
Abstract
Objective
Adolescents (aged 15-18 years) and young adults (19-24 years) living with HIV (AYAH) face particular challenges with HIV care engagement and achieving viral suppression, especially in rural areas. We have few in-depth, qualitative understandings of engagement with HIV care from AYAH's perspectives.
Methods
We conducted semistructured, in-depth interviews with 113 AYAH during a 2-year multilevel intervention to improve viral suppression and health outcomes in rural Kenya and Uganda. Youth participants were purposively sampled and balanced for sex, life stage, and HIV care status to achieve heterogeneity of the characteristics thought to influence the pathways of action and challenges to sustaining HIV care retention. Thematic analysis explored how youth themselves perceived factors that facilitated or challenged clinic attendance and HIV care retention, with the aim of uncovering any distinctions they made within these categories.
Results
Findings revealed a youth-defined concept of HIV care that includes intrinsic social components such as familial support, examples of living positively, a sense of maturing as part of a community, and respectful providers. Youth implicitly distinguished between simply keeping appointments (“retention in care”) and caring about oneself with a shared commitment to health in conjunction with their family and providers (“engagement in care”).
Conclusion
We argue for differentiating “retention in care” and ”engagement in care” along lines similar to distinctions between disease (biomedical definition), illness (personal experience), and sickness (social dimension).
Plain Language Summary
Adolescents (aged 15-18 years) and young adults (19-24 years) living with HIV (AYAH) face particular challenges with HIV care engagement and achieving viral suppression, especially in rural areas. We have few in-depth, qualitative understandings of engagement with HIV care from AYAH's perspectives. We conducted semistructured, in-depth interviews with 113 AYAH in a 2-year multilevel intervention in rural Kenya and Uganda. Youth see HIV care as including social components like familial support, examples of living positively, a sense of maturing as part of a community, and respectful providers. We argue for differentiating “retention in care” and “engagement in care” along lines similar to medical anthropology's distinctions between disease (biomedical definition), illness (personal experience), and sickness (social dimension).
Introduction
Achieving viral suppression is the primary goal in the treatment of individuals with HIV and a critical tool for ending the HIV epidemic.1–3 A public health model termed the “HIV cascade of care” describes the pathway to viral suppression in five stages: diagnosis, linkage, initiation of care, retention in care (alternately called engagement in care), and viral suppression. At other times, this cascade is simplified to three steps: test and treat, engagement in care, and viral suppression.4,5 Initial guidelines helped refine the concept of “retention in care” by further distinguishing two components: attending clinic appointments and adhering to antiretroviral therapy (ART), reflecting the reality that PLHIV's actual experience of the cascade of care is often nonsequential, with people falling off the cascade and then re-engaging with it in cyclical fashion.6,7
While viral suppression is indeed achieved through ART adherence, and such adherence is supported by regular clinic attendance, key populations such as adolescents (15-18 years of age) and young adults (19-24 years) with HIV (collectively, AYAH) face challenges with all components of engagement. These challenges include adhering to medication to achieve sustained viral suppression, attending clinic appointments, and engaging in care beyond appointment attendance by, for example, developing resilience or rallying social support.8–14 In Kenya, almost half of new HIV infections in 2023 were in adolescents and young adults, with young women comprising almost four times as many of these new infections as young men. 15 These adolescents face obstacles to HIV care that include both social structures that broadly restrict women's decision-making power and more immediate factors like lack of social support, self- or anticipated stigma related to accessing sexual health resources, or individual perceptions such as mistrust of providers; in contrast, satisfaction with care may be a facilitator of retention.9,16,17 In addition, poverty, a lack of privacy to take medication (especially at school), pill burden, unreliable family networks—in contrast to the strong adolescent peer networks that appear to facilitate retention10,18,19—unstable employment, and challenges related to the life-stage itself also contribute to nonretention in care.11,20 Several other factors have been associated with viral non-suppression among AYAH, including male gender, length of time on ART, age at disclosure or diagnosis, and rural residence.21–24 Combined with the previously mentioned barriers, adolescents in rural areas are particularly vulnerable to disengaging from HIV care. In rural western Kenya and southwest Uganda, we previously identified lower retention in care among adolescents (81%) compared to adults (94%), with only 67% of AYAH virally suppressed. We also noted that a greater proportion of AYAH who lived in households with other people living with HIV were retained in care compared to those who did not (90% vs 77%). 11
Despite such quantitative and mixed-methods associations between various demographic factors and care disengagement, these studies have used varying definitions of “retention in care” (Figure 1). 2 Even fewer qualitative studies have explored how those factors affect specific elements of engagement in care, especially from the perspective of the AYAH concerned. Thus, we have relatively little qualitative data about what factors influence AYAH's ability to keep appointments, their willingness to engage in care (including their own personal definitions of what said care entails), and their capacity to maintain medication adherence.11,16,25 Reporting the implementation and outcomes of previous interventions aimed at adolescent engagement in care, particularly in differentiated service delivery (DSD) models, also continues to lag behind studies of adults.26,27 These gaps in our understanding merit closer qualitative study of the barriers, facilitators, and recommendations that AYAH themselves offer when it comes to engagement in care broadly defined.
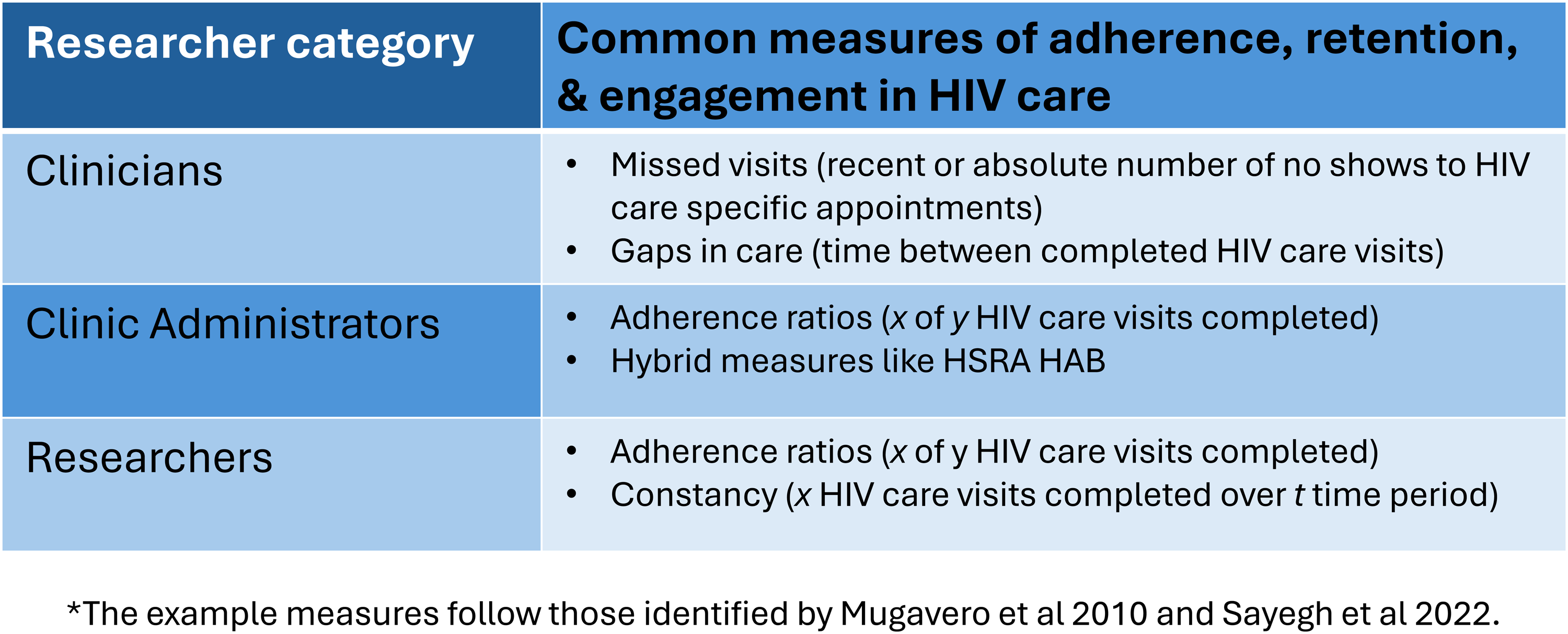
Utility of different definitions for adherence, retention, or engagement in care by professional role.
