
Abstract
Background:
There is a paucity of literature regarding the long-term clinical significance and patient-reported outcome measures (PROMs) after isolated microfracture of the knee for cartilage defects.
Purposes:
To (1) define the minimally clinically important difference (MCID) and patient acceptable symptom state (PASS) thresholds for knee microfracture at a minimum 5-year follow-up, and (2) investigate predictive factors—including preoperative, demographic, and intraoperative variables—to achieve MCID and PASS.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
All patients who underwent isolated microfracture for knee chondral defects from 2013 to 2018 were retrospectively identified through a prospectively-maintained institutional database. MCID thresholds were determined by a distribution-based method, while PASS thresholds were established using an anchor-based method. The PROMs analyzed included the International Knee Documentation Committee (IKDC) score and the Knee injury and Osteoarthritis Outcome Score (KOOS). Multivariate logistic regression was performed to identify factors associated with achieving the MCID and PASS thresholds.
Results:
A total of 70 patients were included in the study. The thresholds for MCID achievement and achievement rates were as follows: IKDC, 11.13 (68.57%); KOOS activities of daily living (ADL), 10.56 (65.71%); KOOS Pain, 9.83 (72.86%); KOOS quality of life (QoL), 14.47 (67.14%); KOOS Sport, 14.65 (68.57%); and KOOS Symptoms, 9.95 (58.57%). The thresholds for PASS achievement and achievement rates were as follows: IKDC, 67.24 (58.57%); KOOS ADL, 96.31 (44.29%); KOOS Pain, 85.54 (51.43%); KOOS QoL, 56.38 (55.71%); KOOS Sport, 57.41 (55.71%); and KOOS Symptoms, 76.74 (54.29%). A lower preoperative score was predictive of achieving the MCID for the IKDC and each KOOS subscale. A Kellgren-Lawrence (K-L) grade of 0 or 1 was predictive of achieving the PASS for the IKDC, KOOS Pain, and KOOS Symptoms. A lower body mass index (BMI) was predictive of achieving the PASS for the KOOS ADL and the KOOS Pain, in addition to attaining the MCID for the KOOS ADL, KOOS Pain, and KOOS Sport. A lesion size of <2 cm2 was predictive of achieving the MCID for the IKDC and the KOOS Sport.
Conclusion:
This study defines the thresholds for MCID and PASS achievement at a minimum 5-year follow-up for patients undergoing isolated microfracture of the knee. Patient-specific and defect-specific factors associated with MCID and PASS achievement included lower BMI, younger age, male sex, lower K-L grade, and smaller lesion sizes.
Chondral knee injuries are identified in up to 66% of knee arthroscopies and arise from a variety of causes, such as acute trauma, joint instability, degenerative processes, or chronic joint overload.1,32 Because cartilage has limited inherent regenerative capacity, chondral defects tend to worsen over time and may contribute to ongoing pain, swelling, and additional degenerative changes.5,38 When patient symptoms are not managed well with nonoperative treatment, surgery is recommended. The specific surgical treatment is guided by both patient-specific and defect-specific factors. While alternatives such as autologous chondrocyte implantation (ACI/MACI), osteochondral allograft transplantation (OCA), and osteochondral autograft transfer (OATS) serve as reliable treatment options, they are better suited for larger defects, require longer operative time, greater technical skill, and are associated with long recoveries.5,29,30,31 For appropriately small-sized focal defects, microfracture of the subchondral bone is easily performed with minimal technical demands and can be done all arthroscopically.6,21,24,27
Microfracture creates a conductive, suitable microenvironment that enhances the body's innate regenerative capacity by releasing marrow cells and cytokines, thereby promoting tissue repair. 40 Through this process, chondral defects can be regenerated into a fibrocartilaginous surface. 39 Clinically significant results at a 2-year follow-up have been previously reported by Chahla et al, 8 with the use of minimum clinically important difference (MCID) and patient acceptable symptom state (PASS). In particular, MCID defines the smallest improvement that a patient can clinically appreciate, while PASS considers persistent symptoms and functional impairments to determine a benchmark for an acceptable state after an intervention.7,16,25 However, clinical studies after isolated microfracture demonstrate a potential deterioration over time at mid- or long-term follow-up.18,36,41 Therefore, it is critical to evaluate the achievement of clinically significant outcomes, such as MCID and PASS, at longer-term follow-up and to identify which patients are more likely to achieve success with this treatment.
This study aimed to (1) define the MCID and PASS thresholds for arthroscopic knee microfracture at a minimum 5-year follow-up; (2) investigate predictive factors—including preoperative, demographic, and intraoperative variables—to achieve MCID and PASS thresholds. The authors hypothesized that preoperative scores and lower body mass index (BMI) would be associated with greater MCID and PASS achievements.
Methods
Patient Selection
A retrospective study was conducted using a prospectively maintained database from a single, high-volume institution. The inclusion criteria consisted of patients who had previously failed nonoperative management for symptomatic cartilage defects and subsequently underwent primary arthroscopic isolated microfracture of the knee for a tibiofemoral cartilage defect, with a minimum of 5 years of postoperative follow-up. All eligible patients were operated on by 1 of 3 fellowship-trained surgeons (B.J., N.N.V., and B.J.C.) between January 2013 and September 2018. The exclusion criteria included patients undergoing revision microfracture procedures, those with a history of cartilage-preserving procedures before microfracture, patients with a concomitant ligamentous knee injury, and those lacking documented patient-reported outcome measures (PROMs). Patients with coronal deformity requiring an osteotomy (limb malalignment >5°) and those with significant meniscal tears requiring repair were also excluded. Furthermore, patients who underwent ipsilateral knee surgery within the 5-year follow-up period and those with incomplete PROMs at the final follow-up were excluded from the analysis. Prior approval from the institutional review board was obtained for database querying and patient follow-up.
