
Abstract
Background:
The Anterior Cruciate Ligament Return to Sport after Injury (ACL-RSI) scale assesses psychological readiness for return to sport (RTS) following anterior cruciate ligament reconstruction (ACLR). Although developed and validated in accordance with ACLR recovery, psychological responses may apply to those recovering from medial patellofemoral ligament reconstruction (MPFLR).
Purpose:
To validate the use of the ACL-RSI scale in pediatric and adolescent patients who underwent MPFLR.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
Scores of the 12-item and shortened 6-item ACL-RSI for patients who underwent their first RTS readiness assessment after MPFLR were analyzed. Statistical analysis was performed using Spearman correlation for convergent validity testing against the International Knee Documentation Committee (IKDC)/Pediatric (Pedi-)IKDC score, Single Assessment Numeric Evaluation (SANE) score, and peak strength symmetry of knee extension and flexion. Discriminant validity testing was performed comparing ACL-RSI with age (Spearman correlation), body mass index (BMI) (Spearman correlation), and sex (Mann-Whitney U tests). Internal consistency reliability was tested using Cronbach alpha. Floor and ceiling effect testing was performed by calculating the proportion of minimum and maximum scores in the cohort.
Results:
A total of 32 patients (59% female; mean age, 15.6 ± 1.7 years) were included. Both 12-item and 6-item ACL-RSI scale versions demonstrated significant correlations of moderate to strong strength with the IKDC/Pedi-IKDC (R = 0.69 and R = 0.67, respectively; P < .001) and with the SANE score (R = 0.56 and R = 0.54, respectively; P = .002). Neither scale version was significantly correlated with peak strength symmetry of knee flexion or extension. Age, BMI, and sex were not significantly correlated with either scale. The 12-item ACL-RSI and 6-item short version demonstrated excellent internal reliability with a Cronbach alpha of .94 and .88, respectively, across individual items. No floor or ceiling effects were found with either scale as the minimum score, 0, was not observed and the maximum score, 100, was only observed twice in both versions (6%).
Conclusion:
The ACL-RSI scale may be valid for use in pediatric and adolescent patients who undergo MPFLR. Both the 12-item and the 6-item versions demonstrated convergent validity, discriminant validity, and internal reliability with no floor or ceiling effects. The 6-item scale version may be preferred, as it is able to quantify these vital psychological data but with minimal questionnaire burden and low redundancy.
The ACL-RSI scale was developed and validated in adults in 2008 24 and was later validated in children and adolescents in 2023. 4 The original ACL-RSI scale includes 12-items centered on 3 psychological subsections: emotions, confidence in performance, and risk appraisal. 24 A 6-item short form, a subset of the 12-item scale, has since been developed to reduce redundancy, 23 and it has been validated in children and adolescents. 4 Although developed in accordance with ACLR recovery, these domains are not unique to ACL injury and may apply to other knee injuries.
MPFLR is performed in patients with patellar instability to restore knee stability and function. 17 However, fear of reinjury is reported to be the primary reason for not returning to sports or to prior level of competition after patellar instability surgery.7,10 No study has assessed the validity of the ACL-RSI scale in patients after patellar instability surgery. This study aimed to validate the use of the ACL-RSI scale in pediatric and adolescent patients who underwent MPFLR.
Methods
Following institutional review board approval, patients ≤18 years of age who underwent MPFLR between January 2021 and September 2024 with 1 of 3 orthopaedic surgeons (P.D.F., D.W.G., or B.S.S.) and completed subsequent RTS assessment were retrospectively identified. Exclusion criteria included previous surgery on the affected knee, revision MPFLR, concomitant bony procedures (eg, tibial tubercle osteotomies, hemiepiphysiodesis), contralateral MPFLR within 3 months, and incomplete ACL-RSI data.
