
Abstract
Background
Human immunodeficiency virus (HIV) disproportionately affects young Nigerian women, yet testing uptake remains suboptimal. This study identified individual- and community-level determinants of HIV testing among this demographic to guide targeted healthcare interventions.
Methods
A secondary analysis of the 2024 Nigeria Demographic and Health Survey (NDHS) was conducted (N = 14,634, ages 15-24). Multilevel logistic regression models were applied to account for the hierarchical data structure, with Model III (the full model containing both individual and community-level covariates) demonstrating the best fit based on Akaike information criterion and Bayesian information criterion.
Results
The prevalence of HIV testing among young women in Nigeria was 21.3%. The multilevel logistic regression analysis revealed that key individual-level factors significantly associated with higher odds of HIV testing included advanced age category, higher educational status, higher wealth index, high individual media exposure, comprehensive HIV knowledge, and a history of sexually transmitted infections. Additionally, marital status was a strong predictor, with married and formerly married women exhibiting significantly higher odds of testing compared to their never-married peers. At the community level, living in communities with high community-level HIV knowledge and high community wealth significantly boosted testing practice. The intraclass correlation coefficient in the null model indicated that 19.0% of the total variance in HIV testing practice was attributable to community-level factors, confirming a notable neighborhood effect.
Conclusion
HIV testing practices among young Nigerian women are multidimensionally shaped by a prominent “neighborhood effect” alongside individual socioeconomic and marital status. To bridge the current implementation gap in Nigeria, clinical and public health interventions must transition toward decentralized, community-based testing models that intentionally reach out to younger, never-married, and socioeconomically disadvantaged women.
Introduction
Globally, young people aged 15 to 24 years remain disproportionately affected by the human immunodeficiency virus (HIV) epidemic, with Sub-Saharan Africa (SSA) bearing the most significant burden. 1 Of all young women living with HIV worldwide, ∼80% reside in SSA, highlighting a critical gender and regional disparity. 2 Nigeria, as the most populous nation in Africa, face a substantial challenge in controlling the epidemic among its youth. 3 Despite national efforts, a significant proportion of sexually active young women in Nigeria remain unaware of their HIV serostatus, leading to high rates of undiagnosed infections and continued transmission. 4
Identifying 95% of people living with HIV (PLHIV) is the first and most crucial pillar of the UNAIDS and Nigerian Federal Ministry of Health targets. 5 Achieving this goal relies entirely on scaling up HIV testing practices. Timely HIV testing is the gateway to early diagnosis, enrollment in antiretroviral therapy (ART), and a reduction in HIV-related mortality and transmission. Furthermore, testing serves as a vital entry point for HIV-negative individuals to access prevention services and maintain their negative status. 6
Evidence from past population-based surveys suggests that HIV testing uptake remains suboptimal among Nigerian youth. 5 While recent summary reports from 2024 indicate improvements, a large segment of the young female population has never been tested, implying that many seropositive individuals are unaware of their status. 7 Identifying the specific barriers and facilitators to testing is, therefore, essential to improving health-seeking behaviors among these high-risk age groups.
Previous studies have identified factors such as age, residence, educational status, wealth index, and HIV knowledge as determinants of testing.8‐10 However, these factors vary significantly across different socio-cultural contexts. In Nigeria, while studies have focused on general reproductive-age women, there is limited updated information specifically addressing the intersection of gender-based violence and educational attainment as structural barriers for the youth population. 11 Most existing research has not adequately addressed how domestic violence, a pervasive issue in the region, inhibits the autonomy of young women to seek testing.
Furthermore, nationwide information reflecting the postpandemic landscape is required to accelerate progress toward the “95-95-95” goals in the country. 12 Therefore, this study aimed to identify the barriers and facilitators for HIV testing practice among young women (15-24 years) in Nigeria using data from the 2024 Nigeria Demographic and Health Survey (NDHS). The findings are intended to inform policymakers in designing age-specific and gender-sensitive interventions to close the testing gap.
Method
Study Design and Setting
This study constitutes a secondary analysis of a cross-sectional, community-based national survey. The investigation was conducted utilizing data from the Federal Republic of Nigeria, which comprises 36 states and the Federal Capital Territory, traditionally grouped into six distinct geopolitical zones. The primary fieldwork and data collection for the 2024 Nigeria Demographic and Health Survey (NDHS) were carried out during the official nationwide Period of study designated by the National Population Commission (NPC), spanning from early 2024 through its field completion.
Inclusion and Exclusion Criteria
Inclusion Criteria
The targeted study population was bounded strictly to young women aged 15 to 24 years who were permanent residents or visitors in the selected households on the night preceding the survey, and who successfully completed the standard individual Women's Questionnaire within the 2024 NDHS.