Demographic and Outcome Measures
An institutional electronic medical record was reviewed to collect descriptive data—including age, sex, injury laterality, and BMI. Preoperative Rosenberg flexion weightbearing radiographs were also evaluated for the severity of osteoarthritis by using the Kellgren-Lawrence (K-L) classification. Mechanical axis was measured on standing long-leg films, with the angle defined as the deviation from a straight line connecting the center of the femoral head to the center of the talus. Intraoperative details, including lesion size (cm2), location, and defect quantity, were also documented. Preoperative and final follow-up PROMs were assessed, which included the International Knee Documentation Committee Score (IKDC), Knee injury and Osteoarthritis Outcome Score (KOOS) for Activities of Daily Living (ADL), KOOS Pain, KOOS Quality of Life (QoL), KOOS Symptoms, and KOOS Sport. PROMs were distributed and stored using a secure electronic platform (Patient IQ). The MCID was defined as the smallest, clinically significant change in a patient's condition. In contrast, the PASS was defined as the point at which patients consider themselves to be in a satisfactory state of health.8,10,19,34 During the final follow-up, patients were asked the following anchor question for the PASS: “Considering all the activities in your daily life, your pain level, and functional impairment, do you consider your current state satisfactory?” in which a yes or no response was given.
Surgical Technique and Rehabilitation
All microfracture procedures were performed arthroscopically through standard portals. After diagnostic arthroscopy, the focal cartilage defect was identified, and any loose or unstable cartilage surrounding the lesion was debrided using a curette to create stable walls. Microfracture of the exposed subchondral bone was then performed using either a 1.5-mm PowerPick (Arthrex) or a Steadman awl, based on surgeon preference. Multiple perforations, approximately 2 to 4 mm in depth and spaced 3 to 4 mm apart, were created across the base of the defect to elucidate bleeding from the subchondral bone. After a uniform array of tunnels was made, the arthroscopic fluid pressure was reduced to 10 mmHg to ensure adequate bleeding from the marrow elements at each perforation site. In a subset of patients (n = 10), the microfracture procedure was augmented with the bone marrow aspirate concentrate (BMAC). The BMAC was harvested from the iliac crest using a standard aspiration technique, processed using a centrifugation system (Arthrex Angel System), and applied directly to the treated cartilage defect.
Postoperatively, a standardized rehabilitation regimen was implemented based on the location of the cartilage defect. All patients were initially placed in a hinged knee brace locked in full extension. For femoral condyle and tibial plateau defects, the brace was maintained in full extension for the first 72 hours. Continuous passive motion (CPM) was then initiated for 6 to 8 hours per day in 2-hour intervals, starting from 0° to 40° of flexion. Flexion was gradually increased by 5° to 10° daily, up to a maximum of 90°, and CPM was continued daily for 6 to 8 weeks. Patients were instructed to remain touch-down weightbearing with crutches for 6 weeks. Progression to partial weightbearing occurred between weeks 6 and 8, with advancement to full weightbearing typically by 8 weeks.
For patellar and trochlear lesions, patients were maintained in full extension for 3 days before the initiation of CPM. CPM was used for 6 to 8 hours per day in 2-hour intervals, from 0° to 60° of flexion, for the first 4 weeks. Flexion was advanced as tolerated to a maximum of 90° before discontinuation. Patients were allowed full weightbearing in the hinged knee brace immediately after the procedure, as tolerated.
Statistical Analysis
Data analysis was performed using R software (8238 Big Sur ARM build, R Foundation for Statistical Computing). After confirmation of normality via the Shapiro-Wilk test, a 2-tailed, paired Student t test was performed to compare pre- and postoperative PROM scores. A distribution-based approach was utilized for calculating the MCID for each PROM. In line with the established literature, 43 the MCID was determined to be one-half the standard deviation of the difference from baseline in PROM scores at a minimum 2-year follow-up. PASS thresholds were calculated using an anchor-based approach. Receiver operating characteristic analysis for the calculation of PASS was conducted using the “pROC” package. Optimal thresholds were calculated using the Youden Index to maximize the sensitivity and specificity of threshold values. To identify patient-related factors at baseline and intraoperative variables associated with achieving the MCID and PASS, multivariate logistic regression analyses were conducted using the Akaike Information Criterion for model selection. This was completed using the “stepAIC” function within the “MASS” package in R. K-L grades were treated as a binary variable (minimal to mild osteoarthritis [OA] [K-L, 0-1] vs moderate to advanced OA [K-L, 2-3]). A subgroup analysis was performed to evaluate the MCID and PASS achievement rates between the BMAC-augmented subgroup (n = 10) and the nonaugmented subgroup (n = 60).
Results
A total of 468 patients who underwent knee microfracture at a single institution from January 2013 to September 2018 were identified. Of these patients, 103 were eligible for a 5-year follow-up, and ultimately, 70 patients were included with complete PROMs (68% compliance) (Figure 1). Included patients had a mean follow-up of 7.06 ± 1.49 years. The cohort consisted of 64.3% men and had a mean age of 33.54 ± 15.14 years at the time of surgery. The majority of the cohort had symptoms for >12 months (n = 46; 70.7%). A total of 37 patients (52.9%) had a K-L grade of 0 or 1, while 33 patients (47.1%) had a K-L grade of 2 or 3 immediately before surgery. The cohort was 1.1°± 3.2° of varus on average (Table 1). Twelve patients (17.1%) underwent partial meniscectomy for meniscal tears of the periphery (n = 7 medial meniscus; n = 5 lateral meniscus). The mean lesion size was 1.95 ± 1.53 cm2, and 25 (35.7%) of lesions were >2 cm2. The most common locations for cartilage defects were the medial femoral condyle (n = 24; 34.3%), the trochlea (n = 17; 24.3%), and the lateral femoral condyle (n = 16; 22.9%). Eight patients (11.4%) had cartilage defects in multiple locations (Table 2).