The authors’ preferred technique for MPFLR is variable but shares several common elements. Autograft or allograft gracilis or semitendinosus tendon is used in a 2-limbed graft configuration. Patellar fixation is performed either with 2 short sockets with tenodesis screw fixation or via an onlay technique, with 2 suture anchors placed ≥1 cm apart, centering the graft at the junction of the proximal third and distal two-thirds of the patella. For skeletally mature patients, an interference screw is used for femoral graft fixation. For skeletally immature patients, 1 surgeon (B.S.S.) uses an all-epiphyseal socket with tenodesis screw fixation, and 1 (P.D.F.) uses a double-loaded suture anchor for onlay femoral fixation. Both techniques are guided by palpation and direct visualization of the saddle between the adductor tubercle and medial epicondyle with radiographic confirmation of graft placement at the Schöttle point. In addition, isometrics with knee range of motion is checked before final fixation.
Patients underwent RTS readiness testing at a mean of 6 months following their surgeries with a physical therapist. The 12-item ACL-RSI, International Knee Documentation Committee (IKDC) questionnaire or Pediatric-IKDC (Pedi-IKDC), and Single Assessment Numeric Evaluation (SANE) scores were recorded at this visit. A 6-item ACL-RSI score was calculated by extracting responses from the 6 items that comprise the short version. Patients underwent hamstring and quadriceps muscle strength testing using either the isometric or the isokinetic method. Isometric testing was performed using a traction dynamometer (Kinvent Physio, Inc). Knee flexion strength was assessed in a prone position with the knee in 30° of flexion. Knee extension strength was assessed in a seated position with the knee in 90° of flexion. Patients performed 3 repetitions of maximal force. Isokinetic testing (Biodex System 4 isokinetic dynamometer; Biodex Medical System Inc) was performed in a seated position at a velocity of 180 deg/sec (10 repetitions). Two familiarization trials were performed, followed by maximal effort. Peak force for isometric testing and peak torque for isokinetic testing were extracted, and the ratio between the involved limb and uninvolved limb was calculated as the limb symmetry index using the following method: (involved limb/ uninvolved limb) x 100%.
Normality of the distribution of demographic variables and patient-reported outcome measures, including the ACL-RSI scores, was assessed using Shapiro-Wilk tests. Convergent validity testing of the 12-item and 6-item ACL-RSI scale versions were performed against the IKDC/Pedi-IKDC score, SANE score, and limb symmetry of knee flexion and extension strength using Spearman correlations for moderate or strong correlation strength (0.4-0.89). 21 Discriminant validity testing was performed comparing ACL-RSI with age (Spearman correlation), body mass index (BMI) (Spearman correlation), sex (Mann-Whitney U tests), race (Kruskal-Wallis), and ethnicity (Kruskal-Wallis) for an expected lack of significance (P > .05). Internal consistency reliability testing was performed by calculating Cronbach alpha. A Cronbach alpha of .70 to .95 was considered reliable with low redundancy between items. 22 Floor and ceiling effect testing was performed by calculating the proportion of minimum and maximum scores in the cohort. A floor or ceiling effect was considered present if >15% of patients achieved the lowest or highest possible score, respectively. Significance was set to P≤ .05 (2-tailed) for all other statistical analyses, which were performed on SPSS (Version 23.0; SPSS Inc).
Results
After applying exclusion criteria (Figure 1), 32 patients were included in the final analysis. The mean age at surgery was 15.6 ± 1.7 years, and 59% were female. There were 9 patients (28%) who sustained their first patellar dislocation, and 11 patients (34%) reported having experienced >3 dislocations on the affected patella. Seven patients had osteochondral fractures on magnetic resonance imaging. Three patients had contralateral patellar instability prior to enrollment in the current study (1 treated nonoperatively and 2 treated surgically). A total of 30 patients (94%) sustained their injury during sports participation, all of whom intended to RTS. All patients underwent primary MPFLR (29 autografts, 3 allografts). Concomitant procedures are listed in Table 1. The mean age at RTS readiness testing was 16.1 ± 1.7 years, and the median time between surgery and RTS visit was 6.5 months (range, 4.6-10.7 months). Because the RTS assessment used in the current study serves as the first assessment for readiness to RTS, none of the patients had been cleared to RTS at the time RTS data were collected. Of the 32 patients, 27 patients underwent isometric strength testing and 5 patients underwent isokinetic strength testing (Table 1). The median 12-item ACL-RSI score was 82.1 (range, 25.8-100.0), and the median 6-item ACL-RSI score was 80.0 (range, 20.0-100.0). The median IKDC/Pedi-IKDC score was 91.1 (range, 66.7-100.0), and the median SANE was 85 (range, 60-100). Knee flexion strength symmetry was 91% (range, 53%-195%), and knee extension strength symmetry was 92% (range, 46%-133%) (Table 2).

