
Abstract
Background:
There is a paucity of literature investigating the effect of preoperative opioid use on outcomes after hip arthroscopy.
Purpose:
To evaluate the short-term outcomes and the recovery curve of patients undergoing hip arthroscopy for femoroacetabular impingement (FAI) and labral tears who reported preoperative opioid use and to compare these results to a control group of patients without preoperative opioid use.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We retrospectively analyzed data for patients who underwent primary hip arthroscopy for FAI and labral tears between 2009 and 2021. Patients were included if they reported daily opioid-based pain management within 1 year of surgery (preoperative opioid [PO] group) and had completed preoperative and postoperative patient-reported outcome (PRO) measures at 2-year follow-up. Patients were propensity score matched in a 1:1 ratio to a control group based on sex, age, body mass index, acetabular Outerbridge grade, and labral and capsular treatment. Analysis included comparisons of PROs at 3 months, 1 year, and 2 years as well as clinical thresholds and secondary surgery.
Results:
A total of 236 patients in the PO group were matched to 236 control cases. The PO group demonstrated significant improvements on all PRO measures at 2-year follow-up. Compared to the control group, the PO group had lower preoperative scores for the modified Harris Hip Score (mHHS), Non-Arthritic Hip Score (NAHS), and Hip Outcome Score–Sports-Specific Subscale (HOS-SSS) and experienced a prolonged recovery, as indicated by lower mHHS and HOS-SSS scores at 3 months and lower mHHS, HOS-SSS and NAHS scores at 1 year. However, by 2-year follow-up, the PO group achieved comparable scores for the mHHS, NAHS, HOS-SSS, and visual analog scale (VAS). Despite these improvements, the PO group reported lower patient satisfaction compared to the control group (6.3 vs 8.7, respectively; P = .03), reaching the PASS for the VAS at a lower rate (P = .03). No significant differences were observed for secondary surgery rates.
Conclusion:
Hip arthroscopy for the treatment of FAI and labral tears in patients using daily opioid-based pain control resulted in significant short-term improvements in PROs. Compared to a control group, these patients experienced a prolonged recovery process but ultimately achieved comparable functional outcomes at 2-year follow-up. Despite these improvements, they reported lower patient satisfaction and met the PASS for the VAS at a lower rate.
Keywords
Preoperative opioid-based pain control is recognized as an adverse prognostic factor in multiple orthopaedic procedures, often leading to lower patient-reported outcomes (PROs), higher complication rates, and an increased likelihood of secondary surgery.2,11,15,23 Femoroacetabular impingement (FAI), a common source of chronic hip pain, is usually treated surgically with hip arthroscopy when nonoperative measures have failed, showing consistently favorable outcomes.8-10,14,16,22 Prior research has shown that up to 30% of patients waiting for hip arthroscopy are on an opioid-based pain management protocol.12,20,26
While preoperative opioid use has been shown to increase the risk of chronic postoperative consumption, less attention has been given to evaluating the impact of preoperative opioid use on surgical outcomes in this patient population.6,7,26 Several reports on the topic, to date, suggest that preoperative opioid use has been associated with lower baseline and postoperative functional scores as well as an increased risk of revision surgery.2,19 For instance, Maldonado et al 17 conducted a study comparing 17 patients with preoperative opioid consumption to a control group of opioid-naïve patients who underwent hip arthroscopy for FAI. The authors observed that patients with preoperative opioid use had lower preoperative scores on the Non-Arthritic Hip Score (NAHS). 17 Postoperatively, visual analog scale (VAS) pain scores were significantly higher at 1- and 6-month follow-up, while modified Harris Hip Score (mHHS) values were significantly lower at the 2-year mark compared to the opioid-naïve group.
The present study aimed to build on the findings of the aforementioned study by analyzing a larger cohort, incorporating additional validated hip PRO measures, and evaluating short-term outcomes and the recovery curve of patients undergoing hip arthroscopy for FAI and labral tears who reported preoperative opioid use. A secondary analysis compared these results to a control group of patients without preoperative opioid use. We hypothesized that while patients with preoperative opioid use would experience significant improvements after hip arthroscopy, their recovery curve would be significantly longer compared to those without opioid consumption.