Flow chart of patient inclusion. PROMS, patient-reported outcome measures.
Demographic and Intraoperative Characteristics of the Patients a

Data are presented as mean (SD), or n/n (%). BMI, body mass index; K-L, Kellgren-Lawrence.
Mechanical axis reported in degrees of varus.
Intraoperative Cartilage Lesion Characteristics a
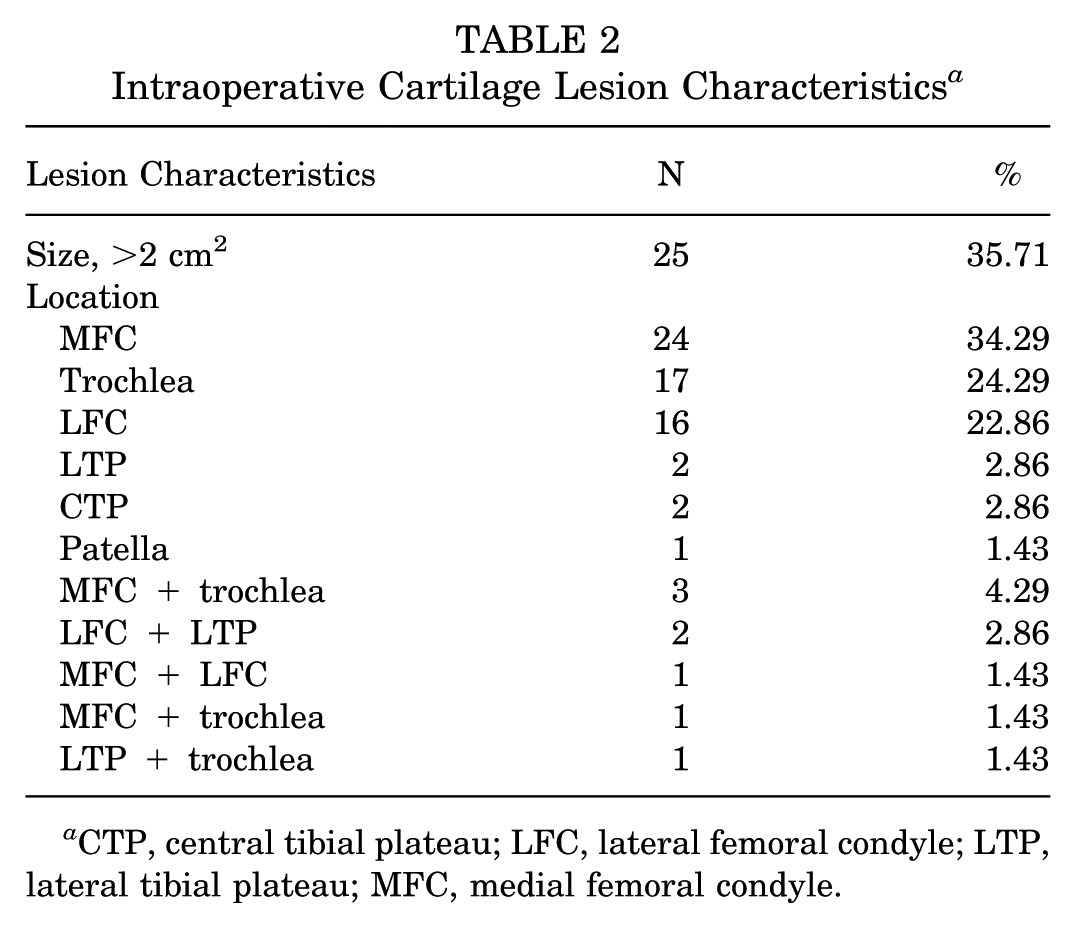
CTP, central tibial plateau; LFC, lateral femoral condyle; LTP, lateral tibial plateau; MFC, medial femoral condyle.
The mean preoperative score, mean postoperative score, MCID threshold, MCID achievement rate, PASS threshold, and PASS achievement rates for IKDC and KOOS subscores are listed in Table 3. The predictive value for all PASS thresholds was good to excellent, with area under the curve values for IKDC and KOOS subscores ranging from 0.778 to 0.903 (Figure 2).
