
Abstract
Objective
The Building HIV Pathways initiative was developed to address gaps in retention in HIV care.
Methods
The initiative consisted of small-group didactic sessions and faculty/participant discussions with HIV providers and external partners.
Results
We delivered small-group educational sessions to 219 participants at 9 HIV clinics. The average relative gain in confidence at posttraining in regard to implementing measures to identify and reengage patients with care was 27% (P < .01) and at 30-day follow-up was 22% (P < .01). Intent-to-change practices at posttraining around identifying patients no longer attending clinic were observed, including intent to improve use of resources and increase collaboration with external organizations. There was a 58% increase (P < .01) in collaboration with external partners at follow-up.
Conclusion
The Building HIV Pathways initiative demonstrated that in-person, small-group education and strengthening linkages with external partners can improve HIV clinic staff awareness and help build relationships with community partners to reengage patients in HIV clinical services.
Plain Language Summary
Retention in care remains a critical challenge in HIV care, as it has significant implications for both individual and public health outcomes, but few health system-level interventions exist to support retention efforts. The Building HIV Pathways initiative was developed to address gaps in retention in HIV clinic services. The initiative consisted of small-group didactic sessions and faculty/learner discussions with HIV provider teams and external partners. We delivered 10 small-group educational sessions to 219 learners at 9 HIV clinics in the United States. Following education, learners were more confident in their ability to implement measures to identify and reengage patients in care. Learners intended to adopt practices to help identify patients lost to care, including intent to improve the use of resources and increase collaboration with external organizations. There was a subsequent increase in collaboration with external partners at follow-up. The Building HIV Pathways initiative demonstrated that in-person, small-group education and strengthening linkages with external partners can improve HIV clinic staff awareness and help them build relationships with community partners to reengage patients in HIV clinic services.
Keywords
Introduction
People living with HIV often navigate multiple, complex responsibilities alongside their health care, including challenges related to social determinants of health, logistical barriers, and stigma.1,2 These circumstances can make it difficult for them to stay continuously engaged in care and may sometimes result in temporary or prolonged care gaps. In fact, according to the United States Centers for Disease Control and Prevention (CDC), approximately 46% of people living with HIV in the United States are not currently engaged in care, defined as having 2 HIV viral load or CD4 tests at least 3 months apart in a year. 3 Lack of engagement in HIV care has numerous downstream effects at the patient and population levels, namely increased risk of disease progression and death, comorbidities, HIV transmission, and healthcare costs.4–6
Identifying people living with HIV who are not engaged in care can be difficult. Individual clinics may have differing definitions of “not engaged in care,” based on time since the last appointment, time since last laboratory work, or having missed a certain number of appointments, or may not have or be aware of a definition to apply. 7 Without a standard definition, clinics can face challenges in identifying clients who have fallen out of care. Identifying clients not engaged in care is further complicated by challenges in determining whether a patient has moved or otherwise relocated and is thus in care elsewhere. 7
Myriad reasons exist as to why people living with HIV may no longer be engaged in care, both from the patient side—including logistical considerations, competing priorities, medical mistrust, and prior negative experiences in health care—and from the clinic or system side. 8 Numerous strategies for identifying and contacting clients who are not engaged in clinic services, including medical treatment or social support, have proven successful, such as flagging a patient's electronic medical records (EMR); contacting the patient by phone, email, or mail; contacting the patient's emergency contact; utilizing the city or county department of health; and collaborating with community partners who may see the patient more frequently.2,9,10
Although individual interventions to support reengagement in HIV care have been studied, there is limited evidence on initiatives designed to help clinics strengthen their internal protocols and external partnerships to systematically identify and reengage patients who no longer attend clinic. In fact, utilizing internal resources or external partners to provide wraparound services can help in caring for the whole patient and addressing competing priorities.11,12 Co-located services are not widely available, and many HIV clinics lack working relationships with external partners, which can make it difficult for their patients to navigate both routine care and obtain referrals to external resources. Developing and implementing clinic protocols to accomplish change at the patient and clinic levels, thereby affecting public health, is a significant undertaking. 12
Prior to Integritas Communications developing the Building HIV Pathways educational initiative, our team conducted a quantitative survey of 14 HIV care providers who had previously completed continuing medical education (CME) activities through our website to validate the development of the activity by assessing gaps in practices around identifying patients no longer attending clinic and efforts to reengage with them. The survey found that approximately half of these responders believed that “identifying patients lost to follow-up” (from the clinic's perspective) along with “care reengagement” (also from the clinic's perspective) was somewhat to very difficult, as rated on a 5-point Likert scale. 13 Unsurprisingly, approximately 70% of responders believed their clinic lacked resources to fully reengage people living with HIV in clinic services, and only about half of responders were confident in their protocols around patient-provider reengagement. Between 15% and 70% of responders cited a lack of external partnerships, with responses varying for each type of external organization. The most frequently identified external partner for regular collaboration was mental health service organizations, and, least frequently, child services or daycares. 13 In response to these findings, and acknowledging the challenges faced by HIV clinics across the country, Integritas Communications created the Building HIV Pathways educational initiative. The goals of the initiative were to develop and hone each individual HIV clinic's protocols to encourage retention and reengagement with their clients in clinic services and to facilitate collaboration with community partners, each contributing to efforts to improve outcomes for people living with HIV.