As a vulnerable population, adolescents serve as a “canary in the coal mine.” Given the changes in the HIV landscape (eg, rollout of test and treat, PrEP, U = U, long-acting injectables) over the more than 15 years since the cascade of care model was articulated, exploring how youth themselves understand “engagement in care” remains crucial if we are to design highly focused interventions targeting specific aspects of the patient-centered care cascade. This is even more the case for adolescents in rural areas. Lessons learned from this population can inform adult HIV care not only as these adolescents on the continent transition to adult care, but also for those outside Africa. 28
This article sought to explore Kenyan and Ugandan AYAH's perceptions of factors that facilitate or challenge clinic attendance and HIV care retention, and to uncover any distinctions they made within these categories during an effective multicomponent youth-centered intervention designed to address the dynamic social and cognitive needs of AYAH. Apart from approaching adolescents through the lens of the life-stage model of youth development as part of a person-centered care model,14,16,29,30 attending to youth's own distinctions within these categories during analysis of the data further centers participants’ illness and care experiences. Because the illness experience differs from the experience of diagnosis and treatment, which was the earlier, near-exclusive focus of biomedical practice,31–33 anthropologists proposed distinguishing between disease, illness, and sickness.33,34 Disease is the term for a diagnosis or label used by professionally-trained practitioners to explain ill health, whereas illness reflects the patient's experience and societal reaction to a disease; sickness then becomes “the process through which worrisome behavioral and biological signs … are given socially recogniszble meanings.” 33 Importantly, because “illness is the way the sick person, his family, and his social network perceive, label, explain, valuate, and respond to disease” 34 and because illness categories “condense fields of experience,” 31 this distinction of terms allows us to attend to “the broad contextual implications of deeply human experiences of suffering.” 32 Since these terms also have a rough corollary in the care process, wherein illnesses are healed, while diseases are cured, 33 we can also distinguish people's experiences of the healing process from the process of curing a disease, a distinction made more complex in the case of chronic managed conditions. These distinctions align with the movement towards patient-centered care, which invites an understanding of the whole person by giving people's experiences primacy.35–39 While global health delivery has advocated moving from disease-specific to person-centered care at the health care delivery level, with the aim of increasing patient agency in their own health care decisions, we also argue that a patient-experience lens should be applied to analytical categories like “retention/engagement in care” as well.
Methods
Larger Study Context
SEARCH-Youth (NCT03848728) was a community cluster-randomized controlled trial conducted in 28 rural communities in western Kenya and southwestern Uganda where HIV prevalence is high (19.6% in Homa Bay county, Kenya; 6.3% in SW Uganda).15,16,40 The SEARCH-Youth intervention was designed to accommodate the dynamic growth of AYAH aged 15 to 24 years and help them navigate challenges to maintain their engagement with their healthcare. It combined elements aimed to improve client–provider relationships (life-stage-based discussion around youth behaviors and supports as well as life-event-based discussions through a patient-centered care approach), improve flexibility and access to facilities (offering out-of-hours, offsite, and phone access appointments), and offered a biomedical tool (rapid viral load feedback), as well as a communication platform to facilitate collaboration among providers at different rural facilities. 16 A cluster randomized trial, SEARCH-Youth, was shown to increase rates of virologic suppression across all study subgroups, with the greatest improvement observed among AYAH re-engaging in care (RR 1.60, 95% CI 1.00-2.55; P = .025), and increased the rate of retention (91% vs 72% at 2 years).
Immediate Study Context and Participants
A longitudinal qualitative study embedded within the trial included indepth, semistructured interviews (IDIs) with purposively-selected samples of AYAH from both arms of the study, balanced by age (15-17 vs 18-24 years), sex, trial arm, country, and ART status and HIV care status (engaged in care for ≥6 months, re-engaging in care after dropping out >6 months, and new to care within the previous 6 months (Table 1); family members the youth identified as most involved in their HIV care; and HIV care providers (clinical officers, nurses, peer educators) from two intervention clinics per region, to include perspectives from both service uptake and service provision sides. We have published the longitudinal case study results elsewhere. 41 We chose semistructured IDIs to identify the pathways of action and challenges to sustaining implementation of the intervention and to elicit potentially unknown or overlooked variables identifiable through later inductive analysis in the interpretivist tradition (see below), and purposive sampling to achieve heterogeneity of the characteristics thought to influence the phenomena under study, while reflecting the demographic composition of the main study.
Participant demographics.
