
Abstract
Background:
Patellar instability is common in skeletally immature patients; however, the presence of open physes presents unique challenges to surgical management.
Purpose:
To (1) assess the safety and efficacy of anatomic medial patellofemoral ligament reconstruction (MPFL-R) in a skeletally immature patient population at short-, mid-, and long-term follow-up and (2) determine the influence of patient factors and surgical and radiographic characteristics on the risk of recurrent instability and clinical outcomes after surgery.
Study Design:
Case series; Level of evidence, 4.
Methods:
A retrospective analysis was conducted of the records of skeletally immature patients who underwent primary, anatomic MPFL-R with concomitant procedures at a single academic institution between 2010 and 2019. Patients with <2 years of follow-up were excluded. Demographic data, preoperative radiographic parameters, and surgical details were collected through chart review. Recurrent instability, growth disturbance, and return-to-sport rates were documented via telephone follow-up. The final follow-up included assessment of Kujala, Lysholm, and International Knee Documentation Committee (IKDC) scores. Subgroup analysis focused on patients undergoing isolated MPFL-R.
Results:
A total of 54 knees in 51 skeletally immature patients with a mean age of 15.6 years (range, 10-18 years) were available for analysis. At a mean follow-up of 8.15 years (range, 55-152 months), 4 of 54 (7.4%) knees experienced subsequent patellar subluxation events. There were no confirmed patellar dislocations, and no patients underwent reoperation for patellar stabilization or growth disturbance. At the final follow-up, the mean Kujala, Lysholm, and IKDC scores were 85.7 (range, 11-100), 83.6 (range, 14-100), and 76.1 (range, 10-95.4), respectively. Patients with a younger age at the time of surgery (hazard ratio, –0.83; 95% CI, –1.53 to −0.14; P = .018) and an increased patellar tendon–to–lateral trochlear ridge (PT-LTR) distance (13.46 vs 8.59 mm; P = .043) demonstrated an increased risk of recurrent patellar instability. Three of 23 (13.0%) knees undergoing isolated MPFL-R, experienced subsequent patellar subluxation events. In subgroup analysis, high-grade trochlear dysplasia (P = .002) and PT-LTR distance >5.55 mm (P = .004) correlated with an increased risk of recurrent instability events.
Conclusion:
Anatomic MPFL-R paired with concomitant procedures as indicated is a safe, efficacious, and durable treatment option for lateral patellar instability in adolescent patients with an open or partially open distal femoral physis.
Keywords
Patellar instability is a common condition in adolescents, occurring in approximately 29 to 43 per 100,000 persons aged 10 to 17 years, exceeding the rate found in the adult patient population.14,32,35,47 The incidence of recurrent instability events in the skeletally immature population is correspondingly high, with reported rates as great as 69% after an initial patellar dislocation. 23 Recurrent patellar instability may result in significant functional disability for patients and the development of early osteoarthritis due to repeated osteochondral injury. 37 Appropriate surgical management, therefore, is indicated in these patients after a first-time patellar dislocation associated with a displaced osteochondral fragment or significant underlying anatomic risk factors and in patients with recurrent instability episodes.3,15,19,35-37,47
Surgical treatment of patellar instability in patients with open physes presents unique challenges to the correction of multifactorial soft tissue and osseous characteristics that contribute to its occurrence.15,35,47 Likewise, numerous surgical techniques for medial soft tissue repair and reconstruction have been described for use in the skeletally immature patient population to avoid injury to the physis.16,23,29,32,35,45-47 While anatomic medial patellofemoral ligament reconstruction (MPFL-R) is possible given the femoral insertion of the MPFL being just distal to the distal femoral physis, its close proximity renders this procedure more technically demanding.15,35 Concerns exist regarding the possibility of inducing growth disturbance or arrest. 41 Modifications to the biomechanically ideal insertion point of the MPFL on the femur in an attempt to avoid the physis may compromise graft isometry and lead to poorer functional outcomes and graft failure.4,5,10,38,39 While short-term follow-up studies have demonstrated anatomic MPFL-R in skeletally immature patients to be safe and effective in treating recurrent patellar instability, skeletally immature patients have higher rates of recurrent instability than adult patients after isolated MPFL-R.1,11,15,22,24,34,42
Therefore, the primary purpose of this study was to (1) assess the safety and efficacy of anatomic MPFL-R in a skeletally immature patient population at short-, mid-, and long-term intervals and (2) explore potential associations between patient factors, preoperative radiographic parameters, and surgical characteristics with the risk of recurrent instability and clinical outcomes after surgery. We hypothesized that anatomic MPFL-R would be safe, efficacious, and durable in addressing recurrent patellar instability in skeletally immature patients.
Methods
Study Population and Design
This retrospective case series was performed at a single academic institution, and the records of all skeletally immature patients who underwent primary MPFL-R between January 2010 and December 2019 were reviewed for potential inclusion. Institutional review board approval was obtained, and all individuals provided informed consent for participation. Patients were excluded if they were >18 years of age or had undergone previous ipsilateral tibial tubercle osteotomy (TTO) or trochleoplasty. Patients were then evaluated via MRI to confirm the presence of open or partially open physes at the time of index surgery (Figure 1). The 2018 Pennock knee MRI tool was used as a reference to define the physis as open, partially open, or closed. 31 Partially open was specifically defined as central physis closure of the distal femur (median age of 16.9 years in males) and proximal tibia (median age of 16.05 years in males). 31 Eight patients were identified as having closed physes at the time of surgery and were excluded. Of note, patients undergoing concomitant patellar stabilization procedures, additional ligamentous reconstruction, or meniscal repair at the time of primary MPFL-R were included in the analysis. Patients and their families were contacted by telephone to assess clinical outcomes. Patients with <2 years of clinical follow-up were also excluded from the final analysis. Minimum 3-year, 5-year, and 10-year follow-up were considered short-, mid-, and long-term follow-up, respectively.
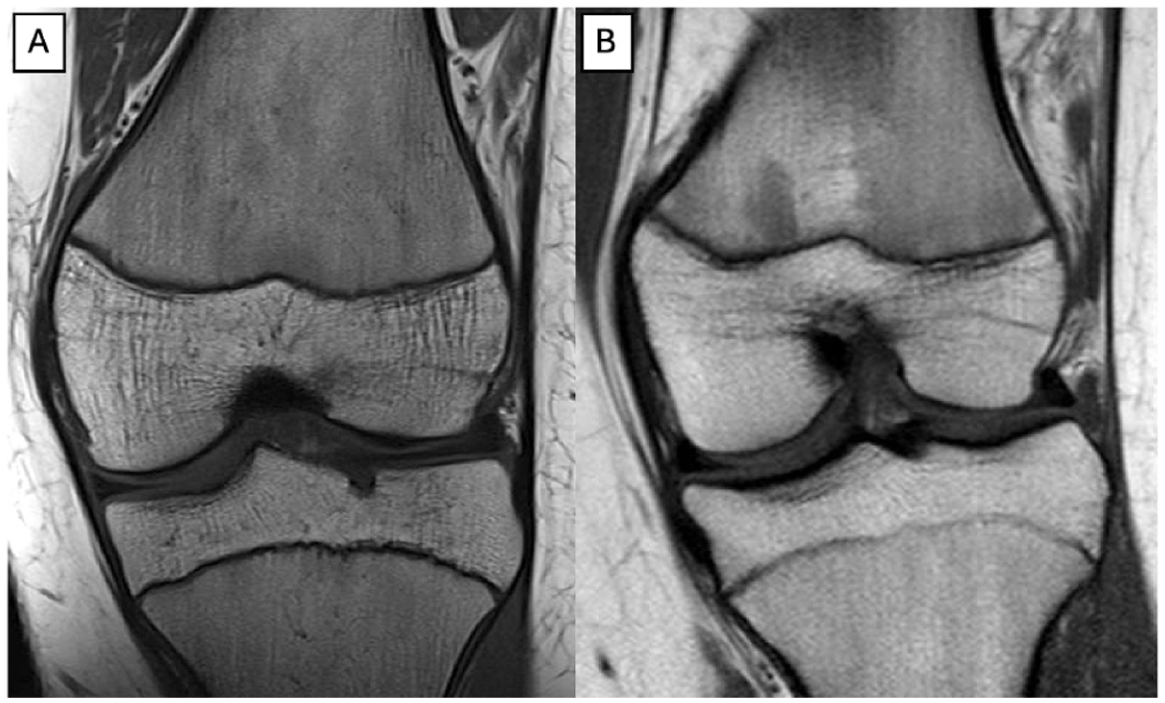
Coronal T1-weighted magnetic resonance imaging slices depicting a (A) completely open distal femoral physis and a (B) partially open distal femoral physis with central physis closing.
Indications and Technique for MPFL-R
Patients were indicated for MPFL-R in the setting of recurrent patellar dislocations that failed a trial of nonoperative management consisting of activity modification, physical therapy, and bracing, or a first-time patellar instability event resulting in an osteochondral lesion that was determined would benefit from surgery. All surgeries were performed by 1 of 6 fellowship-trained, high-volume orthopaedic surgeons (D.R.D.) on an outpatient basis. All patients underwent an examination under anesthesia and knee arthroscopy to assess and treat concomitant intra-articular pathology. Graft type was determined by surgeon preference, although hamstring tendon allograft was utilized in patients with documented conditions predisposing them to patholaxity. Concomitant procedures, such as meniscal repair, osteochondral fracture fixation, and TTO, were performed as indicated by individual patient pathology and presentation. Although TTOs in patients with open proximal tibial physes are contraindicated, the literature, as well as the senior author (D.R.D.), may consider a TTO as a viable option in a patient with central closure of the proximal tibial physis. 30 Nearly all patients in the current study had a closed or partially closed proximal tibial physis during the time of their MPFL-R.
Two techniques for patella-sided graft fixation were performed after the medial patella was exposed in standard fashion: (1) 2 oblique, 3.2-mm patellar tunnels with a looped graft, or (2) 2 suture anchors (Gryphon Suture Anchor [Johnson & Johnson] or 3.0-mm SutureTak [Arthrex]).8,26 The technique for patella-sided graft fixation was determined by surgeon preference in consideration of the patient-specific anatomy.