Materials and Methods
Initiative Development
Integritas Communications created the Building HIV Pathways initiative, which facilitated small-group, in-person, 75- to 90-min educational sessions for HIV clinic staff and external community partners from June 2023 to March 2024. The educational training, strategies, and assessment methods were based on implementation science, influenced by historically successful similar initiatives conducted by Integritas Communications that focused on practice changes at individual clinics. Building HIV Pathways targeted US clinics in areas of high HIV prevalence. These clinics had previously participated in Integritas Communications’ live small-group CME programs on pre-exposure prophylaxis or hepatitis C virus and were contacted via email by the Building HIV Pathways program manager. Site liaisons, identified in previous live small-group CME programs, were the main point of contact for each of the 9 clinics, and they were informed of the nature of the education, the pre- and posttraining surveys, the follow-up survey at 30 days, and the in-depth post-program interviews to be held 60 days after training. They received a small stipend for their work in coordinating the educational session and participating in the post-program interviews. Clinicians, nonclinician staff, and representatives from external partners, such as peer support organizations, substance use treatment centers, and community-based organizations, were invited to attend each of the sessions. The goal of the sessions was to create networking opportunities between clinics and external partners to enhance patient-provider communication and to support efforts to retain or reengage with patients in clinical and social services. External partners were identified through research of organizations that could support client needs located within a reasonable driving distance of the HIV clinic. The site liaison validated the list of partners to be invited. Exclusion criteria for participants were not established.
Three physicians who are experts in managing HIV were involved in the development of this initiative: they reviewed the clinic survey content, handout materials, didactic content, pre- and posttraining surveys, and the follow-up survey. Each site hosted 1 of the 3 physicians, based on physician availability, to deliver the educational session content in person. After the sessions were scheduled, the site liaison was sent the online 16-question clinic survey, to be completed at any time before session start, to provide Integritas Communications and the host physician with information about the clinic's practices in identifying people living with HIV no longer retained in clinical and social services and strategies that had successfully reengaged clients in care. Participants were asked if they had coordinated with other healthcare services or searched the internet, social media, or used electronic databases (incarceration websites) to ascertain patient status if patient appointments were missed. Results from these surveys were assessed by Integritas Communications and used to influence the direction of interactive discussions and emphasize certain portions of didactic content for each clinic.
Each live session included a didactic portion, in which the physician presented definitions of lost from care, strategies for contacting clients no longer attending the clinic, recommendations on reengaging with them to aid return to clinic, and potential staff roles for bringing these recommendations to fruition. An interactive discussion was also included that focused on definitions of people living with HIV not engaged in clinic services and strategies to create a comprehensive definition at the clinic level, potential causes of poor care engagement, historically successful methods for contacting people living with HIV not engaged in care, and approaches to best reengage with clients to encourage a return to clinic and improve provider-patient relationships, including patient education and strategies to address competing priorities for people living with HIV. Depending on the allotted session time (based on clinic schedule and availability), clinics were offered the opportunity to receive additional didactic education on 2 or 3 of 6 available supplemental topics: HIV in adolescents, women with HIV, mental health and HIV, managing concomitant HIV and substance use disorder, HIV in people experiencing homelessness, and incorporating trauma-informed care into HIV practice. These didactic sessions were developed from a review of literature and all featured evidence-based interventions.
