
Abstract
Objectives
This qualitative study used the Consolidated Framework for Implementation Research (CFIR) to examine how stigma emerges in HIV prevention services for young Hispanic/Latino sexual minority men in North Carolina.
Methods
In-depth interviews were conducted with n = 14 community- and clinic-based providers between November 2023 and July 2024. Interviews were analyzed using a hybrid deductive–inductive approach.
Results
Findings identified multi-level factors shaping stigma experiences and practices. In the Outer Setting, sociocultural beliefs, discriminatory policies, and preventive care norms facilitated stigma, undermining trust and engagement in HIV prevention. Within the Inner Setting, organizational culture, physical space, accessibility, and workforce representation influenced whether services felt safe and trustworthy. Individual biases, limited awareness, stigmatizing communication, narrow biomedical framings of HIV risk, and inflexible service designs further reinforced stigma. Implementation processes that emphasized inclusive messaging, routine sexual health discussions, intentional workforce planning, and ongoing stigma-reduction training were described as opportunities to disrupt stigma across all CFIR domains.
Conclusion
Stigma in HIV prevention for young Hispanic/Latino sexual minority men emerges across policy, organizational, and interpersonal levels. Implementation strategies that promote inclusive messaging, routine sexual health conversations, representative staffing, and ongoing training may help reduce stigma.
Plain Language Summary
Stigma in HIV Prevention Services for Young Hispanic/Latino Gay, Bisexual, and Other Men Who Have Sex With Men: What Providers See and How They and Their Organizations Can Build Trust and Welcoming Care
Young Hispanic/Latino gay, bisexual, and other men who have sex men face high HIV risk and often feel unwelcome or judged when trying to get or receive HIV-prevention services. This study explains how stigma manifests in those services and what providers and organizations can do to make services safer and more affirming.
This qualitative study conducted one-on-one interviews with 14 providers who work in community organizations and clinics that serve young Hispanic/Latino gay, bisexual, and other men who have sex men in North Carolina. We used 2 well-known implementation and stigma frameworks to organize what providers said, enabling us to map where and how stigma appears in HIV-prevention services and how it might be reduced.
Stigma was described at every level of the HIV-prevention system: in wider social values, in how organizations are run, in individual provider and staff attitudes, and in the way HIV-prevention programs are designed and put into practice. Providers reported that factors such as discriminatory laws, cultural norms that discourage preventive care, unwelcoming clinic environments, lack of representative staff, and personal biases all combined to make services feel less safe, less inclusive, and less trustworthy for young Hispanic/Latino gay, bisexual, and other men who have sex men.
Because stigma is embedded across multiple levels, efforts to reduce it must also occur at those levels. Examples include redesigning services to be more flexible and person-centered and improving provider and staff training on stigma reduction and inclusive communication. The study provides suggestions for where organizations and decision-makers can act, such as using inclusive messaging, routinely discussing sexual health without judgment, planning for a more diverse workforce, and offering ongoing training, to improve the reach and impact of HIV-prevention services.
Keywords
Introduction
In the United States, Hispanic/Latino sexual minority men (H/LSMM) are disproportionately affected by the HIV and AIDS epidemic relative to their population size. Among H/LSMM, young gay and bisexual men ages 13 to 24 are markedly affected. 1 In 2022, young H/LSMM accounted for 32% of HIV diagnoses among all gay and bisexual adolescents and young adults.2,3 During the same period, young H/LSMM made up 20% of new HIV diagnoses among H/LSMM. These numbers suggest that effective biomedical HIV interventions, including pre-exposure prophylaxis (PrEP), while reducing HIV diagnoses in other groups, may not be effective or meet the needs of young H/LSMM. 4
The high burden of HIV among H/LSMM, including young H/LSMM, has been linked to multiple layers of stigma they might face.5,6 In North Carolina (NC), as in much of the Southern United States, the intersection of sexual orientation and race/ethnicity with HIV creates unique and compounded barriers to HIV prevention for young H/LSMM.7,8 In addition to facing stigma based on sexual orientation and perception of HIV as a predominantly gay men's disease, young H/LSMM often contend with racialized and prejudicial assumptions tied to perceived immigration status and English language proficiency.6,8 These overlapping forms of stigma shape distinct experiences that further hinder access to needed HIV preventive care, including regular HIV testing and PrEP.5,9,10
Although stigma has been known to shape HIV vulnerability and engagement in HIV prevention among young H/LSMM,5,6 less is understood about how stigma emerges within HIV-prevention environments—defined as the physical, social, or organizational settings where prevention services are delivered, including health clinics and community-based organizations—and how it affects access to and use of HIV prevention services. Studies have examined organizational and individual-level adaptations to improve uptake of health services among underserved populations.11‐13 For H/LSMM, these adaptations include representation of bilingual and bicultural staff, ongoing cultural responsiveness and trauma-informed training, and trust-building approaches.5,14,15 These studies highlight that culturally congruent and affirming care is critical for supporting H/LSMM's engagement in biomedical HIV prevention strategies. This pattern aligns with research showing the importance of culturally responsive preventive care more broadly among other Latino and sexual and gender minority populations.16‐19 However, these studies offer limited insight into whether these organizational and individual-level adaptations shape stigma experiences among young H/LSMM or influence the routine stigmatizing or stigma-reducing practices of individuals and organizations.20,21 Less attention has been given to the multi-level and dynamic ways in which stigma manifests across organizational culture, individual attitudes and behaviors, and implementation processes. Furthermore, little is known about how these multi-level stigma manifestations function across different HIV-prevention environments or how they influence critical outcomes such as disclosure and perceived psychological safety, PrEP initiation, and sustained HIV prevention engagement among young H/LSMM.22,23
The current gaps in knowledge are critical, given the structural and sociocultural factors that shape young H/LSMM's experiences and engagement in HIV prevention.5,24 Unlike older H/LSMM, many young H/LSMM are only beginning their HIV-prevention journey, making their earliest encounters with prevention systems especially consequential. Early missteps or stigmatizing experiences during this initial stage can undermine trust, limit disclosure, and negatively affect long-term engagement in HIV prevention and care.25,26 To address the limitations in prior research, this study examines how stigma manifests within HIV-prevention environments—both within organizations and among providers and staff who deliver services to young H/LSMM—and how specific individual and organizational-level practices may either reinforce or disrupt stigma. Drawing on perspectives from providers in community-based and clinic-based settings, this study explores how stigmatizing practices emerge through everyday interactions, organizational culture, characteristics of prevention services, implementation strategies, and broader cultural norms, and how these processes shape young H/LSMM's experiences of stigma in HIV prevention services. By centering the perspectives of those who design, provide, and implement services, the objective of this exploratory study is to generate evidence and inform future hypotheses with clear implications for actionable interventions to mitigate stigma practices at the individual and organizational levels and to reduce stigma experiences among young H/LSMM when seeking HIV prevention services in community- or clinic-based settings.
Methods
Study Design
The study used a descriptive qualitative design to examine how stigma manifests within HIV-prevention environments and how organizational- and provider-level practices may reinforce or disrupt stigma experiences among young H/LSMM. Data were collected through in-depth interviews with key informants (KIs), defined as community- and clinic-based providers who work directly with young H/LSMM across diverse HIV-prevention settings in North Carolina. This design enabled a nuanced exploration of how structural, organizational, interpersonal, and individual factors are viewed as stigma-reducing or stigma-reinforcing and shape young H/LSMM's experiences with HIV prevention.
Participants, Sampling Strategy, and Sample Size
The study used a purposive sampling strategy to recruit KIs (n = 14), or community-based and clinic-based providers with direct experience serving young H/LSMM in HIV-prevention settings. KIs were recruited through professional networks, community-based organizations, HIV clinics, and referrals from key contacts with experience working with this population. Eligibility criteria required KIs to be at least 18 years old and to have a minimum of 2 years of current or prior experience delivering social or health services related to HIV prevention in young H/LSMM. These services included—but were not limited to—HIV testing and counseling, PrEP navigation, sexual health education, mental health support, substance use services, case management, community outreach, spiritual care, advocacy, linkage-to-care activities, and other prevention-support services. These criteria ensured that KIs could offer informed perspectives on how stigma emerges within different HIV-prevention environments and how organizational and provider-level practices contribute to or mitigate young H/LSMM's experiences of stigma when accessing prevention services. The final sample size of 14 was determined through an iterative review of emerging patterns from the interviews, which the team used to identify data saturation on the primary research questions. Data saturation was reached for the primary research questions after 14 KI interviews. This determination was made through the research team's iterative review of emerging patterns during data collection and analysis, indicating that no new themes were emerging, and informed the decision to finalize the key informant sample at 14 participants.