Patellar Tunnel Technique
At the upper one-third of the patella, a 3.2-mm drill bit was utilized to create a tunnel beginning just anterior to the articular surface and emerging one-third of the way across the width of the patella. Approximately 1 cm distally to the initial tunnel, the 3.2-mm drill bit was utilized to create a second tunnel in a similar fashion. The hamstring graft was then shuttled in a looped configuration through the tunnels, a technique previously described by Moran et al. 26 Specifically for skeletally immature patients, on the femoral side a transphyseal technique was utilized when the femoral physis demonstrated visible signs of beginning central closure. In cases in which the physis remained clearly open on both anteroposterior and lateral radiographic views, a physis-sparing approach was performed, positioning the graft distal to the growth plate.
Suture Anchor Technique
Two suture anchors (Gryphon Suture Anchor or 3.0-mm SutureTak) were placed along the medial patellar border at the upper one-third to one-half of the patella with approximately 1 cm of intervening space that was prepared using a curette to encourage soft tissue healing to bone by creating a shallow trough. The hamstring graft was then secured in each anchor. This technique is further described by Deasey et al. 8
After patella-sided graft fixation, the graft ends were shuttled between layers 2 and 3 of the medial knee, and the Schottle point was then identified with a Beath pin on a perfect lateral radiograph. In patients with fully open physes, a physis-sparing technique for creating the femoral tunnel was utilized. An anteroposterior fluoroscopic view was additionally used to confirm the trajectory of the Beath pin distal to the physis. The use of orthogonal imaging ensured that the pin did not violate the trochlea and intercondylar notch. After pin placement and confirmation of graft isometry, the Beath pin was overreamed with a 7-mm reamer. The graft ends were then pulled into the blind-ended socket. An interference screw (7-mm Milagro Advance interference screw [Johnson & Johnson] or 7-mm BioComposite interference screw [Arthrex]) was placed for femur-sided graft fixation with approximately 0.5 pounds (2 N) of force placed through the graft with the knee at approximately 40° of flexion.
Rehabilitation
In the setting of isolated MPFL-R, patients were restricted to 50% weightbearing on the operative extremity for 2 weeks before weightbearing as tolerated was allowed. A hinged knee brace was utilized to restrict motion to 0° to 90° for the first 4 weeks, after which point range of motion was unrestricted. Patients were counseled on avoiding high-level activity for up to 5 months postoperatively, after which time return to sport was allowed provided the patient successfully completed a return-to-sport progression and assessment by the surgeon.
Evaluation Methods
A retrospective chart review was performed for all included patients to determine demographics, including age, sex, body mass index (BMI) at time of surgical intervention, surgical indications, and previous operations. Operative notes were reviewed to record graft type, methods of graft fixation, and any concomitant procedures that were performed at the time of MPFL-R.
MRI was used to evaluate radiographic parameters. Axial sections were used to measure patellar tilt, congruence angle, and sulcus angle, as well as the tibial tuberosity–to–trochlear groove (TT-TG) distance and PT-LTR distance. Sagittal sections were used to assess patellar height by calculation of the Caton-Deschamps Index (CDI). 6 Trochlear dysplasia was characterized utilizing the Dejour and Le Coultre classification. 9 Preoperative radiographic measurements were performed independently by 2 researchers (B.J.M., T.E.M.) and interrater reliability was assessed.
Patients were contacted by telephone and were queried utilizing standardized questionnaires regarding the occurrence of postoperative patellar subluxation and dislocation events, and regarding any reoperation on the surgical knee for patellar instability events, growth disturbances, or other conditions. Patients were also assessed for return to sport postoperatively, and whether they returned to performance at a lower, equivalent, or higher level after surgery. Objective patient-reported outcome measures (PROMs) were assessed using validated scoring systems (Kujala, Lysholm, and International Knee Documentation Committee [IKDC] knee scores).17,21,44
Statistical Analysis
The mean, standard deviation, standard error (SE), and frequency were calculated for all patient characteristics (age, sex, laterality, BMI, and concomitant procedures). For preoperative radiographic measurements, the mean, standard deviation, and standard error were calculated and a Student t test was used for statistical evaluation. Chi-square and Fisher exact tests were used to evaluate nominal data between the cohort with postoperative subluxations and the cohort without postoperative subluxations. All PROMs were assessed using mean, median, standard deviation, and standard error. A Student t test was used to evaluate differences of PROMs at different time points. Frequencies were calculated for return to sport, subluxations and dislocations, subsequent surgeries, and revision surgeries. Univariate analysis of failure for discrete data such as occurrence of concomitant TTO (without anteromedialization), anteromedializing TTO, osteochondral fracture fixation, type of allograft used, use of semitendinosus graft, ipsilateral surgery, and BMI >25 kg/m2 was done using the odds ratios of patient-specific variables. 43 A Cox regression analysis was used to calculate the hazard ratios (HRs) of continuous patient variables such as age, BMI, TT-TG distance, PT-LTR distance, CDI, patellar tilt, sulcus angle, and congruence angle. A linear regression was performed using the preoperative measurements for each patient paired with their corresponding PROMs: Kujala, Lysholm, and IKDC scores. 40 Interrater reliability was evaluated using the standard error of measurement, as it has been suggested to be the preferred method of evaluation. 33 All statistical tests were 2-sided when applicable, and a P value <.05 was considered significant. Separate subgroup analysis was performed for patients undergoing isolated MPFL-R.
Results
A total of 83 patients met inclusion criteria. In the final analysis, 54 knees in 51 skeletally immature patients (male: n = 16 [31.4%]; female: n = 35 [68.6%]) with mean age of 15.6 years (range, 10-18 years) were included based on reaching a minimum 2-year clinical follow-up (51/83; 61.4%) (Figure 2). There were no statistically significant differences between the baseline characteristics of patients excluded for lack of 2-year clinical follow-up and patients included for final analysis (age [P = .288], sex [P = .071], laterality [P = .404], and BMI [P = .566]). Characteristics of the included patient population are further described in Table 1.
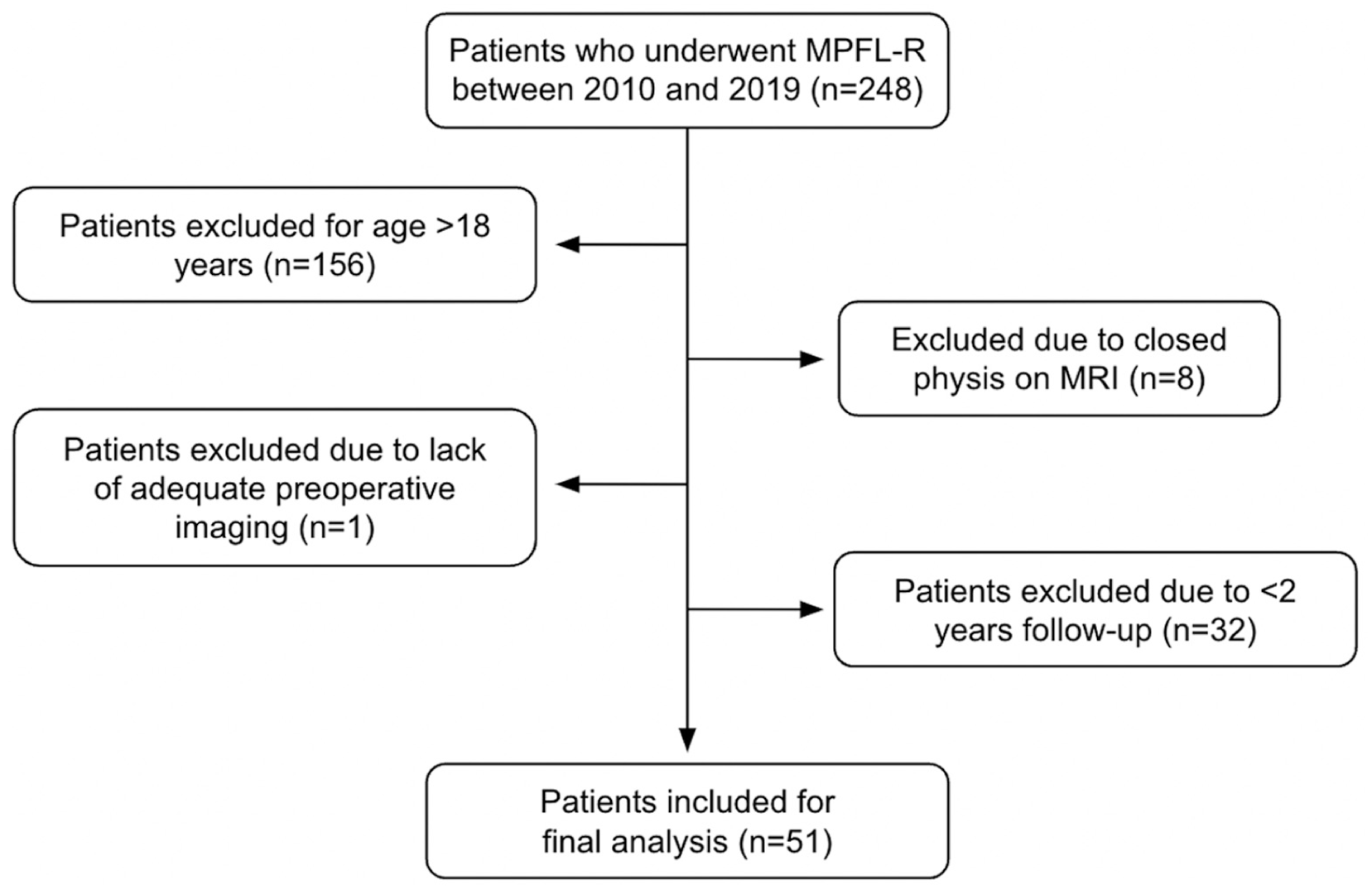
Flowchart demonstrating the study population available for analysis after application of the inclusion and exclusion criteria. MPFL-R, medial patellofemoral ligament reconstruction; MRI, magnetic resonance imaging.