Each attendee, whether clinician, nonclinician staff, or external partner, was to complete a pretraining survey before the educational session and a posttraining survey immediately following the educational session and was considered a participant in the intervention (Table 1). These surveys were developed by educational staff at Integritas Communications in conjunction with the 3 physicians who delivered content to participants. Surveys consisted of 2 knowledge-based questions and six 5-point Likert scale questions about the use of clinic protocols for reengaging and supporting people living with HIV, barriers to these protocols, confidence in interventions to identify and reengage clients in care, and the type of relationship their clinic has with external partners (found in Supplemental Material). Although there was an opportunity to write in additional responses or comments, participants did not provide additional information about their implementation barriers. A follow-up survey was sent to all participants 30 days after the session, with the same questions about clinic protocols, barriers, confidence, and the nature of the relationship with external partners. In addition, the follow-up survey asked participants if they had made any changes to their practice based on the information from the educational session, and, through open-ended questions, asked if they could share specific clinic or patient successes. A second attempt was made to contact participants who completed the posttraining assessment but not the 30-day follow-up survey. A $20 e-gift card was offered to follow-up survey responders. The surveys included a question about trauma-informed care, but data were analyzed only for the sites that received education on this supplemental topic and are not reported here. Data were analyzed by Integritas Communications.
Building HIV Pathways Initiative Pretraining, Posttraining, and 30-Day Follow-Up Survey.

In-depth phone interviews were conducted with the 9 same site liaisons 60 days after the training session, probing the most impactful changes implemented following the educational sessions, changes to in-clinic protocols, development of relationships with external partners, value of the program structure and content, and persisting needs.
Study Design and Data Analysis
This was a mixed-methods analysis and the Standards for Quality Improvement Reporting Excellence were followed for this project. 14 The checklist we followed can be found in Supplemental Material. Quantitative data were obtained from the pretraining, immediate posttraining, and 30-day follow-up surveys, as is standard protocol for CME activities. Data from only the Likert scale questions were collected at the follow-up survey. Discrete, independent, nonpaired data were used for analysis. Statistical analysis was performed on all quantitative data. A 2-sample unpaired t-test using GraphPad (GraphPad Software; Boston, MA) was performed on the average scores for Likert scale confidence-based questions across surveys. For Likert scale questions that asked “how often” and “how familiar,” mean Likert scores were converted to percent respondents (eg, 1 = 0% of the time to 5 = 100% of the time), and percentages were averaged. A chi-square analysis using MedCalc (MedCalc Software Ltd; Ostend, Belgium) was performed on unmatched average pretraining, posttraining, and follow-up question scores across surveys. Statistical significance was considered at P ≤ .05.
Qualitative data from interviews and open-ended survey responses were analyzed using thematic analysis with inductive coding to identify recurring themes across participants.15–18
Ethics
This project was conducted as a quality improvement initiative to enhance care delivery within participating health systems. Because the activities were undertaken for internal improvement, the evaluation did not meet the definition of human subjects research and therefore did not require Institutional Review Board approval.
Results
The Building HIV Pathways sessions were held at 9 individual HIV clinics, with 1 site hosting 2 sessions, for a total of 10 sessions. A total of 219 health care professionals and representatives from external partner organizations attended the live sessions across 9 US cities in 6 states: Georgia, Florida, South Carolina, Mississippi, Washington, and West Virginia. Participants for these sessions were staff from these treatment centers, including physicians, nurses/nurse practitioners, social workers, case managers, administrative staff, and other allied healthcare professionals, and external partners (Table 2). All participants were given a pretraining survey, posttraining survey, and 30-day follow-up survey. Not all participants responded to the surveys: there were 141 responders to the pretraining survey (64% of participants), 123 to the posttraining survey (87% of participants completing the pretraining survey), and 48 (39% of participants completing the posttraining survey) to the follow-up survey. The responders who self-reported managing people living with HIV when asked how many patients they managed (n = 134 in the pretraining survey) reported managing an average of 25 people living with HIV per week.
Building HIV Pathways Participant Demographics.

Results from this educational intervention revealed significant improvements in confidence across key areas of clinical and social services, with confidence related to implementing policies to identify and reengage with clients no longer attending clinic showing strong gains from pretraining to posttraining and sustained improvements through 30-day follow-up. The average relative improvement (compared to baseline confidence) at posttraining was 27% (P < .01) and at follow-up was 22% (P < .01). Table 3 provides the average score for each measure of confidence asked in the pretraining, posttraining, and follow-up surveys.
Confidence Levels of Responders in the Building HIV Pathways Initiative.