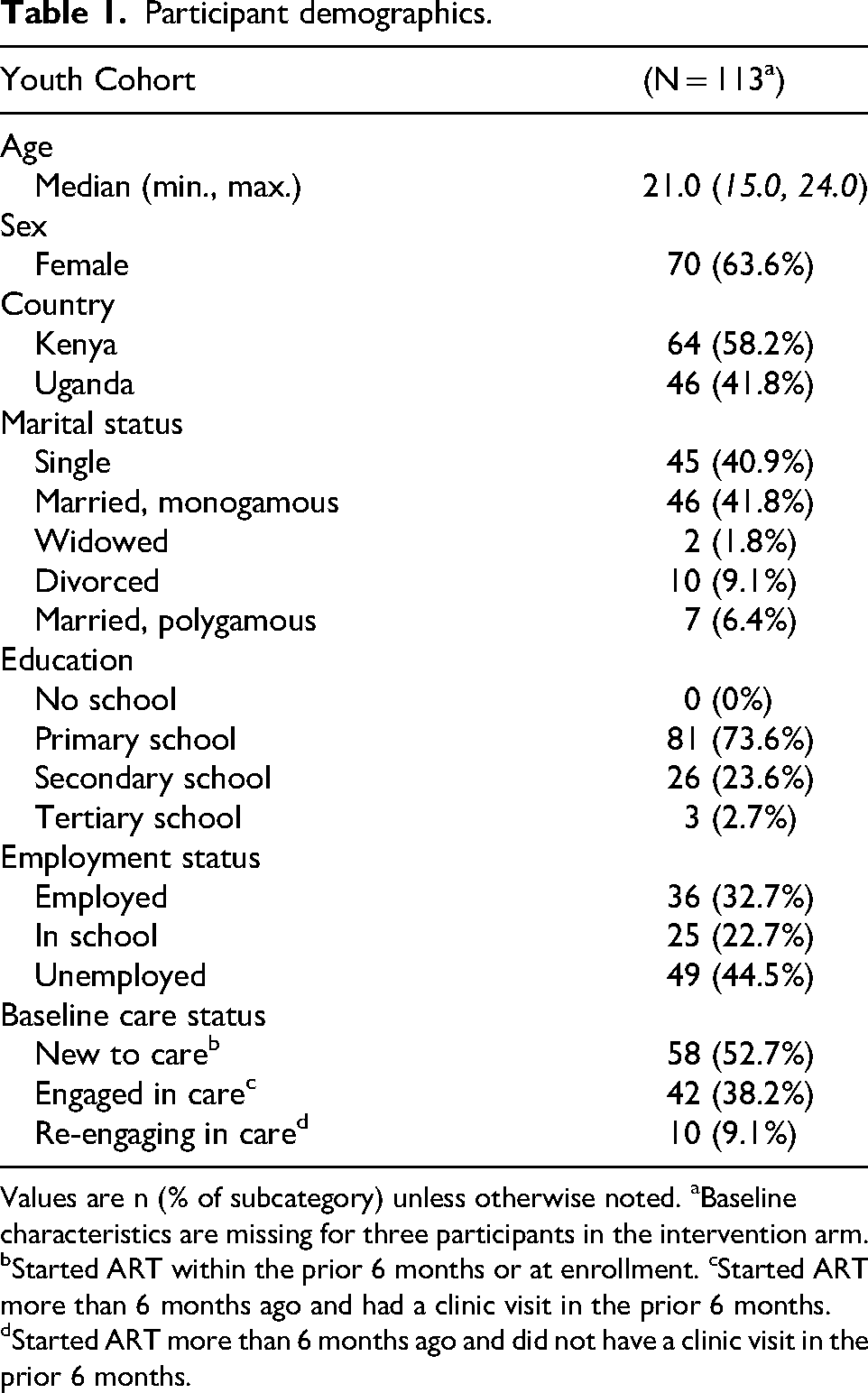
Values are n (% of subcategory) unless otherwise noted. aBaseline characteristics are missing for three participants in the intervention arm. bStarted ART within the prior 6 months or at enrollment. cStarted ART more than 6 months ago and had a clinic visit in the prior 6 months. dStarted ART more than 6 months ago and did not have a clinic visit in the prior 6 months.
Data Collection
A gender-balanced team (2 female: CA, AO; 2 male: FA, LO) of trained qualitative researchers who were community members and native speakers of the local languages (DhoLuo, English, Runyankole, English) and trained to establish rapport based on sensitivity and respect for youth participants administered the 30 to 90-min long in-depth, semi-structured interviews with youth from both arms at three time points: at baseline (June to December 2019; n = 83), at 1-year follow-up (F1; September 2020 to February 2021; n = 76, of whom 27 were replaced baseline participants who moved or were lost to follow-up) and at the end of the second year with intervention-arm youth having a previous BL or F1 interview (F2; October 2021 to December 2021; n = 46) (see Table S1). We also interviewed family members (n = 51) and purposively sampled providers (n = 32) of youth HIV care at baseline (June 2019 to December 2019) or year 1 (October 2020 to March 2021). The semi-structured nature of the interviews led to the above-noted variability in interview length.
We interviewed participants in quiet and convenient locations to ensure comfort (eg, at home or in private clinic rooms) and confidentiality, aware of the social contexts of HIV stigma. Interviews explored participant household and life context, clinical experiences, ART adherence, HIV care history, social support systems, and (for family members) caregiving for AYAH, following guides codesigned by the senior author (CSC) with additions from the qualitative team (CA, AO, LO, FA, MG, JL) (Table S2; Baseline IDI guides attached as Supplemental Material). The theory-informed guides drew on life-stage and health-belief models,29,42–44 as well as social learning theory regarding self-efficacy and stigma,45–53 with an eye toward the grounded theory interpretivist tradition in qualitative research. 54 Including challenges and barriers to both clinic attendance and ART adherence as separate prompts in the guides permitted us to distinguish overlapping and distinct factors within two separate components of the HIV care cascade. All participants provided written informed consent before being interviewed. Interviewers audiorecorded, transcribed, and (as needed) translated the interviews into English for analysis. The translation was then checked by a second reviewer, who read the translated transcript while listening to the original-language audio.
Analysis
A 7-person team (LO, AO, CA, FA, IM, JL, JJP) coded the transcripts in Dedoose using a codebook developed by the full team (coders plus MG and CSC). 55 The codebook incorporated both theory-informed a priori codes, which served as the basis for topic-oriented parent codes, and emergent codes derived from group discussion (with CSC) of a set of inductively coded transcripts. 54 These emergent codes formed the basis of child codes that could capture concepts and phenomena in the data. Regular meetings ensured that individual coders had the opportunity to solicit feedback on any questions that arose during the coding process, thereby achieving intercoder consensus through discussion. The benefit of this approach was that it did not rely on intercoder reliability scores that do not account for “minimal coders” and “maximal coders” (ie, those who include the interviewer question in a code, or who include the previous and following sentences in the coded excerpt). Consensus discussions also clarified for other team members what to attend to in future transcripts, if they had not already encountered similar questions during their coding process.
During an earlier phase of analysis, we pooled data from BL and F1 interviews to identify the challenges and facilitators of HIV care retention among youth in our cohort. We pooled both intervention and control participants in this analysis because we did not seek to identify the intervention's mechanisms of action, but rather to inductively draw out the common perspectives that youth in both arms held about HIV care. Using the code search function in Dedoose on all available BL (n = 135; FC = 32, PC = 20, YC = 83) and F1 (n = 123; FC = 29, PC = 18, YC = 76) transcripts, we exported into MS Excel excerpts from the parent-child code pairs shown in Table 3. The first author <JJP> then conducted a thematic analysis via the rigorous and accelerated data reduction (RaDAR) technique 56 —an iterative and systematic process to reduce excerpts and inductively identify data that responds to a single research question—to identify recurring themes, note the proportion of themes within each code family, and select representative quotes for each emergent theme from the resulting framework tables. For our purposes, we modified the technique to focus solely on exported coded excerpts, rather than the usual pairing of interviewer question-participant response by row; we chose this approach because the volume of data to sift through did not permit reduction of nearly 300 full interviews. After familiarizing ourselves with these excerpts and identifying the main themes, we slowly pared them down to the primary themes identified in the results section. Once youth F2 results became available (n = 40), we compared these with the earlier data to validate that we had achieved data saturation by the close of F1, and that no new themes emerged from the final longitudinal interview with respect to our primary research question for this analysis. The reporting of this study conforms to COREQ guidelines (see Table S4). 57
Results
Below, we decompose the category “retention” into the two main components mentioned above: keeping appointments and engaging in care. While barriers to HIV care were often amplifications or extensions of challenges to keeping appointments (Figure 2), youth treated the two components as qualitatively separate categories, most in evidence in the section on HIV care facilitators and reiterated in their suggestions for improving care. Thus, we maintain the distinction between the 2 components of keeping appointments and engaging in care within the larger themes of challenges, facilitators, and suggestions below. In each case, we present exemplary quotes from either youth or family participants to illustrate these themes. We present additional evidence from these interviews in the Supplemental Table. Age is reported as approximate to the interview date. We did not separate out ART adherence as a separate category, since participants commented on adherence within both appointment-keeping and care engagement domains. Although we interviewed slightly more female participants than male, this reflected the overall distribution of participants in the main study.
