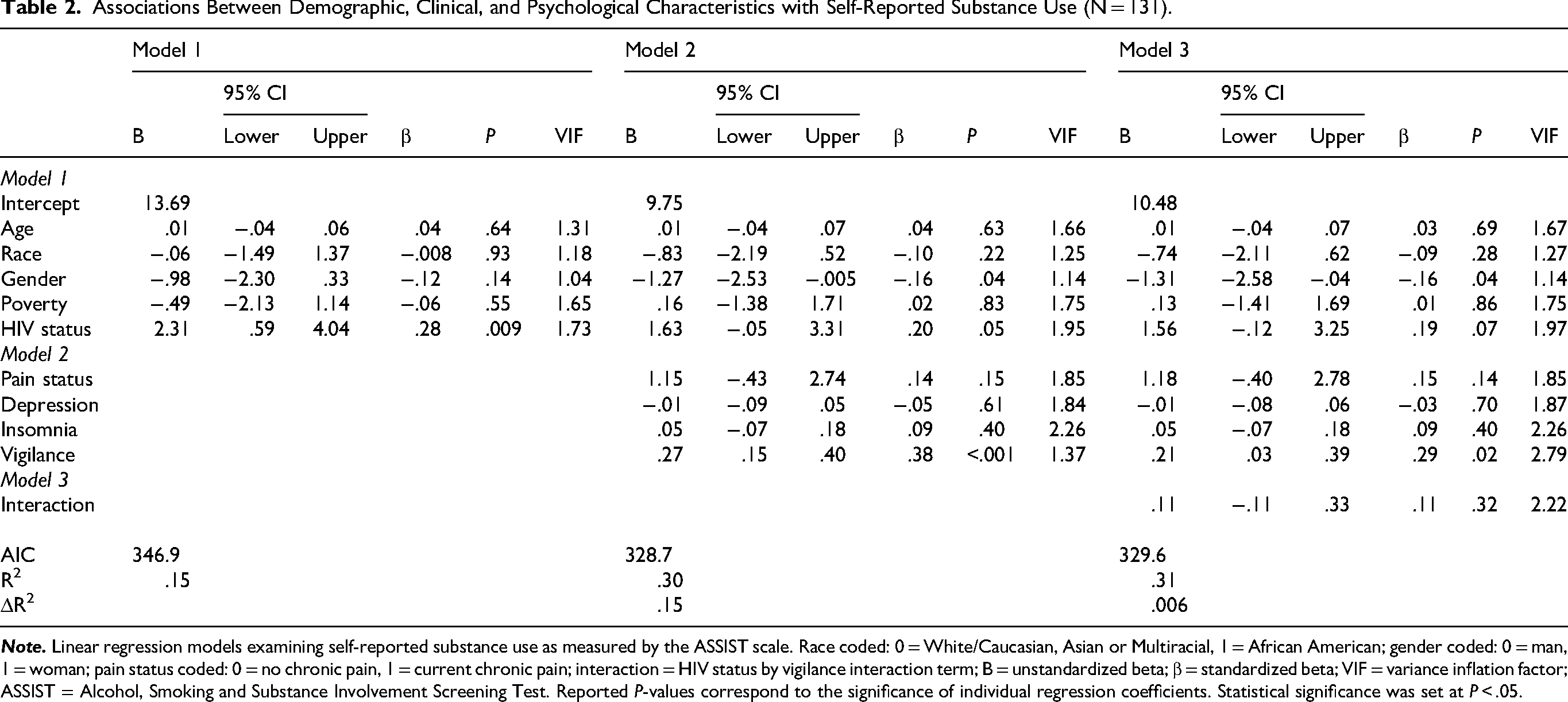
To examine the effects of HIV-related risk factors on self-reported substance use, hierarchical linear regressions were conducted (Table 2). Demographic variables (age, race, gender, poverty level, HIV status) were entered into Model 1, explaining 15% of the variance in self-reported substance use scores (F = 4.52, P < .001). Specifically, having HIV was associated with greater self-reported use (P = .009). When entered into the second block, clinical and psychological factors (pain status, depressive and insomnia symptoms, heightened vigilance) contributed an additional 15% of the variance to the model (FΔ = 6.68, P < .001, f2 = .214). Specifically, identifying as a man (P = .04) and greater heightened vigilance (P < .001) was associated with higher self-reported substance use. After entering the interaction term (ie, HIV status by heightened vigilance) into Step 3, the total variance explained by the model was 31% (F = 5.44, P < .001), explaining an additional .006% of the variance in self-reported substance use (FΔ = .97, P = .32, f2 = .014). Specifically, identifying as a man (P = .04) and greater heightened vigilance (P = .02) was associated with higher self-reported use. The interaction between HIV status and heightened vigilance was not significant (P = .32).