Methods
Study Design
All patients included in this study consented to participate in the American Hip Institute Hip Preservation Registry. Although the findings of the present study represent a unique analysis, some patient data may have been reported and used in previous studies. This study was performed in accordance with the ethical standards of the 1964 Declaration of Helsinki. This study was carried out in accordance with relevant regulations of the United States Health Insurance Portability and Accountability Act.
Patient Selection and Data Collection
Prospectively collected data were analyzed for patients who underwent primary hip arthroscopy to treat FAI and labral tears at the American Hip Institute between November 2009 and July 2021. Patients were included if they reported daily opioid-based pain control medications within 1 year of surgery and had completed a minimum 2-year follow-up. This was defined as having completed the mHHS, NAHS, Hip Outcome Score–Sports-Specific Subscale (HOS-SSS), patient satisfaction questionnaire, and VAS for pain preoperatively and postoperatively, or documenting an endpoint, defined as revision hip arthroscopy or conversion to total hip arthroplasty. Patients were excluded if they had previous ipsilateral hip abnormalities, hip dysplasia defined as a lateral center edge angle (LCEA) <18°, documented spine abnormalities, open work compensation claims, or a preoperative Tonnis grade >1 (Figure 1).
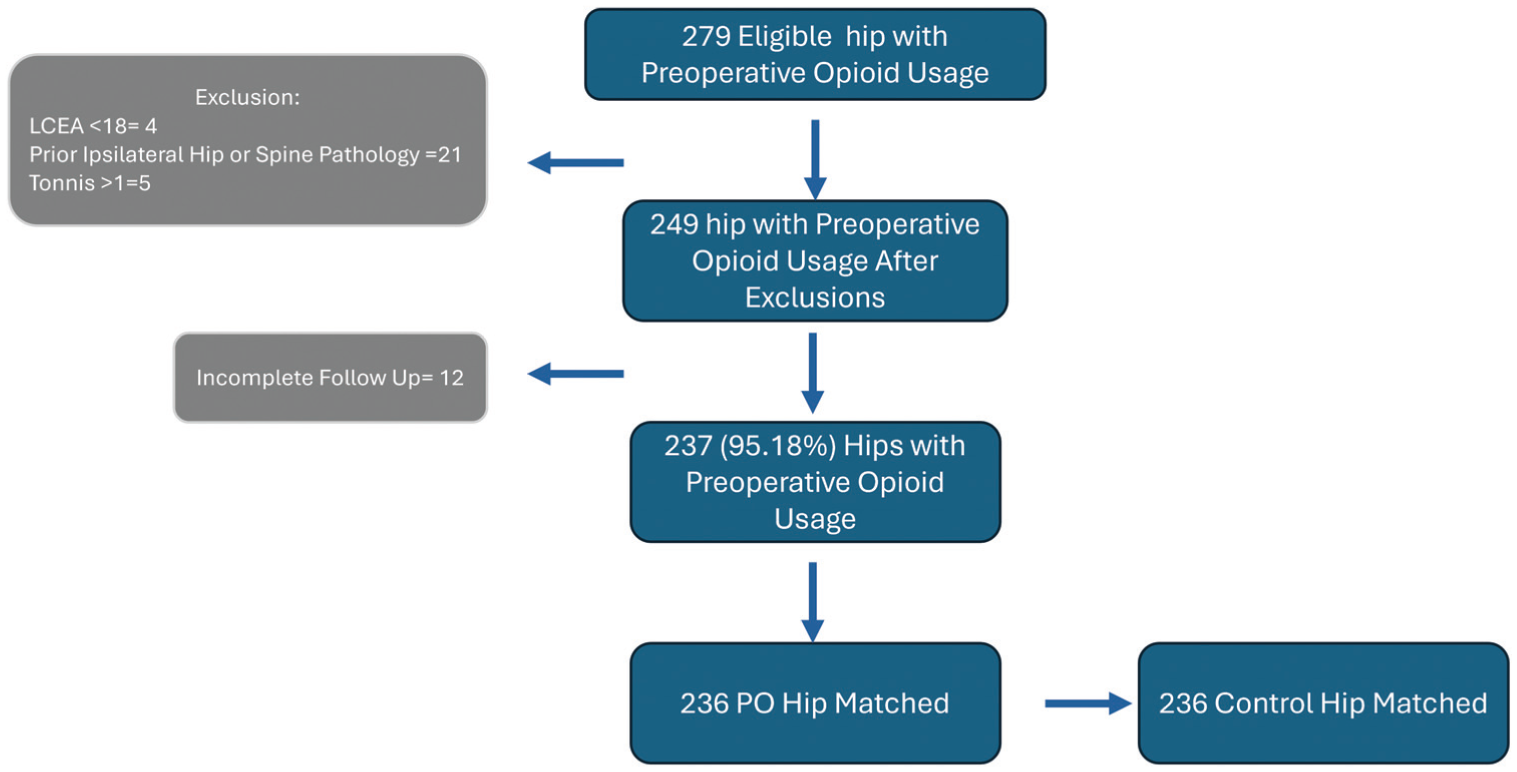
Patient selection flowchart. PO, preoperative opioid.