Exclusion Criteria
Women outside the specified youth demographic bracket (such as adolescents aged <15 years or adult women aged 25-49 years) were excluded from this analysis. Furthermore, respondents with missing or incomplete information for the primary outcome variable (ever tested for HIV) or missing observations for the core mandatory analytical covariates (such as educational status, wealth index, marital status, or media exposure parameters) were excluded from the final analytical sample.
Data Source and Sampling Technique
The empirical data for this study were extracted from the individual Women's Recode (IR) file of the 2024 NDHS, a nationally representative health survey managed globally by the DHS Program. The primary survey was mathematically optimized to yield reliable, high-quality population and health indicators across national, zonal, and state boundaries.
To achieve a representative national sample, the 2024 NDHS utilized a rigorous, stratified two-stage cluster sampling design. In the primary sampling stage, a total of 1400 enumeration areas or clusters (consisting of 701 urban and 699 rural localities) were selected from the national census sampling frame using a systematic sampling technique with a probability proportional to the cluster size. In the secondary sampling stage, a fixed quota of 30 households per cluster was selected via simple random sampling from the newly updated household listing.
Primary data collection was executed by trained field personnel using a structured, interviewer-administered questionnaire. Comprehensive quality control measures were implemented during the primary survey, including instrument pretesting, rigorous technical training for data collectors, and close on-site monitoring by field supervisors. After filtering the raw records to target the youth cohort and applying complex survey sample weights, a final analytical sample of 14,634 young women aged 15 to 24 years was yielded (Figure 1).
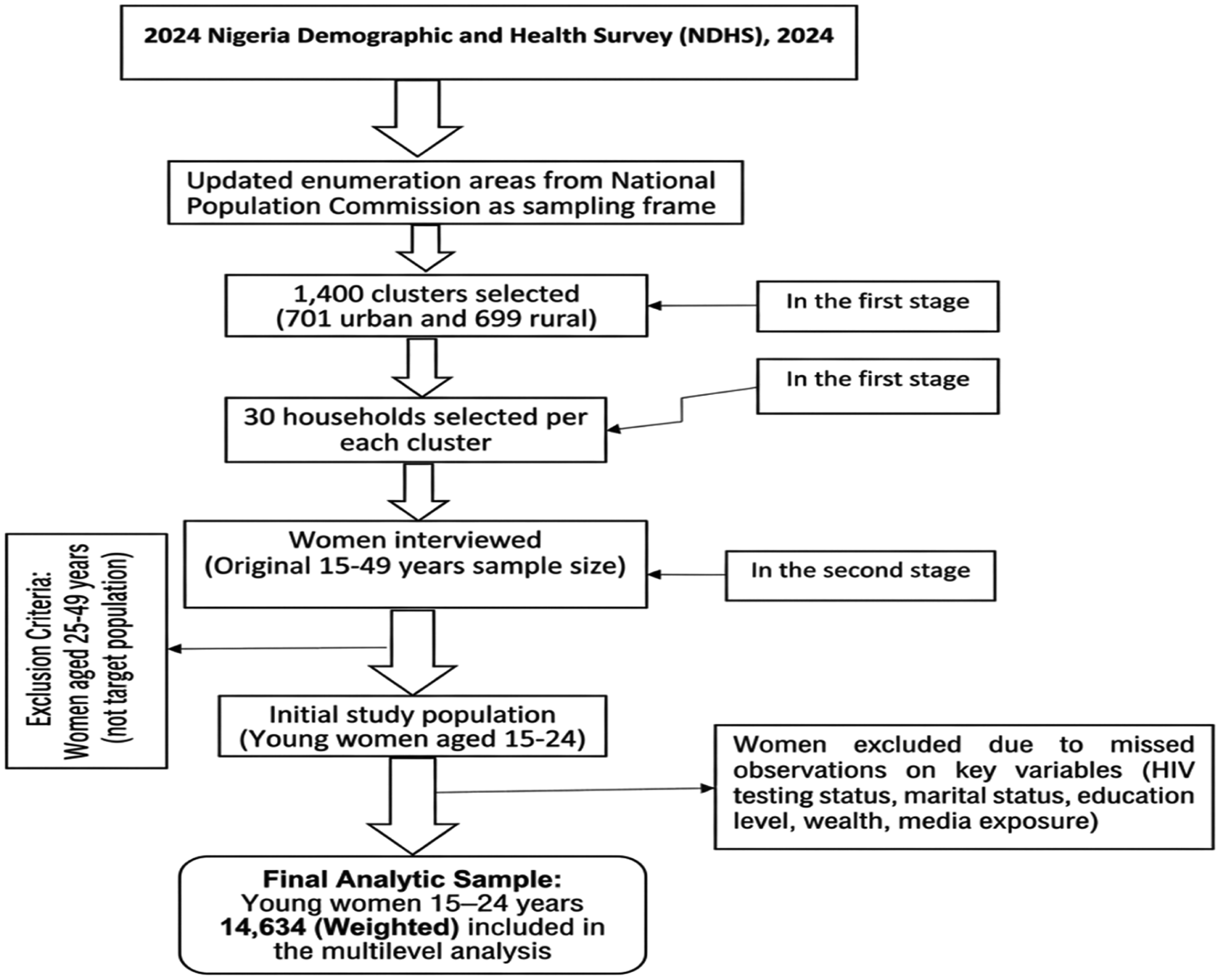
Flowchart of Nigerian Demographic and Health Survey sampling procedure and data extraction.