Not all responders provided an answer to all questions; therefore, the number of responders varies, with N = 105-138 for the pretraining survey, N = 90-122 for posttraining survey, and N = 47-48 for the follow-up survey.
Questions utilized a Likert scale from 1 = “not at all confident” to 5 = “very confident.” Statistical analysis was performed on individual answer options.
P < .01 for average pretraining versus average posttraining mean confidence scores.
P < .01 for average pretraining versus average 30-day follow-up mean confidence scores.
Participants were asked to identify practice and systemic barriers to implementing clinic protocols around identifying and reengaging with clients no longer engaged in care. The top 3 highest rated barriers after training were lack of staffing/funding (46% in the pretraining survey vs 53% in the posttraining survey), lack of existing protocols (28% vs 47%), and lack of confidence in using the identification/reengagement strategies (18% vs 30%).
This educational initiative led to substantial increases in self-reported pretraining practice and posttraining intent to incorporate practice changes related to utilizing clinic and patient resources and collaborating with external partner organizations. The greatest changes to practice can be seen in Figure 1. “Collaborate with external partners” included collaborating with external organizations, the health department, and providing HIV care co-located with other health care or services; “utilize clinic resources” included transportation assistance, telehealth, and flexible clinic hours; and “utilize patient resources” included using a patient navigator, providing patient education, and identifying potential causes for becoming disengaged from clinic services. A significant increase was observed between pretraining practice and posttraining intent to incorporate specific practices across all 3 major themes (average 42% relative increase from pretraining to posttraining assessment; P < .01). The average self-reported practice change scores at follow-up were not as high as the average intent-to-change scores from the posttraining survey (average 8% relative increase; P = .65), indicating these specific changes were not sustained at 30 days despite high intent to change. When surveyed at follow-up, 85% of responders indicated that the education session they attended had led to changes in their practice or reinforced current practice behaviors; changes could include things outside the listed options in the surveys.

Mean frequency of implementation of resources to identify people living with HIV no longer engaged in care and reengage them. The Likert scale ranged from 1 = “never” to 5 = “100% of the time.” Answer options within the “collaborate with external organizations” theme include collaborate with external partner organizations, co-located care, and collaboration with health department; answer options within the “utilize clinic resources” theme include flexible clinic hours, telehealth, and transportation assistance; and answer options within the “utilize patient resources” theme include peer navigators, identifying and noting patients with risk factors for becoming disengaged from care, and providing written and verbal patient education. Not all responders provided a response to all answer options, resulting in the range of the number of responders seen in the figure. aAs stated in the pretraining survey. bAs stated in the posttraining survey. cAs stated in the 30-day follow-up survey. Data from responders who reported managing people living with HIV. dP < .01 versus pretraining score.
Results of the pretraining survey indicated that clinics most commonly reported existing collaborations with mental health services, shelters, and transportation assistance providers. Immediately following the training, respondents reported a significant increase in their intent to establish or expand collaborations with external organizations that could better support patients of HIV clinics, compared with baseline practice. At the 30-day follow-up, respondents reported actual changes in collaborative practice, indicating that some of these intended partnerships had been implemented. The 3 external organizations most frequently reported as new or expanded collaborations at follow-up were mental health service providers (48% pretraining vs 67% at follow-up; P = .02), food pantries (37% vs 60%; P < .01), and transportation assistance providers (36% vs 63%; P < .01; Figure 2). Across these 3 domains, there was an average relative increase of 38% (P < .05) from pretraining baseline to posttraining intent, and a larger average relative increase of 58% (P < .01) from pretraining baseline to reported practice change at follow-up.