Associations Between Demographic, Clinical, and Psychological Characteristics with Self-Reported Substance Use (N = 131).
Hierarchical Regressions: Urine Drug Screen
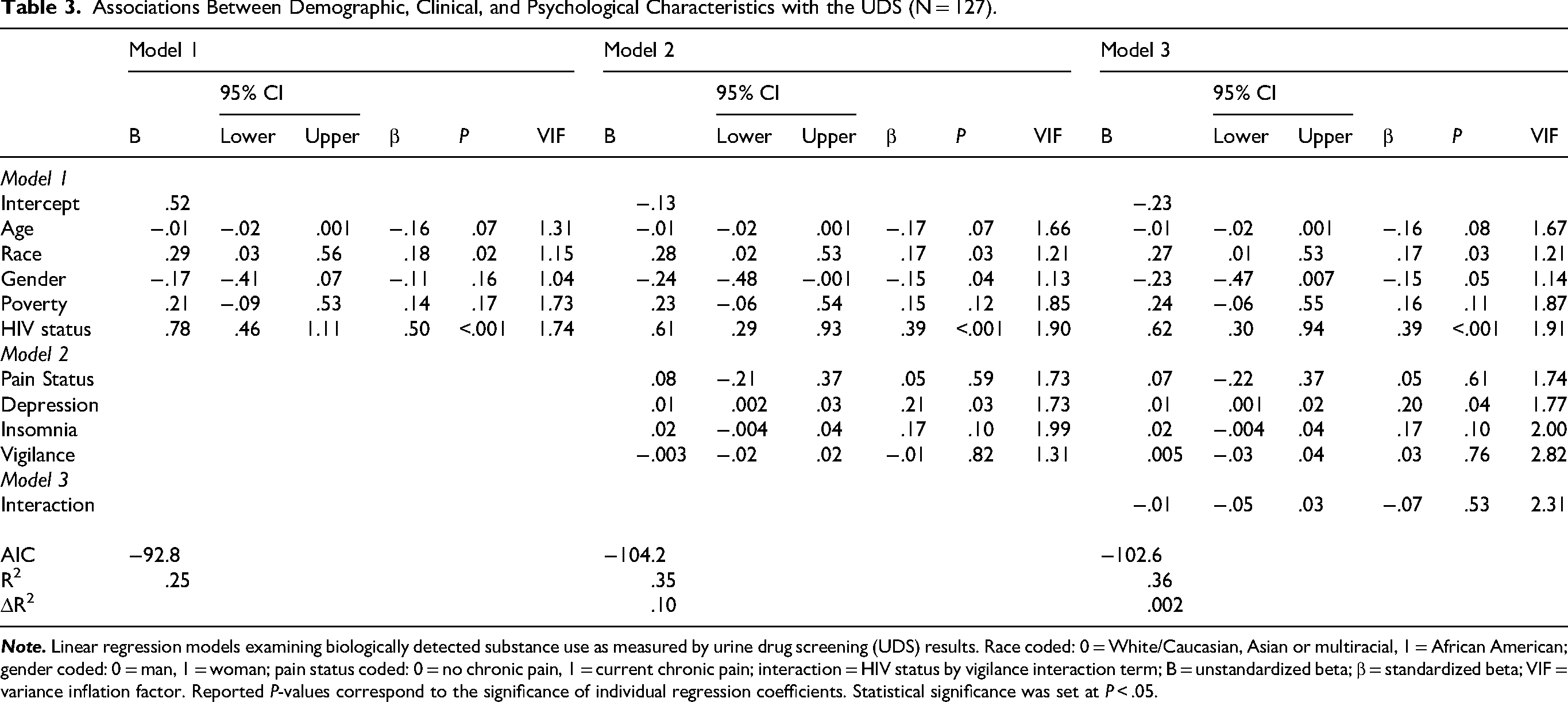
Additional analyses were conducted to examine the effects of HIV-related risk factors on substance use via the urine drug screen (Table 3). Demographic variables (age, race, gender, poverty level, HIV status) were entered into Step 1, explaining 25% of the variance in UDS scores (F = 8.14, P < .001). Specifically, identifying as African American (P = .02) and having HIV (P < .001) were associated with using greater substances on the UDS. When entered into the second block, pain status, depressive and insomnia symptoms, and heightened vigilance contributed an additional 10% of the variance in UDS scores (FΔ = 4.81, P = .001, f2 = .154). Identifying as African American (P = .03) and as a man (P = .04), having HIV (P < .001), and reporting greater depressive symptoms (P = .03) were associated with greater substance use on the UDS. Model 3 explained an additional .002% of the variance in UDS scores (FΔ = .38, P = .53, f2 = .016). Specifically, identifying as African American (P = .03), having HIV (P < .001), and greater depressive symptoms (P = .04) were associated with greater substance use on the UDS; however, the interaction between HIV status and heightened vigilance was not significant (P = .53).
Associations Between Demographic, Clinical, and Psychological Characteristics with the UDS (N = 127).
Discussion
Living with HIV can impact physical and emotional well-being, as people navigate stressors such as social isolation and ongoing health concerns42,62–64 Among these, substance use is common, and frequently co-occurs with psychological and behavioral challenges, yet the interplay among these factors remains poorly understood.42,63,65,66 Heightened vigilance has emerged as an important indicator of discrimination-related stress among minoritized groups.35,39 Therefore, the primary goal of this study was to assess whether heightened vigilance is a stronger predictor of substance use relative to established risk factors, and whether this association was more pronounced among PWH. Our secondary aim was to evaluate differences in substance use frequency by HIV status. Although our hypotheses were mostly supported, we did not observe significant moderation effects between HIV status and heightened vigilance.