PRO analysis included comparisons at the 3-month, 1-year, and 2-year time points. Complications, revision hip arthroscopy, and conversion to total hip arthroplasty were documented at clinical visits and on follow-up questionnaires.
Radiographic Imaging
Patients underwent preoperative and postoperative radiography as the standard of care: upright and supine anteroposterior pelvic, false profile, and 45° Dunn views. Lateral acetabular coverage was approximated using the LCEA in the supine anteroposterior pelvic view. The alpha angle was measured in the Dunn view, with values >60° being defined as cam deformities of the femoral head-neck junction. 25 Radiography was performed using a picture archiving and communication system (GE Healthcare).
Surgical Indications
Patients who met the following criteria were recommended for an arthroscopic hip intervention: presented symptomatically with FAI and labral tears based on a provocative examination and patient history; underwent a radiographic analysis; showed a compromised labral abnormality on magnetic resonance imaging; and failed to improve after a minimum of 3 months of nonoperative treatment including rest, activity modification, nonsteroidal anti-inflammatory drugs, and physical therapy. Before the surgical intervention, all patients underwent a physical examination and consultation with the senior author (B.G.D.), which included counseling on the associated risks of preoperative opioid consumption.
Surgical Interventions
All surgical procedures were performed by the senior author. Each patient was positioned in a modified supine position on a postless traction table. To access the joint, a minimum of 2 portals were used (anterolateral and midanterior portals). 17 Other portals were used on a case-by-case basis. Interportal capsulotomy was performed to access the joint. Diagnostic arthroscopy was conducted to initially assess the labrum, intra-articular cartilage, and ligamentum teres. Labral tears were categorized using the Seldes classification system. 24 Femoral head chondral injuries were noted using the ALAD (acetabular labrum articular disruption) and Outerbridge classification systems. Tears of the ligamentum teres were defined using the Domb and Villar classification systems.1,3
With the use of a mechanical bur under fluoroscopic guidance, cam and pincer osseous deformities were corrected with femoroplasty and acetabuloplasty. Labral tears were either repaired or selectively debrided to maximize stability. If the labral tear was unrepairable, allografts were used to perform labral reconstruction. If full-thickness chondral defects were present, microfracture was performed. 9 Patients who had a history of painful internal snapping hip syndrome underwent iliopsoas fractional lengthening. 4 Ligamentum teres tears were treated with debridement if necessary. 5 With a multifactorial consideration of age, range of motion, generalized ligamentous laxity, acetabular coverage, and arthritic changes, the capsule was released or repaired. 13
Propensity Score Matching
Using R (Version 4.3.2; R Foundation for Statistical Computing), propensity score matching was used to control potentially confounding variables. Patients with a history of daily opioid-based pain control medications were included in the preoperative opioid (PO) group. Patients were matched in a 1:1 ratio based on age at the time of surgery, sex, body mass index, acetabular Outerbridge grade, labral treatment, and capsular treatment to a control group of patients without a history of preoperative opioid consumption. Matching was performed with an optimal pair matching algorithm and a caliper of 0.2 times the logit of the propensity score. Matching was then performed until no further matches could be made.