Operationalization of Study Variables
The Dependent (Outcome) Variable
The primary outcome variable for this investigation was HIV testing practice. This behavioral metric was operationalized using self-reported data from the individual Women's Questionnaire. Respondents were asked the foundational question: “Have you ever been tested for HIV?” To facilitate multivariable multilevel logistic regression analysis, the responses were transformed into a distinct binary outcome, coded as follows:
0 (no): Denoting young women who had never undergone an HIV test in their lifetime. 1 (yes): Denoting young women who had been tested for HIV at least once.
Independent (Explanatory) Variables
To accurately capture the structural hierarchy of the 2024 NDHS dataset and evaluate the presence of contextual neighborhood phenomena, the independent variables were categorized into two analytical strata: individual-level factors (Level-1) and community-level factors (Level-2).
Individual-Level (Level-1) Covariates
Level-1 factors comprised the demographic, socioeconomic, and behavioral characteristics specific to each respondent. These included:
Age bracket: Categorized into two developmental cohorts: adolescents aged 15 to 19 years and young adults aged 20 to 24 years. Marital status: Structured into six distinct groups to evaluate relational dynamics: never in a union, currently married, living with a partner, widowed, divorced, or separated. Educational attainment: Stratified into four incremental levels reflecting academic exposure: no formal education, primary education, secondary education, or higher education. Household Wealth Index: Operationalized using the standard DHS asset-based quintiles, grouping respondents into five distinct wealth strata: poorest, poorer, middle, richer, and richest. Type of residence: Divided geographically based on the respondent's residential location into urban or rural settings. Comprehensive HIV/AIDS knowledge: Dichotomized as a binary parameter (yes vs no) measuring whether the respondent possessed correct scientific knowledge regarding transmission, prevention, and common misconceptions about the virus. HIV/AIDS-related stigma: Categorized into a binary response (yes vs no) indicating whether the respondent endorsed stigmatizing attitudes or discriminatory beliefs toward people living with HIV/AIDS.
Community-Level (Level-2) Covariates
Level-2 factors were designed to capture the structural and normative characteristics of the broader social environment. Because the NDHS dataset does not inherently collect structural parameters at the community level, these explanatory variables were constructed by aggregating the specific Level-1 individual characteristics within each primary sampling unit (PSU/cluster).
Community wealth level: This structural parameter was derived by calculating the mean concentration of household wealth indices within each distinct cluster. Community media exposure: This variable captures the neighborhood communication infrastructure, operationalized as the proportion of young women within the cluster who reported regular exposure to at least one form of mass media (specifically radio, television, or newspapers).
To facilitate objective evaluation in the multilevel regression models and minimize collinearity, both community-level parameters were transformed from continuous variables into binary factors (low vs high). The national sample median across all clusters was utilized as a standardized statistical cut-off threshold; clusters tracking below the national median were classified as “low,” while those scoring at or above the median were categorized as “high.”
Statistical Analysis
Prior to conducting inferential analyses, the dataset was cleaned, checked for completeness, and weighted. Sampling weights were strictly applied during the computation of descriptive and inferential statistics to adjust for nonproportional sample allocation across different states and urban/rural strata, ensuring the national representativeness of the findings. All data management and statistical processing were executed using Stata version 17.0 software.
Due to the nested data structure (individual young women clustered within 1400 distinct communities), standard logistic regression models would violate the assumption of independent observations, leading to underestimated standard errors and overinflated type I errors. Therefore, multivariable multilevel logistic regression models were applied.
Four sequential models were constructed to evaluate the predictors of HIV testing practices:
Null model (empty model): Contained no explanatory variables and was used to calculate baseline community random intercept variance. Model I: Adjusted exclusively for individual-level (Level-1) covariates. Model II: Adjusted exclusively for community-level (Level-2) covariates. Model III (full model): Simultaneously adjusted for both individual- and community-level covariates.