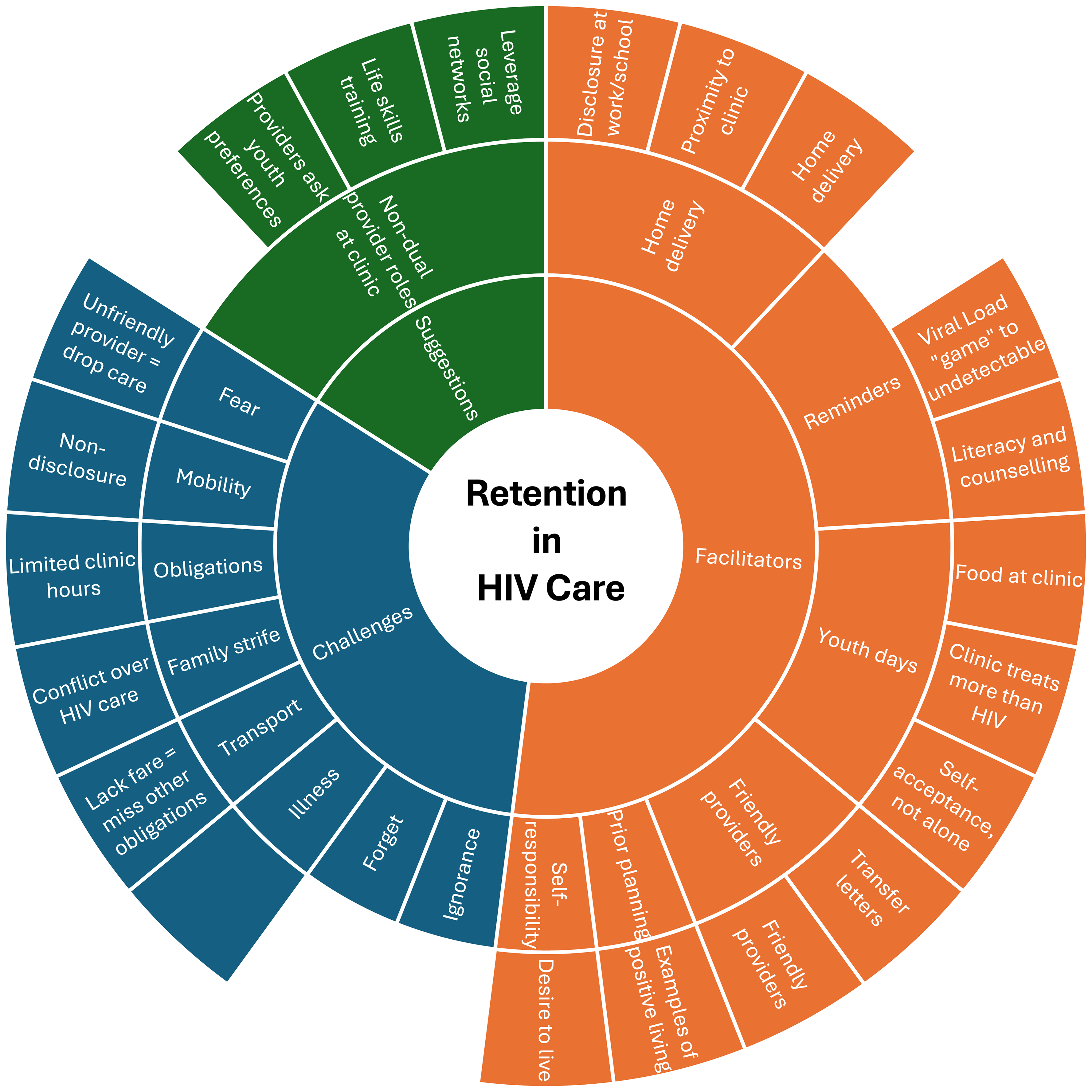
Amplification of Factors by aspect at appointment and engagement levels of care.
We begin with adolescents’ stated reasons for missing appointments before presenting their reports of barriers to engaging in HIV care. We also incorporate providers’ views of these barriers. We then turn to the facilitators of each component before taking up suggestions for increasing engagement in care offered by both adolescents and providers.
Challenges
Missed Appointments. Fear, inclusive of anticipated stigma, was one of the most mentioned reasons adolescents cited for having previously missed appointments. While some feared being seen at the clinic by others, others dreaded providers scolding them or treating them poorly, leading these youth to avoid clinic appointments altogether. This seems to have been a common experience by participants both in and outside the study: When my husband came to the clinic with me, he wished he could get a transfer to come to Y— clinic because there was a provider at S—-town who did not treat him well, and there were times I had to force him to go to the clinic. The providers at this clinic treat people well; I have not had any bad experiences. (20-year-old female, intervention arm, Kenya)
The next most common set of factors involved AYAH's mobility. Some youth had funerals to attend or were traveling with others for longer than anticipated and thus missed previously scheduled appointments. School and work schedules also interfered with making appointments on time, as one guardian explained: “The only challenge he has to keeping his appointment is that he might be in class at the time or doing his exams” (Father of 18-year-old male, intervention arm, Kenya). Though rarely mentioned, some participants also noted domestic instability as a reason for not making their appointments: Although God has been on my side, sometimes we were not born together with our spouses. You may disagree among yourselves. When you disagree, you may run away and forget to take your drugs with you. If that happens to me, though, I usually go to the hospital the next day and explain to them, and they will give me the drugs. (23-year-old female, intervention arm, Kenya)
Participants also cited lack of fare and forgetfulness as reasons for missing clinic appointments, along with fatigue. Fatigue among our participants was due to factors like pregnancy or illnesses, as one woman said: “I was very tired because of the pregnancy and I missed [the appointment] for 2 days.” Occasionally, some youth also lacked knowledge about the importance of care and re-engaged in care only after providers counseled them. “There's some time when I had stopped care, but when the providers counseled more, I was retained back to care” (24-year-old female, intervention arm, Uganda).