Key informants represented 10 organizations spanning multiple sectors, including educational institutions, faith-based organizations, public health agencies, medical and hospital systems, and community-based organizations. Most participants were based in the Raleigh/Durham metropolitan area, with additional representation from the Charlotte metropolitan area. The sample reflected diverse identities and professional backgrounds: 9 identified as Latino/a/e, 8 as lesbian, gay, bisexual, or transgender (LGBT+), and 5 as Hispanic/Latino sexual minority men. Participants’ expertise spanned mental health, spiritual care, LGBT+ medical care, legal and advocacy services, substance use services, and HIV prevention (including testing and PrEP). Including providers across these varied settings and identities enabled a comprehensive understanding of how organizational structures, service-delivery contexts, and frontline practices shape stigma experiences and engagement in prevention among young H/LSMM. Table 1 summarizes KI and organizational characteristics.
Key Informant and Organizational Characteristics.
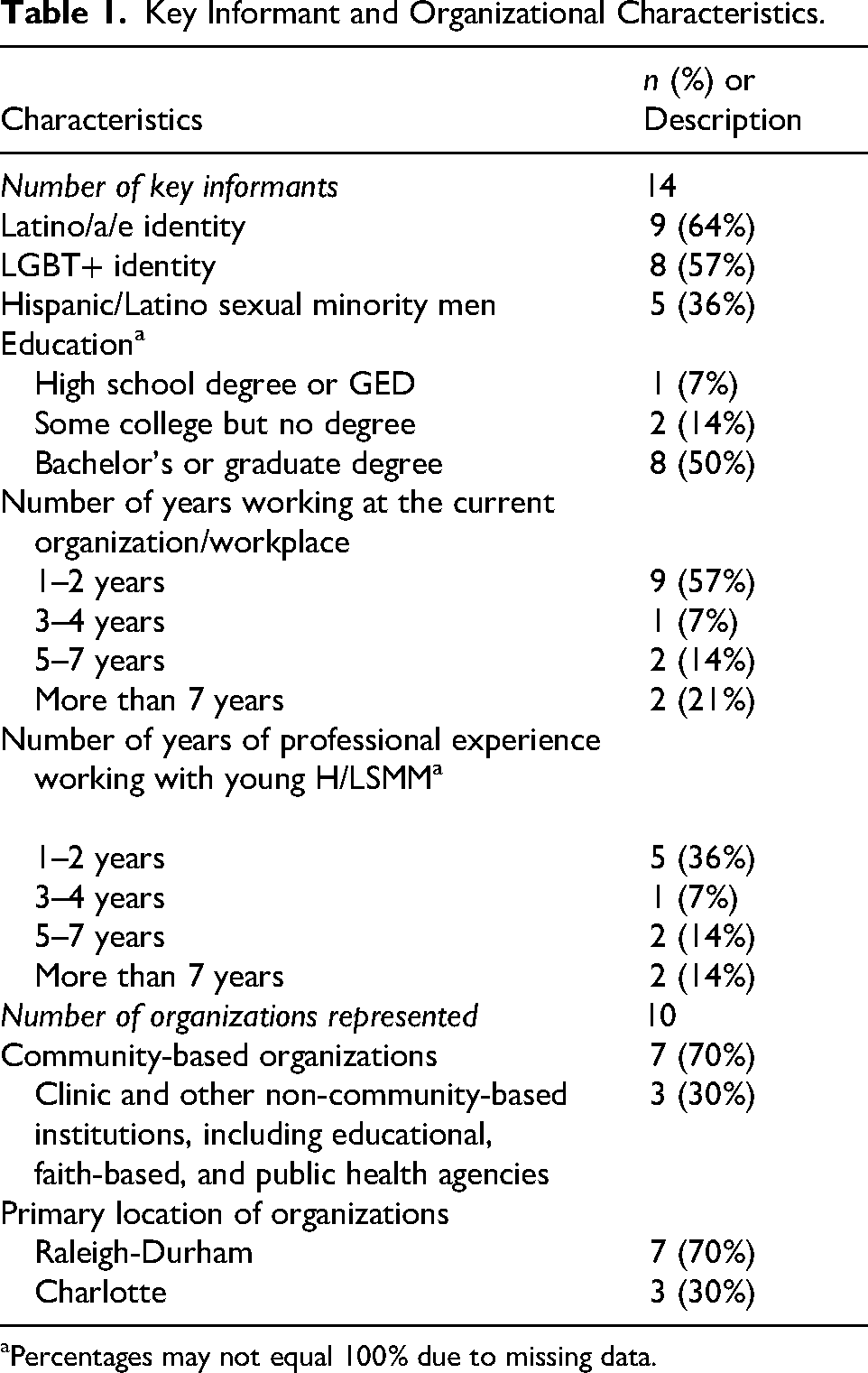
Percentages may not equal 100% due to missing data.
Data Collection Tools
Consistent with community-engaged research principles, an interview guide (see Appendix A) was developed through close collaboration between community partners and research staff and was used across all in-depth interviews (IDIs). During a formative start-up phase, we convened partners to review the project's overarching objectives and specific aims and to co-develop interview domains and probes intended to inform subsequent phases of intervention design. The initial guide included 19 questions and was refined through multiple rounds of structured feedback to enhance conceptual alignment with study aims, improve clarity and sequencing, and ensure cultural and contextual relevance.
The final guide comprised 12 questions addressing 5 primary domains: (a) personal and professional experiences related to HIV prevention among young H/LSMM; (b) perceptions of community strengths, needs, and structural barriers; (c) examples of successful and challenging practices within HIV prevention settings; (d) manifestations of stigma across organizational policies, interpersonal interactions, and routine service practices; and (e) recommendations for interventions, policies, and organizational change. This format supported methodological rigor while preserving flexibility, allowing interviewers to probe emergent themes and contextual nuances related to stigma, organizational culture, and service delivery. This iterative development process strengthened the guide's content validity and enhanced the credibility and trustworthiness of the qualitative data.
The final guide was translated into Spanish by the fourth and fifth authors, who are bilingual and have more than 20 years of combined experience providing HIV prevention and clinical services to the target population. The Spanish-language version was reviewed for semantic accuracy, cultural appropriateness, and consistency with the English-language guide. Any discrepancies in wording or meaning were discussed and resolved collaboratively before data collection. The translated guide was further validated through review by bilingual community partners and research staff familiar with the local service context, HIV prevention terminology, and culturally responsive language for discussing stigma, sexuality, and HIV.
Data Collection Procedures
We conducted 14 IDIs between November 2023 and July 2024 to capture rich, contextually grounded narratives about how stigma manifests within HIV-prevention environments and how organizational and individual-level practices shape experiences and engagement in prevention among young H/LSMM. IDIs were selected for their ability to elicit detailed accounts of organizational, individual, and sociocultural dynamics that cannot be captured through survey methods. 27
Interviews followed a protocol that allowed flexibility to probe emerging themes related to organizational culture and practices, individual attitudes and behaviors, stigma experiences, and barriers within different HIV-prevention environments. This approach facilitated the identification of multi-level contextual influences on stigma and HIV preventive service uptake. Interviews were conducted either in person or virtually, lasted 45–90 min, and were held in the language of the key informant's choice (English or Spanish) by bilingual interviewers.
Interviews were conducted by trained research staff. In addition to language proficiency, interviewers were selected for their familiarity with the community's lived social and cultural experiences. These attributes strengthened the team's ability to build rapport and meaningfully engage participants. Interviewers received training on the overarching project goals and on specific interviewing techniques, including establishing trust, effective probing, re-centering conversations when interviews strayed off topic, and recognizing potential sources of bias that could influence data collection. During data collection, the research team met weekly to review emerging patterns from the interviews. Through this iterative process, the team determined that thematic saturation had been achieved regarding the study's primary research questions.
Data Analysis
Reflexivity and Trustworthiness
Data analysis was conducted by a multidisciplinary team of social-behavioral scientists with expertise in HIV prevention and health equity research. All team members identify as members of racial/ethnic minoritized groups, and the majority identify as members of the LGBT+ community. We recognize that researchers’ social and professional identities may shape data interpretation; therefore, reflexivity was incorporated throughout the analytic process. At the outset of the project, team members engaged in structured discussions to reflect on their positionalities, assumptions, and potential biases related to HIV, stigma, and health equity. In particular, the team intentionally centered strengths, resilience, and community assets within the H/LMSM community to avoid deficit-oriented framings. Reflexive practices continued throughout data collection and analysis through regular team debriefings and collaborative review of emergent codes and themes. The team also maintained analytic notes and meeting documentation to support transparency and to create an audit trail of the process. During all interactions with participants and community partners, team members emphasized mutual respect, transparency about study goals, and shared commitment to improving community health. This approach supported trust-building while mitigating potential power imbalances between researchers and community members. Formal member checking with interview participants was not conducted because scheduling constraints made it difficult to re-engage KIs within the study timeline. However, community-based partners were engaged throughout the study through weekly meetings that included updates on recruitment and interview processes as well as discussions of emerging patterns and preliminary thematic interpretations. These discussions provided opportunities to assess the contextual relevance of emerging findings. Community partners possessed relevant contextual and clinical knowledge through their backgrounds and experience as clinical providers, including nurses and social workers, who have worked directly with young H/LSMM and HIV prevention services in the local context. Their familiarity with the population, service environment, organizational constraints, and stigma-related challenges helped assess whether themes were plausible, contextually grounded, and consistent with practice-based realities.