Model selection and goodness-of-fit were rigorously evaluated using the Akaike information criterion (AIC) and the Bayesian information criterion (BIC). The model yielding the lowest AIC and BIC values (Model III) was selected as the best-fitting model to interpret the final measures of association.
Variables demonstrating a liberal association (P < .20) in the bivariable multilevel analysis were advanced into the final multivariable models. The strengths of associations were reported as adjusted odds ratios (AOR) alongside their corresponding 95% confidence intervals (CIs). Statistical significance was defined using a standardized, two-decimal P-value threshold of P ≤ .05, with highly significant minimal values explicitly denoted as P < .01.
To measure random effects and cluster-level variation, the intraclass correlation coefficient (ICC), median odds ratio (MOR), and proportional change in variance (PCV) were computed. Crucially, in nonlinear probability models like multilevel logistic regression, the individual level-1 residual variance is mathematically fixed to π2/3 ≈ 3.29. When powerful individual-level covariates are added to the model, the underlying scale of the latent variable changes. This rescaling artifact can artificially expand the community-level variance estimate (σ2), which can yield negative mathematical percentages when calculating PCV via traditional linear equations. Where this occurs, it indicates a data structure artifact driven by individual-level adjustments rather than statistical error, and is interpreted accordingly.
Ethical Considerations
This study represents a secondary analysis of a fully de-identified, publicly available dataset. The primary protocol for the 2024 NDHS was reviewed and officially approved by the National Health Research Ethics Committee of Nigeria (NHREC) and the Institutional Review Board of ICF International, ensuring adherence to international standards for human subject protection. Informed consent was obtained from all participants (or parents/guardians in the case of minors) by the primary field teams before any interviews were administered. The authors obtained official authorization from the DHS Program to access, download, and analyze the data for scientific research. Because the data are fully anonymized and aggregated, additional primary institutional review board approval from the authors’ home institution was not required.
Results
Socio-Demographic and Economic Profiles of Respondents
The final weighted analytical sample encompassed a total of 14,634 young women within the primary reproductive and youth demographic age bracket of 15 to 24 years. Cross-tabulation of life-stage characteristics against lifetime diagnostic uptake demonstrated a clear disparity across geographic and academic strata. With respect to environmental settings, young women residing in urban clusters exhibited a higher lifetime HIV testing rate at 22.73% (representing 1589 respondents) than their counterparts in rural localities, who tracked a testing prevalence of 19.97% (representing 1526 respondents). Educational attainment acted as a strong axis of stratification; only 16.07% of young women who lacked any formal schooling had ever undergone HIV diagnostic screening. Conversely, a prominent majority (41.14%) of respondents who achieved higher education had successfully accessed HIV testing services.
Household wealth quintiles also played an undeniable structural role in determining healthcare-seeking behavior. Young women belonging to the most economically secure households (the richest quintile) demonstrated nearly double the testing uptake at 25.79% compared to the most economically marginalized cohort (the poorest quintile), where lifetime testing prevalence dropped to a minimal 13.19%.
Behavioral, Cognitive, and Health-Related Covariates
The descriptive analysis revealed a pronounced positive association between health literacy, sexual behavioral patterns, and active clinical engagement. In terms of cognitive determinants, young women who demonstrated comprehensive scientific knowledge regarding HIV transmission routes, prevention strategies, and common societal misconceptions achieved a lifetime testing rate of 30.84% (or ∼30.8%). In sharp contrast, only 17.12% (∼17.1%) of those tracking limited or low comprehensive HIV awareness had ever participated in diagnostic screening.
The influence of sexual risk profiles and clinical markers was equally evident. Assessment of behavioral indicators showed that over one-third (35.58%) of young women who reported having one or more sexual partners within the preceding 12 months had been tested for HIV. Conversely, testing uptake plummeted to just 7.99% among youth who reported no active sexual partners during the same tracking period.
Finally, experiencing a syndemic reproductive health condition emerged as a primary catalyst for clinical testing encounters. Nearly half (43.31%) of the young women who documented having an active sexually transmitted infection (STI) within the past 12 months had been screened for HIV. In comparison, the prevalence of lifetime testing was less than half that rate among respondents who did not experience an underlying STI in the previous year, tracking at only 20.29% (Table 1).
Background Information of Participants (N = 14,634).

Note: Total N = unweighted count; (%) = weighted percentage. HIV, human immunodeficiency virus; STI, sexually transmitted infection. Overall testing prevalence: 21.3% (n = 3115).
Random Effects Measures and Neighborhood Variation
To evaluate the presence of contextual neighborhood clustering and confirm the statistical necessity of an advanced hierarchical model over standard single-level modeling, a random intercept variance analysis was systematically conducted (Table 2).
Random Effect Analysis and Model Fitness (N = 14,634).