Information for Study Population Included in Final Analysis a
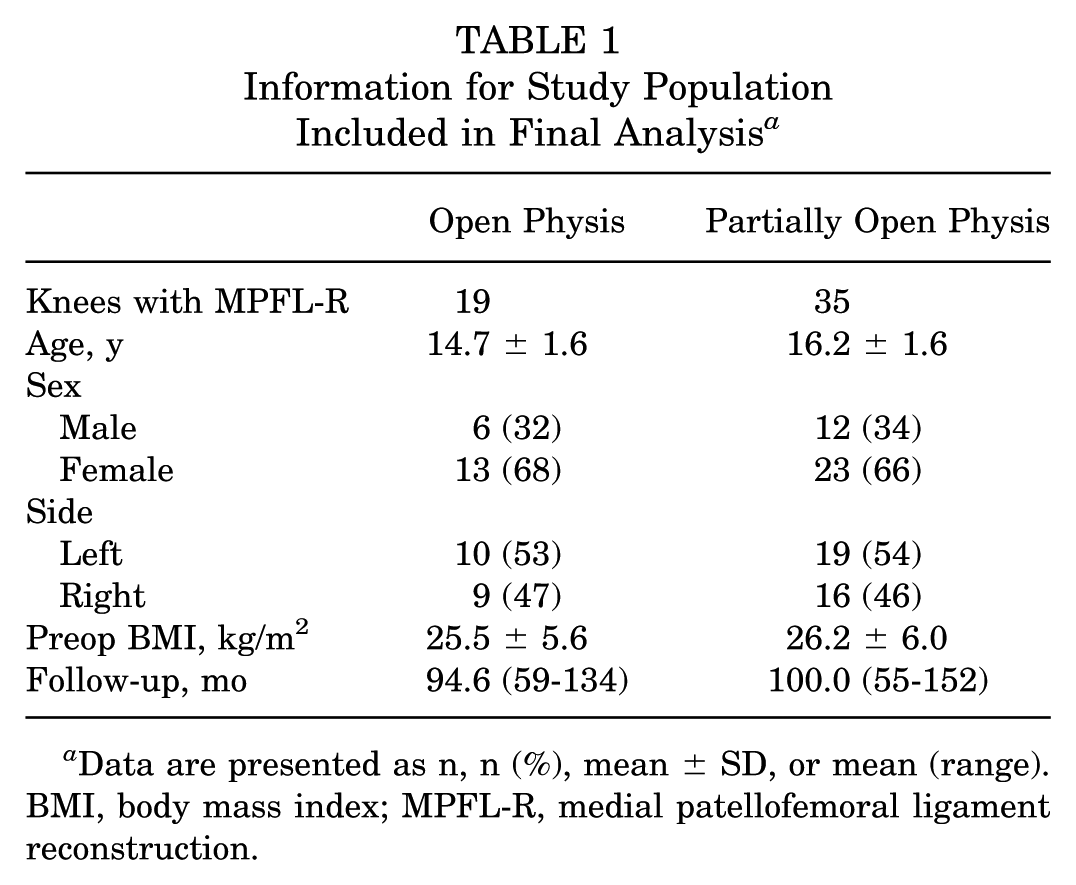
Data are presented as n, n (%), mean ± SD, or mean (range). BMI, body mass index; MPFL-R, medial patellofemoral ligament reconstruction.
All included knees had open (n = 19) or partially open (n = 35) physes at the time of index surgery. Bilateral knees were evaluated and analyzed separately. The mean follow-up time was 8.15 years (range 55-152 months).
Looking at the combined cohort, including both patients with open and those with partially open distal femoral physes, 31 (57.4%) knees underwent an anteromedializing TTO at the time of index MPFL-R, with 5 (9.3%) of these knees undergoing concomitant distalization of the tibial tubercle. No knees underwent additional ligamentous reconstruction, hemi-epiphysiodesis, or other osteotomy. Patella-sided graft fixation was performed with patellar tunnels with a looped graft in 50 (92.6%) knees, and hamstring tendon autograft was used in 52 (96.3%) knees. The gracilis tendon was used for the graft in 46 (85.2%) knees (Table 2).
Concomitant Procedures Performed at Time of Index MPFL-R a
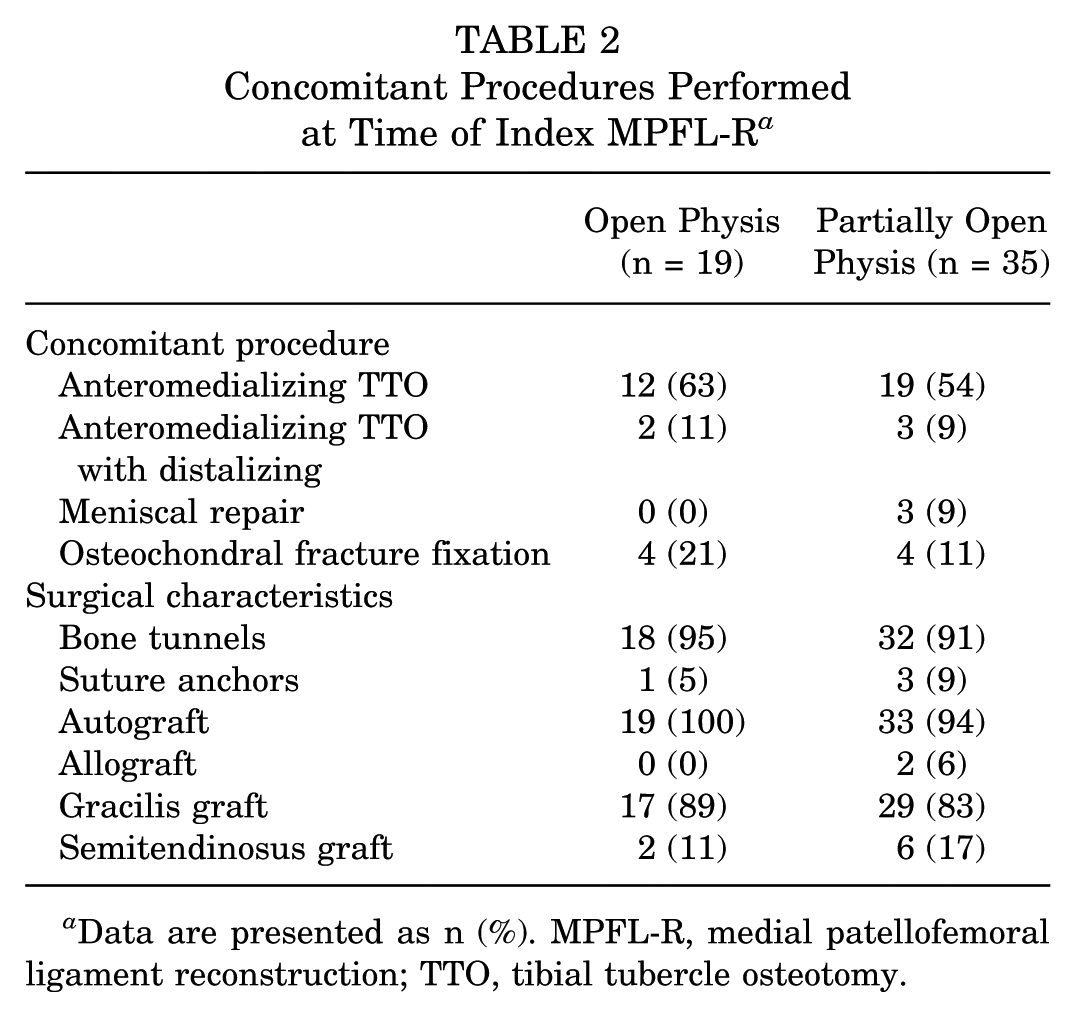
Data are presented as n (%). MPFL-R, medial patellofemoral ligament reconstruction; TTO, tibial tubercle osteotomy.
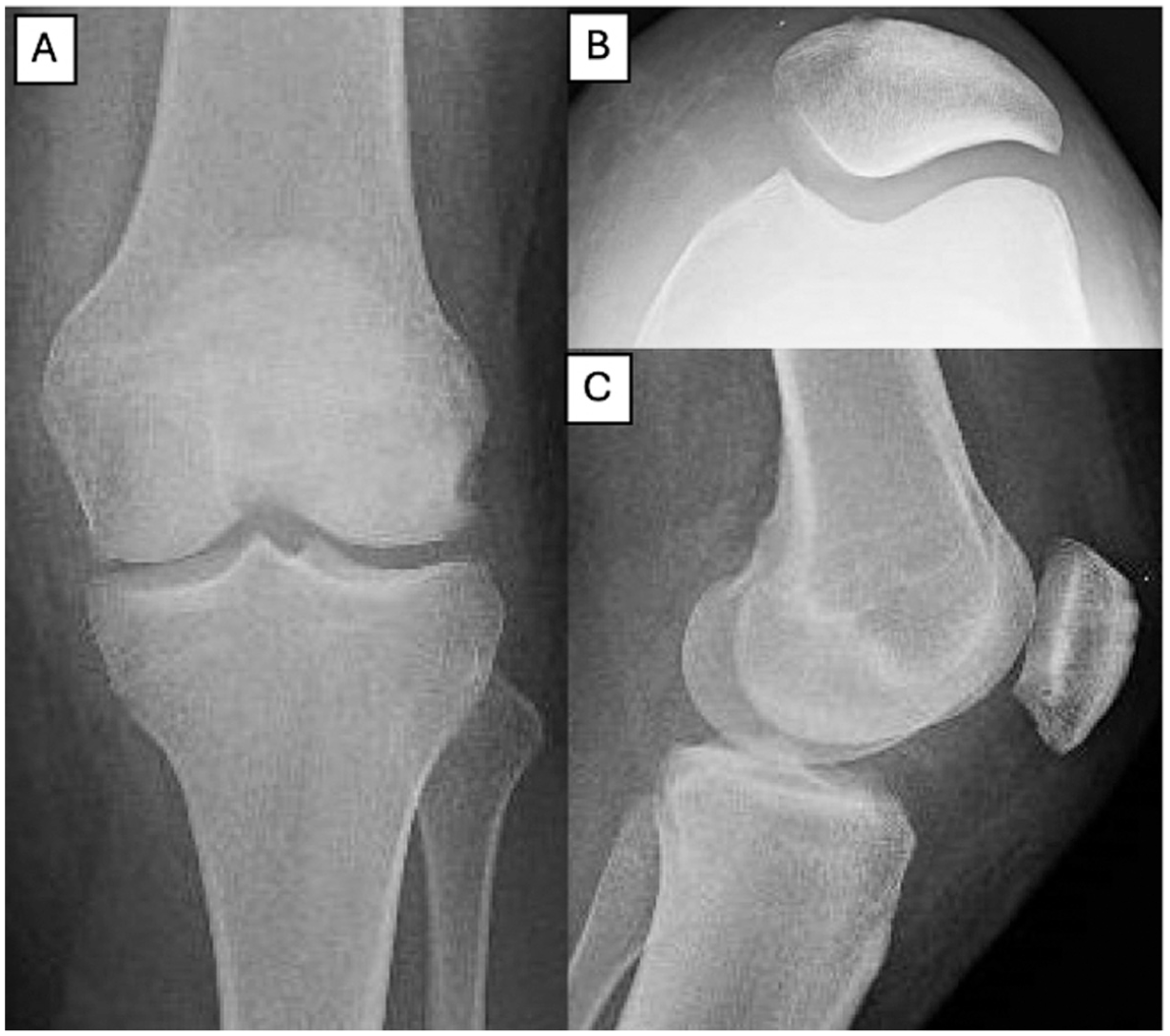
Preoperative radiographs and MRI scans were available for all patients (Figure 3). The mean CDI was 1.25 (range, 0.93-1.73). A total of 37 (68.5%) knees demonstrated CDI >1.2. The mean TT-TG distance was 15.8 mm (range, 6.95-25.5 mm), with 12 (22.2%) knees having a TT-TG distance >20 mm (Table 3). Interobserver reliability values for radiographic measures were as follows: 0.08 for CDI, 0.51 mm for TT-TG distance, 0.99 mm for PT-LTR distance, 1.21° for patellar tilt, 2.24° for sulcus angle, and 8.22° for congruence angle.
