
Abstract
Background:
Tendinopathies are common in middle-aged women. While estrogen regulates tendon remodeling, the influence of systemic hormone replacement therapy (HRT) on the risk of tendon degeneration remains unclear.
Hypothesis/Purpose:
The purpose of this study was to investigate the association between systemic HRT use and tendon injuries/repair in perimenopausal women. It was hypothesized that systemic HRT would be associated with an increased incidence of tendon injuries and repair.
Study Design:
Cohort study; Level of evidence, 4.
Methods:
Using the TriNetX Research Network, we identified female patients aged ≥45 years diagnosed with major tendon abnormalities, including rotator cuff tears, bicipital tendinitis, lateral or medial epicondylitis, Achilles tendinopathy, patellar tendinitis, or quadriceps strain, from January 2004 to July 2025. HRT exposure was defined as systemic estrogen and/or progestin use within 1 year before a diagnosis. Patients with contraindications to HRT were excluded. After 1:1 propensity score matching, 2 groups of 63,836 patients each were generated. Primary outcomes included diagnosis rates of specific tendon conditions; secondary outcomes were lifetime rates of corresponding tendon repair procedures. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. The independent t test and chi-square test were used for analysis.
Results:
HRT users had significantly higher rates of several tendon abnormalities compared to matched controls, including rotator cuff tears (39.2% vs 37.9%, respectively; P < .001), bicipital tendinitis (13.3% vs 11.0%, respectively; P < .001), lateral epicondylitis (27.8% vs 22.7%, respectively; P < .001), and medial epicondylitis (6.8% vs 5.3%, respectively; P < .001). Achilles tendinopathy had similar rates between the 2 groups (14.6% vs 14.5%, respectively; P = .387). Surgical repair was more common in the HRT group, including biceps tendon repair/tenodesis (3.9% vs 3.3%, respectively; OR, 1.16 [95% CI, 1.10-1.23]; P < .001), rotator cuff repair (6.6% vs 6.2%, respectively; OR, 1.06 [95% CI, 1.01-1.11]; P = .013), and Achilles tendon repair (0.7% vs 0.6%, respectively; OR, 1.23 [95% CI, 1.06-1.41]; P = .005).
Conclusion:
Our study showed that systemic HRT use in women aged ≥45 years was associated with an increased risk of tendon injuries and a greater likelihood of surgical repair, although the absolute risk differences were modest. These findings underscore the need for awareness of the possible musculoskeletal effects of hormone therapy and highlight an underexplored area in women's orthopaedic health.
Tendon disorders are among the most common musculoskeletal conditions affecting adults, with their prevalence rising steadily with age.21,38 These injuries range from degenerative tendinopathies to full-thickness ruptures and frequently result in pain, functional limitations, and long-term disability. 36 Many cases require prolonged nonoperative management, and a significant proportion ultimately undergo surgical repair. 36 While the burden of a tendon injury is well documented, less attention has been given to systemic biological factors that may predispose certain populations, particularly women, to an increased risk.4,9
Hormonal influences on tendon biology are increasingly recognized as a contributing factor in sex-specific injury patterns. 14 Estrogen receptors are expressed in tenocytes, and estrogen has been shown to regulate collagen turnover, tendon stiffness, and healing capacity. 14 Experimental models have demonstrated that both estrogen deficiency and supraphysiological supplementation can alter extracellular matrix organization, potentially reducing mechanical strength and compromising tendon integrity.23,28 These mechanisms are especially relevant during the perimenopausal transition, when women experience significant endocrine changes and report increased rates of generalized musculoskeletal symptoms. 26 Up to 70% of perimenopausal women develop new-onset joint or soft tissue discomfort, often localized to tendon-rich regions such as the shoulder, elbow, or Achilles tendon. 26
Hormone replacement therapy (HRT), consisting of exogenous estrogen with or without progestin, is widely prescribed to relieve menopausal symptoms. 17 Some studies suggest that HRT may influence tendon remodeling or protect against degenerative changes, but the evidence remains limited and inconsistent.1,9,12 Despite the broad clinical use of HRT, its musculoskeletal effects, particularly on tendons, remain insufficiently characterized at the population level. The relationship between systemic HRT exposure and tendon-specific outcomes, including injury diagnosis and surgical repair, is underexplored in real-world settings. Thus, the purpose of this study was to investigate the association between systemic HRT use and the incidence of common tendon injuries and surgical repair in a national cohort of perimenopausal women. We hypothesized that systemic HRT use would be associated with an increased incidence of tendon abnormalities and repair procedures among perimenopausal women.