Note: Negative PCV values in nonlinear multilevel logistic regression configurations result from the statistical rescaling effect of the latent variable upon the addition of powerful individual-level covariates, which expands the community-level variance estimate relative to the fixed individual-level-1 residual variance (π2/3 ≈ 3.29).
Model III represents the final best-fitting model based on the lowest AIC and BIC.
In the baseline null model (the empty model excluding all fixed covariates), the community-level variance intercept (σ2) was estimated at 0.616. The corresponding baseline ICC revealed that15.8% of the total variation in lifetime HIV testing practice among young Nigerian women was directly attributable to unobserved structural or contextual differences across the primary sampling units (clusters), rather than individual-level attributes alone.
Following the simultaneous adjustment for both individual- and community-level characteristics in the final multivariable model (Model III), the community-level variance parameter stabilized at 0.772 (95% CI: 0.640, 0.931). The resulting final ICC expanded to 19.0%, demonstrating that after fully accounting for the complex array of socio-demographic, economic, and behavioral factors, nearly one-fifth (19%) of the residual variation in HIV screening compliance is structurally driven by the residential context.
The computed MOR further quantified the magnitude of this neighborhood effect. In the final adjusted configuration (Model III), the MOR was estimated at 2.31. This implies that if a young woman were to randomly move from a community characterized by low diagnostic coverage to a community with high coverage, her median odds of undergoing an HIV test would increase by 2.31 times based entirely on the collective normative influences of her new residential area.
Crucially, while moving from the Null Model to Model III, the apparent increase in community-level variance (σ2 from 0.616 to 0.772) led to negative Proportional Change in Variance calculations (specifically −25.2% in the final model). In multilevel logistic regression configurations, the individual-level (Level-1) residual variance is mathematically fixed to π2/3 ≈ 3.29. The addition of powerful Level-1 covariates shifts the underlying scale of the latent variable, creating a rescaling artifact that expands the community-level random intercept variance estimate. This represents a recognized data structure artifact typical of nested categorical models rather than calculation errors, confirming that individual attributes strongly differentiate neighborhood-level testing thresholds.
Model Fit and Selection Diagnostics
Model suitability, fitness, and explanatory power were rigorously cross-examined using information criteria diagnostics and log-likelihood iterations. Model III established the strongest overall data fit, as demonstrated by achieving the lowest numerical parameters for both the AIC = 11,270.96 and the BIC = 11,468.33 across all tested iterations.
Finally, a formal likelihood ratio (LR) test was executed to compare the hierarchical model against an ordinary single-level logistic regression model. The LR test yielded a highly significant chi-square value (χ2 = 339.04, P < .01). This definitive statistical boundary confirms that the nested multilevel logistic regression framework provides a significantly superior fit for the 2024 NDHS dataset, successfully accounting for the data hierarchy and preventing the underestimation of standard errors.
Fixed Effects Analysis: Determinants of HIV Testing Practice
Model Integration and Selection Baseline
As operationalized in the methodology, a sequential series of four hierarchical regression iterations were systematically fitted to evaluate the predictors of lifetime HIV screening: the empty Null Model, Model I (adjusting solely for individual-level-1 factors), Model II (adjusting solely for community level-2 factors), and Model III (the fully saturated model combining both analytical strata). Among these, Model III exhibited the superior data fit based on tracking the lowest numerical values for both information criteria tests (AIC = 11,270.96; BIC = 11,468.33).
Consequently, fixed-effects interpretations were derived exclusively from Model III. In this final fully adjusted model, respondent age group, number of sexual partners, individual media exposure, comprehensive HIV literacy, lifetime history of sexually transmitted infections (STIs), maternal household wealth index, formal educational attainment, marital configuration, community-level HIV knowledge, and community-level wealth strata emerged as statistically significant determinants of HIV testing practices among young women in Nigeria (P ≤ .05).
Individual-Level (Level-1) Socioeconomic and Demographic Predictors
A profound, positive incremental gradient was observed between formal schooling and clinical diagnostic engagement. Young women who achieved primary, secondary, or higher educational attainment demonstrated1.66 times (95% CI: 1.32, 2.09), 2.55 times (95% CI: 2.10, 3.10), and 7.13 times (95% CI: 5.50, 9.25) significantly higher odds of utilizing HIV testing services, respectively, relative to their baseline peers who lacked any formal education (P < .01).
Similarly, the household wealth index functioned as a strong structural driver of service uptake. Compared to young women belonging to the most economically marginalized households (the poorest quintile), those situated in the poorer (AOR = 1.62; 95% CI: 1.32, 1.98), middle (AOR = 2.01; 95% CI: 1.60, 2.52), richer (AOR = 2.58; 95% CI: 1.97, 3.36), and richest (AOR = 2.71; 95 CI: 2.02, 3.63) wealth strata exhibited step-wise, significantly increased likelihoods of accessing diagnostic screening (P < .01).