HIV Care Barriers
The above factors that led to missed appointments continued to influence HIV care (dis-)engagement but in an amplified and extended form, either as a type of “domino effect” or synergistically combining to create a sense of insurmountable situations. This suggests that the factors surrounding HIV care engagement are already wider in scope than for appointment adherence. An example of such amplification was when poor interactions with providers later led to dropping out of care altogether. As one participant who dropped out of care after three months explained, “a healthcare provider was not friendly to me. His attitude was not that good to me, and he quarreled with me when I went to my clinic” (24-year-old female, intervention arm, Kenya) Lack of fare led some participants to walk to clinic; combined with long wait times, childcare obligations, and a lack of food (especially for young children) at the clinic, also impeded engagement in care.
Importantly, however, several barriers to engaging in HIV care did not coincide with reasons for missing clinic appointments. The three most common of these were, first, conflict with a spouse, cowife, or in-law about engaging in HIV care. One woman said her spouse “told me not to take those drugs while I am in his house, and he does not want to see those drugs in the house” (21-year-old female, control arm, Kenya) The second most common challenge concerned the effects of nondisclosure at the workplace or school, leading to both missed appointments and missed ART doses. In one case, this nondisclosure even followed family encouragement to disclose at work: “He went to work and refused to disclose his problem; he forgot the drugs and went to herd the cattle like that—without the drugs—for a whole month without taking a single pill” (25-year-old male, intervention arm, Uganda). A third set of reasons related to the clinic, such as long queues or hours that didn’t coincide with participant availability. “We are being scheduled over the weekend, and you find that people are so many, and the services may run till late and yet we are supposed to be in school at exactly 2
Providers did not sharply distinguish between challenges to keeping appointments and challenges to engaging in care. However, providers made several observations about adolescents that the youth participants hadn’t mentioned. First, adolescents tended to be selective with their providers and may have preferred interacting with clinicians rather than counselors. Some adolescents are selective; you find that when some come, they would want to be attended to by a specific person. When they find that person is not there or that particular clinician is not around, they will walk away. … But we understand the adolescents, and we do not blame them; we do not judge them for that. (Clinical Officer, Kenya)
Providers also suggested that some youth tended to become forgetful with longer time between ART refills, though they acknowledged the youth overall appreciated streamlined care. Finally, at least two providers in Kenya also cited religious community pressure—that is, belonging to a group whose pastor or congregation recommended “praying the disease away,” as another clinical officer mentioned: “There was another [client not retained] which was also due to religion—they then gave him a herbal concoction and went back to prayer and the client came back to care when he was sick; the other one has declined care to date. They are praying and fasting” (Clinical Officer, Kenya).
Facilitators
Appointment Motivators. Youth described several facilitators for attending clinic appointments, with the most common being appointment reminders. Appointment reminders took various forms, from recording the next clinic date on a card or in a treatment book, to family members keeping track of dates for them. Participants also mentioned reminder calls from the provider or a peer educator, and even using the pill bottle as a reminder—either because the return date was written on the bottle or because the pills had almost run out: “The date is always indicated in the treatment book, sometimes it is written on the pill bottle” (16-year-old male, control arm, Uganda).
An approximately equal number of youth reported intrinsic motivators to keeping their appointments. Many reported a sense of self-responsibility for their health and recognized how attending the clinic was a crucial part of caring for their well-being. While a few mentioned the simple desire to keep their viral load low, some youth mentioned attending clinic to stay alive for their children. As one mother put it, “It's all about the love for my life and that of my child” (18-year-old female, control arm, Uganda).
Buttressing these motivators were separate clinic days for youth and a triage system that served those who came from far away first. Flexible scheduling for day scholars, having prior permission from school authorities to attend clinic appointments, friendly providers, and prior planning on the part of the participant were also factors participants mentioned. These contexts were sometimes brokered by family members: “I talked to the teachers at school, he has his treatment book, so when his appointment day arrives, he is given permission to go get his meds because the health facility is very close to his school” (Paternal grandmother of a 16-year-old male, control arm, Uganda). Finally, participants also appreciated the effect that either being given fare, having alternative modes of transport (eg, a bicycle), or taking up the offer of home delivery of medication, had on their clinic attendance and care engagement.
HIV Care Facilitators. Like with barriers to appointment attendance and engagement in care, HIV care facilitators (inclusive of motivators) showed some overlap with clinic appointment motivators, as well as key differences. The most common response to facilitating engagement in care, slightly exceeding even that of friendly providers, was having familial support and examples. You know, at times, some of the youths have HIV-negative parents, so let us assume that at this age, I am HIV-positive and my mother does not have HIV. You know, with us, the youth, we are stubborn; when such a parent tells you that you should go to the health facility, the youth responds with a lot of anger, “I do not care if I die.” Such stubborn youth may refuse their HIV care. But if the parent is also in the same state, they have to handle you carefully to make sure you are in line. My mother advised me, and I learnt, so I have to take it upon myself to know that this is the day of my appointment. Sometimes I may not have time or feel lazy to go there, so she goes there and picks the meds for me. (18-year-old female, already in care, intervention arm, Uganda)
We interpret such statements as indicative of youth conceiving this support as part of care engagement, extending well beyond mere clinic attendance. Other social examples further widened this category of examples, with youth citing community members and friends giving them examples of healthy living, or teacher and workplace support for attending clinic appointments and picking up medicines from pharmacies. As one woman re-engaging in care reflected, “I no longer have those bad thoughts, because I have seen my friends who were badly off before, but now are healthy after starting HIV care and after receiving enough counseling like the one I received” (21-year-old female, intervention arm—re-engaging in care, Uganda).
Almost as frequently mentioned by youth is the role that friendly, responsive, and respectful providers play in facilitating care engagement. “It's all about the way the providers handle me, they always welcome me with respect, talk to me politely, and then give me my drugs. So, when I reach home, I endeavor to responsibly take my drugs” (19-year-old male, intervention arm, Uganda). This category encompassed immediate provider-patient interaction and prompt service at the clinic, as well as coordination among the providers with respect to particular patients, and a willingness to provide transfer letters to move away from bad providers. “I have benefited from the fact that when I come here, I get my meds in private, and I call it a day. What else do they have to tell me?” (18-year-old female, intervention arm—already in care, Uganda). One participant also found a thank you SMS from providers after having shown up for an appointment as a pleasant motivator: “Since they realized that I am forgetful, they only remind me by sending me an SMS … After coming, they stay a day, then they send me another message to thank me for coming” (23-year-old female, control arm, Kenya). Despite some overlap, these descriptions were much more present among HIV care facilitators than clinic appointment motivators, underscoring the importance of friendly providers for motivating not only ongoing attendance at clinic appointments but also for medication adherence at home. Provider attitude at the clinic “echoes” in participants’ lives after they leave the clinic.
Related to prompt service at the clinic, we found that other clinic-specific relationships also played a part in facilitating care. This could be as broad as living near the clinic (especially for control participants) or desiring to continue care at a clinic where other health concerns were already being addressed, such as ANC clinics or clinics not exclusively focused on HIV. “Interviewer: Why did you have to choose this one of all the health facilities? Participant: It was here where I used to come for my antenatal clinic since it is the nearest of all” (23-year-old female, intervention arm—re-engaging in care, Kenya). Some elements more specific to individual clinics, such as youth days, privacy in the clinic, or weekend hours, also played a role. One spouse observed that before, when his wife's clinic date approached, she “really looked hesitant. But since they separated the youth from the general population, you can really see that she does not have any problem with it” (Spouse of a 17-year-old female, intervention arm—new to care, Uganda).