Data Preparation and Management
Data analysis focused on the transcripts from the 14 key informant interviews. All interviews were audio recorded and transcribed verbatim. For interviews conducted in Spanish, transcripts were translated line by line into English and checked for accuracy against the original recordings by bilingual members of the research team. All transcripts were uploaded into NVivo 1.7.1 for coding and data management, with supplemental matrix coding conducted in Microsoft Excel.
Thematic Analysis and Framework-Guided Interpretation
We used a hybrid deductive–inductive thematic analysis approach to ensure that both participant perspectives and theoretical constructs guided data interpretation. Consistent with this approach, the Health Stigma and Discrimination Framework (HSDF) and the Consolidated Framework for Implementation Research (CFIR) were used as complementary interpretive frameworks.28‐30 HSDF served as a problem theory framework to characterize stigma as the central problem, whereas CFIR served as an implementation framework to organize participant-derived findings, including those supported by HSDF, into implementation determinants that may be modified through intervention design.
In the first phase, the team applied an a priori thematic codebook informed by the HSDF. 28 This codebook was developed from the team's prior analysis of 15 IDIs with young H/LSMM who reported regular HIV testing or PrEP-related uptake in the context of multiple stigmas. Guided by the HSDF, the team created an initial, theory-driven set of codes, met to reconcile overlapping codes, and documented any discrepancies. The team then organized these codes into preliminary categories and iteratively reviewed them to identify broader patterns and themes. A detailed account of this earlier thematic analysis is reported in another publication. The HSDF-informed codebook provided a common theoretical grounding that allowed stigma-related constructs, including drivers, facilitators, manifestations, and outcomes across social-ecological levels, to be interpreted systematically and consistently across data sources from the same research project focused on stigma and HIV prevention among young H/LSMM. This phase guided the identification of domains related to (a) stigma drivers, facilitators, manifestations, and outcomes across social-ecological levels, and (b) individual, interpersonal, and community-level assets that shape involvement and engagement in HIV prevention activities among young H/LSMM.
In the second phase, 2 graduate student co-authors conducted inductive coding to identify emergent patterns that capture how organizational culture, individual practices, and contextual features influence the delivery of HIV prevention services and shape young H/LSMM's experiences when accessing services. Inductive coding allowed themes to emerge from KI data without being constrained by predefined HSDF codes or categories. Codes were added, refined, or collapsed based on the KI narratives and the coding team's ongoing review of emergent patterns. Particular attention was given to how stigma manifests or is reinforced across individual, interpersonal, organizational, and structural levels and how these multi-level manifestations influence prevention engagement. The coding team met regularly to compare interpretations, reconcile discrepancies, and refine the emergent code structure. Categories were then reviewed collectively to develop preliminary themes.
After inductive coding was completed, we applied the updated Consolidated Framework for Implementation Research (CFIR) to guide the final classification and interpretation of emergent themes and subthemes and to provide a well-established implementation science vocabulary to situate participant-derived insights within constructs known to influence implementation success.29,30 Themes were mapped to CFIR domains by linking KI narratives to the domain definitions illustrated in CFIR 2.0. 29 For example, when KIs described organizational or clinic policies, staffing shortages, or limited Spanish-language materials, these codes were grouped under the Inner Setting domain because they reflected organizational structures, resources, and climate. Descriptions of each CFIR domain and their alignment with our themes are presented in the Findings. Thus, CFIR provided a pragmatic structure for organizing the findings into multi-level implementation determinants across the Innovation, Outer Setting, Inner Setting, Individuals, and Implementation Process domains.
Using CFIR in the final analytic stage strengthened analytic rigor, coherence, and transferability by integrating inductive and deductive approaches, that is, linking providers’ observations of stigma and their HIV prevention experiences with constructs known to influence implementation success. This approach ensured that emergent findings were grounded in theory (HSDF) while also identifying implementation determinants (CFIR) that clarify how individual- and organizational-level practices can reinforce or disrupt stigma, thereby enhancing the responsiveness of HIV-prevention services for young H/LSMM. The reporting of this study conforms to the Standards for Reporting Qualitative Research (SRQR) statement, 31 and the completed SRQR checklist is provided as a supplementary file.
Ethical Considerations
Study procedures were reviewed and approved by the Institutional Review Board at the University of North Carolina at Chapel Hill (reference # 21-1902). Before participation, all KIs provided written or electronic informed consent, including for audio recording.
Results
We organized the findings using the CFIR domains of Outer Setting, Inner Setting, Individuals, Implementation Process, and Innovation. 29 Each domain reflects a distinct yet interconnected set of factors that shape how stigma emerges within HIV prevention environments and how these experiences influence young H/LSMM's engagement and sustained participation in HIV prevention strategies. At the same time, themes within each domain highlight opportunities for modifying organizational culture, community expectations, individual attitudes, and implementation practices to reduce stigma-related barriers and improve uptake of HIV-prevention services among young H/LSMM. Appendix B presents the full quotes organized by CFIR domain, offering additional context for the themes described in the findings.
Outer Setting
Themes within the Outer Setting domain, defined as contextual factors external to the organizations (and individuals within the organizations) delivering HIV preventive services, highlight how stigmatizing external policies, societal values and beliefs, and cultural norms regarding preventive care collectively shape young H/LSMM's engagement in HIV-prevention services.
KIs described how external discriminatory policies reinforce these stigmatizing beliefs. One KI discussed how policies such as blood donation restrictions reinforce sexual stigma by suggesting that sexual activities between men are “bad,” adding that “this [blood donation] service does not exist for them, so I know it has to be bad… just adding to the stigma.” This finding reflects the Outer Setting by showing how policy-level discrimination communicates moral judgment, deepens stigma, and discourages prevention engagement.
KIs also emphasized how broader stigma experiences, resulting from societal values and beliefs, translate into fear and mistrust even before young H/LSMM interact with an organization or provider delivering HIV preventive services. As one KI explained, young H/LSMM who have “felt discriminated against or oppressed by medical providers in the past or know of [stigmatizing] experiences in the family, they carry with them these experiences,” which “keep them sometimes from finding the services that they needed.” This finding aligns with the Outer Setting domain by showing that past experiences of stigma, whether direct or shared through others’ stories and occurring outside HIV prevention settings, create a broader climate of mistrust that influences decisions about seeking health services.
The same KI explained the effect of these broader stigma experiences on healthcare seeking, noting that even when young H/LSMM are interested in prevention, “maybe they did have the interest, but they kind of just did not want to [seek services] because of that fear of being discriminated against.” This quote reflects how external stigma narratives, shaped by societal beliefs, directly dampen motivation to engage in HIV-prevention services.
Furthermore, while cultural norms around preventive care are known to shape engagement, for young H/LSMM, stigma may exacerbate these deeply rooted cultural norms, further discouraging engagement in HIV prevention services. One KI described that in many Latino communities, “we do not go to the doctor as preventative measures… [instead] you can go to a pharmacy… [and] they will give you a prescription for something,” emphasizing how patterns of care-seeking are shaped by norms external to health systems. Another KI connected this care-seeking norm to narratives of stigma experiences shared across families and communities, noting that youth often come with “a preconceived notion” about the medical system that is “confirmed” by negative experiences. These findings illustrate the Outer Setting domain by showing how external influences such as cultural norms and community stigma narratives compound stigma and interfere with HIV-prevention uptake.
Inner Setting
Themes within the Inner Setting domain, defined as the organizational environments in which HIV prevention services are delivered, highlight the importance of organizational culture, physical infrastructure, and workforce representation in shaping young H/LSMM's engagement.
KIs described 2 central aspects of organizational culture: human-equality-centeredness (the shared belief in the equal worth and value of underserved populations, such as young H/LSMM) and recipient-centeredness (the norms and practices that actively support and address the needs of young H/LSMM). Several KIs emphasized the importance of visual cues and welcome signs. One KI described how a simple sign reading “all are welcome” with “a variety of colors and a variety of flags” elicited positive reactions from clients. This finding aligns with the Inner Setting Domain by showing how organizational culture is communicated through physical design elements that help clients feel valued.