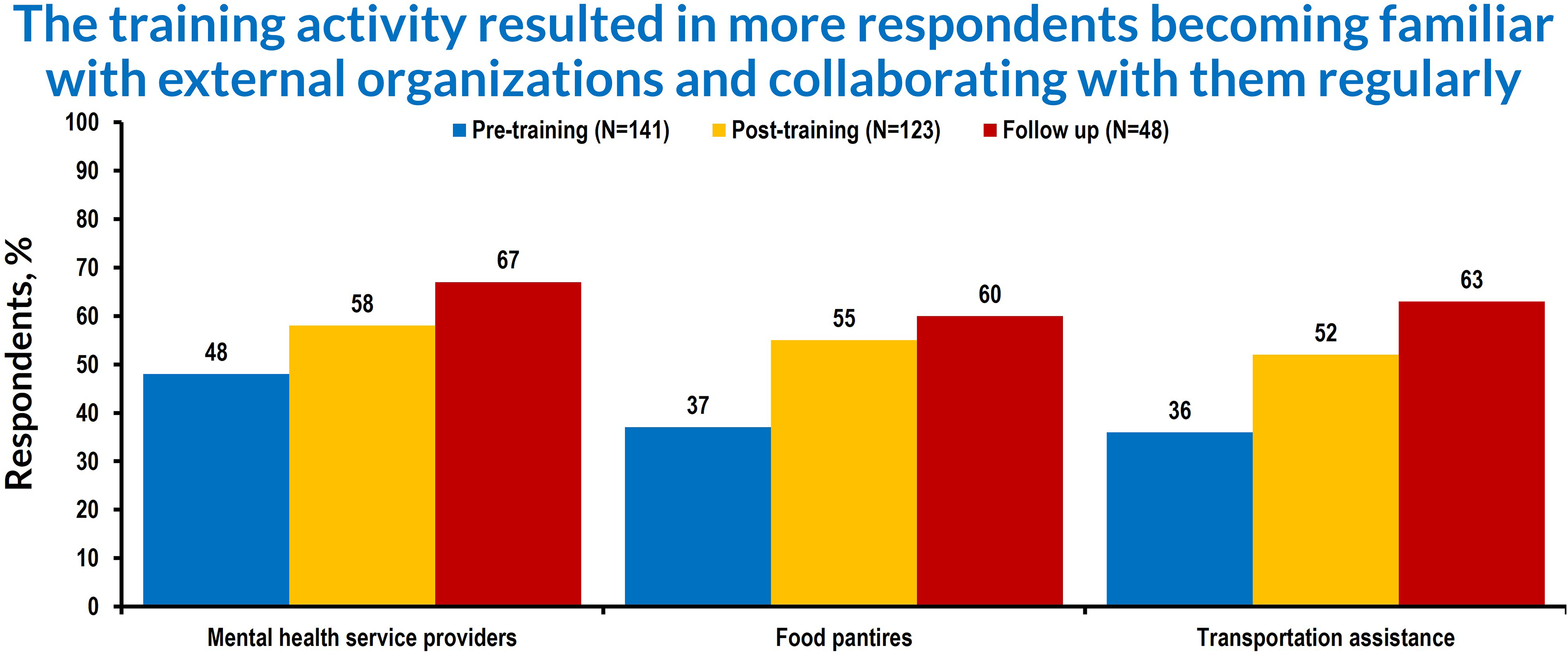
Mean percentage of respondents who stated they were familiar with and regularly collaborated with external partners. Data from responders who self-reported managing people living with HIV for this question. Likert scale from 1 = “not familiar” to 4 = “familiar and regular collaboration/referral.” P < .05 average of the 3 types of external organizations in the pretraining survey versus average posttraining; P < .01 average pretraining versus average follow-up.
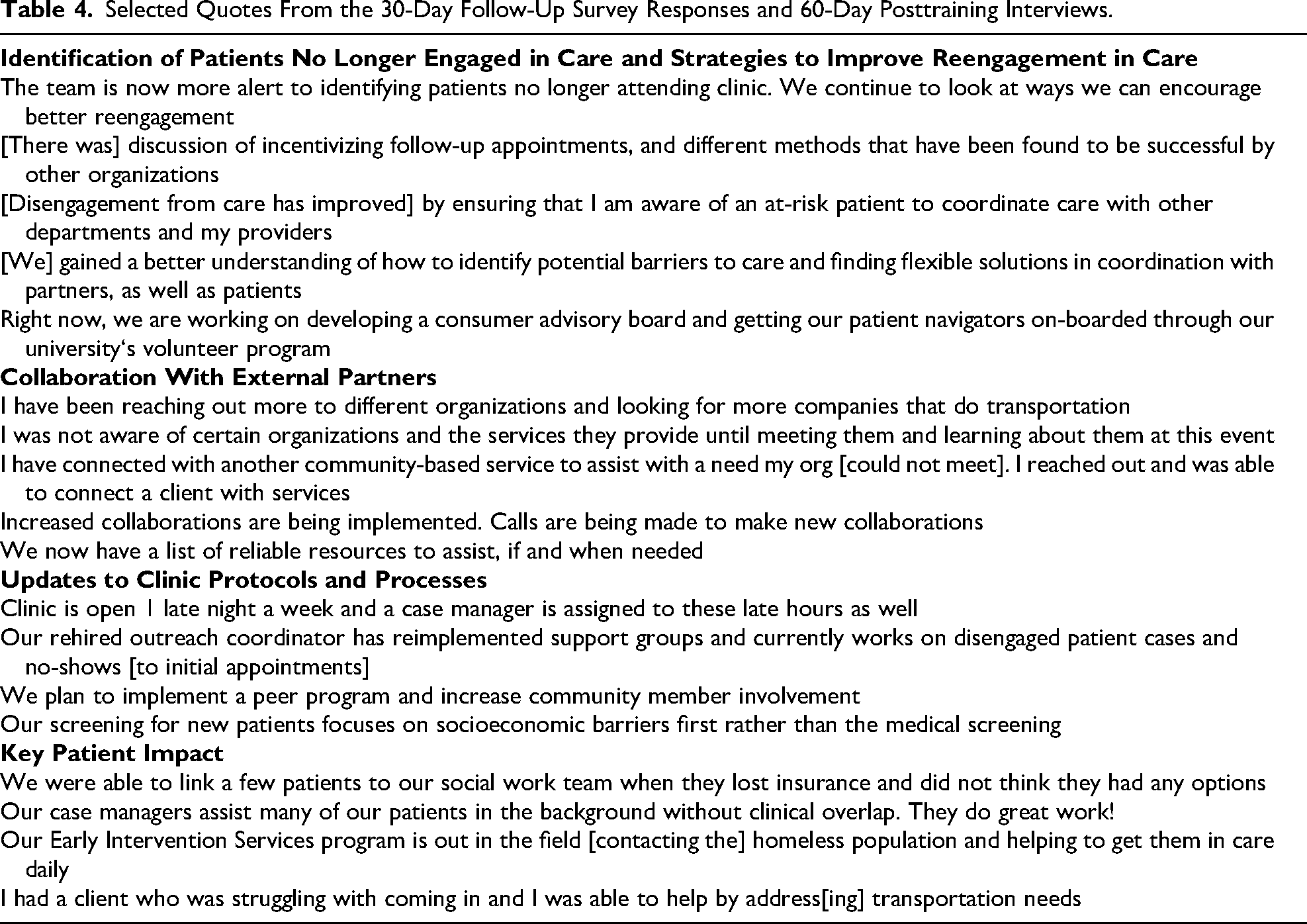
A thematic analysis of 60-day site liaison interviews and open-ended 30-day follow-up survey responses enriched the quantitative findings by illustrating how clinics applied the educational content in practice. Specific responses are described more in Table 4. Four themes emerged: improved identification of clients not engaged in clinic services, strengthened collaboration with external partners, updates to clinic protocols and patient-level impact. Respondents described refining internal definitions and outreach processes, building new partnerships with community organizations, and implementing more structured approaches to reengagement. At the same time, they emphasized ongoing barriers, including staffing limitations, competing patient priorities, and persistent challenges in reaching some clients. These findings suggest that the initiative supported early operational changes while also highlighting the structural constraints clinics continue to face. Data saturation was reached as we saw themes repeated and no new ones emerging.
Selected Quotes From the 30-Day Follow-Up Survey Responses and 60-Day Posttraining Interviews.
Discussion