Patient inclusion and exclusion flow diagram. ACL-RSI, Anterior Cruciate Ligament Return to Sport after Injury; MPFLR, medial patellofemoral ligament reconstruction; RTS, return to sport.
Patient Characteristics (N = 32) a
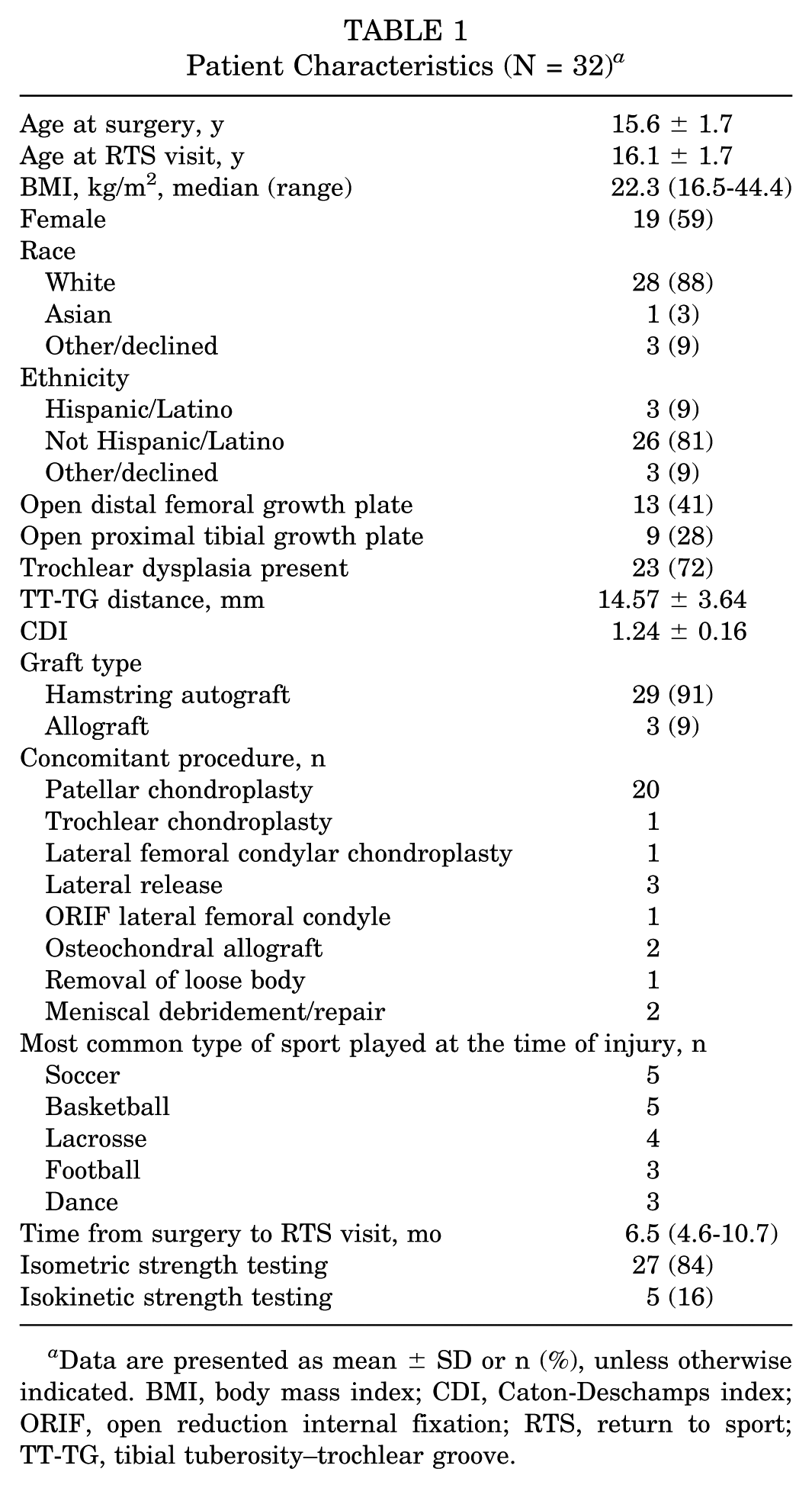
Data are presented as mean ± SD or n (%), unless otherwise indicated. BMI, body mass index; CDI, Caton-Deschamps index; ORIF, open reduction internal fixation; RTS, return to sport; TT-TG, tibial tuberosity–trochlear groove.