MCID and PASS Thresholds and Percentage Achievement Among Study Patients a
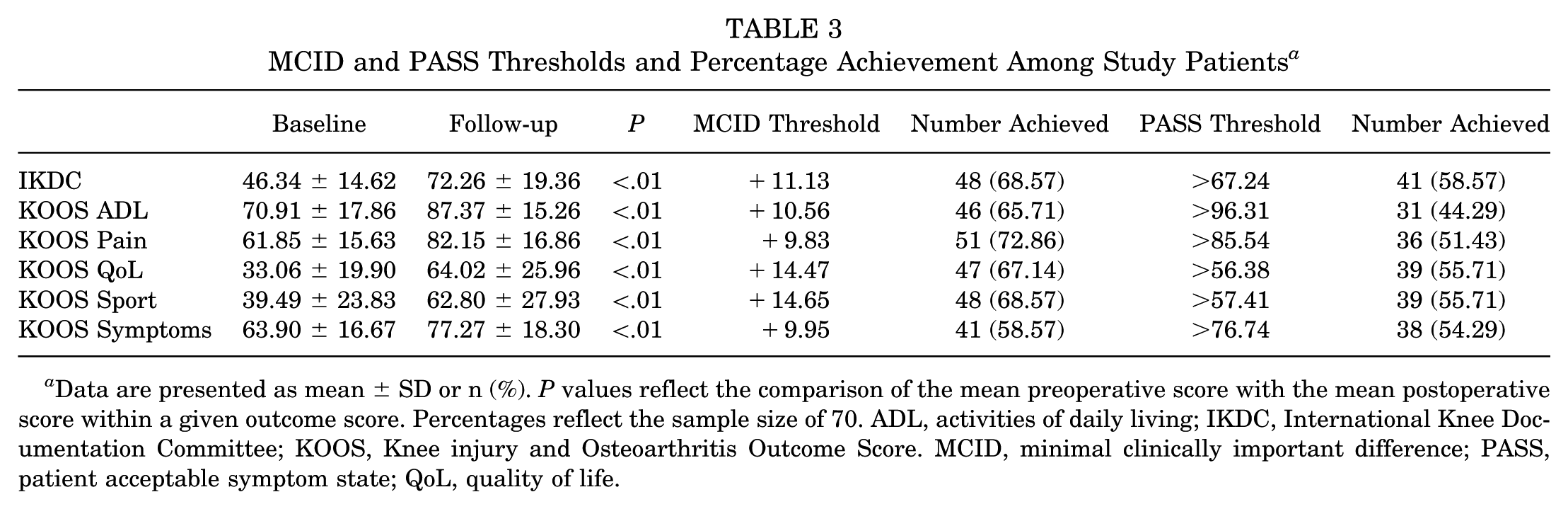
Data are presented as mean ± SD or n (%). P values reflect the comparison of the mean preoperative score with the mean postoperative score within a given outcome score. Percentages reflect the sample size of 70. ADL, activities of daily living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score. MCID, minimal clinically important difference; PASS, patient acceptable symptom state; QoL, quality of life.

ROC curves for PASS thresholds. IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; PASS, patient acceptable symptomatic state; ROC, receiver operating characteristic; QoL, quality of life.
Factors Predictive of MCID/PASS Achievement
For the IKDC, lower weight (odds ratio [OR], 0.98 [95% CI, 0.96-0.99]; P = .03), lower preoperative score (OR, 0.93 [95% CI, 0.90-0.95]; P = .01), and smaller intraoperative lesion size (OR, 0.17 [95% CI, 0.02-0.86]; P = .04) were predictive of MCID achievement, whereas lower weight (OR, 0.98 [95% CI, 0.97-0.99]; P = .04) and K-L grades of 0 or 1 (OR, 4.12 [95% CI, 1.29, 14.82]; P = .02) were predictive of PASS achievement (Tables 4 and 5).
Significant Predictors of MCID Achievement in Logistic Regression Analyses a
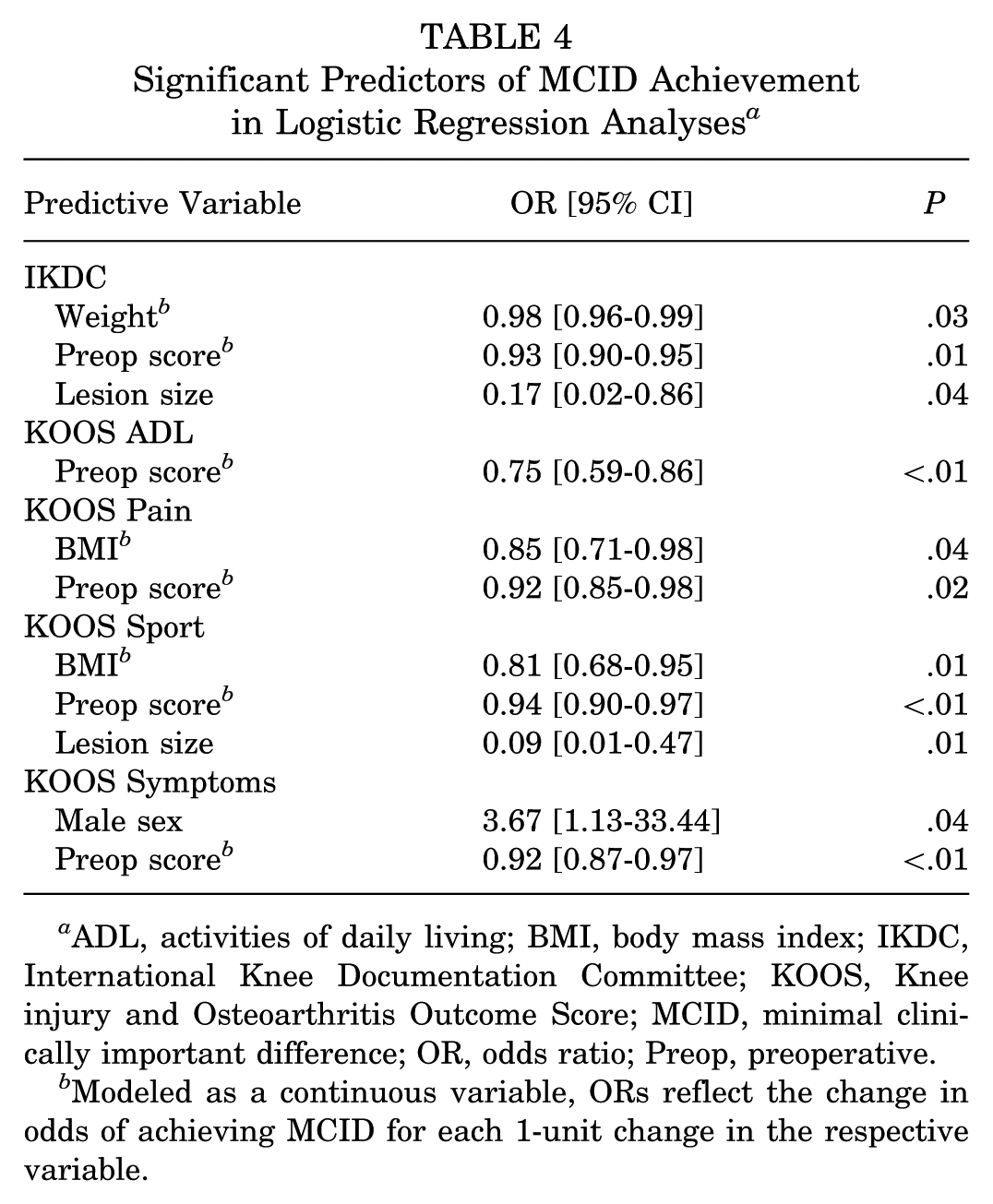
ADL, activities of daily living; BMI, body mass index; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; MCID, minimal clinically important difference; OR, odds ratio; Preop, preoperative.