Methods
Data Source
This retrospective cohort study was conducted using the TriNetX Research Network (TriNetX), a federated health research platform comprising deidentified electronic health records from more than 100 health care organizations across the United States and internationally, from January 2004 to July 2025. At the time of our query in July 2025, the network included over 140 million patients. 31 TriNetX has been previously validated for large-scale outcomes research and provides access to demographic information, diagnoses, procedures, medications, and laboratory values.27,29 Because the data are deidentified and compliant with the Health Insurance Portability and Accountability Act, this study was exempt from institutional review board approval.
Study Population
The study population consisted of female patients aged ≥45 years with a recorded diagnosis of at least one major tendon abnormality. Within this population, patients were stratified into 2 groups based on HRT exposure. Tendon abnormalities included rotator cuff tears, bicipital tendinitis, lateral or medial epicondylitis, Achilles tendinopathy, patellar tendinitis, and quadriceps strain (see AppendixTable A1 for codes). The date of the first qualifying diagnosis was defined as the index event. Patients were considered HRT users if they received systemic estrogen and/or progestin within the year before the index diagnosis. Those with contraindications to HRT, such as a personal history of breast or endometrial cancer, venous thromboembolism, myocardial infarction, stroke, or liver disease, were excluded from both groups.
Outcomes of Interest
The primary outcomes were diagnosis rates of specific tendon injuries. Secondary outcomes included any subsequent repair procedures corresponding to the tendon injury, as captured in the longitudinal patient record (AppendixTable A1).
Propensity Score Matching
To reduce confounding, 1:1 propensity score matching was conducted using nearest neighbor algorithms without replacement. Matching variables included age, race, body mass index, baseline comorbidities (including those in the Charlson Comorbidity Index), serum albumin level, and relevant medication exposures (eg, corticosteroids, fluoroquinolones). Inflammatory conditions (eg, systemic lupus erythematosus, rheumatoid arthritis, ankylosing spondylitis) as well as neoplasms and chemotherapy usage were also matched. All matching variables had a target of <0.1 for the standardized mean difference.
Statistical Analysis
Descriptive statistics were reported as means ± standard deviations for continuous variables and as frequencies and percentages for categorical variables. Between-group comparisons were made using the independent-samples t test or chi-square test, as appropriate. Odds ratios (ORs) and 95% confidence intervals (CIs) were generated using TriNetX's built-in “Compare Outcomes” tool. Cells containing <10 patients were suppressed in accordance with TriNetX privacy protocols. A 2-sided P value <.05 was considered statistically significant. Data visualization and figure generation were performed using RStudio (Version 2022.12.0; Posit).
Results
Cohort Characteristics
Among 638,357 eligible female patients aged ≥45 years with a diagnosis of a tendon injury, 61,015 had documented systemic HRT use within the preceding year. After 1:1 propensity score matching, 2 well-balanced groups of 63,836 patients each were formed (Table 1).