Almost equally as often mentioned as aspects of a specific clinic was the role played by counseling and health literacy talks. These talks included helping youth come to terms with their status when they seroconverted later in life; aiding in disclosure to others; and emphasizing the importance of taking medication to avoid illnesses and live a healthy life. One peer educator explained that “especially we, the peers, we always try as much as possible to befriend these youths. We may no longer be youths, but we also went through that stage; we understand their challenges. So, we have to befriend the youths as much as possible” (Female peer educator, intervention, Uganda).
Similar to the intrinsic motivators for attending clinic were responses which adverted to a desire to live, avoid illness, or to having a sense of responsibility either for one's own health or to others dependent on oneself (eg, children). Some motivation also came from having seen neighbors default and pass away. We include in this category elements related to stigma reduction, including self-acceptance, not feeling alone, and having the privacy to take medication or possessing a more discreet pill bottle. Together, these social and psychological factors acted synergistically to motivate youth to engage in care by internalizing that care in their daily lives: Providers who are here are the ones who motivated me; they are the ones who encouraged me to start care. I saw many people who were sick, especially from this side. I saw how it affects people, and I did not want it to do the same to me; that is why I decided to take care of my life and my children, who are still young—for them to see me for some time. That is why I try as much as possible to take care of my life. (23-year-old female, control arm, Kenya)
Mentioned about a third as often as the previous groups, home delivery of medication—which seemed related to avoiding stigma by attending clinic—and having a regular schedule for clinic appointments or medication refills were elements that, from a youth perspective, facilitated care. Although in contrast to the most commonly mentioned factors, one participant called private delivery of medication “the most important gesture,” or failing that, meeting the youth in-between, that is, neither at home nor at the clinic, as another youth described: The providers always make an appointment with me in time, and I also plan accordingly. For instance, I have to travel a day before the providers bring me the drugs, I also requested them to leave my drugs with my uncle's wife in case I fail to travel in time. [We meet] at my uncle's home, we always have a free and secret room to meet from. The provider comes on a motorcycle, but he leaves it at a distance, and then walks to my Uncle's home. (21-year-old female, intervention arm—re-engaging in care, Uganda)
Longer refill times and having transportation assistance to the clinic were also factors youth mentioned as helping to engage in care, especially among fishermen whose work can be unpredictable.
With very few mentions, but useful in the context of engagement in care, were three additional facilitators: the “gamification” provided by sharing viral load information with youth as they attempt to achieve undetectable status at successive appointments; outreach by pharmacies—as men tended to avoid clinics but visited pharmacies to manage opportunistic infections; and time to get used to medication once initiated. One provider also mentioned that for perinatally infected youth, early disclosure, beginning at around age 6 and progressively expanding on the specifics of HIV as the child matures, could help them stay engaged in care. Incentives, food, and free care were also occasionally mentioned.
Suggestions
Youth offered multiple suggestions for improving their HIV care that speak to the influence of social networks on care engagement among this age group. These could relate more directly to clinic policies, like requesting providers to ask the patient if the patient already knows the person handling their file, in order to preserve confidentiality around their HIV status, or more broadly to helping youth establish themselves in the world. Some youth floated the idea of allowing friends to pick up ART and suggested that providers could stay in touch with them through their friends. Several youth also mentioned that counseling and ART education, including counseling around disclosure at home, school, and work, could go a long way in helping them engage in care. Others mentioned having programs that could teach marketable or life skills as ways to help improve or buttress HIV care. As one young man put it, “If possible, the organization can give us funding to start some income-generating activities so that we can be able to raise funds to cater for our essential needs” (23-year-old male, intervention arm, Uganda).
Providers generally concurred with the tenor of youth and family suggestions, such as advocating for youth-friendly services at the clinic or providing a place for youth to play games while they waited. Importantly, they also suggested ways to approach youth that target their social perceptions, such as asking young people which clinic days work best for them and what the patient's own preferences for care might be. What I know is the first time a patient comes to the facility for the HIV services, they need to be taken through comprehensive HIV education, and this is what matters throughout the patient's life. This is the point that you also need to talk to them about other social issues that may, in the long run, affect their adherence. So, to me, it is about the first interaction with the patient. (Male clinical officer, Kenya)
Discussion
Youth, as well as adults, living with HIV in rural areas face numerous challenges to initiating and remaining engaged in care.58–60 In this qualitative study, youth described different facilitators to HIV care compared to appointment adherence. We found that AYAH hold a broad concept of HIV care that includes intrinsic social components: familial support; peers and community members giving examples of living positively and educating youth on how to do so; a sense of maturing and shouldering responsibility for oneself or others as part of a community or family; clinic recognition of personal situations (day scholars, long travel distances, youth days); and respectful and attentive providers who could promote a good relationship with the clinic for other aspects of non-HIV-related care.
Thus, rather than defining care quantitatively by statistical measures of appointments kept, intervals between appointments, or prescriptions refilled (all of which are concrete and clinically important outcomes), youth participants suggested that “care” encompassed social components not covered by either clinic or medication adherence alone, and even extended to internalizing HIV care as self-care (Figure 3). Building on Sayegh et al's suggestion that “engagement in care” may reflect a broader concept than “retention in care,” 2 and to better reflect the experience of AYAH in this study, we therefore suggest that “retention in care” and “engagement in care” should be differentiated along lines similar to the way disease (biomedical definition) is contrasted with illness (personal experience) and sickness (social dimension), as described in the introduction. Thus, “retention in care” would equate to clinical measures, while “engagement in care” would encompass the social components and relations of care. Attending to this definition of “engagement in care” can help identify opportunities to further patient-centered care since it broadens the horizon to the patient's lived context.