The detrimental effects of patients living with HIV leaving clinic services and the difficulties clinics face in reengaging with patients have long been established, yet an easily implementable solution remains elusive. The goal of this initiative was 2-fold: first, to help hone HIV clinic protocols to encourage a return to clinic services after periods of absence, and second, to form relationships with external partners that can help to facilitate retention in clinic services. The results of this educational initiative demonstrated that on-site, in-person education that provided practical approaches to reengagement of people living with HIV in clinic services and facilitated networking between clinics and external partners was able to engender impactful changes at the clinic level, with several notable examples cited in the follow-up surveys and 60-day interviews with site liaisons. The total number of participants exceeded our anticipated estimates, and the initiative reached many different clinicians, nonclinical staff, and external partners across a variety of specialties.
Statistically significant improvements in responder confidence and practice changes, in addition to anecdotal evidence from clinic interviews, illustrate the practical effects of this educational initiative. The sustained significant difference in confidence levels likely indicates that responders gained and retained knowledge and skills following the program, particularly in critical areas such as identifying and reengaging people living with HIV who had not been engaged in clinic services and identifying the most appropriate educational or reengagement strategies based on individual patient needs. The responders’ incorporation of new strategies to identify and reengage clients no longer engaged in clinic services, as well as enhanced collaboration with external organizations, for 2 months after the educational program, indicates that the intervention successfully supported long-term changes in clinical practice. Despite these improvements, certain barriers to patient reengagement in clinic services remain.