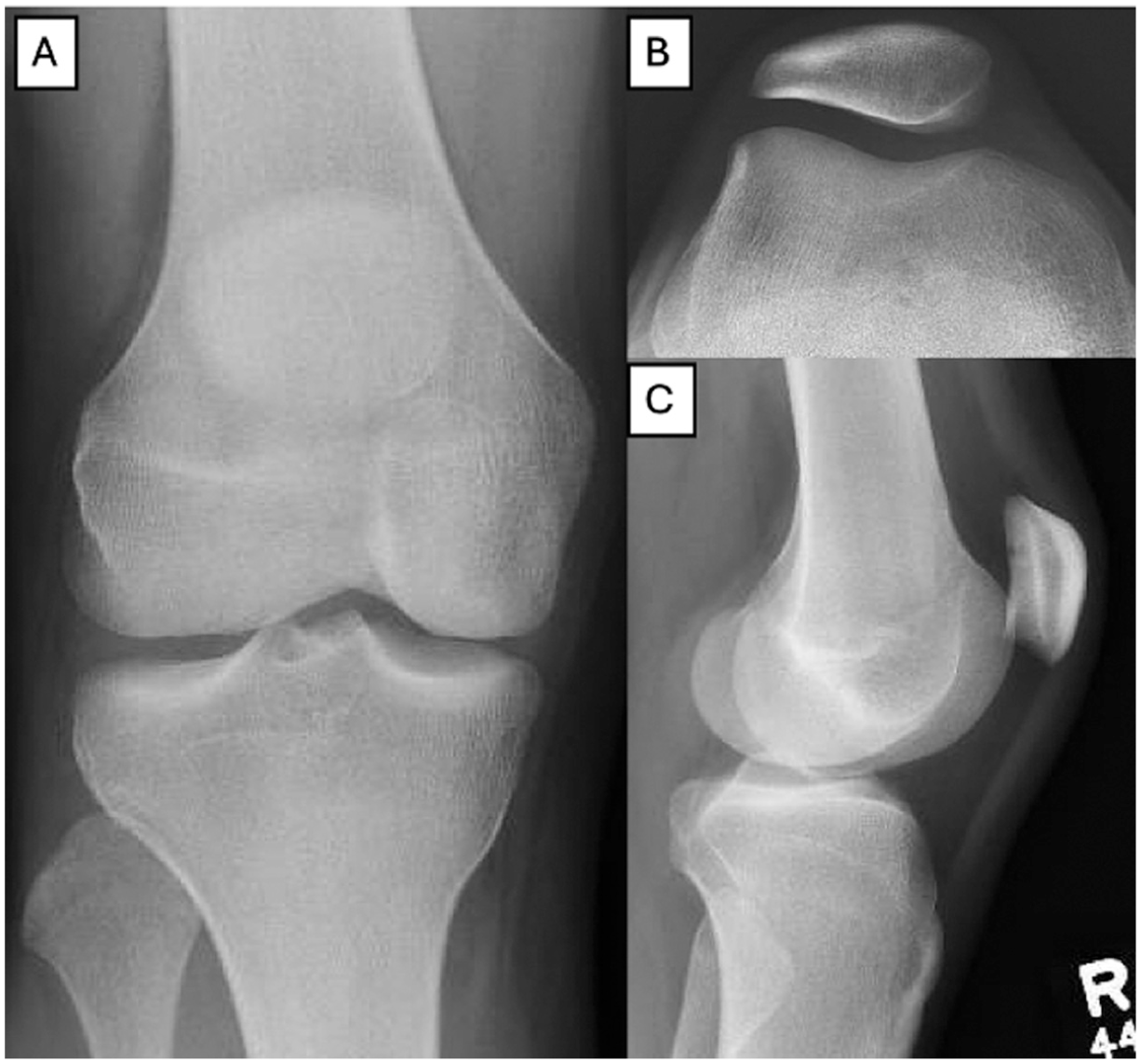
Preoperative (A) anteroposterior, (B) sunrise, and (C) lateral radiographic views of a right knee.
Preoperative Measurements Obtained Using MRI for All Included Knees and Frequency of Trochlear Dysplasia by Dejour Classification a
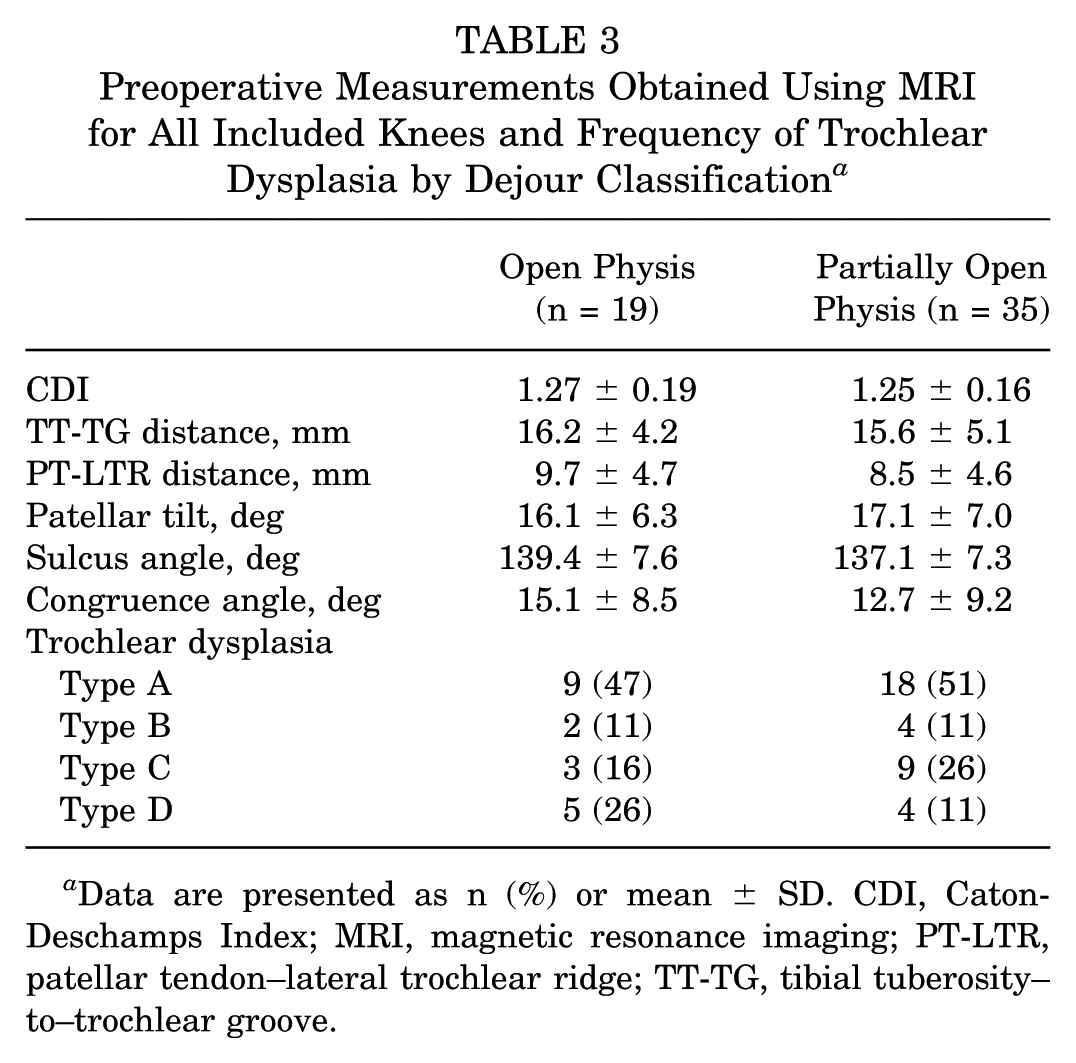
Data are presented as n (%) or mean ± SD. CDI, Caton-Deschamps Index; MRI, magnetic resonance imaging; PT-LTR, patellar tendon–lateral trochlear ridge; TT-TG, tibial tuberosity–to–trochlear groove.
Clinical Outcomes
Recurrent Patellar Instability
Four of 54 (7.4%) knees experienced subsequent patellar instability events. All events were characterized as subluxation episodes. There were no clinically confirmed recurrent patellar dislocations postoperatively. No patients underwent revision MPFL-R or subsequent procedures for patellar stabilization (Table 4).