Age category served as a key demographic predictor; young adults transitioning into the older youth cohort (ages 20-24) exhibited 1.88 times higher odds of testing (95% CI: 1.67, 2.12) than adolescents in the younger age group (ages 15-19, P < .01).
Marital configuration emerged as the single most powerful individual fixed effect in the model. When compared directly against never-married young women, the odds of undergoing an HIV test were over sevenfold higher among respondents who were currently married or cohabiting with a partner (AOR = 7.21; 95% CI: 6.08, 8.55), and escalated to over eightfold among young women who were formerly in a union, such as those who were widowed, divorced, or separated (AOR = 8.62; 95% CI: 5.79, 12.83, P < .01).
Individual Behavioral and Cognitive Facilitators
Enabling cognitive and communication factors substantially boosted proactive health behaviors. Young women possessing a comprehensive scientific understanding of HIV prevention modalities and transmission pathways had significantly higher odds of testing (AOR = 1.61; 95% CI: 1.43, 1.80) compared to those hampered by limited or low health literacy (P < .01). Regular individual exposure to mass media communication platforms functioned as a similar facilitator, increasing the likelihood of testing uptake by 1.48 times (95\% CI: 1.27, 1.72, P < .01).
Furthermore, experiencing an underlying reproductive health vulnerability served as an immediate clinical trigger; young women who reported contracting a STI within the preceding 12 months were 1.35 times more likely to have completed an HIV test (95% CI: 1.09, 1.66, P = .01) than those who remained free of STIs during the same timeframe.
Contextual Community-Level (Level-2) Predictors
At the macro-environmental level, the surrounding neighborhood context exerted a significant independent influence on youth behavior even after adjusting for all individual characteristics. Living within a cluster characterized by high collective community-level HIV knowledge significantly normalized clinical engagement, resulting in 1.43 times higher odds of diagnostic testing among residents (95% CI: 1.21, 1.68, P < .01).
Intriguingly, high community-level wealth demonstrated an inverse relationship with the outcome variable after stringently controlling for individual-level wealth quintiles; young women residing in collectively wealthier clusters had lower odds of utilizing testing services (AOR = 0.72; 95% CI: 0.56, 0.93, P = .01). Finally, macro-level aggregate parameters for community media exposure, collective literacy thresholds, and localized institutional stigma failed to cross the threshold for statistical significance in the final multivariable model, indicating that their influences were largely absorbed by individual-level characteristics (Table 3).
Multilevel Mixed-Effects Logistic Regression Analysis of Factors Associated With HIV Testing Practice (N = 14,634).

Note: AOR, adjusted odds ratio; CI, confidence interval. Odds ratios > 1 indicate increased likelihood of testing; < 1 indicate decreased likelihood. Significant P-values (P < .05) are highlighted in bold.
Discussion
The HIV Testing Prevalence Gap: Implementation Versus Practice
In strict alignment with the ambitious UNAIDS Fast-Track mandates and the corresponding Nigerian National Strategic Plan, achieving epidemic control is fundamentally predicated on ensuring that 95% of PLHIV are fully aware of their serostatus. However, the empirical findings from this nationally representative analysis of 14,634 young women illuminate a stark implementation-to-practice chasm. With an overall lifetime HIV testing prevalence of just 21.3% among this highly vulnerable youth demographic (ages 15-24), the reach of current diagnostic infrastructure remains critically suboptimal and drastically below the minimum threshold required to systematically interrupt ongoing transmission networks. 13
When contextualized within the wider epidemiological landscape of SSA, Nigeria's diagnostic coverage for young women lags significantly behind several regional peers. Comparative demographic analyses from East African nations, such as Uganda and Rwanda, frequently document youth testing rates hovering between 50% and 60%. 14 This pronounced performance disparity implies that Nigeria's conventional reliance on passive, facility-bound clinical testing pathways fails to resonate with the youth demographic. Conversely, the successes observed in East Africa underscore the utility of aggressive, decentralized, community-anchored, and peer-led mobile diagnostic campaign modalities that have yet to be universally brought to scale within the Nigerian healthcare apparatus.
Our random-effects analysis provides a rigorous mathematical explanation for this implementation bottleneck. The highly significant community-level variance (σ2 = 0.772) and a notable MOR (MOR = 2.31) demonstrate that a young woman's interaction with diagnostic services is not an isolated or random occurrence. Instead, her healthcare-seeking behavior is profoundly structured by the specific residential cluster in which she resides. This potent “neighborhood effect” indicates that a young woman's probability of knowing her HIV status is tightly bound to local geographical, cultural, and structural environments. Consequently, public health interventions that focus exclusively on individual-level behavioral modifications while ignoring cluster-level constraints will remain fundamentally limited in their capacity to bridge the testing gap.