Compared to other risk factors (ie, depression, pain, insomnia), heightened vigilance was significantly associated with self-reported substance use, a finding that underscores the role of discrimination-related stress on coping behaviors.38,49,67 This highlights the importance of cognitive appraisal and anticipated stress arising from cumulative experiences of discrimination and/or stigma in PWH.34,50 Although the measure of vigilance does not identify specific sources of stress, it is plausible that experiences of racial, gender, class, and/or health-related discrimination contribute to elevated vigilance and, in turn, substance use patterns. Minority stress theory provides a useful framework for interpreting these findings, as it posits that marginalized populations such as African Americans experience chronic stressors related to stigma, structural disadvantage, and social inequities, which contribute to adverse mental and behavioral outcomes.7,68 In this context, individuals with intersecting marginalized identities (eg, African American race, low socioeconomic status, HIV-positive status) may experience compounding stress, which increases vulnerability to maladaptive coping strategies. Heightened vigilance, as a form of anticipatory stress, may reflect this cumulative burden and contribute to a “weathering effect” with downstream implications for substance use. 69 Supporting this, prior research has linked similar processes to sleep disturbances among African Americans. 37 Our study extends this literature by demonstrating the relevance of vigilance in understanding substance use behaviors among PWH.
We also found that identifying as a man was associated with self-reported substance use, a pattern consistent with broader gender trends in substance use research59,70–72 Prior work indicates that men have a higher likelihood of using alcohol and illicit substances, whereas women are more likely to progress to dependence, in part due to intersecting mental and physical health challenges (eg, depression, anxiety, pain) that can create barriers to accessing timely and effective treatment.73,74 As a result, men tend to have higher rates of substance use disorders, while women report greater treatment needs related to dependence. Given the substantial heterogeneity in substance use patterns across gender (ie, differences in biological processing, stress exposures, structural and social resources), 75 future research is needed to identify gender-specific risks, trajectories, and treatment needs among men and women living with HIV.