Patient-Reported Outcome Measures and Strength Symmetry (N = 32) a

ACL-RSI, Anterior Cruciate Ligament Return to Sport after Injury; IKDC, International Knee Documentation Committee; Pedi-IKDC, Pediatric IKDC; SANE, Single Assessment Numeric Evaluation.
The 12-item ACL-RSI scale demonstrated significant moderate strength correlations with the IKDC/Pedi-IKDC (R = 0.69; P < .001) and with the SANE score (R = 0.56; P = .002). The 12-item ACL-RSI scale was not significantly correlated with peak strength asymmetry of knee flexion (R = 0.15; P = .41) or extension (R = 0.02; P = .91). Age, BMI, and sex were not significantly correlated with the 12-item ACL-RSI.
The 6-item ACL-RSI scale demonstrated significant moderate strength correlations with the IKDC/Pedi-IKDC (R = 0.67; P < .001) and with the SANE score (R = 0.54; P = .002). The 6-item ACL-RSI scale was not significantly correlated with peak strength asymmetry of knee flexion (R = 0.18; P = .34) or extension (R = −0.02; P = .93). Age, BMI, and sex were not significantly correlated with the 6-item ACL-RSI (Table 3).
Convergent and Discriminant Validity Comparing Collected Variables to 12-Item and 6-Item ACL-RSI Scores (N = 32 except SANE) a
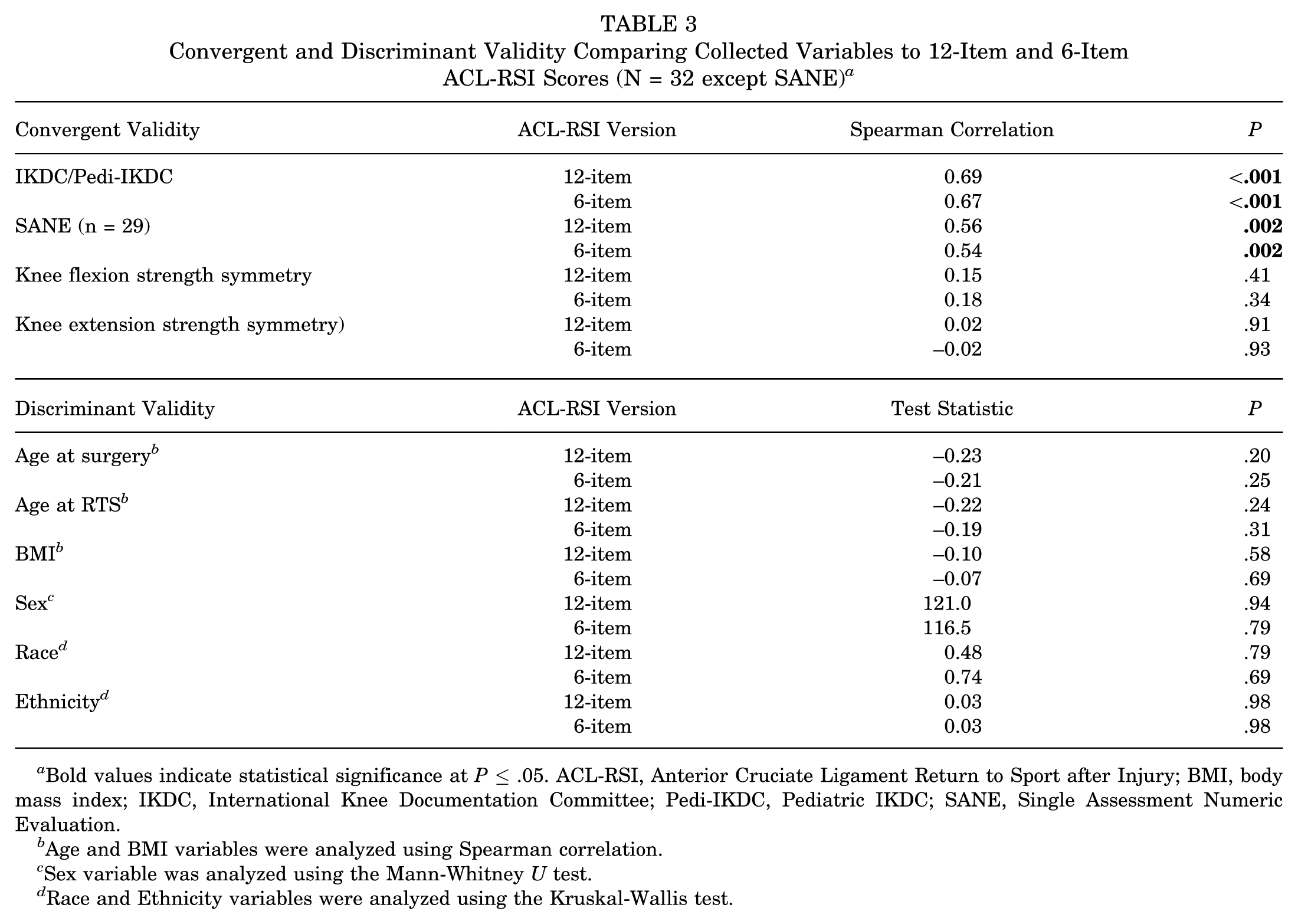
Bold values indicate statistical significance at P≤ .05. ACL-RSI, Anterior Cruciate Ligament Return to Sport after Injury; BMI, body mass index; IKDC, International Knee Documentation Committee; Pedi-IKDC, Pediatric IKDC; SANE, Single Assessment Numeric Evaluation.
Age and BMI variables were analyzed using Spearman correlation.
Sex variable was analyzed using the Mann-Whitney U test.
Race and Ethnicity variables were analyzed using the Kruskal-Wallis test.
The 12-item and 6-item ACL-RSI scale versions demonstrated excellent internal consistency reliability with a Cronbach alpha of .94 and .88, respectively, across individual items. Patient responses to each question are reported in Table 4. No floor or ceiling effects were found with either scale, as the minimum score (0) was not observed and the maximum score (100) was only observed twice in both versions (6%).