The Maturation and Life-Stage Effect
A primary individual-level driver identified in this investigation is the clear “maturation effect.” Young adults aged 20 to 24 exhibited substantially higher odds of utilizing HIV testing services (AOR = 1.88) than their younger, adolescent counterparts aged 15 to 19. This developmental discrepancy aligns with contemporary behavioral literature from other SSA settings, including Ethiopia, which shows that younger adolescents face immense systemic exclusion from sexual health services due to a combination of restricted financial autonomy, legal ambiguities surrounding minor consent, and pervasive, judgmental provider-level biases that stigmatize sexually active unmarried teenagers. 15
Furthermore, the exceptionally high odds ratios observed among married or cohabiting women (AOR = 7.21) and formerly married individuals (AOR = 8.62) point to a powerful structural mechanism that can be conceptualized as “marital gatekeeping.” Within the current Nigerian healthcare architecture, HIV screening is largely operationalized not as a routine, proactive wellness check, but as a mandatory structural box to be checked during premarital counseling or routine “opt-out” antenatal care services. Because testing is heavily bundled with pregnancy and maternal health infrastructure, single and never-married young women are effectively stranded in a clinical “prevention vacuum.” This dynamic mirrors qualitative evidence from Kenyan cohorts, where unmarried young women purposefully avoid entering clinical spaces for HIV testing due to intense social anxieties, fearing that seeking a test will be interpreted by community members as a public confession of premarital sexual activity. 16
Socioeconomic Stratification: Education and Wealth Gradients
The findings of this study reinforce the established global paradigm of educational attainment acting as a structural “social vaccine.” Young women who attained higher education demonstrated over a sevenfold increase in testing uptake (AOR = 7.13; 95% CI: 5.50, 9.25) relative to peers with no formal schooling. This profound socioeconomic gradient reflects dynamics observed in Malawi, where formal schooling dramatically enhances health literacy, equips young women with the cognitive tools to process complex epidemiological info, and deconstructs deeply ingrained mythological fallacies regarding HIV transmission. 17
Educated young women are also structurally empowered to navigate complex medical bureaucracies, possess higher relative autonomy, and confidently assert their right to diagnostic care. 18
Mirroring the educational gradient, household wealth acts as an undeniable axis of stratification. Young women belonging to the wealthiest wealth quintile exhibited nearly triple the odds of testing (AOR = 2.71; 95% CI: 2.02, 3.63) compared to those in the poorest cohort. Wealthier individuals typically enjoy greater financial independence and reside in areas with a higher density of health facilities. Crucially, this economic divide persists despite the existence of national policies guaranteeing “free” HIV testing services. This reality confirms that indirect, out-of-pocket expenditures such as prohibitive transportation costs, lengthy travel times, and the opportunity cost of missed economic labor continue to price the poorest young women out of the clinical market, rendering institutional fee exemptions ineffective for the most vulnerable populations. 19
Community-Level Determinants: The “Neighborhood Effect”
A compelling contribution of this multilevel analysis is the clear delineation of the “neighborhood effect” through macro-level variables. Our final adjusted model yielded an ICC of 19.0%, meaning nearly one-fifth of the total variance in HIV testing practices among young Nigerian women is strictly determined by the characteristics of their broader community context. This structural clustering closely mirrors multilevel evaluations from other high-burden settings, such as Ethiopia, which report community-level variance shares between 18.7% and 23.1%. 15 Our final MOR of 2.31 indicates that if an individual were to move from a community characterized by low diagnostic coverage to one with high coverage, her odds of undergoing an HIV test would increase by 131% based solely on the collective norms of her new residential area. Notably, this MOR is slightly higher than the cross-national average of 2.18 reported in a macro-level study spanning 33 African nations, suggesting that localized community inequities are especially pronounced in Nigeria. 14
At the intersection of community dynamics and behavioral modification, our study highlights the importance of normalization. Individual media exposure (AOR = 1.48; 95% CI: 1.27, 1.72) and residing within a cluster with high collective HIV knowledge (AOR = 1.43; 95% CI: 1.21, 1.69) both emerged as powerful, independent facilitators of testing. This finding aligns with empirical work from Ghana, which suggests that saturation of health information at the community level acts as a powerful “stigma-diluter.” 20
In environments where HIV awareness is collective and visible, undergoing a diagnostic test is repositioned as a rational, responsible, and normalized health practice rather than a source of social shame or a “confession” of risky behavior. Interestingly, while individual media access was a significant predictor, community-level media exposure failed to achieve statistical significance in the fully adjusted model. This indicates that localized, interpersonal knowledge saturation within the immediate social network is a much more powerful driver of clinical engagement than a person's solitary exposure to mass media broadcasts. 21
Limitations of the Study
While this investigation features several distinct strengths, including the use of a large, nationally representative dataset (N = 14,634) and the application of a robust multilevel modeling framework, certain intrinsic limitations must be acknowledged:
Cross-sectional constraints: The cross-sectional design of the 2024 NDHS makes it impossible to establish definitive temporal sequences or draw firm causal inferences between the identified individual or community predictors and actual HIV testing behavior. Self-reporting and recall bias: The primary outcome variable relies entirely on self-reported data regarding lifetime testing history, which introduces potential vulnerability to recall inaccuracies or social desirability bias, possibly leading to an over-reporting of pro-health behaviors. Unmeasured supply-side barriers: The secondary nature of the DHS data means we could not account for critical institutional and supply-side constraints. Vital structural factors such as the geographic proximity of youth-friendly clinics, the specific quality of care provided by healthcare workers, or localized stockouts of HIV rapid test kits were not captured in the master dataset and could not be controlled for in the regression models, potentially leaving a portion of the community-level variance unmeasured.