Summary of Postoperative Outcomes After Index MPFL-R, Comparing Knees With Concomitant TTO Versus Those Without a
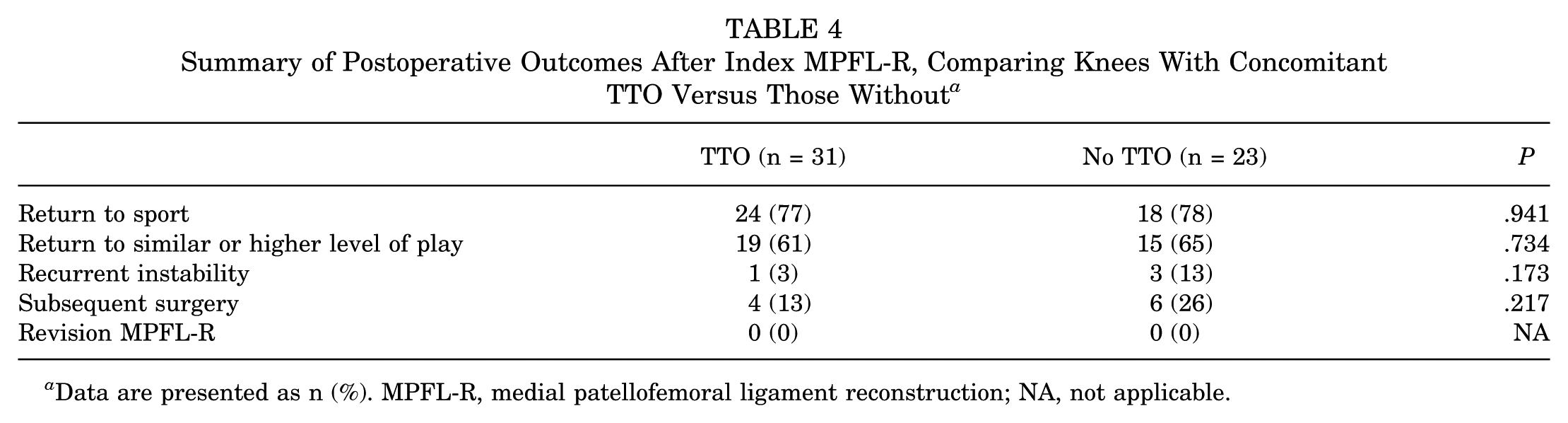
Data are presented as n (%). MPFL-R, medial patellofemoral ligament reconstruction; NA, not applicable.
Using Cox regression analysis for hazard ratios of continuous patient-specific variables, we found that younger age at the time of surgery was associated with a significant increase in the risk of recurrent patellar instability (HR, –0.83; 95% CI, –1.53 to −0.14; P = .018). Patients experiencing recurrent patellar instability events also had, on average, a significantly greater PT-LTR distance than those without recurrent instability (13.46 vs 8.59 mm; P = .043). No other patient factors, surgical characteristics, or radiographic measurements demonstrated a statistically significant relationship with recurrent patellar instability (Tables 5-7).
Hazard Ratios for Recurrent Patellar Instability Based on Patient-Specific Variables a
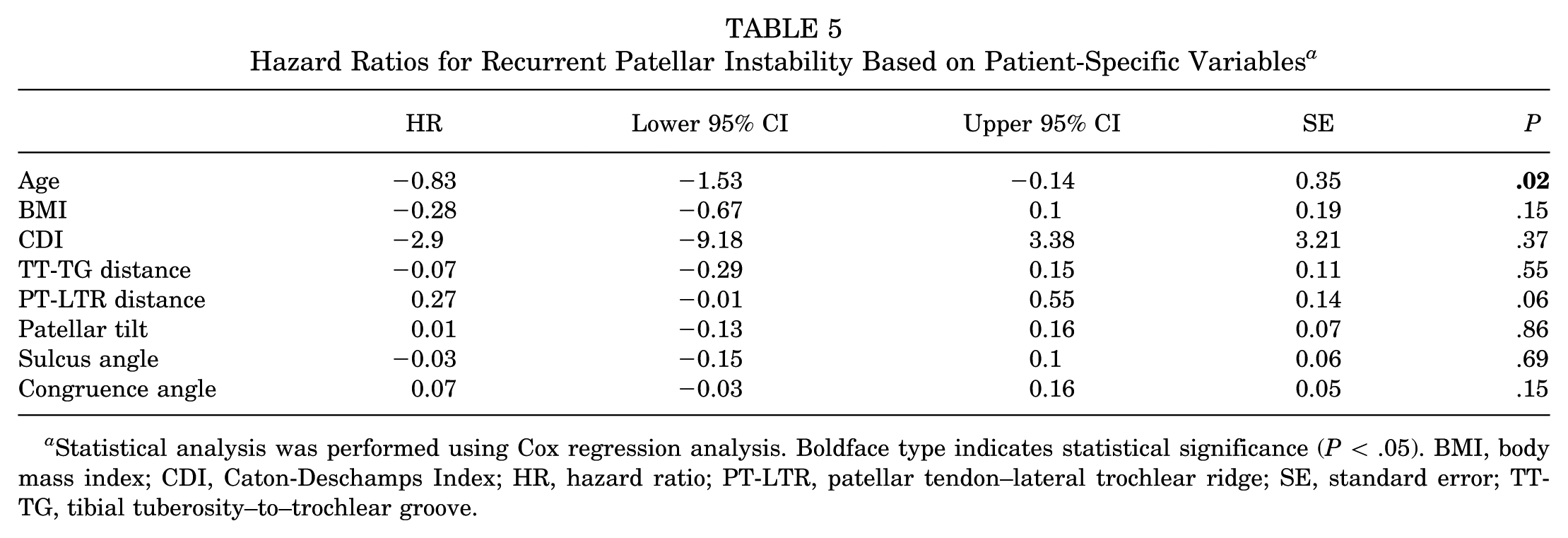
Statistical analysis was performed using Cox regression analysis. Boldface type indicates statistical significance (P < .05). BMI, body mass index; CDI, Caton-Deschamps Index; HR, hazard ratio; PT-LTR, patellar tendon–lateral trochlear ridge; SE, standard error; TT-TG, tibial tuberosity–to–trochlear groove.
Odds Ratios for Recurrent Instability Based on Patient-Specific Variables a
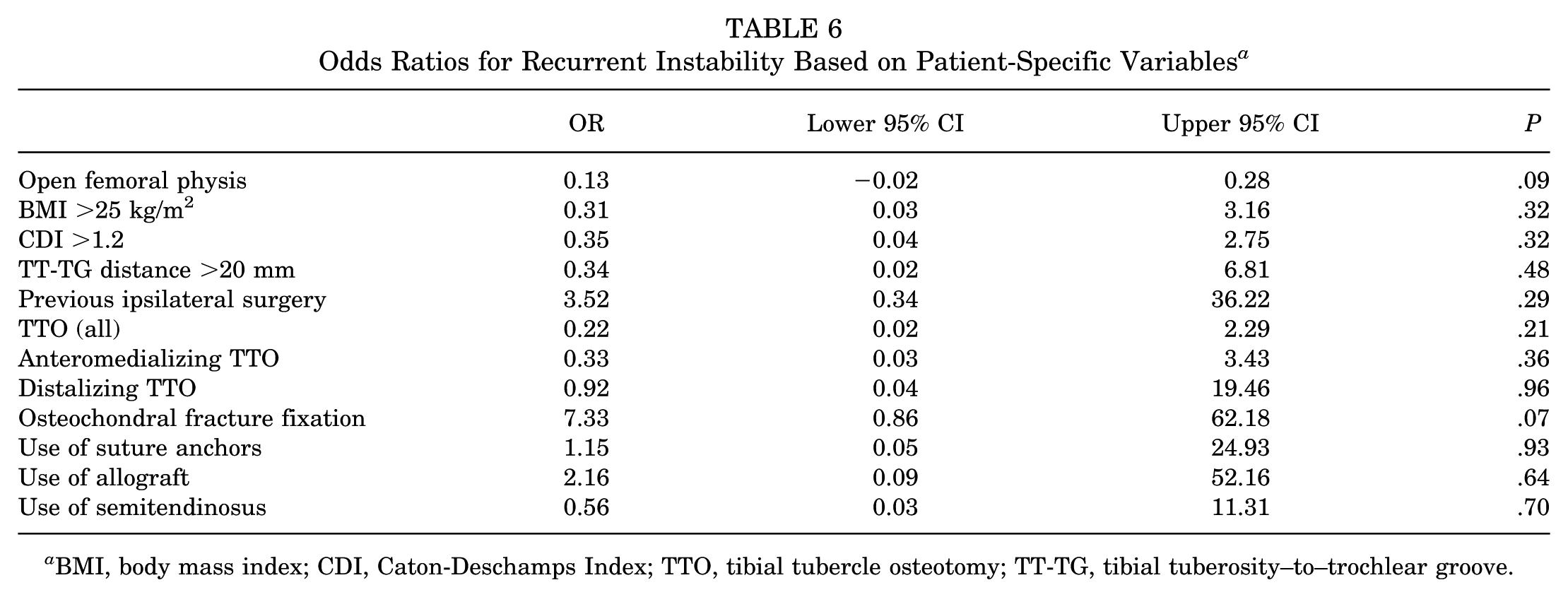
BMI, body mass index; CDI, Caton-Deschamps Index; TTO, tibial tubercle osteotomy; TT-TG, tibial tuberosity–to–trochlear groove.