Visual representation within clinics also shaped perceptions of safety. A KI noted that when young H/LSMM “walk in the clinic, who is on the wall?” they immediately assess whether the environment includes and represents people like them. Sustaining a truly welcoming environment was described as an ongoing responsibility “to constantly work really hard to maintain that environment where people feel really welcome.”
Psychological safety was another central theme. One KI explained that some young H/LSMM avoided entering the HIV clinic because “everybody knew where the HIV clinic was,” underscoring how clinic layout can inadvertently disclose HIV status and heighten stigma. This finding reflects the Inner Setting because it shows how physical space shapes young H/LSMM's willingness to engage in care.
Workforce representation was also described as vital to the Inner Setting. As one KI explained, seeing staff who were Latino, Black, or trans made them feel, “I could trust these people.” This finding represents the Inner Setting domain by showing how workforce diversity fosters trust and a sense of belonging. Another KI emphasized that a lack of diversity signals priorities that may not include marginalized communities. This finding reflects the Inner Setting's focus on organizational culture and climate as determinants of engagement. Representation at multiple levels—staff, providers, and administrators—also broadens exposure across the organization, helping personnel better understand, empathize with, and effectively interact with Latine LGBT+ clients while normalizing their presence and fostering safety and belonging for young H/LSMM.
Finally, language accessibility and infrastructure gaps also shaped experiences. One KI described some youth who discontinued treatment because no Spanish-speaking staff were available at the front desk, showing how organizational processes can reinforce exclusion. Another cited delays in providing patient portals in Spanish, highlighting physical/technological infrastructure barriers embedded in the Inner Setting.
Individuals
Themes within the Individuals domain, defined as the roles and characteristics of individuals who directly or indirectly deliver HIV prevention services, highlight how negative or prejudicial attitudes, limited awareness, and insufficient interpersonal skills among staff and providers contribute to young H/LSMMs’ stigma experiences and shape their willingness to engage in services.
Several KIs described how perceived prejudicial attitudes create immediate barriers. One KI noted that, “depending on who is behind the desk … if they have that stigma against young Latino men, off the bat there is that push back, … that feeling of I do not understand you, you do not belong.” This finding reflects the Individuals domain by showing how individual biases and nonverbal behavior communicate exclusion and reinforce anticipated stigma.
Another KI emphasized that these barriers often arise from unwillingness to understand young H/LSMM, describing how staff say, “Well, I do not understand them,” even when youth are speaking English with only an accent. The same KI also noted that when young H/LSMM come to their organization, “the question, ‘why’ comes up a lot? Why do they need that? Why do they ask that?” which reflects a lack of willingness to understand where the young H/LSMM are coming from. This finding aligns with the Individuals domain by illustrating how linguistic bias and limited cultural awareness lead to stigmatizing interactions that undermine trust.
KIs further noted that limited provider awareness about sexual diversity and Latino LGBT+ populations impedes effective HIV-prevention counseling. One KI observed that providers may find clients with partners of multiple genders “confusing and weird,” leading them to avoid conversations about risk reduction. This finding aligns with the Individuals domain by showing how insufficient knowledge and discomfort discussing sexual behavior contribute to stigma and reduce the effectiveness of prevention services.
Communication skills emerged as a central component of reducing stigma. One KI emphasized that providers “can do a lot of damage” if they are not careful with their words, underscoring the critical role of interpersonal communication competencies in ensuring non-stigmatizing interactions. This finding aligns with the Individuals domain by underscoring the impact of provider language on trust and engagement.
Another KI stressed the importance of rapport-building and timing in sensitive conversations: “it is how you ask it and it is when you ask it… Maybe after 10 or 15 min, that person is more likely to be open.” This example represents the Individuals domain by showing how interpersonal skills, such as timing, tone, and rapport, affect young H/LSMM's comfort, disclosure, and willingness to engage in preventive care.
Innovation
Themes within the Innovation domain, defined as the characteristics of HIV prevention services, highlight the importance of design and adaptability in delivering holistic, culturally responsive, and non-stigmatizing care for young H/LSMM.
Several KIs described the limitations in current HIV prevention designs, noting that programming for Latinx LGBT+ communities focuses narrowly on the biomedical risk. One KI explained that “LGBTQ programming in Latinx communities has been based around HIV prevention,” highlighting the need for whole-person approaches. This finding reflects the Innovation domain by emphasizing how design features, such as content, framing, and focus, must evolve to promote holistic, culturally grounded prevention.
KIs emphasized that young H/LSMM need more than testing and PrEP; they also require mental health care, housing support, and broader wraparound services. One KI noted that discussing only HIV “is not the only thing that concerns [young H/LSMM],” underscoring how integrated services better reflect their lived experiences. This finding aligns with the Innovation Domain by demonstrating how expanded design features can reduce stigma and improve relevance.
KIs also emphasized the importance of “explicit inclusivity” in intervention design, such as pronoun pins, rainbow symbols, or inclusive intake forms. These design features help young H/LSMM feel safe and affirmed in prevention settings.
Adaptability emerged as a complementary theme. One KI explained that using bilingual providers and culturally responsive approaches was the “primary intervention,” highlighting adaptability in meeting linguistic and cultural needs. Another KI described the need for innovations that better reach communities of color, emphasizing adaptations that reduce stigma and increase cultural congruence.
Implementation Process
Themes within the Implementation Process Domain describe the activities and strategies that organizations and individuals use to implement non-stigmatizing HIV prevention services for young H/LSMM.
KIs highlighted the importance of executing inclusive practices, such as creating visible signage and welcoming symbols. One KI described “creating signage… where people know that they are welcome,” reflecting the Implementation Process domain by illustrating concrete implementation actions that signal safety and inclusivity.
Another KI emphasized the need to normalize sexual health discussions, explaining that avoiding conversations about HIV “can lead to transmission happening without knowledge.” This finding represents the Implementation Process domain by showing how engaging patients in regular, open dialogue is an essential implementation strategy for reducing stigma.
KIs described how providers’ proactive communication strategies, such as asking relevant questions, help establish trust and invite disclosure. One KI noted that when providers ask about risk factors, “patients relax,” representing the Process Domain through the execution of patient-centered communication practices.
Strategic planning for diverse workforce representation was also seen as a key process for shaping organizational priorities and signaling commitment. One KI noted the importance of bringing in BIPOC providers to better signal inclusivity. Although “the timing has not worked to bring in a BIPOC provider,” the KI explained that there is a plan, as “it is on my list of things to do.” This finding reflects the Implementation Process Domain by emphasizing planning as a core implementation activity that shapes organizational climate.
Finally, training was identified as essential. One KI emphasized the need for “a lot of training for health care workers” to communicate in non-stigmatizing ways. This finding aligns with the Implementation Process domain by highlighting training and capacity-building as key to implementing stigma-free HIV-prevention practices.
Cross-Domain CFIR-Based Model for Stigma Reduction and HIV-Prevention Uptake Among Young Hispanic/Latino Sexual Minority Men
Drawing on our findings, we developed a cross-domain conceptual model (Figure 1) illustrating how stigma emerges from factors operating across all CFIR domains. The model highlights how societal stigma and cultural norms (Outer Setting), provider and staff attitudes and skills (Individuals), organizational culture and infrastructure (Inner Setting), characteristics of HIV-prevention services (Innovation), and implementation strategies (Process) collectively shape young H/LSMM's experiences and engagement with HIV-prevention services. The Outer Setting creates a context of mistrust through narratives of stigma, cultural norms, and discriminatory policies, which in turn shape expectations and willingness to seek HIV prevention care. Individuals reinforce stigma through prejudicial attitudes and biases, limited knowledge and awareness, and stigmatizing communication practices, which in turn influence whether young H/LSMM experience HIV prevention services as welcoming or stigmatizing. Inner Setting amplifies or reduces stigma through organizational culture, visual and environmental cues, staff diversity, and language accessibility, which, in turn, shape whether young H/LSMM experience prevention settings as inclusive and trustworthy. Innovation characteristics determine whether HIV prevention services are responsive, inclusive, and adaptable—or rigid and stigmatizing. In turn, the design and adaptability of services contribute to perceived relevance and cultural fit that meet the full spectrum of young H/LSMM's needs. Implementation Process activities, such as training, planning, and normalization strategies, determine how well HIV preventive practices are enacted. In turn, these implementation processes influence delivery quality, consistency, and execution. Collectively, these multi-level mechanisms influence whether young H/LSMM feel safe enough to access, initiate, and remain engaged in HIV-prevention services.