Modeled as a continuous variable, ORs reflect the change in odds of achieving MCID for each 1-unit change in the respective variable.
Significant Predictors of PASS Achievement in Logistic Regression Analyses a
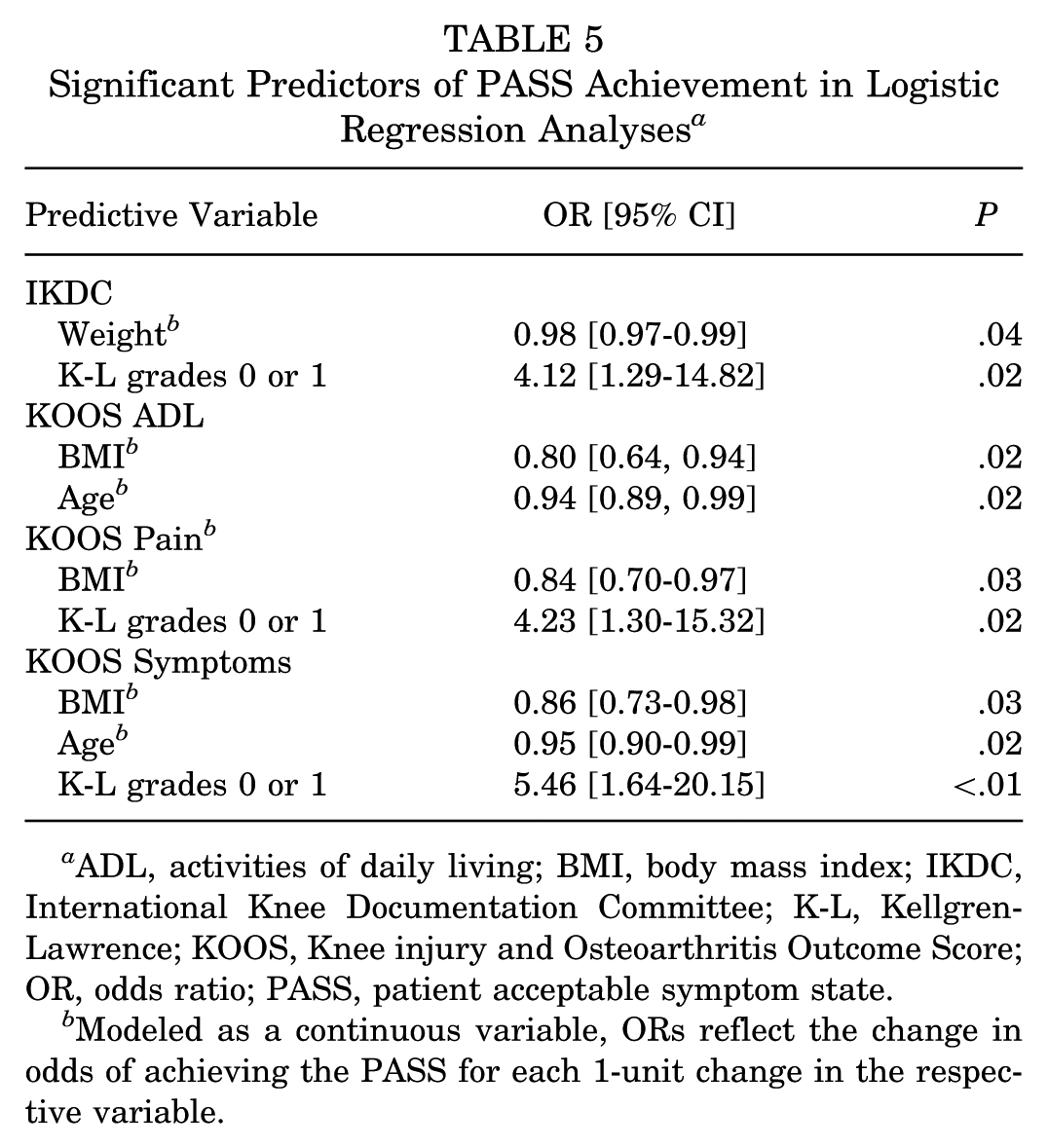
ADL, activities of daily living; BMI, body mass index; IKDC, International Knee Documentation Committee; K-L, Kellgren-Lawrence; KOOS, Knee injury and Osteoarthritis Outcome Score; OR, odds ratio; PASS, patient acceptable symptom state.
Modeled as a continuous variable, ORs reflect the change in odds of achieving the PASS for each 1-unit change in the respective variable.