Comparison of All Knees With and Without Recurrent Instability After MPFL-R a
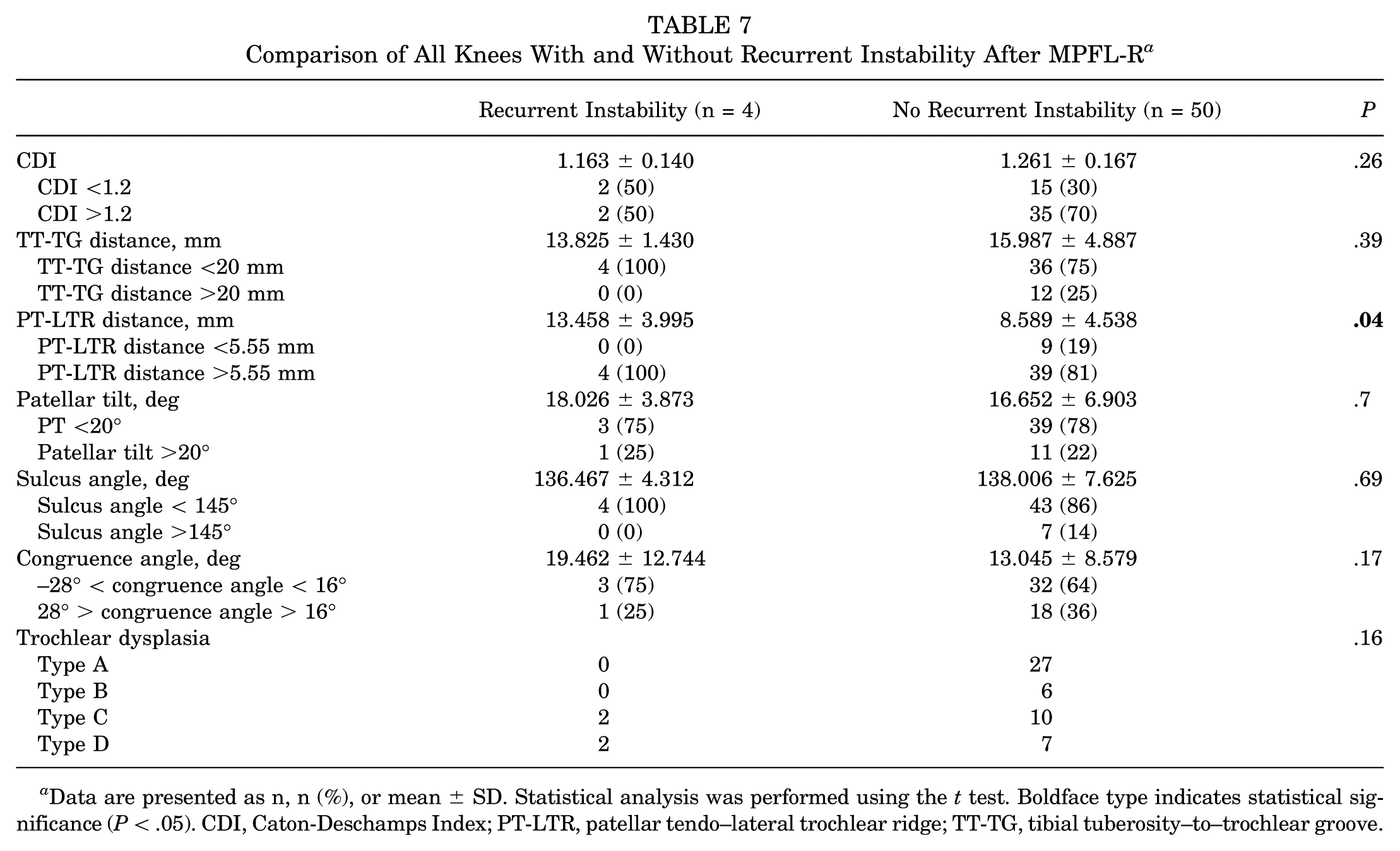
Data are presented as n, n (%), or mean ± SD. Statistical analysis was performed using the t test. Boldface type indicates statistical significance (P < .05). CDI, Caton-Deschamps Index; PT-LTR, patellar tendo–lateral trochlear ridge; TT-TG, tibial tuberosity–to–trochlear groove.
In subgroup analysis, 3 of 23 (13.0%) knees undergoing isolated MPFL-R experienced subsequent patellar subluxation events. High-grade trochlear dysplasia (P = .002) and PT-LTR distance >5.55 mm (P = .004) correlated with an increased risk of recurrent instability events. No other patient factors, surgical characteristics, or radiographic measurements demonstrated a statistically significant relationship with recurrent patellar instability (Tables 8 and 9).
Subgroup Analysis of Knees That Underwent Isolated MPFL-R a
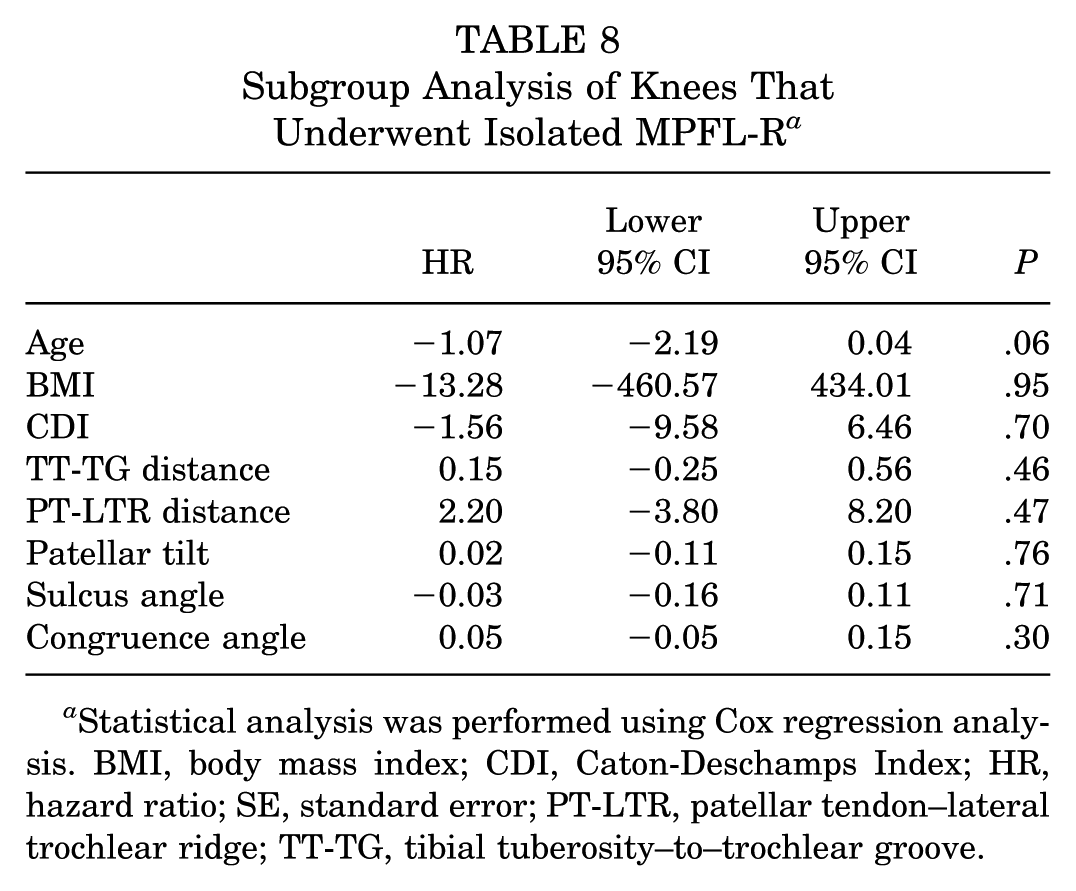
Statistical analysis was performed using Cox regression analysis. BMI, body mass index; CDI, Caton-Deschamps Index; HR, hazard ratio; SE, standard error; PT-LTR, patellar tendon–lateral trochlear ridge; TT-TG, tibial tuberosity–to–trochlear groove.
Subgroup Analysis of Knees That Underwent Isolated MPFL-R and Experienced Recurrent Instability Versus Those That Did Not a
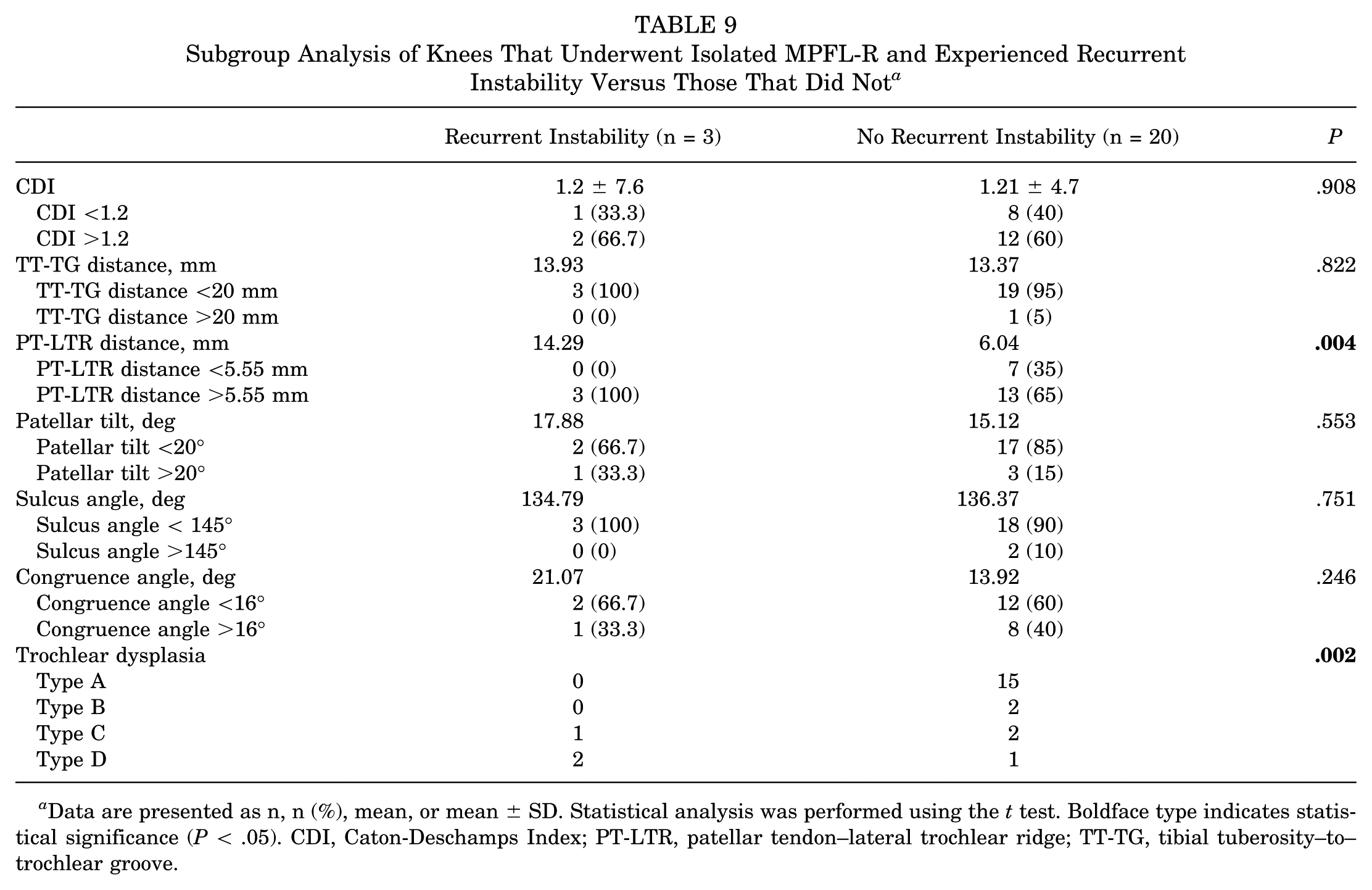
Data are presented as n, n (%), mean, or mean ± SD. Statistical analysis was performed using the t test. Boldface type indicates statistical significance (P < .05). CDI, Caton-Deschamps Index; PT-LTR, patellar tendon–lateral trochlear ridge; TT-TG, tibial tuberosity–to–trochlear groove.