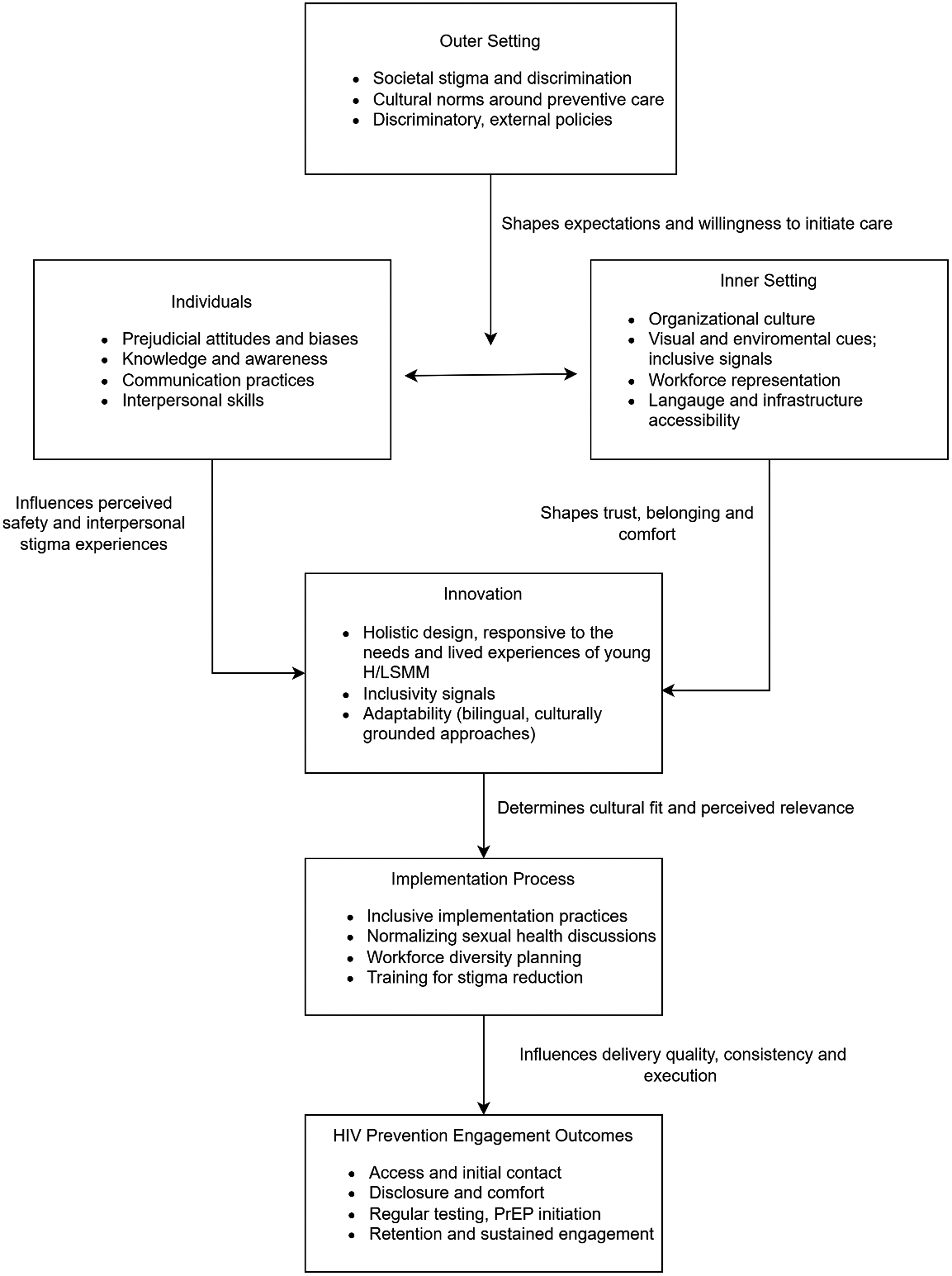
A conceptual model of multi-level mechanisms illustrating how external factors, provider and staff attitudes, organizational culture, intervention characteristics, and implementation strategies interact to influence whether HIV-prevention environments feel safe, welcoming, and responsive to young H/LSMM, which in turn, shape uptake, initiation, and sustained engagement in HIV-prevention services.
Discussion
Across CFIR domains, our findings underscore that stigma manifestations in HIV prevention services for young H/LSMM are generated and reinforced through multi-level mechanisms that extend beyond individual encounters. These multi-level findings are consistent with theoretical and empirical evidence that highlights the multi-level nature of stigma and the critical role of intersectionality, defined as a way of understanding how young H/LSMM's different identities come together and shape their life experiences, in HIV prevention.19,28,32 At the broadest and external level, the Outer Setting highlights how stigmatizing societal values, discriminatory policies, and cultural norms that discourage preventive care collectively deepen mistrust and reduce willingness to seek HIV-prevention services. These external forces may shape expectations before young H/LSMM enter a clinic or see a provider. Within HIV prevention organizations, the Individuals and Inner Setting domains illustrate how provider and staff characteristics, young H/LSMM's interactions with these personnel, and the broader organizational climate can either buffer against or intensify stigma. These findings align with prior work with H/LSMM and other underrepresented racialized sexual minorities in the U.S. South that have similarly documented the role of organizational contexts in shaping stigma experiences.33,34 In particular, providers’ and support staff's knowledge, attitudes, and communication skills appear central to whether young H/LSMM experience services as affirming and welcoming or, conversely, judgmental and stigmatizing, echoing findings from studies with other Latino groups, including sexual minority men.15,35 At the same time, organizational culture, physical design, workforce representation, and language accessibility signal whether young H/LSMM are valued, safe, and understood. These findings underpin themes highlighted in recent calls to strengthen the US HIV response and address HIV disparities among H/LSMM.4,36 Moreover, the interplay between individual readiness and organizational context is critical. Even well-designed interventions may fail if the personnel responsible for implementing them lack the cultural knowledge, self-efficacy, or interpersonal skills required to engage young H/LSMM effectively.37,38 Conversely, highly skilled and affirming providers may be limited by organizational cultures that do not prioritize representation, language accessibility, or environments conducive to psychological safety.21,39
At the intervention and implementation levels, the Innovation and Implementation Process domains highlight the importance of culturally responsive design and thoughtful execution to reduce stigma and support sustained engagement. Prior studies have noted the limitations of interventions that remain narrowly focused on biomedical risk, as these programs may inadvertently reinforce stigma.40,41 In contrast, holistic and culturally grounded approaches, such as integrating mental health, housing support, or bilingual service delivery, increase relevance and trust.42,43 Consistent with our findings, prior research has noted that visible signals of inclusion within intervention materials and physical spaces strengthen perceptions of safety.44,45 Furthermore, implementation processes shape the delivery of non-stigmatizing HIV prevention: inclusive messaging, normalization of sexual health conversations, strategic planning for diverse workforce representation, and ongoing staff training are essential to operationalizing stigma-reducing practices.24,46 Our findings demonstrate that HIV-prevention engagement for young H/LSMM requires attention to all CFIR domains, recognizing that stigma is not merely an intrapersonal or interpersonal issue, but a multi-level phenomenon embedded within community norms, personnel characteristics, organizational environments, intervention design, and implementation practices. These multi-level dynamics are consistent with prior studies involving H/LSMM and community stakeholders that similarly emphasize the need to address multiple forms of stigma and stigma-related barriers across structural, organizational, and relational levels.6,43,47
The Outer Setting also encompasses the growing sociopolitical context, including escalating federal anti-immigrant and anti-LBGT+ policies and rhetoric that profoundly impact HIV prevention engagement among young Hispanic/Latino/e sexual minority men (H/LSMM). Although such sentiments existed when we conducted the key informant interviews, their intensity has surged since then, driven by restrictive policy actions and public messaging targeting immigrant and LGBT+ communities.48,49 This shifting context has direct implications for how young H/LSMM and the broader Latino, immigrant, and LGBT+ communities navigate health services, including HIV prevention. Heightened fears of discrimination, surveillance, or legal repercussions may further exacerbate existing fear and mistrust, reduce willingness to disclose sensitive information, and deepen avoidance of healthcare systems.