Patient Characteristics a
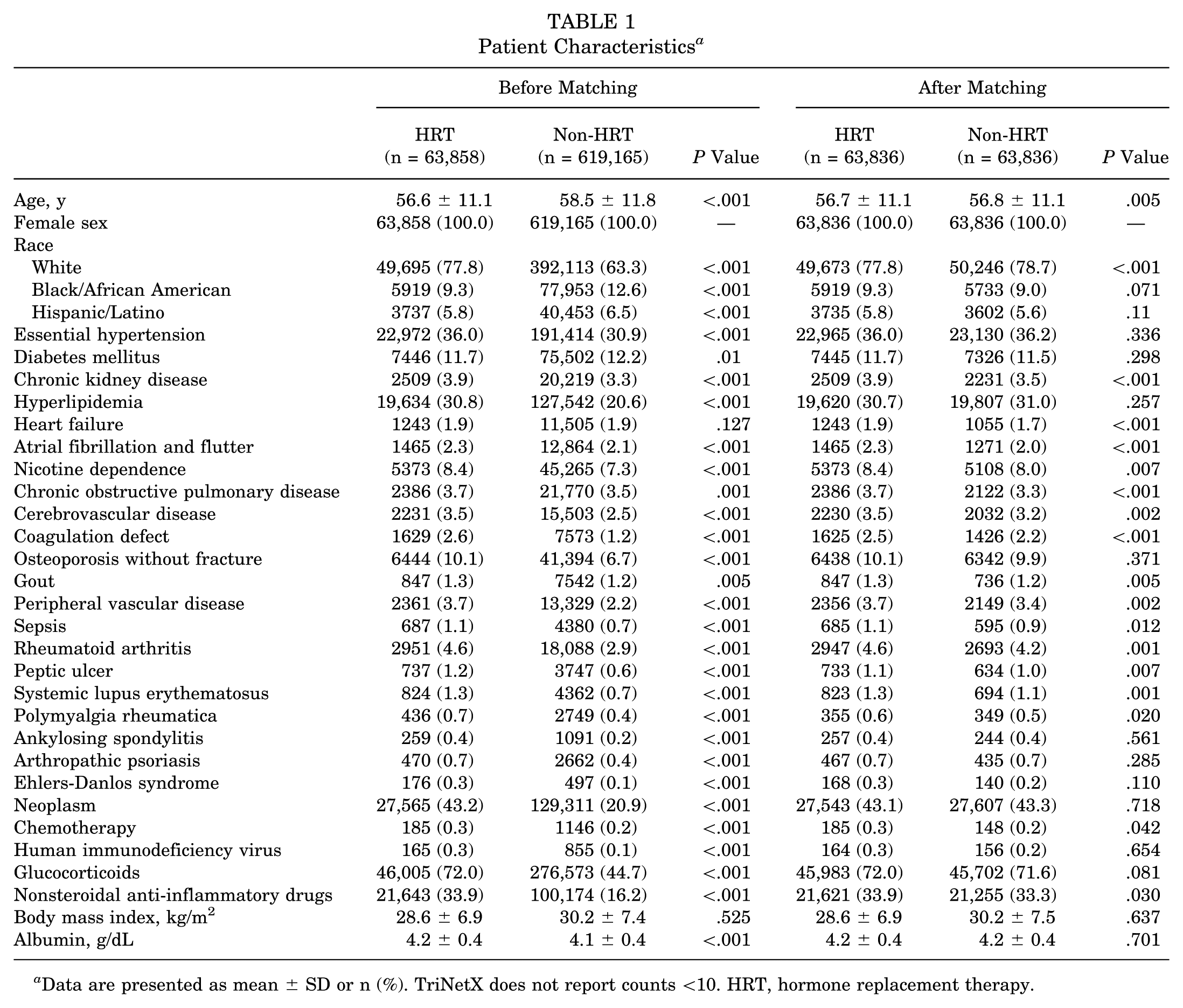
Data are presented as mean ± SD or n (%). TriNetX does not report counts <10. HRT, hormone replacement therapy.