Malalignment and Growth Arrest
There were no cases of clinical malalignment or physeal damage that required treatment or surgical intervention. In the patients with available postoperative imaging, there was no observable evidence of focal growth delay (Figure 4).
Postoperative (A) anteroposterior, (B) sunrise, and (C) lateral radiographic views of a left knee.
Patient-Reported Outcome Measures
All included knees reached a minimum 3-year follow-up (n = 54; 100%). At a minimum 3-year follow-up, the mean Kujala, Lysholm, and IKDC scores were 85.7 (range, 11-100), 83.6 (range, 14-100), and 76.1 (range, 10-95.4), respectively. Of the 54 knees, 51 (94.4%) reached a minimum 5-year clinical follow-up. The mean Kujala, Lysholm, and IKDC scores were 85.1 (range, 11-100), 83.2 (range, 14-100), and 75.5 (range, 10-94.3), respectively. Of the 54 knees, 31 (57.4%) reached a minimum 8-year clinical follow-up. The mean Kujala, Lysholm, and IKDC scores were 82.5 (range, 11-100), 82.5 (range, 14-100), and 75.0 (range, 10-94.3), respectively. Ten of the 54 (18.5%) knees reached a minimum 10-year clinical follow-up. The mean Kujala, Lysholm, and IKDC scores were 77.0 (range, 11-99), 84.5 (range, 14-100), and 71.3 (range, 10-87), respectively (Table 10). There were no statistically significant differences in PROMs between patients at minimums of 3, 5, 8, and 10 years of follow-up.
Patient-Reported Outcome Measures at Short-, Mid-, and Long-term Follow-up a
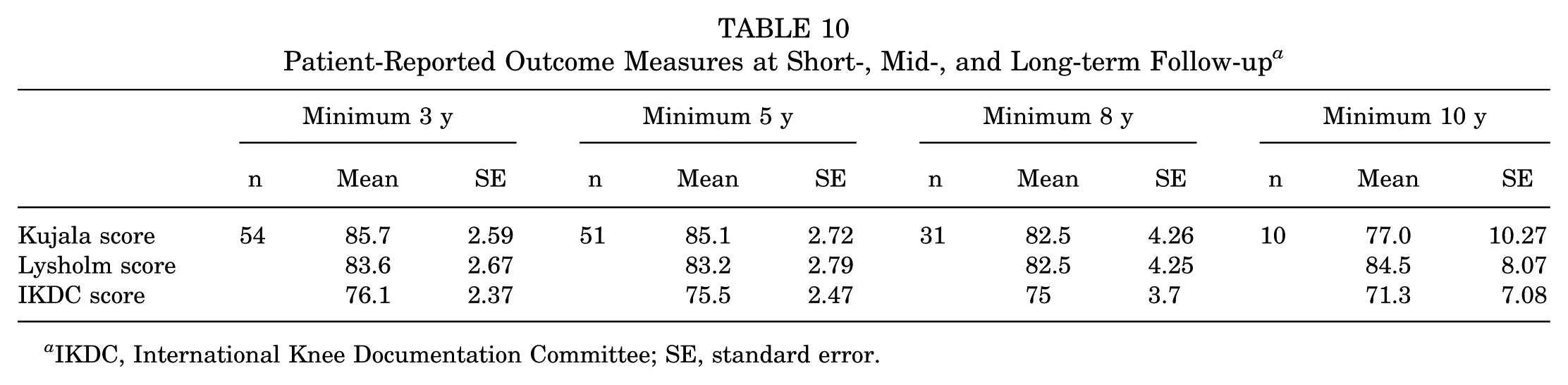
IKDC, International Knee Documentation Committee; SE, standard error.
Younger age correlated with a risk of lower IKDC score (P = .04); however, no other patient demographic factors, surgical characteristics, or radiographic measurements demonstrated a statistically significant relationship with any of the PROMs on linear regression analysis (Table 11).
Linear Regression of All Knees Between Patient-Reported Outcome Measures and Patient-Specific Variables a
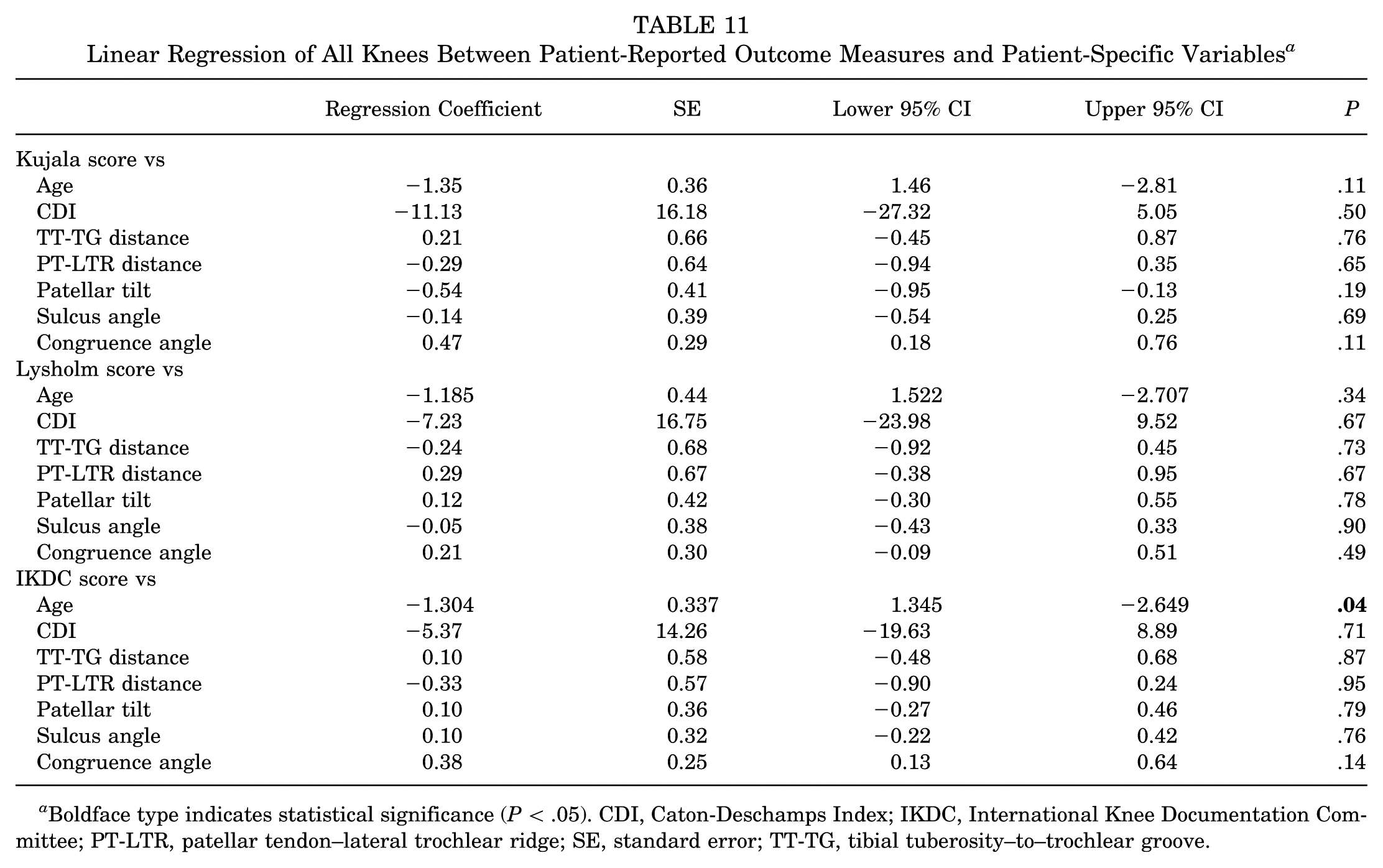
Boldface type indicates statistical significance (P < .05). CDI, Caton-Deschamps Index; IKDC, International Knee Documentation Committee; PT-LTR, patellar tendon–lateral trochlear ridge; SE, standard error; TT-TG, tibial tuberosity–to–trochlear groove.
Return to Sport
For patients who played sports preoperatively, 40 of 49 (81.6%) returned to sport, with 30 of 40 (75.0%) of those returning to a similar or higher level of competition (Table 12).