Analysis of Patient Responses to Each Question of the ACL-RSI Scale a
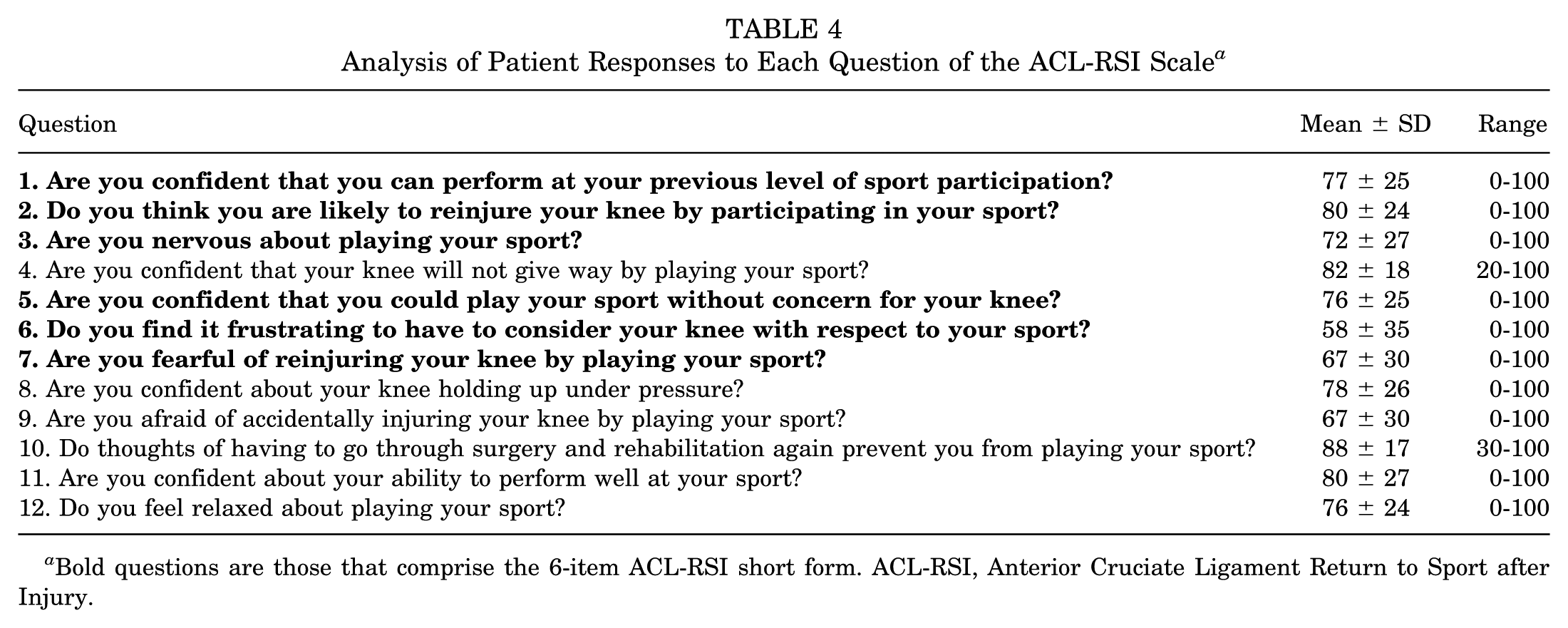
Bold questions are those that comprise the 6-item ACL-RSI short form. ACL-RSI, Anterior Cruciate Ligament Return to Sport after Injury.
Discussion
The incidence of patellar dislocations is highest among children and adolescents,5,19 and, as a result, so is the rate of surgical intervention.8,11 Approximately 15% of children and adolescents do not RTS, and up to 32% reduce their level of competition after patellar stabilization surgery.10,13 Fear of reinjury and lack of confidence are cited to be the most common reasons for not returning to sports or to their prior level of play after MPFLR.7,10,18 It is well-established that psychological factors play an important role in a safe RTS after ACLR.1-3,12,14 While the ACL-RSI scale was developed to assess patients’ emotions, confidence, and risk appraisal in preparation for RTS after ACLR, these items may also apply to patients after MPFLR. The results of this study demonstrate that the ACL-RSI may be a valid tool in pediatric and adolescent patients after MPFLR. Both the 12-item ACL-RSI and the 6-item short version demonstrated high convergent and discriminant validity without floor or ceiling effects.