For the KOOS ADL, lower preoperative score (OR, 0.75 [95% CI, 0.59-0.86]; P < .01) was predictive of MCID achievement, whereas lower BMI (OR, 0.80 [95% CI, 0.64-0.94]; P = .02) and younger age (OR, 0.94 [95% CI, 0.89-0.99]; P = .02) were predictive of PASS achievement. For the KOOS Pain, lower BMI (OR, 0.85 [95% CI, 0.71-0.98]: P = .04) and lower preoperative score (OR, 0.92 [95% CI, 0.85-0.98]; P = .02) were predictive of MCID achievement, whereas lower BMI (OR, 0.84 [95% CI, 0.70-0.97]; P = .03) and K-L grades 0 or 1 (OR, 4.23 [95% CI, 1.30- 15.32]; P = .02) were predictive of PASS achievement. For the KOOS Sport, lower BMI (OR, 0.81 [95% CI, 0.68-0.95]; P = .01), lower preoperative score (OR, 0.94 [95% CI, 0.90-0.97]; P < .01), and smaller intraoperative lesion size (OR, 0.09 [95% CI, 0.01-0.47]; P = .01) were predictive of MCID achievement, whereas no variables were predictive of PASS achievement. For the KOOS Symptoms, male sex (OR, 3.67 [95% CI, 1.13-33.44]; P = .04) and lower preoperative score (OR, 0.92 [95% CI, 0.87-0.97]; P < .01) were predictive of MCID achievement, whereas lower BMI (OR, 0.86 [95% CI, 0.73-0.98]; P = .03), younger age (OR, 0.95 [95% CI, 0.90-0.99]; P = .02), and K-L grades 0 or 1 (OR, 5.46 [95% CI, 1.64-20.15]; P < .01) were predictive of PASS achievement.
Subanalysis of BMAC-Augmented Microfracture Versus Nonaugmented Microfracture
A total of 10 patients underwent BMAC augmentation, while the nonaugmented subgroup consisted of 55 patients. No significant differences were found in MCID achievement for the IKDC (BMAC [50%] vs non-BMAC [71.7%]; P = .172), the KOOS ADL (BMAC [70%] vs non-BMAC [65%]; P = .758), the KOOS Pain (BMAC [60%] vs non-BMAC [75%]; P = .323), the KOOS QoL (BMAC [60%] vs non-BMAC [68.3%]; P = .603), the KOOS Sport (BMAC [70%] vs non-BMAC [68.3%]; P = .916), and the KOOS Symptoms (BMAC [60%] vs non-BMAC [58.3%]; P = .921). Furthermore, no significant differences were found in PASS achievement for the IKDC (BMAC [50%] vs non-BMAC [60%]; P = .552), the KOOS ADL (BMAC [50%] vs non-BMAC [43.3%]; P = .694), the KOOS Pain (BMAC [40%] vs non-BMAC [53.3%]; P = .435), the KOOS QoL (BMAC [60%] vs non-BMAC [55%]; P = .768), the KOOS Sport (BMAC [50%] vs non-BMAC [56.7%;] P = .694), and the KOOS Symptoms (BMAC [40%] vs non-BMAC [53.3%]; P = .328).
Discussion
This study analyzed long-term clinical outcomes in a large cohort of patients who underwent isolated arthroscopic microfracture of the knee at a single, high-volume institution, and established MCID and PASS thresholds for the IKDC and KOOS subscales at a 5-year follow-up. Moreover, this investigation delves into pre- and intraoperative variables that may serve as predictive indicators for achieving MCID and PASS after this procedure. Factors associated with clinically significant outcomes at a minimum of 5 years after arthroscopic microfracture included preoperative scores, a lower BMI, younger age, male sex, a smaller degree of arthritic changes, and a smaller lesion size.
The present study reports on a minimum of 5-year postoperative outcomes after arthroscopic microfracture for chondral defects of the knee (mean follow-up, 7.06 ± 1.49 years). At final follow-up, there was a significant improvement in all PROMs, suggesting that in appropriately indicated patients, microfracture can be successful at midterm follow-up. In this study, 5-year thresholds were also established for the MCID and PASS. In total, 82.85% of patients achieved the MCID threshold for at least 1 of the 6 PROMs evaluated, and 37.81% achieved the MCID for all of the PROMs, with a range from 58.57% to 72.86% per PROM. The rates of PASS achievement were lower, with 71.43% of patients meeting PASS criteria for at least 1 of the 6 evaluated PROMs and 34.28% for all the PROMs (range, 44.29% to 58.57% per individual PROM). The finding of overall lower achievement rates for PASS thresholds is typical, as the PASS requires a patient to be satisfied with their symptom state, whereas the MCID only requires a noticeable improvement. Furthermore, lower preoperative scores being associated with a greater chance of achieving the MCID but not PASS is in line with previous literature, 8 as patients with lower scores have a greater room to improve, with less of a ceiling effect.
Because some data suggest that the durability of microfracture may be less than that of other cartilage restoration procedures,3,13-15,28,31,35,36,37 it is important to evaluate the ability to achieve meaningful outcomes over time. Chahla et al 7 established MCID and PASS thresholds in 206 patients undergoing microfracture, with a minimum 2-year follow-up. In that study, MCID and PASS thresholds were calculated at each of the 6-, 12-, and 24-month postoperative time points. Interestingly, the score differences or scores required to meet criteria for MCID or PASS tended to increase over time, with all of the 24-month thresholds exceeding the 6- and 12-month thresholds. 8 Furthermore, more patients achieved MCID over time; however, the proportion achieving PASS began to decline at the end of 24 months. 8 Notably, the MCID thresholds for microfracture previously established by Chahla et al 8 at a 2-year follow-up term were higher than those established in this study for IKDC (16.7 vs 11.13), KOOS ADL (11.2 vs 10.56), KOOS Pain (10.5 vs 9.83), KOOS Sport (15.1 vs 14.65), and KOOS Symptoms (10.2 vs 9.95). As the MCID was defined using the distribution method as one-half the standard deviation of the difference in preoperative and final follow-up scores among both studies, the consistent decrease in the MCID thresholds can be attributed to functional decline from 2 years to 5 years postoperatively.