Tendon Injuries
Some tendon injury types were found to be more frequent among HRT users compared to matched controls. Rotator cuff tears were most common (25,044 [39.2%] vs 24,182 [37.9%], respectively; P < .001), followed by lateral epicondylitis (17,757 [27.8%] vs 14,468 [22.7%], respectively; P < .001), bicipital tendinitis (8514 [13.3%] vs 6999 [11.0%], respectively; P < .001), Achilles tendinopathy (9347 [14.6%] vs 9238 [14.5%], respectively; P = .387), and medial epicondylitis (4323 [6.8%] vs 3374 [5.3%], respectively; P < .001). Patellar tendinitis was slightly more common in HRT users (1876 [2.9%] vs 1796 [2.8%], respectively; P = .180), while quadriceps strain was slightly less frequent (690 [1.1%] vs 763 [1.2%], respectively; P = .054) (Figure 1 and AppendixTable A2).

Rate of tendon injuries in the hormone replacement therapy (HRT) and non-HRT groups (n = 63,836 each). *P < .05.
Tendon Repair
Tendon repair was modestly more common among HRT users compared to matched controls. Higher rates were observed for biceps tendon repair/tenodesis (3.9% vs 3.3%, respectively; OR, 1.16 [95% CI, 1.10-1.23]; P < .001), rotator cuff repair (6.6% vs 6.2%, respectively; OR, 1.06 [95% CI, 1.01-1.11]; P = .013), and Achilles tendon repair (0.7% vs 0.6%, respectively; OR, 1.23 [95% CI, 1.06-1.41]; P = .005) (Table 2).
Rates of Tendon Repair a

Data are presented as n (%) unless otherwise indicated. HRT, hormone replacement therapy; OR, odds ratio.
Discussion
The major findings of our study of over 63,000 perimenopausal women are that systemic HRT use in perimenopausal women was associated with significantly increased rates of tendon injuries and surgical repair. Specifically, HRT users exhibited higher diagnosis rates for rotator cuff tears (39.2% vs 37.9%, respectively), lateral epicondylitis (27.8% vs 22.7%, respectively), and bicipital tendinitis (13.3% vs 11.0%, respectively) compared to matched controls (P < .001). Furthermore, HRT use was associated with increased odds of a surgical intervention, including Achilles tendon repair (OR, 1.23) and biceps tenodesis (OR, 1.16). These findings suggest that chronic hormone exposure in perimenopausal women may increase tendon susceptibility to degenerative or traumatic injuries and raise the likelihood of the progression to operative management.
The results of the present study may appear to conflict with the body of evidence suggesting the beneficial role of estrogen in maintaining connective tissue health, especially in the context of an estrogen-deficient state. The decline in estradiol during the menopausal transition is understood to be a primary driver of a broader “musculoskeletal syndrome of menopause,” which encompasses not only bone and muscle loss but also an increased risk of tendon and ligament injuries. 39 This is biologically plausible, as tendons are known to be hormonally responsive tissue, with tenocytes expressing both estrogen receptor alpha (ER-α) and estrogen receptor beta (ER-β). 23 The estrogen-deficient state is associated with reduced collagen production, fiber diameter shrinkage, and catabolic tissue turnover, which can weaken tendons and make them more susceptible to damage.9,30 However, while it is hypothesized that supplemental estrogen via HRT may be beneficial for preserving tendon collagen and reducing tendon abnormalities, the overall body of research on this remains ambiguous, with inconsistent data on the relationship between female sex hormone supplementation and tendon outcomes.10,23
Biological and molecular evidence further describes the complex role of estrogen in tendon homeostasis and its links to impaired regenerative abilities.6,9 In vitro studies have shown that estradiol can suppress type I collagen production while upregulating matrix metalloproteinases (MMPs), thereby weakening structural integrity.4,34 Animal models have further demonstrated that estrogen deficiency disrupts collagen fiber alignment and reduces mechanical strength, while estrogen levels over physiological limits may impair the normal tendon healing response.1,13,19 These effects are particularly relevant in dense, load-bearing tendons such as the rotator cuff and Achilles tendon, which experience high repetitive stress and require efficient remodeling to maintain function.7,35 Further in vivo studies using stable isotope tracers have revealed that while HRT is associated with a markedly higher rate of tendon collagen synthesis at rest, it simultaneously blunts the adaptive collagen synthesis response after exercise. 