Additionally, our findings underscore the vulnerability of young H/LSMM during the early stages of their HIV-prevention journey. For many, the first point of contact—often a front desk staff member, intake coordinator, or peer navigator—is a decisive moment that shapes their perception of whether the organization is safe and welcoming. When frontline staff display hesitation, bias, or limited comfort engaging with young H/LSMM, they inadvertently reinforce anticipated stigma, leading some young H/LSMM to disengage before ever seeing a provider. Early missteps in communication or attitude may have long-term consequences for young H/LSMM, particularly because they are just beginning to form relationships with the healthcare system and may lack prior positive experiences to counterbalance negative encounters or narratives of stigmatizing experiences shared by their families and communities. 50
Finally, young H/LSMM's experiences with stigma often originate outside of the organizations delivering HIV prevention services, shaped by broader cultural norms, family experiences, and societal discrimination.32,36 These external forces influence how young H/LSMM approach healthcare encounters and may predispose them to expect judgment, misunderstanding, or harm. This background of mistrust underscores the importance of intentional, stigma-aware implementation efforts across all domains to counteract the accumulated weight of stigma. 21
Findings from this study highlight several key implications for improving HIV prevention engagement among young H/LSMM. First, organizations must address stigma as a multi-level issue shaped by societal forces, organizational environments, interpersonal interactions, and intervention characteristics. Because young H/LSMM may make decisions about care engagement based on early impressions, investing in the first point of contact is critical. Training frontline staff to communicate in non-stigmatizing ways, both verbal and non-verbal, and to provide culturally responsive, nonjudgmental support is as essential as training providers. Second, HIV prevention interventions should expand beyond biomedical risks to include holistic, culturally grounded supports such as mental health care, housing assistance, and bilingual or family-inclusive services. These approaches help counteract stigma and align services with the needs and lived experiences of young H/LSMM. Third, policy and public health efforts must take into account the shifting sociopolitical landscape, particularly the intensifying anti-immigrant environment in major urban areas, including cities in North Carolina where this study was conducted. Fear of discrimination, surveillance, or legal consequences may discourage young H/LSMM, regardless of citizenship and documentation status, from accessing or remaining engaged in care. Health systems and public health agencies should explicitly communicate safety, confidentiality, and immigrant-inclusiveness to mitigate fears that hinder service use. Finally, integrating CFIR-guided assessments into routine practice can help organizations identify where stigma is produced and reinforced and tailor stigma-reduction strategies accordingly. Focusing on cultural responsiveness, inclusive design, and continuous training across all staff roles can strengthen HIV prevention uptake and retention among young H/LSMM.
A key strength of this study is its use of CFIR to examine how stigma operates across multiple levels of the HIV-prevention environment, yielding a nuanced understanding of structural, organizational, interpersonal, and intervention-specific determinants affecting young H/LSMM. Including providers from both community-based and clinical settings—many serving immigrant, LGBT+, and Spanish-speaking populations—enabled rich insights into how multiple forms of stigma shape prevention engagement. Although the study was conducted in North Carolina, the CFIR framework enhances analytic transferability by identifying general factors that influence service delivery. In regions with restrictive policies toward immigrants and LGBT+ people, outer-setting factors such as discrimination, fear of surveillance, and institutional mistrust can amplify barriers described in this study. In more affirming policy environments, outer-setting factors may mitigate the concerns noted in this study. Our analysis of other CFIR domains (inner setting, individuals, innovation, and implementation process) can identify modifiable organizational or interpersonal practices that may influence how outer-setting factors affect HIV prevention with H/LSMM.
This study also has limitations. Because data were drawn solely from providers, we were unable to capture young H/LSMM's firsthand experiences. The sample was geographically concentrated in one state, which may limit generalizability to regions with different sociopolitical climates or healthcare infrastructures. Interviews were conducted between November 2023 and July 2024, before the recent federal-level intensification of anti-immigrant and anti-LGBT+ policies and rhetoric, meaning providers may not have fully anticipated the heightened impact these national shifts now have on prevention engagement. Finally, because CFIR domains are interrelated, some quotes could reasonably align with multiple domains; in these cases, we chose the domain that best captured the underlying meaning and intent reflected in the participant's full narrative. Despite these limitations, the study provides valuable multi-level insights to guide stigma-reduction and implementation strategies tailored to young H/LSMM.
Conclusion
This qualitative study demonstrates that multi-level determinants contribute to stigma experiences and practices in HIV prevention for young H/LSMM. Stigma emerges not only from individual attitudes and communication but also from organizational culture, physical environments, intervention design, and broader sociopolitical forces. Therefore, improving HIV prevention uptake among young H/LSMM may require coordinated strategies that address sociocultural barriers, strengthen inclusive organizational practices, and ensure culturally responsive and holistic prevention services. By identifying where stigma manifests and is reinforced through the CFIR lens, study findings offer actionable guidance for designing and implementing stigma-reducing approaches that can enhance overall engagement in HIV-prevention efforts for young H/LSMM.
Supplemental Material
sj-docx-1-jia-10.1177_23259582261458953 - Supplemental material for Welcoming or Warning Signs? A Qualitative Study of Providers’ Perspectives on Stigma Experiences and Practices in HIV Prevention Services for Young Hispanic/Latino Sexual Minority Men
Supplemental material, sj-docx-1-jia-10.1177_23259582261458953 for Welcoming or Warning Signs? A Qualitative Study of Providers’ Perspectives on Stigma Experiences and Practices in HIV Prevention Services for Young Hispanic/Latino Sexual Minority Men by Rainier Masa, Allison Burns, Dicky Baruah, Natalia Villegas, José Orlando Martínez and Don Operario in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgments
The authors thank Paula Castellanos for their assistance with transcript verification and translation. We also thank all the participants for their contributions to this study.
Ethics Approval Obtained
This study was approved by the University of North Carolina at Chapel Hill Institutional Review Board (Reference # 21-1902).
Informed Consent Obtained for Research
All participants provided written informed consent prior to enrolment in the study for participation and for the collection, analysis, and reporting of their de-identified study data.
Author Contributions
R.M. led the conceptualization of the study, drafted the original manuscript, and contributed to subsequent review and editing. A.B. and D.B. conducted formal analysis and data management. N.V. and D.O. contributed to reviewing and editing the manuscript. R.M., D.B., and J.O.M. conducted the interviews.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Minority Health and Health Disparities (Grant Number R21MD016356).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to the relatively small sample size and the potential risk of participant identification, full interview transcripts are not publicly available. De-identified excerpts relevant to the findings may be made available from the corresponding author upon reasonable request, subject to ethical and confidentiality considerations.
Supplemental Material
Supplemental material for this article is available online.
Appendix A: Key Informant Interview Guide
How important do you think HIV is as a health issue affecting YLSMM? From your experience, how big a challenge is stigma in addressing/preventing HIV among YLSMM? What issues around HIV concern you the most? If you had to pick 1 or 2 top concerns, what would those be? What do you think is the role of stigma in decreasing (or increasing) HIV transmission among YLSMM? What do you think is the impact on your organization of not addressing stigma and HIV? Could you please describe your experience related to increasing HIV testing awareness and screening for HIV in YLSMM? What are some successes and challenges? What worked? What did not work? Describe any experience you have (or your organization's) in “going the extra mile” to ensure YLSMM or other similar clients have access to HIV testing and/or PrEP. What do you see as the greatest challenges around reducing stigma and preventing transmission of HIV among YLSMM? Thinking about reducing stigma to promote HIV testing and PrEP use among YLSMM, what do you think are the community's greatest strengths or assets around these issues? What is currently being done at your organization to reduce stigma as a way to increase HIV testing and PrEP use among YLSMM? What programs or services are available for organizations that would like to integrate stigma reduction in their HIV prevention work with YLSMM? Why do you think there are few programs or services available to YLSMM? What has been your experience or your organization's experience reaching out to YLSMM? What are some notable successes? What are some recurring challenges? How would you describe your experience or your organization's experience in retaining YLSMM or encouraging them to come for follow-up visits? If you could do one thing to reduce stigma and to improve HIV testing and PrEP uptake among YLSMM, what would it be? If you could change or implement a new program, service, or policy, what would it be? What individuals/organizations should lead this effort?