Summary of Postoperative Outcomes After Index MPFL-R, Comparing Knees With Open Versus Partially Open Physes a
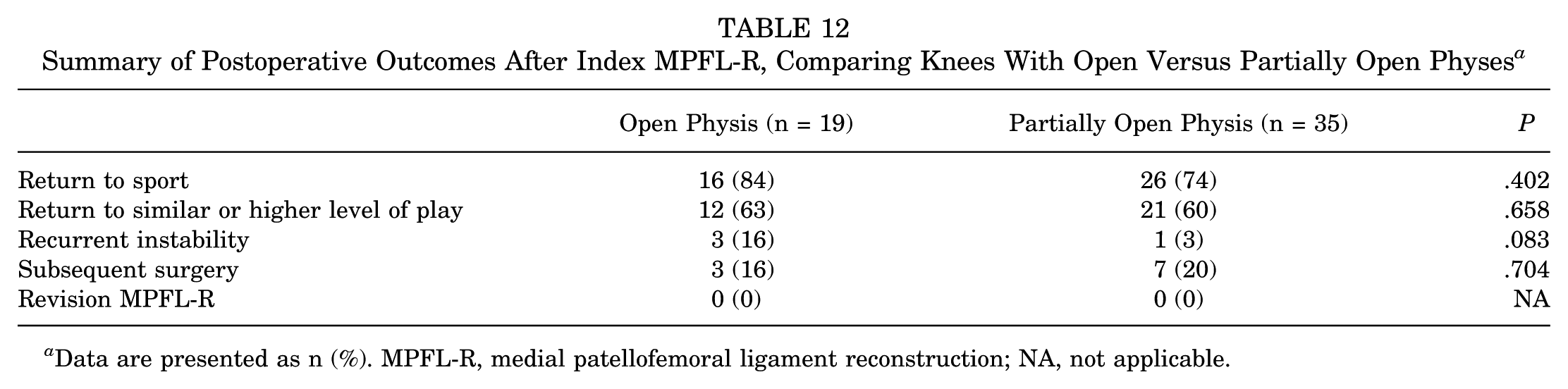
Data are presented as n (%). MPFL-R, medial patellofemoral ligament reconstruction; NA, not applicable.
Additional Operation
Ten of 54 (18.5%) knees underwent subsequent surgery (Table 12). The most common reason for subsequent operation was for hardware removal (n = 4). Other indications for subsequent operation were anterior cruciate ligament reconstruction (n = 3), arthroscopic shaving chondroplasty (n = 1), manipulation under anesthesia and arthroscopic lysis of adhesions (n = 1), and later osteochondral allograft transplantation for a femoral condyle lesion (n = 1).
Discussion
We hypothesized that anatomic MPFL-R in patients with open or partially open distal femoral physes would lead to low rates of both recurrent patellar instability and instances of clinically relevant growth disturbance. The most significant finding of this retrospective series is that anatomic MPFL-R in skeletally immature patients appears to be a safe, effective, and durable treatment for addressing patellar instability. In this series, there were no occurrences of subsequent intervention for recurrent patellar instability or growth disturbance after surgery.
MPFL-R in skeletally immature patients presents unique challenges given the risk of injury to the distal femoral physis.15,35,47 Technical modifications to attempt to avoid injury to the physis and subsequent growth disturbance may compromise graft isometry and lead to poorer functional outcomes and graft failure.4,5,10,38,39 The activity level of this adolescent patient group and these surgical factors may contribute to the greater risk of recurrent patellar instability seen in skeletally immature patients in comparison with an adult patient population.1,24,34,42 Anatomic MPFL-R has emerged as the treatment of choice for skeletally immature patients, although there is a relative paucity of existing studies evaluating the clinical outcome of this procedure in this patient population.15,28,35,36,45 Nelitz et al 28 reported outcomes of 21 patients with a mean age of 12.2 years at a mean of 2.8 years postoperatively. Two (9.5%) patients had ongoing patellar apprehension, and the mean Kujala and Tegner activity scores changed from 72.9 to 92.8 and 6.0 to 5.8 pre- to postoperatively, respectively. 28 Seventeen of 21 (81.0%) patients returned to sport at the same or higher level. 28 Uppstrom et al 45 described outcomes for 54 knees in 49 patients (mean age, 13.3 years) at median follow-up of 2.2 years postoperatively. The authors reported recurrent patellar instability in 5 (9.3%) knees, with 3 (5.6%) knees undergoing subsequent surgery for patellar stabilization. 45 Rueth et al 36 reported recurrent patellar instability events in 1 of 101 (0.9%) patients with a mean age of 14.8 years at mean 32 months postoperatively. Overall, 86% of patients in this series were able to return to sport, and the mean Kujala score improved from 47.1 to 85.3 postoperatively. 36 More recently, Husen et al 15 described outcomes in 79 knees in 69 patients with a mean age of 14.7 years. At a mean follow-up time of 37.9 months, 11 patients experienced recurrent patellar instability requiring reoperation. 15 The mean Lysholm, Kujala, and Tegner scores were 96.5, 96.5, and 4.9 at the final follow-up, respectively. 15 Postoperatively, 90.5% of patients were able to return to sport at the same or higher level. 15 Collectively, the findings of this current study in the context of the existing literature suggest that anatomic MPFL-R is efficacious in treating patellar instability in skeletally immature patients, contributes to good to excellent clinical satisfaction based on validated PROMs, and allows successful return to sport. Additionally, the longer follow-up time of the present study adds to the existing literature by suggesting a durable treatment effect, which is particularly relevant considering the young age and relatively high activity level of the patient population in question.
While anatomic MPFL-R is possible given the femoral insertion of the MPFL being just distal to the distal femoral physis, its close proximity maintains the potential for injury.15,18,27,35 The existing literature reports a low rate of clinical growth disturbance after anatomic MPFL-R. Uppstrom et al 45 found no evidence of clinical or radiographic growth disturbance on full-length lower extremity radiographs or MRI scans after MPFL-R. Husen et al 15 and Rueth et al 36 also found no clinically significant evidence of growth disturbance in their series of patients after MPFL-R. While the current study and the studies by Husen et al 15 and Rueth et al 36 did not objectively quantify modulation of growth radiographically as Uppstrom et al 45 did postoperatively, the risk for clinically relevant growth disturbance collectively appears to be low with the appropriate surgical technique.
The current study also sought to evaluate the association of various patient factors, preoperative radiographic parameters, and surgical characteristics for patellar maltracking with clinical outcomes after anatomic MPFL-R. On regression analysis, greater preoperative PT-LTR distance and younger age at the time of surgery demonstrated an increased risk of recurrent patellar instability postoperatively. PT-LTR, a measurement of the axial width of the patellar tendon seen beyond the lateral trochlear ridge on an axial MRI section, has been shown to be sensitive and specific for patellofemoral instability through its evaluation of containment of the extensor mechanism within the trochlear groove. 25 Skeletal immaturity, and by extension young age, has been described by Lewallen et al 23 as a significant risk factor for recurrent patellar instability, increasing the likelihood of failure of nonoperative management. Notably, in the current study, no other patient factor, preoperative radiographic parameters, or surgical characteristic corresponded with an increased risk of recurrent patellar instability.
It remains debated in the literature when patients definitively benefit from other concomitant procedures to individualize surgical management based on other anatomic risk factors versus MPFL-R alone. In a subgroup analysis of patients undergoing isolated MPFL-R, the current study observed an increased risk of recurrent patellar instability in patients with high-grade trochlear dysplasia and increased PT-LTR distance. Trochlear dysplasia has been cited as the main anatomic risk factor for recurrent patellar instability in patients undergoing nonoperative management.2,7,37 Additionally, Kita et al 20 found that severe trochlear dysplasia was the most important predictor of recurrent instability among 42 patients who underwent isolated MPFL-R. The authors observed that among patients with type D trochlear dysplasia, elevated TT-TG distance further negatively impacted outcomes. 20 The authors did not evaluate the influence of PT-LTR on outcomes. 20 Collectively, the findings of this study and the current study are suggestive that treatment based on the interplay of the multifactorial risk factors contributing to patellar instability is more appropriate than decision-making based on any single measurement alone. Further study is ongoing regarding this topic and will be important to better understand the indication for including other concomitant patellar stabilization procedures to address these predisposing anatomic risk factors in addition to MPFL-R.12,13
Limitations
The following limitations should be taken into account in the interpretation of this study's results. There are inherent limitations to a retrospective series, although other reports in the literature examining clinical outcomes after MPFL-R in skeletally immature patients are similarly limited. Additionally, the lack of randomization and control limits true subgroup comparison of patients undergoing isolated MPFL-R and individualized surgical management. Given the lack of complete follow-up for patients available for inclusion in this study, the lack of capture of outcomes of interest cannot be ruled out in patients who were excluded for failing to reach a minimum follow-up time of 2 years postoperatively. Additionally, while good to excellent mean PROMs were seen at the final follow-up, the lack of preoperative PROMs for comparison limits the objective quantification of improvement in function from pre- to postoperatively. Subclinical growth disturbance postoperatively also cannot be ruled out given that full-length alignment films were not routinely obtained. Additionally, obtaining information via telephone interviews limits our ability to fully assess potential subclinical or radiographic evidence of minor growth disturbance. Finally, the results of this study are specific to a single site and surgical technique, which may, therefore, limit the generalizability of the results. The current study's findings should be interpreted relative to the surgical technique described, and further study is necessary to better understand optimal graft choice and fixation techniques. Despite these limitations, the findings of this study bear significant clinical relevance given the frequency of patellar instability in patients with open physes and the relative paucity of literature present on clinical outcomes of anatomic MPFL-R in skeletally immature patients, particularly at mid- to long-term follow-up.
Conclusion
Anatomic MPFL-R paired with concomitant procedures as indicated is a safe, efficacious, and durable treatment option for lateral patellar instability in adolescent patients with an open or partially open distal femoral physis.
Footnotes
Final revision submitted July 7, 2025; accepted July 26, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.A. has received grants from Smith & Nephew and Arthrex. E.L.K. has received hospitality payments from Arthrex, Pinnacle, Medical Device Business Services, and Stryker Corporation; and support for education from Great Lakes Orthopedics. D.R.D. has received royalties from DePuy Synthes Products, OsteoCentric Technologies, and Smith & Nephew; consulting fees from DePuy Synthes Products, Mitek, Medical Device Business Services, Smith & Nephew, and OsteoCentric Technologies; publishing royalties from Springer; and research support from Aesculap/B. Braun, DJ Orthopedics, and Moximed. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from The University of Virginia Health System.