15 This blunting effect has also been observed in young women using oral contraceptives containing high levels of synthetic estrogen, which were found to suppress the normal exercise-induced increase in collagen synthesis in both tendon and muscle connective tissue. 16 This suggests that while estrogen promotes a higher baseline of tissue turnover, it may impair the tendon's ability to mount an appropriate hypertrophic response to mechanical loading. This is accompanied by a shift toward a higher proportion of smaller collagen fibrils and a reduction in tendon stiffness (lower Young modulus) in the estrogen-rich state, which may compromise mechanical strength and resilience to loading. 15 High estrogen levels are also associated with a decreased tendon cross-sectional area in physically active women, which further potentiates the reduction in tendon robustness under certain conditions. 8
Estradiol acts nongenomically to inhibit the enzyme lysyl oxidase (LOX), which is the catalyst for covalent collagen cross-links that give tendons their tensile strength. 24 In engineered human anterior cruciate ligament constructs, 48-hour exposure to physiologically high estradiol cut LOX activity by approximately 80% and decreased the tangent modulus, despite a slight rise in total collagen content.4,24 Fewer mature cross-links translate into a more compliant but mechanically weaker tendon. Continuous systemic dosing in HRT mimics a chronic midluteal hormonal environment, sufficient to keep LOX suppressed and MMPs primed but lacking the physiological estrogen troughs that may permit matrix recovery. 24 The triad of LOX inhibition, catabolic MMP upregulation, and poor load-induced responses could provide the driving mechanism for the higher odds of tendon abnormalities and subsequent repair seen in the present study. This is in addition to the overall increase in activity levels and muscle performance often reported with HRT users, which can amplify tendon loading and predispose to failure. 32
Overall, estradiol appears to exhibit a U-shaped, level-specific relation with tendon health: lower estrogen levels reduce collagen synthesis, fiber diameter, and tensile strength, while sustained high levels undermine cross-link maturation and adaptive remodeling.4,9,15,40 The present data capture the latter end of the curve. Timing, dose, delivery route (oral vs transdermal), receptor-isoform balance, activity level, and the presence of progestins modulate where a patient might fall on this curve, explaining the differences seen in the literature. Future prospective studies incorporating hormonal profiling, biomechanical assessments, and longitudinal imaging are needed to clarify whether specific HRT formulations, doses, or durations confer an increased risk and whether targeted tendon screening or injury prevention strategies may be beneficial in this population.
Progesterone may also influence tendon physiology, although this has been less extensively studied.1,25 Experimental data suggest that progesterone may alter tenocyte activity and shift the MMP-to-inhibitor balance toward matrix breakdown, compounding the degradative effects of estrogen.2,3,22 In addition to direct structural changes, hormone-induced alterations in neuromuscular control, such as decreased proprioceptive acuity, reduced tendon stiffness, and impaired coordination, have been proposed as contributors to tendon overloading and the injury risk in middle-aged women. 18 These mechanisms may also help to explain the higher observed rates of tendinopathy and surgical repair among HRT users in our cohort. 10
An important factor to consider is that HRT users could have unmeasured differences in lifestyle or health care behavior that contribute to higher recorded injury rates. Women on HRT may be more health conscious or physically active, on average (eg, engaging in exercise to manage weight and health during menopause), which would expose them to a greater risk of sports or overuse injuries.11,37 They also have regular medical contact for prescription management, which might lead to more frequent reporting and diagnoses of musculoskeletal complaints. Despite the strict matching protocol used, residual confounders such as activity level, occupational demands, or baseline tendon degeneration were not captured in our data. It is therefore possible that the observed association is partly caused by such factors rather than a direct causal effect of HRT. Nonetheless, even if health care utilization played a role, the consistent pattern across multiple tendon sites and the higher surgical rates in HRT users suggest a real and clinically relevant signal.