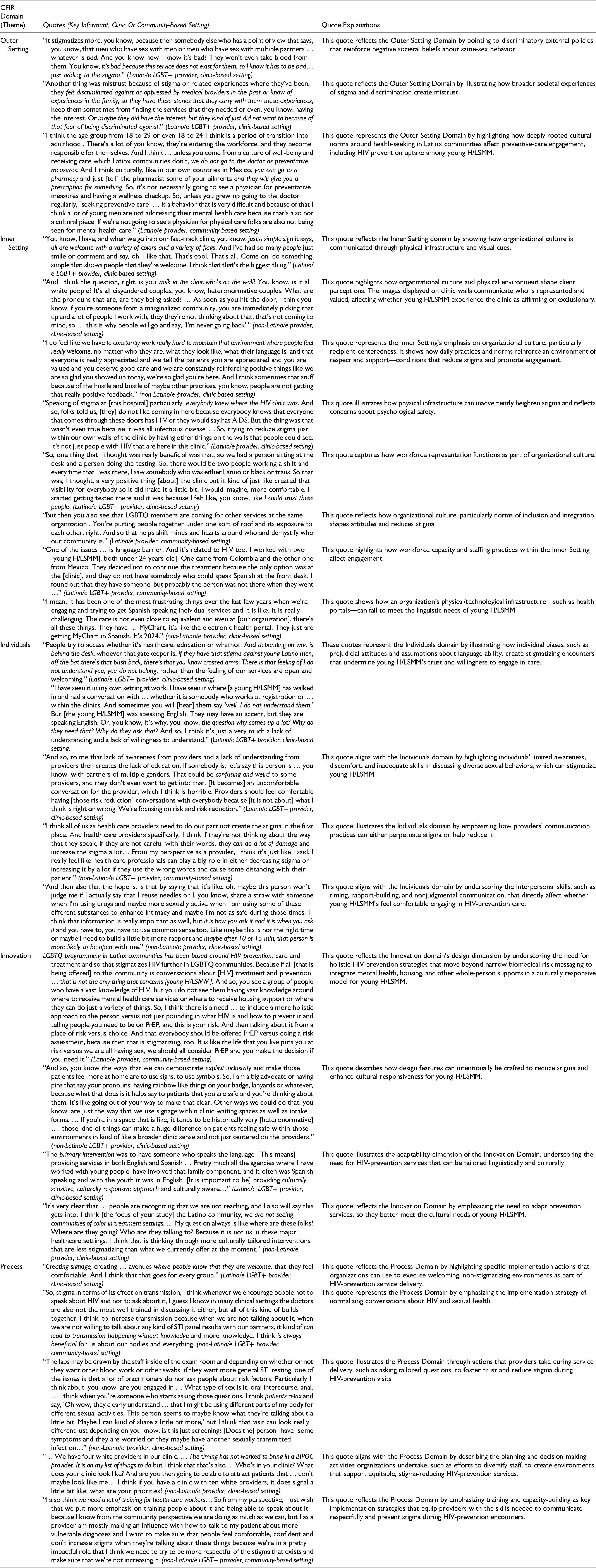
Appendix B. Representative Quotes From Key Informant Interviews Illustrating How Stigma Experiences and Practices Map Onto CFIR Domains in the Context of HIV Prevention for Young H/LSMM
| CFIR Domain |
Quotes (Key Informant, Clinic Or Community-Based Setting) | Quote Explanations |
|---|---|---|
| Outer Setting | “It stigmatizes more, you know, because then somebody else who has a point of view that says, you know, that men who have sex with men or men who have sex with multiple partners … whatever is bad. And you know how I know it's bad? They won't even take blood from them. You know, it's bad because this service does not exist for them, so I know it has to be bad… just adding to the stigma.” (Latino/e LGBT+ provider, clinic-based setting) | This quote reflects the Outer Setting Domain by pointing to discriminatory external policies that reinforce negative societal beliefs about same-sex behavior. |
| “Another thing was mistrust because of stigma or related experiences where they've been, they felt discriminated against or oppressed by medical providers in the past or know of experiences in the family, so they have these stories that they carry with them these experiences, keep them sometimes from finding the services that they needed or even, you know, having the interest. Or maybe they did have the interest, but they kind of just did not want to because of that fear of being discriminated against.” (Latino/e LGBT+ provider, clinic-based setting) | This quote reflects the Outer Setting Domain by illustrating how broader societal experiences of stigma and discrimination create mistrust. | |
| “I think the age group from 18 to 29 or even 18 to 24 I think is a period of transition into adulthood . There's a lot of you know, they're entering the workforce, and they become responsible for themselves. And I think … unless you come from a culture of well-being and receiving care which Latinx communities don't, we do not go to the doctor as preventative measures. And I think culturally, like in our own countries in Mexico, you can go to a pharmacy and just [tell] the pharmacist some of your ailments and they will give you a prescription for something. So, it's not necessarily going to see a physician for preventative measures and having a wellness checkup. So, unless you grew up going to the doctor regularly, [seeking preventive care] … is a behavior that is very difficult and because of that I think a lot of young men are not addressing their mental health care because that's also not a cultural piece. If we're not going to see a physician for physical care folks are also not being seen for mental health care.” (Latino/e provider, community-based setting) | This quote represents the Outer Setting Domain by highlighting how deeply rooted cultural norms around health-seeking in Latinx communities affect preventive-care engagement, including HIV prevention uptake among young H/LSMM. | |
| Inner Setting | “You know, I have, and when we go into our fast-track clinic, you know, just a simple sign it says, all are welcome with a variety of colors and a variety of flags. And I've had so many people just smile or comment and say, oh, I like that. That's cool. That's all. Come on, do something simple that shows people that they're welcome. I think that that's the biggest thing.” (Latino/e LGBT+ provider, clinic-based setting) | This quote reflects the Inner Setting domain by showing how organizational culture is communicated through physical infrastructure and visual cues. |
| “And I think the question, right, is you walk in the clinic who's on the wall? You know, is it all white people? It's all cisgendered couples, you know, heteronormative couples. What are the pronouns that are, are they being asked? … As soon as you hit the door, I think you know if you're someone from a marginalized community, you are immediately picking that up and a lot of people I work with, they they're not thinking about that, that's not coming to mind, so … this is why people will go and say, ‘I'm never going back’.” (non-Latino/e provider, clinic-based setting) | This quote highlights how organizational culture and physical environment shape client perceptions. The images displayed on clinic walls communicate who is represented and valued, affecting whether young H/LSMM experience the clinic as affirming or exclusionary. | |
| “I do feel like we have to constantly work really hard to maintain that environment where people feel really welcome, no matter who they are, what they look like, what their language is, and that everyone is really appreciated and we tell the patients you are appreciated and you are valued and you deserve good care and we are constantly reinforcing positive things like we are so glad you showed up today, we're so glad you're here. And I think sometimes that stuff because of the hustle and bustle of maybe other practices, you know, people are not getting that really positive feedback.” (non-Latino/e provider, clinic-based setting) | This quote represents the Inner Setting's emphasis on organizational culture, particularly recipient-centeredness. It shows how daily practices and norms reinforce an environment of respect and support—conditions that reduce stigma and promote engagement. | |
| “Speaking of stigma at [this hospital] particularly, everybody knew where the HIV clinic was. And so, folks told us, [they] do not like coming in here because everybody knows that everyone that comes through these doors has HIV or they would say has AIDS. But the thing was that wasn't even true because it was all infectious disease. … So, trying to reduce stigma just within our own walls of the clinic by having other things on the walls that people could see. It's not just people with HIV that are here in this clinic.” (Latino/e provider, clinic-based setting) | This quote illustrates how physical infrastructure can inadvertently heighten stigma and reflects concerns about psychological safety. | |
| “So, one thing that I thought was really beneficial was that, so we had a person sitting at the desk and a person doing the testing. So, there would be two people working a shift and every time that I was there, I saw somebody who was either Latino or black or trans. So that was, I thought, a very positive thing [about] the clinic but it kind of just like created that visibility for everybody so it did make it a little bit, I would imagine, more comfortable. I started getting tested there and it was because I felt like, you know, like I could trust these people. (Latino/e LGBT+ provider, clinic-based setting) | This quote captures how workforce representation functions as part of organizational culture. | |
| “But then you also see that LGBTQ members are coming for other services at the same organization . You're putting people together under one sort of roof and its exposure to each other, right. And so that helps shift minds and hearts around who and demystify who our community is.” (Latino/e provider, community-based setting) | This quote reflects how organizational culture, particularly norms of inclusion and integration, shapes attitudes and reduces stigma. | |
| “One of the issues … is language barrier. And it's related to HIV too. I worked with two [young H/LSMM], both under 24 years old]. One came from Colombia and the other one from Mexico. They decided not to continue the treatment because the only option was at the [clinic], and they do not have somebody who could speak Spanish at the front desk. I found out that they have someone, but probably the person was not there when they went …” (Latino/e LGBT+ provider, community-based setting) | This quote highlights how workforce capacity and staffing practices within the Inner Setting affect engagement. | |
| “I mean, it has been one of the most frustrating things over the last few years when we're engaging and trying to get Spanish speaking individual services and it is like, it is really challenging. The care is not even close to equivalent and even at [our organization], there's all these things. They have … MyChart, it's like the electronic health portal. They just are getting MyChart in Spanish. It's 2024.” (non-Latino/e provider, clinic-based setting) | This quote shows how an organization's physical/technological infrastructure—such as health portals—can fail to meet the linguistic needs of young H/LSMM. | |
| Individuals | “People try to access whether it's healthcare, education or whatnot. And depending on who is behind the desk, whoever that gatekeeper is, if they have that stigma against young Latino men, off the bat there's that push back, there's that you know crossed arms. There is that feeling of I do not understand you, you do not belong, rather than the feeling of our services are open and welcoming.” (Latino/e LGBT+ provider, clinic-based setting) “I have seen it in my own setting at work. I have seen it where [a young H/LSMM] has walked in and had a conversation with … whether it is somebody who works at registration or … within the clinics. And sometimes you will [hear] them say ‘well, I do not understand them.’ But [the young H/LSMM] was speaking English. They may have an accent, but they are speaking English. Or, you know, it's why, you know, the question why comes up a lot? Why do they need that? Why do they ask that? And so, I think it's just a very much a lack of understanding and a lack of willingness to understand.” (Latino/e LGBT+ provider, clinic-based setting) |
These quotes represent the Individuals domain by illustrating how individual biases, such as prejudicial attitudes and assumptions about language ability, create stigmatizing encounters that undermine young H/LSMM's trust and willingness to engage in care. |
| “And so, to me that lack of awareness from providers and a lack of understanding from providers then creates the lack of education. If somebody is, let's say this person is … you know, with partners of multiple genders. That could be confusing and weird to some providers, and they don't even want to get into that. [It becomes] an uncomfortable conversation for the provider, which I think is horrible. Providers should feel comfortable having [those risk reduction] conversations with everybody because [it is not about] what I think is right or wrong. We're focusing on risk and risk reduction.” (Latino/e LGBT+ provider, clinic-based setting) | This quote aligns with the Individuals domain by highlighting individuals’ limited awareness, discomfort, and inadequate skills in discussing diverse sexual behaviors, which can stigmatize young H/LSMM. | |