In addition to self-reported substance use, we found that identifying as African American, living with HIV, and having higher levels of depressive symptoms were associated with UDS-detected substance use. Like PWH, African Americans are disproportionately exposed to interpersonal (ie, ostracism, traumatic stress, police brutality) and economic (ie, poverty, lower resources and health literacy) stressors compared to other racial groups, which increases their vulnerability to avoidant coping strategies such as substance use, and contributes to elevated overdose risk.67,76,77 Similarly, PWH may use substances to cope with the additive stressors of their daily lives (eg, health-related stigma, comorbid conditions, economic issues).18,78,79 Consistent with this, research shows that chronic exposure to demands that exceed interpersonal and environmental resources can impair coping capacities and decision making.67,80,81 The association between depressive symptoms and substance use also aligns with prior research documenting the bidirectional interplay between depression and substance use, with minoritized groups facing a heightened risk for both conditions.82,83 These findings highlight the need to recognize intersecting risk factors that shape substance use, which could help inform targeted preventive care for both PWH and the broader population.
Heightened vigilance did not moderate the association between HIV status and substance use outcomes, despite its main effect on self-reported substance use. While the study may have been underpowered to detect an interaction effect, this finding suggests that vigilance influences substance use similarly across PWH and PWoH. It is possible that the cumulative stressors faced by PWH may overshadow the influence of vigilance-related processes on substance use, thereby underscoring the need for broader and more intersectional assessments of stress among PWH. 63 PWH are at a greater risk for health-related stigma and discrimination, social and economic challenges, and health comorbidities (ie, depression, insomnia, chronic pain) that require ongoing management.50,84,85 These stressors can create barriers to health-seeking behaviors and treatment, thereby resulting in reduced ART adherence, missed doctors’ visits, and self-coping behaviors such as substance use.25,86 Consequently, the non-significant interaction between HIV status and vigilance may reflect the stronger influence of other contextual or psychosocial factors (eg, income, depression, race) on substance use behaviors. At the same time, PWH may possess higher levels of resilience, or the ability to adapt and cope with daily stressors and challenges,17,87 which could buffer against the negative effects of vigilance. This aligns with research demonstrating that experiences of internalized stigma and heightened vigilance can vary widely depending on individual coping resources, psychological capacities, and broader environmental contexts.34,46,88
This study has several important clinical implications. The observed association between heightened vigilance and self-reported use highlights a potential target for interventions aimed at improving stress-related coping behaviors. Evidence-based approaches such as cognitive-behavioral therapy and mindfulness-based stress reduction may be particularly useful in addressing maladaptive thought patterns, anticipatory stress, and emotional reactivity associated with heightened vigilance89–91 In addition, community-based strategies such as structured peer support groups may help reduce stress and improve coping among PWH.92,93 Interventions that specifically address stressors related to race, gender, socioeconomic disadvantage, and HIV-related stigma may be especially relevant for populations disproportionately affected by these intersecting factors.94–96 Prior research also demonstrates that interventions incorporating positive reappraisal, mindfulness, and physical activity can improve depressive symptoms and stress, while also promoting reductions in substance use.97–100 Taken together, interventions that target stress regulation and harm reduction may represent a promising approach for reducing substance use and improving overall well-being among PWH.
Our study has some limitations that merit acknowledgment. Firstly, the cross-sectional nature of this study limits our ability to draw causal conclusions. Future research should include a longitudinal design to elucidate the directionality of risk factors and substance use. Second, the small sample size may have constrained statistical power, particularly for the detection of interaction effects. In fact, sensitivity analyses indicated that the study was powered to detect small-to-moderate interaction effects and thus may have been underpowered to detect smaller moderation effects, thereby increasing the risk of Type II error. Additionally, the sample consisted primarily of African American participants. While this reflects well-documented disparities in HIV diagnoses, replication in larger and more diverse samples is needed to increase generalizability across both rural and urban populations in the United States. Finally, although our study focused on HIV-related risk, the HVS was not specifically designed to assess HIV-related vigilance. Thus, findings should be interpreted with caution.