Conclusion
In conclusion, the empirical evidence from the 2024 NDHS demonstrates that accelerating progress toward the UNAIDS 95-95-95 targets in Nigeria requires an aggressive focus on resolving deep socioeconomic and structural inequalities. Public health strategies must deliberately look beyond the traditional, antenatal-centric diagnostic frameworks that currently exclude unmarried and adolescent girls. To close the implementation gap, the Nigerian Federal Ministry of Health and its international partners must transition toward decentralized, community-driven, and youth-friendly testing spaces that proactively reach single, uneducated, and economically marginalized young women directly within their residential environments.
Supplemental Material
sj-pdf-1-jia-10.1177_23259582261458942 - Supplemental material for Prevalence and Determinants of HIV Testing Practice Among Young Women in Nigeria: A Multilevel Analysis of the 2024 Demographic and Health Survey
Supplemental material, sj-pdf-1-jia-10.1177_23259582261458942 for Prevalence and Determinants of HIV Testing Practice Among Young Women in Nigeria: A Multilevel Analysis of the 2024 Demographic and Health Survey by Tsegaamlak Kumelachew Derse, Desalegn Mitiku Kidie, Addisu Simachew Asgai, Tadios Lidetu and Jenberu Mekurianew Kelkay in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-pdf-2-jia-10.1177_23259582261458942 - Supplemental material for Prevalence and Determinants of HIV Testing Practice Among Young Women in Nigeria: A Multilevel Analysis of the 2024 Demographic and Health Survey
Supplemental material, sj-pdf-2-jia-10.1177_23259582261458942 for Prevalence and Determinants of HIV Testing Practice Among Young Women in Nigeria: A Multilevel Analysis of the 2024 Demographic and Health Survey by Tsegaamlak Kumelachew Derse, Desalegn Mitiku Kidie, Addisu Simachew Asgai, Tadios Lidetu and Jenberu Mekurianew Kelkay in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Abbreviations
Acknowledgments
We would like to thank the DHS Program for providing access to the dataset.
Ethical Approval and Informed Consent
This study is a secondary analysis of de-identified, publicly available data from the 2024 Nigeria Demographic and Health Survey (NDHS). The primary survey protocol was officially approved by the National Health Research Ethics Committee of Nigeria (NHREC) and the Institutional Review Board of ICF International. Written permission to download and analyze the dataset for scientific research was obtained by the authors from the DHS Program (ICF International). Because this research utilizes fully anonymized, publicly available secondary data, direct institutional review board (IRB) review from our home institution, and individual primary informed consent from participants were not required. Primary consent was securely managed by the original data collectors. (![]() ) upon reasonable request and formal registration approval.
) upon reasonable request and formal registration approval.
Author Contributions
Tsegaamlak Kumelachew Derse: Conceptualization, methodology, formal analysis, and drafting of the original manuscript. Desalegn Mitiku Kidie: Data curation, methodology, and critical revision of the manuscript. Addisu Simachew Asgai: Validation, software, and editing the manuscript. Tadios Lidetu: Supervision and critical review of the intellectual content. Jenberu Mekurianew Kelkay: Investigation, visualization, and final approval of the version to be published. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets analyzed in this study are publicly available from the DHS Program.
Generative AI Statement
The authors declare that generative artificial intelligence (AI) tools were used solely to assist with language editing, grammar correction, and improvement of readability. AI was not used in the design of the study, data analysis, interpretation of results, or generation of scientific content. All analyses, results, and conclusions presented in this manuscript were conducted and verified by the authors, who take full responsibility for the integrity and accuracy of the work.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.