| “I think all of us as health care providers need to do our part not create the stigma in the first place. And health care providers specifically, I think if they're not thinking about the way that they speak, if they are not careful with their words, they can do a lot of damage and increase the stigma a lot… From my perspective as a provider, I think it's just like I said, I really feel like health care professionals can play a big role in either decreasing stigma or increasing it by a lot if they use the wrong words and cause some distancing with their patient.” (non-Latino/e LGBT+ provider, community-based setting) | This quote illustrates the Individuals domain by emphasizing how providers’ communication practices can either perpetuate stigma or help reduce it. | |
| “And then also that the hope is, is that by saying that it's like, oh, maybe this person won't judge me if I actually say that I reuse needles or I, you know, share a straw with someone when I'm using drugs and maybe more sexually active when I am using some of these different substances to enhance intimacy and maybe I'm not as safe during those times. I think that information is really important as well, but it is how you ask it and it is when you ask it and you have to, you have to use common sense too. Like maybe this is not the right time or maybe I need to build a little bit more rapport and maybe after 10 or 15 min, that person is more likely to be open with me.” (non-Latino/e provider, clinic-based setting) | This quote aligns with the Individuals domain by underscoring the interpersonal skills, such as timing, rapport-building, and nonjudgmental communication, that directly affect whether young H/LSMM's feel comfortable engaging in HIV-prevention care. | |
| Innovation | LGBTQ programming in Latinx communities has been based around HIV prevention, care and treatment and so that stigmatizes HIV further in LGBTQ communities. Because if all [that is being offered] to this community is conversations about [HIV] treatment and prevention, … that is not the only thing that concerns [young H/LSMM]. And so, you see a group of people who have a vast knowledge of HIV, but you do not see them having vast knowledge around where to receive mental health care services or where to receive housing support or where they can do just a variety of things. So, I think there is a need … to include a more holistic approach to the person versus not just pounding in what HIV is and how to prevent it and telling people you need to be on PrEP, and this is your risk. And then talking about it from a place of risk versus choice. And that everybody should be offered PrEP versus doing a risk assessment, because then that is stigmatizing, too. It is like the life that you live puts you at risk versus we are all having sex, we should all consider PrEP and you make the decision if you need it.” (Latino/e provider, community-based setting) | This quote reflects the Innovation domain's design dimension by underscoring the need for holistic HIV-prevention strategies that move beyond narrow biomedical risk messaging to integrate mental health, housing, and other whole-person supports in a culturally responsive model for young H/LSMM. |
| “And so, you know the ways that we can demonstrate explicit inclusivity and make those patients feel more at home are to use signs, to use symbols. So, I am a big advocate of having pins that say your pronouns, having rainbow like things on your badge, lanyards or whatever, because what that does is it helps say to patients that you are safe and you're thinking about them. It's like going out of your way to make that clear. Other ways we could do that, you know, are just the way that we use signage within clinic waiting spaces as well as intake forms. … If you're in a space that is like, it tends to be historically very [heteronormative] …, those kind of things can make a huge difference on patients feeling safe within those environments in kind of like a broader clinic sense and not just centered on the providers.” (non-Latino/e LGBT+ provider, clinic-based setting) | This quote describes how design features can intentionally be crafted to reduce stigma and enhance cultural responsiveness for young H/LSMM. | |
| “The primary intervention was to have someone who speaks the language. [This means] providing services in both English and Spanish … Pretty much all the agencies where I have worked with young people, have involved that family component, and it often was Spanish speaking and with the youth it was in English. [It is important to be] providing culturally sensitive, culturally responsive approach and culturally aware…” (Latino/e LGBT+ provider, clinic-based setting) | This quote illustrates the adaptability dimension of the Innovation Domain, underscoring the need for HIV-prevention services that can be tailored linguistically and culturally. | |
| “It's very clear that … people are recognizing that we are not reaching, and I also will say this gets into, I think [the focus of your study] the Latino community, we are not seeing communities of color in treatment settings. … My question always is like where are these folks? Where are they going? Who are they talking to? Because it is not us in these major healthcare settings, I think that is thinking through more culturally tailored interventions that are less stigmatizing than what we currently offer at the moment.” (non-Latino/e provider, clinic-based setting) | This quote reflects the Innovation Domain by emphasizing the need to adapt prevention services, so they better meet the cultural needs of young H/LSMM. | |
| Process | “Creating signage, creating … avenues where people know that they are welcome, that they feel comfortable. And I think that that goes for every group.” (Latino/e LGBT+ provider, clinic-based setting) | This quote reflects the Process Domain by highlighting specific implementation actions that organizations can use to execute welcoming, non-stigmatizing environments as part of HIV-prevention service delivery. |
| “So, stigma in terms of its effect on transmission, I think whenever we encourage people not to speak about HIV and not to ask about it, I guess I know in many clinical settings the doctors are also not the most well trained in discussing it either, but all of this kind of builds together, I think, to increase transmission because when we are not talking about it, when we are not willing to talk about any kind of STI panel results with our partners, it kind of can lead to transmission happening without knowledge and more knowledge, I think is always beneficial for us about our bodies and everything. (non-Latino/e LGBT+ provider, community-based setting) | This quote represents the Process Domain by emphasizing the implementation strategy of normalizing conversations about HIV and sexual health. | |
| “The labs may be drawn by the staff inside of the exam room and depending on whether or not they want other blood work or other swabs, if they want more general STI testing, one of the issues is that a lot of practitioners do not ask people about risk factors. Particularly I think about, you know, are you engaged in … What type of sex is it, oral intercourse, anal. … I think when you're someone who starts asking those questions, I think patients relax and say, ‘Oh wow, they clearly understand … that I might be using different parts of my body for different sexual activities. This person seems to maybe know what they're talking about a little bit. Maybe I can kind of share a little bit more,’ but I think that visit can look really different just depending on you know, is this just screening? [Does the] person [have] some symptoms and they are worried or they maybe have another sexually transmitted infection…” (non-Latino/e provider, clinic-based setting) | This quote illustrates the Process Domain through actions that providers take during service delivery, such as asking tailored questions, to foster trust and reduce stigma during HIV-prevention visits. | |
| “… We have four white providers in our clinic. … The timing has not worked to bring in a BIPOC provider. It is on my list of things to do but I think that that's also … Who's in your clinic? What does your clinic look like? And are you then going to be able to attract patients that … don't maybe look like me… I think if you have a clinic with ten white providers, it does signal a little bit like, what are your priorities? (non-Latino/e provider, clinic-based setting) | This quote aligns with the Process Domain by describing the planning and decision-making activities organizations undertake, such as efforts to diversify staff, to create environments that support equitable, stigma-reducing HIV-prevention services. | |
| “I also think we need a lot of training for health care workers… So from my perspective, I just wish that we put more emphasis on training people about it and being able to speak about it because I know from the community perspective we are doing as much as we can, but I as a provider am mostly making an influence with how to talk to my patient about more vulnerable diagnoses and I want to make sure that people feel comfortable, confident and don't increase stigma when they're talking about these things because we're in a pretty impactful role that I think we need to try to be more respectful of the stigma that exists and make sure that we're not increasing it. (non-Latino/e LGBT+ provider, community-based setting) | This quote reflects the Process Domain by emphasizing training and capacity-building as key implementation strategies that equip providers with the skills needed to communicate respectfully and prevent stigma during HIV-prevention encounters. |
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.