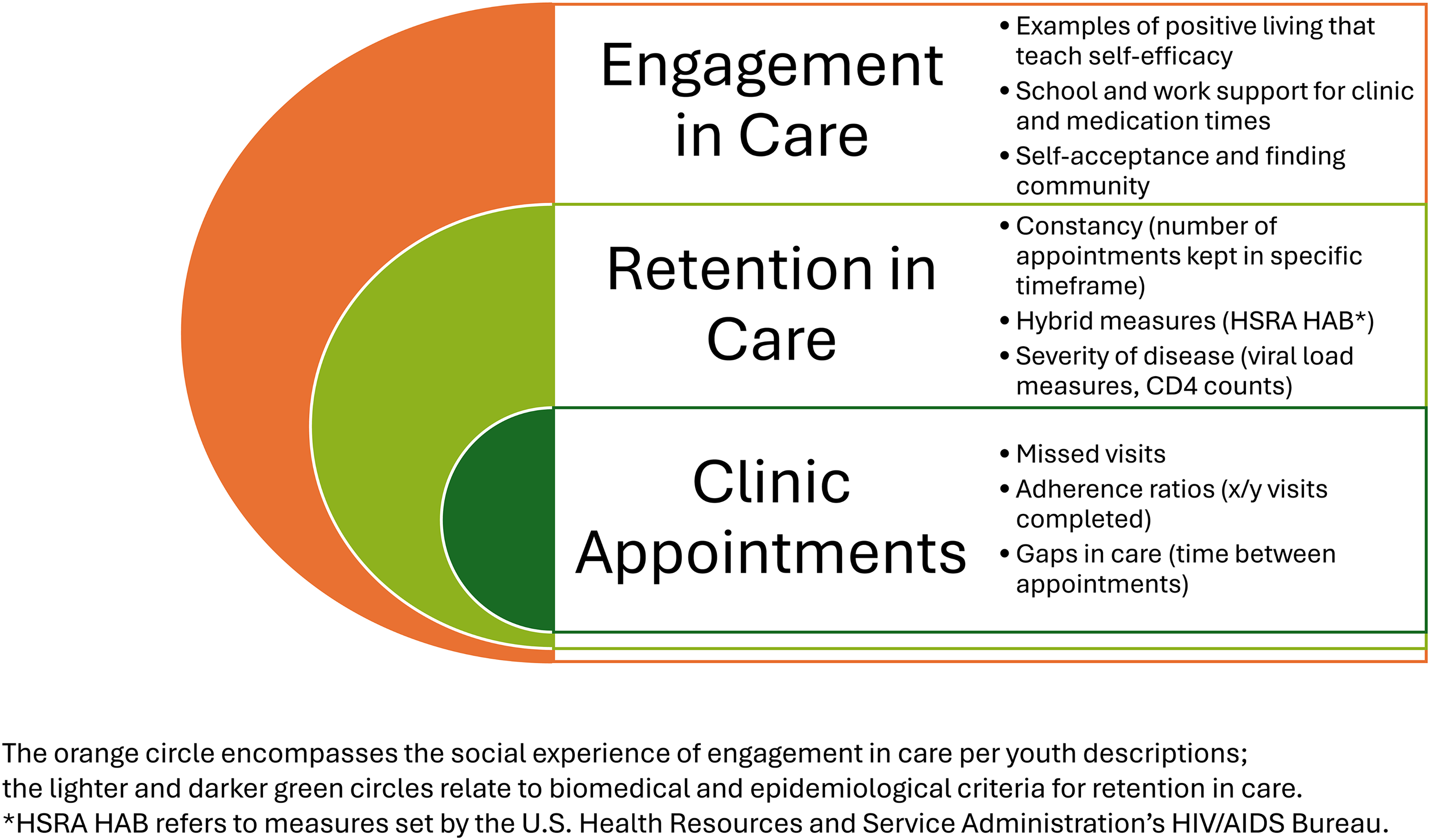
Distinguishing the social and biomedical contents of HIV care.
While virologic suppression and retention rate endpoints remain clinically important, the qualitative findings presented above suggest key insights into additional positive impacts and the potential mechanism of the intervention. First, the qualitative findings described here offer an explanation for Brown et al's and Williams et al's open question about why youth living in households with other members with HIV have higher care engagement and viral suppression than youth living in households without others of the same HIV status.6,11 In our study, family example and support played an outsized role in youth explanations of those factors that facilitated their engagement in care. This supports earlier observations about household roles affecting engagement in care among young women, 15 and grounds other researchers’ advocacy for a household-care-centered approach. 25 Further, our findings support the importance of HIV status disclosure to perinatally-infected youth within family contexts in order to develop the resiliency necessary for care engagement as children become adolescents and pass through additional life stages into early adulthood and beyond. Given that at this life stage, adolescents are highly attuned to social norms and deviations, as well as their own task to create a place in the social world,29,61,62 peer networks also influenced youth's behavior through providing either examples to imitate or avoid, confirming other work on how gendered friendship patterns influence HIV perceptions among youth in East Africa more generally.63,64 Together, these elements of family and peer influence illustrate non-clinical components that youth include in their experience of HIV care engagement.
Correspondingly, while some barriers overlapped, the social contexts of domestic conflict, non-disclosure at the workplace or school, incompatible clinic schedules, and religious pressure impacted care engagement more broadly than simply causing missed clinic appointments, similar to findings from other studies. 65 These barriers may be wrapped up in how participants integrate clinical care into social care, and the ways they choose to prioritize different types of social care over others. Importantly, discussing these life contexts was part of the person-centered care in the intervention arm of the trial, and may therefore point to a potential mechanism behind our previous findings of lower rates of depressive symptoms in that arm of the SEARCH-Youth study. 30 Thus, despite earlier studies looking at clinic attendance as a measure of care engagement, we also argue that it is crucial to distinguish between barriers to appointments and barriers to care, as the latter category is more extensive than the former. Having both socially accessible encouragement with examples of successful engagement in care and provider interactions that carry over into creating a sense of reciprocal responsibility for the youth's health are two facilitators of HIV care that overcome these barriers and go beyond clinic-oriented definitions of engagement in care.
Recommendations. When the barriers to care differ from those to appointment adherence, distinct strategies are called for. Similarly, when the facilitators of appointment adherence and care engagement differ, targeted ways to strengthen those facilitators or incorporate them into clinic practice are often necessary. We found that for AYAH, the quality of clinic-related factors such as prompt service (no long waiting times), empathetic relationships between patients and the clinical team, simple and clear communication, and accessible services also play a role in HIV care, similar to findings about youth disengagement in care in Mozambique. 19 Although the study also rolled out when many facilities in Kenya were adopting a patient-centered care approach, the SEARCH project has shown that patient-centered, “streamlined care” that is welcoming, respectful, and empathetic, by reducing structural barriers and improving relationships with providers, can improve outcomes, both in the care of adults with HIV and in HIV preventative services.11,66–68 SEARCH-Youth further built on this model with additional elements specifically for AYAH, including the life stage assessment and clinical access flexibility, and increased rates of virologic suppression and retention as mentioned earlier. 16
In this respect, provider suggestions for engaging adolescents reflected knowledge of clinic processes and infrastructure, “translating” youth suggestions within the context of current clinic constraints and infrastructural possibilities. One such suggestion was to provide games for youth to play while they wait, alleviating the barrier of long wait times by giving them something to do. Providing a place to do homework or having tutors on hand to help with schoolwork might also be attractive options for more academically inclined or ambitious youth. Ultimately, providers in the SEARCH-Youth study recognized that HIV care, from a youth perspective, includes the patient-provider relationship, household relationships, and peer networks, and not simply ART and appointment adherence alone. 69
Ongoing encouragement and education of family members, including caregivers and spouses, therefore, has an important role to play within the HIV cascade of care for youth and also partly explains the constructive influence that such education has on the surrounding community: education of caregivers can overflow to create supportive, positive effects on HIV care engagement for youth and, ultimately, older adults in rural areas. Social outreach and literacy through the presentation of care engagement examples should therefore be incorporated into the appropriate step of the HIV care cascade and funded appropriately, similar to how community testing campaigns address the first step, precisely because of the repercussions these social networks have on engagement and retention in care.