The ACL-RSI scale was significantly correlated with validated patient reported outcome measures (PROMs) including the IKDC/Pedi-IKDC and SANE scores. The moderate correlation appropriately demonstrates the convergent validity of the 12-item and 6-item ACL-RSI scale, indicating that while the ACL-RSI scale is correlated with outcome measures that assess patient rating of knee function, it uniquely identifies self-reported confidence and fear related to performance, reinjury, and returning to prior level of play. 21 This finding is consistent with how the ACL-RSI scale relates to other PROMs in pediatric patients after ACLR. 4
The ACL-RSI scale was not significantly correlated with knee flexion or extension strength symmetry in this cohort, consistent with the previous study investigating the correlation between the ACL-RSI scale and strength symmetry in pediatric patients after ACLR. 4 The lack of correlation suggests that the ACL-RSI scale measures a distinct psychological construct rather than duplicating physical measurements. This result is consistent with a recent study that found objective physical measures of strength and power did not relate closely to self-reported psychological readiness in patients after ACLR. 16
The ACL-RSI scale versions demonstrated appropriate discriminant validity, as they were not associated with age, sex, or BMI. Additionally, both scale versions were found to have excellent internal consistency without floor or ceiling effects. However, the high value (Cronbach alpha of .94) indicates redundancy among the 12 questions. The 6-item short version demonstrated less redundancy (Cronbach alpha of .88) and may be preferred because of fewer items and therefore easier administration.
Despite the increase in case volume of MPFLR in pediatric and adolescent patients, 11 current literature lacks clearly defined objective criteria for assessing RTS readiness after MPFLR.1,6,9,25 However, because fear of reinjury is found to be a common reason for not returning to sport or to the same level of play after MPFLR, it is an important measure to assess during advanced rehabilitation and prior to RTS. In addition to objective data such as muscle strength, functional testing, and movement quality assessment, the ACL-RSI may be useful in assessing psychological factors as a component of a comprehensive RTS readiness screen after MPFLR.
Limitations
There are several limitations to this study. First, the sample size was limited, as several patients were excluded because of incomplete data collection. Second, this study included patients who were ≤18 years; therefore, the results of this study are not necessarily generalizable to patients >19 years of age. Although patellar instability injuries occur in young adults, this study focused on pediatric and adolescent athletes, as they are the highest risk demographic for patellar dislocations. Third, the method of muscle strength testing was not uniform and included both isokinetic and isometric testing because of physician preference as well as equipment available at multiple testing locations at our institution. However, analyses were performed using the limb symmetry index, which is a unitless ratio comparing involved with uninvolved leg that accounts for any differences and has been used in previous research. 4 Fourth, approximately half of the patients in this study received the IKDC. While the Pedi-IKDC is recommended for patients <17 years of age, prior studies have validated the use of the IKDC knee form in children as young as 6 years of age 20 and have also shown high correlation of the Pedi-IKDC and the IKDC in adolescents. 15 Finally, the participants underwent their RTS assessment visits at a mean of 6.5 months postoperatively. While 24 weeks is reported to be the most common timeline to begin to RTS after MPFLR in the pediatric orthopaedics literature, the range is reported to be from 12 to 28 weeks. 6 Therefore, administering the ACL-RSI scale at an earlier time frame, such as 12 weeks postoperatively, may yield useful information to assess and address psychological readiness in pediatric and adolescent patients after MPFLR.
Conclusion
This is the first study to validate and support the use of the ACL-RSI scale in pediatric and adolescent patients who undergo MPFLR. Both the 12-item and the 6-item scale versions demonstrated convergent validity, discriminant validity, and internal consistency reliability with no floor or ceiling effects. The 6-item ACL-RSI may be preferred over the 12-item scale as it is able to quantify these vital psychological data but with minimal questionnaire burden and lower redundancy, especially in this younger population.
Footnotes
Final revision submitted January 23, 2026; accepted February 6, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.S.S. has received royalties from CONMED Corporation and educational support from Arthrex and is on the medical publishing board of AOSSM. D.W.G. has received hospitality payments from Orthopediatrics and is on the board of the Patellofemoral Foundation and the NY State Society of Orthopaedic Surgeons and is a consultant for Arthrex Inc. D.W.G. also receives royalties from Arthrex Inc. and faculty/speaker fees from Synthes. P.D.F. has received consulting fees from BICMD Inc and OssoVR and publishing royalties from Springer Nature; he serves as associate editor of Clinical Orthopedics and Related Research. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Hospital for Special Surgery (No. 2022-2301).