In addition, the differential findings between self-reported and UDS substance use outcomes highlight methodological and individual differences in how substance use is captured and/or expressed. Specifically, the ASSIST relies on self-report and reflects broader patterns of substance use (ie, within the past 3 months), whereas the UDS provides a time-limited, biological snapshot of explicit substances within the past 24 h. Additionally, the UDS measures a series of substances that may be prescribed or illicit, while the ASSIST depicts both illicit substances, as well as tobacco and alcohol use. These differences in scope and measurement may contribute to variation in scoring and participant responses. Responses to self-report measures may also be shaped by contextual and structural factors. For example, historical malpractice in clinical research has contributed to mistrust, which may influence disclosure of substance use. 101 Among PWH, reporting illicit substance use may carry perceived risks, including criminalization or loss of public benefits, and potentially lead to selective reporting. In this context, this may help explain why heightened vigilance is more strongly associated with self-reported substance use, whereas sociodemographic attributes and depressive symptoms may exert a greater influence on biologically detected use. Collectively, these findings highlight both the value and complexity of incorporating multiple assessment modalities. While the combined use of the ASSIST and UDS allows for a more comprehensive characterization of substance use than single-method approaches, discrepancies between measures underscore the need for more integrated and standardized assessment strategies, particularly among PWH and other minoritized groups.
Conclusions
Substance use remains a major public health concern in the United States and represents an added burden for PWH. 79 The observed associations between demographic characteristics and substance use underscore the need for intervention approaches that extend beyond condition-specific factors to incorporate an intersectional perspective that addresses the broader social and structural determinants influencing health. Given that substance use is often stigmatized, particularly in socially conservative regions like the Deep South, there is also a critical need to move beyond individual-level explanations to address the upstream drivers of substance use.2,64 Integrated care models that combine substance use treatment with stigma reduction, psychoeducation, and strategies for addressing chronic psychosocial stressors may offer a more effective and compassionate framework for supporting PWH and those at risk for HIV.102,103
Supplemental Material
sj-pdf-1-jia-10.1177_23259582261451960 - Supplemental material for Psychological and Clinical Risk Factors for Substance Use in People With and Without HIV
Supplemental material, sj-pdf-1-jia-10.1177_23259582261451960 for Psychological and Clinical Risk Factors for Substance Use in People With and Without HIV by Joanna M Hobson, Shameka L Cody and Shannon R Gilstrap, Michael A Owens, Myles D Moody, Dyan M White-Gilliam, Stephen Justin Thomas, Emily J Bartley, Burel R Goodin in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-2-jia-10.1177_23259582261451960 - Supplemental material for Psychological and Clinical Risk Factors for Substance Use in People With and Without HIV
Supplemental material, sj-docx-2-jia-10.1177_23259582261451960 for Psychological and Clinical Risk Factors for Substance Use in People With and Without HIV by Joanna M Hobson, Shameka L Cody and Shannon R Gilstrap, Michael A Owens, Myles D Moody, Dyan M White-Gilliam, Stephen Justin Thomas, Emily J Bartley, Burel R Goodin in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Ethical Considerations
All methods for this study were approved by the University of Alabama at Birmingham Institutional Review Board (IRB-300003778) in 2019 and were carried out with ethical research guidelines (ie, Declaration of Helsinki).
Consent to Participate
All participants provided written informed consent prior to participating in the study.
Consent for Publication
All participants were aware that their data would be published, and provided written informed consent during their baseline appointments as advised by UAB's institutional review board.
Author Contributions
JMH was responsible for data conceptualization, analyses, and wrote the original and revised drafts of the manuscript. BRG was responsible for study conceptualization, interpretation of data, and approval of the final version. EJB was responsible for study conceptualization, analysis and interpretation of data, writing (review and editing), and approval of the final version. DWG, SRG, SJT and SLC assisted in daily project administration, study conceptualization, data collection and execution, and provided edits throughout the revision process. MDM and MAO assisted in study conceptualization and provided edits throughout the revision process.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by the University of Alabama at Birmingham Health Services Research Training Program award T32HS013852 (J.M.H.) and NIH/NHLBI R01HL147603 (B.R.G.).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.