The improvements in confidence and practice change seen in this initiative parallel successes in other clinic models. For example, many clinics have had success in using EMR to identify clients who meet their clinic's definition of not engaged in care and using their EMR to flag clients more likely to disengage. 10 Similarly, data-to-care (D2C) programs as a collaboration between local health departments and HIV clinics have shown great success in returning people living with HIV to clinic services; the D2C model is recommended by the CDC.9,19,20 The PATHways Program at the Vanderbilt Comprehensive Care Clinic is an example of a clinic that provides a comprehensive, patient-centered approach to care and utilizes a D2C program to help identify and reengage people living with HIV who have become disengaged from clinic services. 21
Previous studies have demonstrated that HIV clinic collaboration with community organizations has been particularly successful for people living with HIV facing challenges in social determinants of health, including people living with HIV experiencing homelessness or substance use disorder.22,23 These relationships can help shape clinic-level interventions, potentially reducing clinic burden or enhancing the clinic's ability to identify and reengage people living with HIV. Furthermore, many clinics have reported success using peer navigators, transportation assistance, co-location of services, and encouraging clinic flexibility in terms of hours and missed appointment penalties.9,24,25 Patient-identified key factors in returning to HIV care are the use of patient navigators, support groups, a stable and communicative relationship with clinicians, and incentives.26–29 Although it can be challenging for clinics, providing co-located care or a “medical home” that includes outreach services, wraparound services, social services, and multiple methods of team communication has proven highly successful in reengaging and maintaining people living with HIV in care. 30 It is important to note that even though people living with HIV may be retained in care according to the definitions of the CDC or Health Resources and Services Administration, if a patient does not have a trusting relationship with a healthcare provider, their competing priorities are not addressed, and their other health needs met, it can be argued that the patient is not truly engaged in care. 10
An aspect of Building HIV Pathways that should be explored in more detail is the numeric increase in the percentage of responders who rated implementation barriers higher in the posttraining survey than in the pretraining survey. Participants were not queried on the rationale for this change, but it is possible that responders had a greater understanding of the barriers following the education. This initiative may have heightened awareness about shortcomings in approaches to clinic protocol development and in existing clinic protocols for identifying and reengaging clients who are no longer engaged in clinic services. This speaks to the need for continued education in this area, reflected by numerous publications about challenges in identifying and reengaging people living with HIV who have become disengaged from clinic services. 7
A particular challenge identified in this activity and others is that clinicians believe certain clients are not interested in or are unwilling to return to clinic services for a variety of reasons, including the patients’ competing priorities, stigma faced in society and in health care, medical mistrust, and an unawareness of the importance of remaining in care.31–33 This represents a large barrier to improving HIV care and may seem nearly insurmountable to clinicians. With community engagement, collaboration with external partners, and clinician and patient education, this barrier may begin to diminish over time.
Some limitations are associated with the Building HIV Pathways initiative. For example, it had limited geographic variability, with a focus on the US Southeast, which faces a disproportionate burden of HIV, accounting for nearly one-half of new HIV acquisitions in 2024. 3 It is not clear whether results from this geographic region are generalizable to the rest of the United States. This initiative also had a relatively small sample size, again hampering the ability to generalize results to the wide variety of clinics seen throughout the United States. Sample size was not calculated prior to the educational sessions, as attendance is variable and optional for small-group CME education. Furthermore, there is a risk of bias in site selection, as all had shown previous interest in receiving CME education. There are additional limitations associated with the data. For example, not all participants completed the follow-up survey; therefore, analyses were conducted using unmatched data. Although there is attrition from the immediate posttraining survey to the 30-day follow-up survey, the percentage of follow-up survey responses is far higher than the typical CME follow-up survey completion rate. The authors, however, acknowledge that this lack of full representation of participants exposed to the educational training limits our ability to effectively measure practice changes and intervention implementation. We also lack a complete understanding of the rationale behind increased reports, following the education, of barriers to implementing strategies to better identify and reengage clients who were no longer engaged in clinic services, although it may be possible to obtain this information in future educational initiatives. Lastly, while community-based organizations (including those with peer support) were invited to attend sessions, we did not query anyone who attended about their HIV status, and, as a result, it is not guaranteed that individuals with lived experience were included among the participants. No one living with HIV was a co-author of the study, as they were not directly involved in content development or in the educational training.