Finally, testosterone therapy is also increasingly utilized in perimenopausal women, primarily for hypoactive sexual desire disorder. Unlike estrogen, which can decrease tendon stiffness and increase laxity, testosterone has been shown to enhance collagen synthesis and tendon stiffness in animal models. 33 While supraphysiological testosterone doses (eg, in male anabolic steroid users) are associated with an increased tendon rupture risk due to muscle hypertrophy outpacing tendon adaptation, the musculoskeletal effects of physiological testosterone replacement in women remain undercharacterized.5,20 Future research should specifically isolate this cohort to determine if testosterone confers a protective or deleterious effect on tendon integrity.
Several limitations warrant a discussion. The use of the TriNetX network and diagnosis codes meant dependence on the accuracy of clinical coding with possibilities for underdiagnosing or overdiagnosing. The retrospective study design could not establish causality, only association. HRT exposure, as defined in this study, did not account for the duration or dosage of therapy and only accounted for any HRT use within 1 year of the injury and subsequent surgery because of limitations in the database. No separate analysis between estrogen-only therapy and combined estrogen-progesterone therapy was conducted, and different therapies (eg, testosterone replacement therapy) might yield different risks for tendon abnormalities. Despite rigorous propensity score matching on many variables, physical activity and health care utilization could not be matched because of the lack of respective data within the database. Future analyses could benefit from a time-to-event approach to assess whether longer exposure correlates with a higher cumulative risk. While the associations observed in this study were statistically significant, the absolute risk differences between groups were generally modest (eg, a 1.3% absolute increase in rotator cuff tears). Therefore, these findings should be interpreted as one of many factors contributing to musculoskeletal health in this population rather than a sole determinant for clinical decision making regarding HRT prescription. Finally, as specific International Classification of Diseases–10th Revision (ICD-10) codes for quadriceps tendinopathy do not exist, we utilized the code for “strain of quadriceps muscle, fascia and tendon,” which may capture muscle injuries not strictly related to tendon abnormalities. We also noted that unlike the biceps tendon (which has a specific code, M75.2, for “bicipital tendinitis”), the rotator cuff lacks a specific ICD-10 code for noncalcific tendinitis, which is why “rotator cuff tear or rupture, not specified as traumatic” (M75.1) was used. These were still included to cover a breadth of tendon abnormalities across the studied population.
Conclusion
Our study showed that systemic HRT use in women aged ≥45 years was associated with an increased risk of tendon injuries and a greater likelihood of surgical repair, although the absolute risk differences were modest. These findings underscore the need for awareness of the musculoskeletal effects of hormone therapy and highlight an underexplored area in women's orthopaedic health.
Footnotes
Appendix
Tendon Injuries After Propensity Score Matching a

| HRT (n = 63,836) | Non-HRT (n = 63,836) | P Value | |
|---|---|---|---|
| Rotator cuff tear | 25,044 (39.2) | 24,182 (37.9) | <.001 |
| Bicipital tendinitis | 8514 (13.3) | 6999 (11.0) | <.001 |
| Lateral epicondylitis | 17,757 (27.8) | 14,468 (22.7) | <.001 |
| Medial epicondylitis | 4323 (6.8) | 3374 (5.3) | <.001 |
| Patellar tendinitis | 1876 (2.9) | 1796 (2.8) | .180 |
| Quadriceps strain | 690 (1.1) | 763 (1.2) | .054 |
| Achilles tendinopathy | 9347 (14.6) | 9238 (14.5) | .387 |
Data are presented as n (%). HRT, hormone replacement therapy.
Final revision submitted January 5, 2026; accepted February 1, 2026.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.