Limitations and Strengths. Our study has some limitations. One limitation is that combining both control- and intervention-arm youth in this comprehensive analysis means that facilitators unrelated to the intervention are over-represented and thus given more weight. Youth interviewees may have been subject to both social desirability and authority biases when discussing the part played by their caregivers and providers, while family and providers may have also displayed some social desirability bias. Nonetheless, a strength of the study is its longitudinal design, which allowed youth to become accustomed to person-centered care and to offer considered insights after reflecting on their experiences. Although our data collection overlapped with the COVID pandemic, and the resulting changes in care delivery may have altered the treatment landscape, some evidence exists that pre-existing systems of care proved resilient through the pandemic lockdowns.28,40
Because the study was conducted in rural Kenya and Uganda, it may not be applicable in urban areas or in areas outside East Africa. Even so, sub-Saharan Africa continues to make great strides in reducing HIV transmission and mortality and is no longer the region where most new HIV infections are occurring.70,71 Other regions, therefore, stand to benefit from lessons learned by interventions that have succeeded in Africa, especially those that address certain key populations, such as adolescents, young adult women, and men who have sex with men (MSMs), who remain more vulnerable than others on the continent.15,72 Although the challenges that adolescents face are often unique to their age group, the challenges associated with establishing oneself in the world, finding viable employment, and starting new families are also commonly faced by migrants, refugees, and other displaced populations, as well as vulnerable populations more generally, all of whom face disruptions in medical care continuity and potential barriers to optimal HIV care engagement. In this regard, our findings that youth distinguish between engagement in care and retention in care have implications for intervention measurements, suggesting that including questions asking how participants define HIV care for themselves and their peers may reveal opportunities for future interventions to address.
Finally, we did not include adherence in this article out of space concerns; future studies might examine how adherence fits within the umbrella category of engagement in care for a more holistic view of the individual components and the interaction between, or differences among, the barriers and facilitators of each element of care.
Conclusions. The qualitative results described here, from participants in both intervention and control settings, shed important general insights into how AYAH in these regions of rural SAA perceive HIV care. Youth implicitly distinguished between simply keeping appointments (“retention in care”) and caring about oneself with a feeling of sharing that commitment to health in conjunction with family and provider investment in their health (“engagement in care”). Implementing the suggestions youth and providers offered to account for the distinction between clinic values and patient-identified elements of person-centered care may have downstream effects beyond HIV care engagement, potentially improving the lives of youth and local economies more broadly.
Supplemental Material
sj-docx-1-jia-10.1177_23259582261457320 - Supplemental material for Retaining Versus Engaging Youth in HIV Care: Perspectives From a Qualitative Study among Youth Living With HIV and Their Care Providers in Kenya and Uganda
Supplemental material, sj-docx-1-jia-10.1177_23259582261457320 for Retaining Versus Engaging Youth in HIV Care: Perspectives From a Qualitative Study among Youth Living With HIV and Their Care Providers in Kenya and Uganda by Jason Johnson-Peretz, Angeline Onyango, Cecilia Akatukwasa, Fredrick Atwine, Lawrence Owino, Marilyn Nyabuti, Janice Litunya, Jane Kabami, Elizabeth Bukusi, Florence Mwangwa, Moses R. Kamya, Diane V. Havlir, James Ayieko, Theodore Ruel and Carol S. Camlin in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-pdf-2-jia-10.1177_23259582261457320 - Supplemental material for Retaining Versus Engaging Youth in HIV Care: Perspectives From a Qualitative Study among Youth Living With HIV and Their Care Providers in Kenya and Uganda
Supplemental material, sj-pdf-2-jia-10.1177_23259582261457320 for Retaining Versus Engaging Youth in HIV Care: Perspectives From a Qualitative Study among Youth Living With HIV and Their Care Providers in Kenya and Uganda by Jason Johnson-Peretz, Angeline Onyango, Cecilia Akatukwasa, Fredrick Atwine, Lawrence Owino, Marilyn Nyabuti, Janice Litunya, Jane Kabami, Elizabeth Bukusi, Florence Mwangwa, Moses R. Kamya, Diane V. Havlir, James Ayieko, Theodore Ruel and Carol S. Camlin in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgments
We want to thank our participants, the communities that host our study, local clinic personnel and staff. In particular, we would like to acknowledge Joi Lee and Monica Getahun for their contribution to project management and coding of data. We also thank the Prevention and Treatment through a Comprehensive Care Continuum for HIV-affected Adolescents in Resource Constrained Settings (PATC3H) consortium (![]() ), of which this study was a part.
), of which this study was a part.
Ethical Approvals
We obtained written informed consent from all participants prior to interviewing them. National guidelines in Kenya and Uganda do not require parental consent to participate in research if youth have a sexually transmitted disease, including HIV, and are over the age of 12 (Kenya) or 14 (Uganda). The Kenya Medical Research Institute (KEMRI, 3834), the Makerere University School of Medicine Research and Ethics Committee (REC REF 2019-014), the Uganda National Council of Science and Technology (UNCST, HS 2542), and the University of California San Francisco (UCSF) Committee on Human Research (18-25703) all approved the SEARCH-Youth study.
Additional Declarations
We obtained informed written consent from all participants.
Author Contributions
JJP conceived and wrote the article. CSC edited and contributed to various sections of the manuscript. CA, FA, AO, and LO gathered data, translated, and transcribed the interviews and gave feedback on data analysis and interpretations. Coding of transcripts was done by CA, FA, AO, LO, IM, JL, and JJP. CA, FA, AO, LO, IM, JL, JJP, and CSC participated in and contributed to overall data analysis and theme identification. All authors approved the final article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by a grant from the National Institutes of Health/National Institute of Child Health and Human Development (Grant Number UG3 HD06915-01; Eunice Kennedy Shriver National Institute of Child Health and Human Development). The views in this article do not necessarily reflect those of the funders.
Declaration of Conflicting Interests
The authors declare no conflict of interest. The sponsors had no role in the design, execution, interpretation, or writing of the study. EB has provided scientific advisory for MSD and has an MSD-funded clinical treatment trial; she has also been involved in scientific conference presentations for ViiV and coached young talents for the LOREAL Foundation.
Data Availability Statement
Source data are transcribed and translated interview data, which require redaction to protect confidentiality. Following SEARCH Scientific Review Committee approval of a concept sheet that includes a summary of proposed analyses, we can make available deidentified study data and a data dictionary via a secure online repository and a signed data access agreement. Please direct further inquiries to the SEARCH Scientific Review Committee via Douglas.Black@ucsf.edu
Author Position Statement
We ground our team-based analytical approach in team members’ cultural experience and first-hand understanding of the study setting (AO, CA, FA, LO). These research team members were involved in the entire analytical process from data gathering in local languages (Dholuo—LO, AO; Runyankole—CA, FA; Swahili—AO), participating in data analysis and confirming the findings of additional team members (JJP, CSC). Such cultural rigor helps ensure that data interpretation respectfully captured participants’ voices. Given the linguistic capacity of team members (JJP) and to surmount colonially-derived linguistic barriers between regions and nation-states in Africa, we have committed to citing at least one source from Francophone Africa and one from Lusophone Africa in our articles. Even with these practices in place, we recognise the relativity of our analysis and the possibility of contested interpretations.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.