There are numerous reasons to continue this educational initiative: increased collaboration with external partners, implementation of a variety of interventions to identify and reengage with people living with HIV who have become disengaged from clinic services, and increased staff confidence were seen across all HIV clinics involved in this initiative, and we recognize the need to expand the sample size and number of geographic regions in an effort to gain a deeper understanding of barriers to the implementation of strategies for identifying and reengaging people living with HIV in clinic services. Future iterations of Building HIV Pathways will tailor the educational content and survey questions to reflect what was learned from Building HIV Pathways 2023–2024, as well as anecdotal practice changes and identified barriers.
Conclusion
This initiative of small-group, in-person education resulted in increased participant confidence around implementing measures to aid in the identification and reengagement of clients who have left clinic services. There was an increased immediate posttraining intent to utilize clinic and patient resources to improve patient care and engagement. Furthermore, a significant increase was seen in collaboration with external partners when assessed 30 days after the educational session. These quantitative changes were confirmed in 30-day survey responses and in interviews with site liaisons that detailed how clinics had begun changing their protocols, sought expanded collaboration with external partners, and reported examples of successful patient identification and patient reengagement in care. Next steps should include the use of implementation science theories and frameworks to more formally evaluate similar work.
Supplemental Material
sj-docx-1-jia-10.1177_23259582261457314 - Supplemental material for Benefits of Small-Group Education and Community Partner Networking for Reengagement and Retention in Clinical Services Among People With HIV in the United States
Supplemental material, sj-docx-1-jia-10.1177_23259582261457314 for Benefits of Small-Group Education and Community Partner Networking for Reengagement and Retention in Clinical Services Among People With HIV in the United States by Gena Dolson, Amanda Glazar, Kellie L Hawkins, Stacey B Trooskin, Aima A Ahonkhai and Becky Carney in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-2-jia-10.1177_23259582261457314 - Supplemental material for Benefits of Small-Group Education and Community Partner Networking for Reengagement and Retention in Clinical Services Among People With HIV in the United States
Supplemental material, sj-docx-2-jia-10.1177_23259582261457314 for Benefits of Small-Group Education and Community Partner Networking for Reengagement and Retention in Clinical Services Among People With HIV in the United States by Gena Dolson, Amanda Glazar, Kellie L Hawkins, Stacey B Trooskin, Aima A Ahonkhai and Becky Carney in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgments
We would like to acknowledge the participants of this intervention. The authors would like to acknowledge and thank Ann Bledsoe Bollert, MA, CMPP, for her editorial role in the development of this manuscript. Additionally, we would like to acknowledge funding through an unrestricted educational grant from Gilead Sciences, Inc., which had no role in discussions about or writing of the article.
Author Contributions
BC was responsible for developing the overall initiative design and securing funding for the initiative via an educational grant. In consultation with BC, AAA, KLH, and SBT, GD developed all surveys and didactic content. Educational sessions were delivered by AAA, KLH, and SBT. Statistical analysis was performed by AG. The manuscript was written by GD and AG. All authors reviewed and critically revised the manuscript, approved the final draft, and agree to be accountable for the manuscript's accuracy and integrity.
Ethical Approval and Informed Content
This project was conducted as a quality improvement initiative to enhance care delivery within participating health systems. Because the activities were undertaken for internal improvement, the evaluation did not meet the definition of human subjects research and therefore did not require Institutional Review Board approval. Data have been deidentified, and, when possible, aggregate data were used. Learners registered for the CME activity and voluntarily completed pre- and posttraining surveys and the follow-up survey.
Consent for Publication
N/A
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This educational initiative was supported by an unrestricted educational grant from Gilead Sciences, Inc., which had no role in discussions about or writing of the article. KLH, AAA, and SBT received honoraria for participation in the Building HIV Pathways educational initiative and development of this manuscript.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Aima A Ahonkhai, MD, MPH, reported consulting fees/advisory board/speaker relationship with HSC Acquisition, LLC and speaker fees for Gilead Sciences, Inc. Stacey B Trooskin, MD, PhD, MPH, reported consulting fees for Theratechnologies and contracted research for Gilead Sciences, Inc. Kellie L Hawkins, MD, MPH; Gena Dolson, MS; Amanda Glazer, PhD; and Becky Carney, MSPT, have no relevant financial relationships to disclose.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.