Compared with other cartilage restoration procedures, microfracture appears to have inferior MCID and PASS achievement rates beginning at midterm follow-up.12,17,26 A systematic review and meta-analysis consisting of 89 studies and 3984 patients undergoing microfracture, OATS, ACI/MACI, and OCA for the treatment of symptomatic cartilage defects evaluated clinically significant outcome achievement across short- (1-4 years), mid- (5 to 9 years), and long-term (≥10 years) follow-up. 17 Despite microfracture being performed for the smallest lesion sizes, it showed reduced durability beginning at 5 years of follow-up compared with ACI and OATS. 17 The difference in MCID achievement is likely attributed to the fibrocartilage produced by microfracture, which is biomechanically inferior to hyaline-like cartilage restored by ACI, OCA, or OATS. These findings highlight the importance of patient selection, where ACI or OATS may be preferable for patients with larger defects or higher activity levels.5,29,30,31
Given concerns about durability in the mid- to long-term, previous studies have investigated enhancing microfracture with scaffolds, regenerative cells, and growth factors to improve outcomes.40,42 In this study, a subset of the cohort (n = 10) underwent knee microfracture with BMAC augmentation. Fortier et al 11 previously performed a systematic review of the literature, reporting that BMAC augmentation does not significantly improve IKDC, visual analog scale, or Western Ontario and McMaster Universities Osteoarthritis Index scores in patients undergoing knee microfracture for cartilage defects. 11 Our study further substantiates these findings as no significant differences were observed between BMAC-augmented and non-augmented microfracture across all PROMs. However, further studies with larger sample sizes are warranted to assess whether BMAC augmentation results in differences in clinically significant outcome achievement after knee microfracture.
One of the most consistent predictors of MCID and PASS achievement was BMI. Historically, BMI has been associated with worse outcomes after microfracture. In some of the earlier microfracture studies, Mithoefer et al21,22,23 found that an elevated BMI, particularly >30, resulted in poorer short-term clinical outcomes, as well as worse fill on MRI. However, more recent studies have not identified BMI to be a specific risk factor for reoperation or worse outcomes.3,43 BMI was also not recognized as a predictor of MCID or PASS achievement within 2 years of microfracture surgery. 8 It is possible that over a greater period of time, a greater BMI results in increased loads and forces over the knee, making it more challenging for the fibrocartilaginous repair tissue to support the knee joint; however, ongoing data and analysis of clinically significant outcomes at longer-term follow-up are needed to evaluate this hypothesis.
Another commonly evaluated factor for cartilage restoration procedures is the lesion size. Traditionally, microfracture has been best suited for smaller focal lesions with stable walls that are contained and on the femoral condyles. Numerous studies suggest that a larger lesion size is predictive of an unsuccessful outcome or the need for reoperation after microfracture.13,22,23,41 Smaller lesion size is associated with MCID and PASS achievement at short-term follow-up, 7 which remained consistent in the present study at midterm follow-up. Altogether, these data emphasize the importance of vigilance in selecting microfracture for smaller lesions and considering other cartilage restoration techniques for larger lesions.
Other patient-specific variables associated with clinically significant outcomes at a 5-year follow-up were younger age, male sex, and lower K-L grade. Each of these had associations with both the MCID and PASS. Younger age has also been regularly associated with better outcomes after microfracture, in addition to a higher chance of achieving the MCID and PASS at short-term follow-up.8,13,20,23,41 Younger patients may have improved vascularity to the chondral surfaces and better regenerative potential. We also found that male sex was predictive of MCID achievement on the KOOS Symptom subscale, which is consistent with the findings by Weber et al, 41 demonstrating that male patients had better outcome scores than their female counterparts. In addition, male sex was also linked to greater odds of achieving the MCID and PASS at 2 years with microfracture. Lastly, greater preoperative coronal plane deformity and degenerative changes have previously been linked to poorer outcomes. 3 When patients have greater arthritic changes noted on radiographic assessment, the compartment and chondral surfaces face greater load, which makes the success of a fibrocartilaginous chondral surface less likely.
Understanding the preoperative patient-specific and lesion-specific factors that predict clinically significant outcomes is crucial for selecting the optimal patients for microfracture. Poor patient selection can not only result in poor outcomes from the primary procedure but may also affect the success of subsequent cartilage restoration treatment.9,33 The data from the present study can be utilized in patient counseling for expectations after microfracture treatment of appropriately indicated defects if nonoperative treatment is unsuccessful in managing symptoms.
Limitations
This study possesses several limitations that warrant careful consideration. Given the retrospective observational design of this study, we can only determine factors associated with MCID and PASS achievement, rather than predictive variables. Furthermore, the absence of radiographic follow-up in our study limits our ability to assess the correlation between structural changes and clinically significant outcomes. Future studies incorporating serial radiographic evaluations could provide valuable insights into these relationships. Moreover, the findings in this study are specific to a select cohort of patients with isolated chondral knee pathology who underwent microfracture. Additional single-stage procedures to supplement lesions undergoing microfracture, such as a micronized allogenic cartilage matrix (eg, BioCartilage Extracellular Matrix; Arthrex, Inc), matrix-augmented autologous chondrocyte transplantation (eg, AutoCart; Arthrex, Inc), or particulated juvenile cartilage implants (eg, DeNovo; Zimmer Biomet), may affect outcomes2,11 and were not specifically evaluated in the present study.
Because of the retrospective nature of the study design, we were unable to reliably capture precise time intervals (in days) between the onset of symptoms and surgery, as well as the cause of chondral defects (traumatic vs atraumatic/degenerative), which may influence outcomes. Additionally, treating K-L grades as a binary variable (K-L 0-1 vs K-L 2-3) due to limited statistical power may obscure potential differences in outcomes between moderate (K-L 2) and severe (K-L 3) OA, as more advanced degenerative changes could negatively affect microfracture success. Notably, a subset of the present cohort (n = 10/70) underwent microfracture augmented with BMAC, which may introduce variability in our results. 11 Furthermore, alterations in technique, including microdrilling over traditional microfracture, may also change PROM scores. 4
Although we successfully portrayed the midterm outcomes of knee microfracture, it is essential to acknowledge that our cohort originated from a single, high-volume institution, which may limit the external validity of our findings. Furthermore, a potential performance bias may exist within our study due to the predominance of procedures (51/70, 72.9%) being performed by a single surgeon (B.J.C.). Given the constraints of our sample size and the multitude of independent variables in our regression analysis, there is an increased potential of a type 2 error. Additionally, this cohort comprises a sample of patients with chondral defects in various compartments of the knee, which limits our ability to make conclusions regarding defect-specific location. Furthermore, while we found intraoperative lesion size to be predictive of achievement of clinically significant outcomes, this is inherently not an actionable variable for preoperative counseling. Finally, the outcomes were measured at a single time point, with a minimum follow-up of 5 years postoperatively. While this provides valuable information on midterm outcomes, it limits our ability to assess differences in clinically significant outcome achievement between the 2- and 5-year time points. To substantiate these findings, future studies should employ larger sample sizes, include patients from multiple centers, and encompass a comprehensive set of radiographic parameters both pre- and postoperatively.
Conclusion
This study defines the thresholds for the MCID and PASS achievement at a minimum 5-year follow-up in a cohort of patients undergoing isolated arthroscopic microfracture of the knee. More patients achieved the MCID than the PASS for the majority of PROMs, and lower preoperative scores were predictive of the MCID. Patient-specific and defect-specific factors associated with the MCID and PASS achievement included lower BMI, younger age, male sex, lower K-L grade, and smaller lesion sizes.
Footnotes
Final revision submitted June 14, 2025; accepted July 8, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.A. has received hospitality payments from Davol Inc, Encore Medical LP, and Styker Corporation; and support for education from Smith & Nephew, Inc. A.B.Y. has received hospitality payments from Aesculap Biologics, LLC, Breg, Linvatec, Joint Restoration Foundation, Inc, Vericel Corporation, and Zimmer Biomet Holdings, Inc; is a paid consultant for AlloSource, JRF Ortho, Olympus America, Inc, and Stryker; has received research support from Arthrex, Inc, and Organogenesis; owns stock or stock options in Icarus Medical, Patient IQ, and Sparta Biomedical; has received support for education from Medwest Associates; and is an unpaid consultant for Patient IQ and Sparta Biomedical. B.F. has received hospitality payments from AbbVie Inc, Amgen Inc, DePuy Synthes Sales Inc, Linvatec Corporation, and Vericel Corporation; has received research support from Arthrex, Inc, Smith & Nephew, and Stryker; has received publishing royalties, financial, or material support from Elsevier; owns stock or stock options in iBrainTech, Sparta Biopharma, and Zuno Medical; has received support for education from Midwest Associates; and is a paid consultant for Smith & Nephew and Stryker. N.N.V. has received hospitality payments from Abbot Laboratories, Axonics Inc, Boston Scientific Corporation, Foundation Fusion Solutions LLC, Nalu Medical Inc, Nevro Corp, Orthofix Medical Inc, Pacira Pharmaceuticals Incorporated, Relievant Medsystems Inc, Salix Pharmaceuticals, Vericel Corporation, and Vertos Medial Inc; receives intellectual property (IP) royalties from Arthrex, Inc, Graymont Professional Products IP LLC, Smith & Nephew, and Stryker; has received research support from Arthrex, Inc, Breg, Ossur, Smith & Nephew, and Stryker; is a paid consultant for Medacta USA Inc, and Stryker; has received support for education from Medwest Associates; and has received travel and lodging from Spinal Simplicity LLC. J.C. is a paid consultant for Arthrex, Inc, CONMED Linvatec, Ossur, RTI Surgical Inc, Smith & Nephew, and Vericel Corporation; has received hospitality payments from Breg Inc, DePuy Synthes Sales Inc, Joint Restoration Foundation Inc, Medical Device Business Services Inc, Pacira Pharmaceuticals Incorporated, SI-Bone Inc, and Vericel Corporation; and has received support for education from Midwest Associates. B.J.C. has received research support from Aesculap/B. Braun, Arthrex, Inc, and the National Institutes of Health (National Institute of Arthritis and Musculoskeletal and Skin Diseases [NIAMS] and National Institute of Child Health and Human Development [NICHD]); is a paid consultant for Acumed LLC, Arthrex, Inc, Bioventus LLC, DJO LLC, Endo Pharmaceuticals Inc, Flexion Therapeutics Inc, Geistlich Pharma, North America Inc, Pacira Pharmaceuticals Incorporated, and Vericel Corporation; receives IP royalties from Arthrex, Inc, and Elsevier Publishing; owns stock or stock options in Bandgrip Inc and Ossio; has received hospitality payments from Encore Medical LP, Flexion Therapeutics Inc, GE Healthcare, Geistlich Pharma, North America Inc, Mallinckrodt LLC, Merck Sharpe and Dohme Corporation, Organogenesis Inc, Orthofix Medical Inc, PAVmed Inc, Pinnacle Inc, Pylant Medical, Summit Surgical Corp, Trice Medical Inc, and Zimmer Biomet Holdings Inc; has received other financial or material support from JRF Ortho; and is a paid presenter for LifeNet health and Terumo BCT. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Rush University Medical Center (IRB: 15031009).