Statistical Analysis
The minimal clinically important difference (MCID) was determined using a distribution-based method with 2-year PROs. 21 The MCID calculated for the PO group was 7.66 for the mHHS, 8.44 for the NAHS, and 11.86 for the HOS-SSS. The MCID calculated for the control group was 7.94 for the mHHS, 8.74 for the NAHS, and 11.89 for the HOS-SSS. Additionally, the patient acceptable symptom state (PASS) was determined using an anchor-based method. 18 For the PASS, patients answered “yes” or “no” to the following anchor question at the 2-year time point: “Taking into account all the activities you have during your daily life, your level of pain, and also your functional impairment, do you consider that the state of your right/left hip is satisfactory?” Patients who answered “yes” were considered positive responders, and patients who answered “no” were considered nonresponders. To calculate these thresholds, PROs at 2-year follow-up were used to create a receiver operating characteristic curve to discriminate and determine a value that qualitatively separated the 2 groups: the PASS calculated for the PO group was 73.0 for the mHHS, 76.8 for the NAHS, and 68.8 for the HOS-SSS, while the PASS calculated for the control group was 75.0 for the mHHS, 78.1 for the NAHS, and 68.1 for the HOS-SSS. The area under the curve for all evaluated PASS thresholds indicated excellent discrimination (>0.8).
A priori power analysis was used to determine the sample size needed in each matched group to achieve 80% power. With a mean difference of 8 and a standard deviation of 15 between groups for the mHHS and alpha set to 0.05, power analysis determined that 57 patients were required in each group. For continuous variables, the Shapiro-Wilk test was performed to evaluate for a normal distribution, with P > .05 indicating normality. The paired 2-tailed t test or Wilcoxon signed-rank test was used to compare continuous data between groups. To detect significant differences between categorical variables, the chi-square and Fisher exact tests were used. Descriptive statistics including means, standard deviations, proportions, and ranges were reported when relevant. All statistical analyses were performed using R (Version 4.3.2).
Results
Patient Characteristics
A total of 472 patients were included in the study who had completed a minimum 2-year follow-up. There were 236 patients in the PO group who were successfully matched to 236 control patients without opioid consumption. The PO group consisted of 149 female and 87 male patients; the mean age at the time of surgery was 38.49 ± 13.87 years, with a mean follow-up of 72.26 ± 31.97 months. Between the groups, there was no significant difference in patient characteristics (P > .05) (Table 1).
Patient Characteristics a
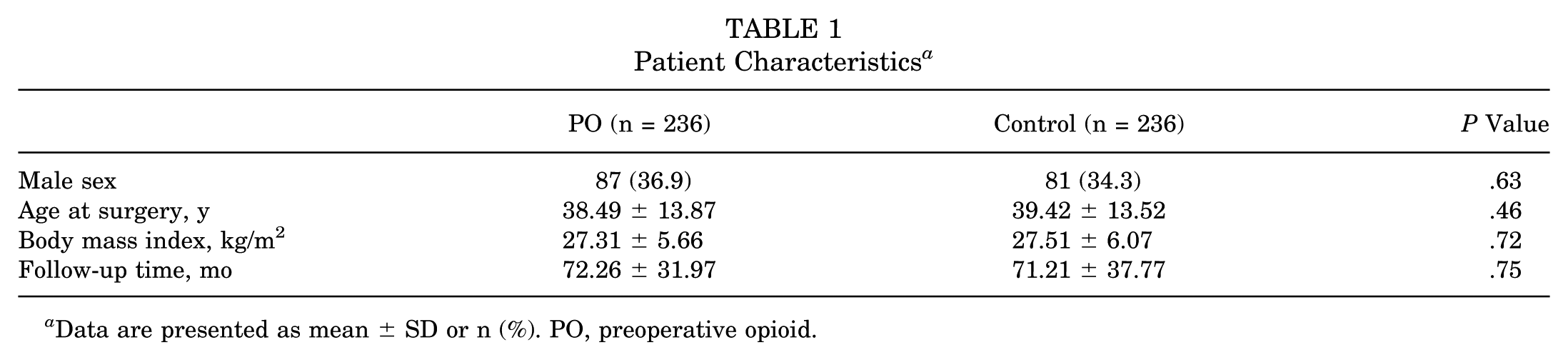
Data are presented as mean ± SD or n (%). PO, preoperative opioid.
Radiographic Findings
In the PO group, 43 patients (18.2%) presented with a preoperative Tonnis grade of 1. The mean LCEA was 31.33°± 6.97°, and the mean alpha angle was 59.45°± 11.87°. Comparatively, in the control group, 31 patients (13.1%) presented with a preoperative Tonnis grade of 1, with a mean LCEA of 30.79°± 6.07° and a mean alpha angle of 61.05°± 11.60° (P > .05).
Intraoperative Findings and Procedures
Intraoperative findings are summarized in Table 2. There were no significant differences in intraoperative findings between the groups (P > .05).
Intraoperative Findings a
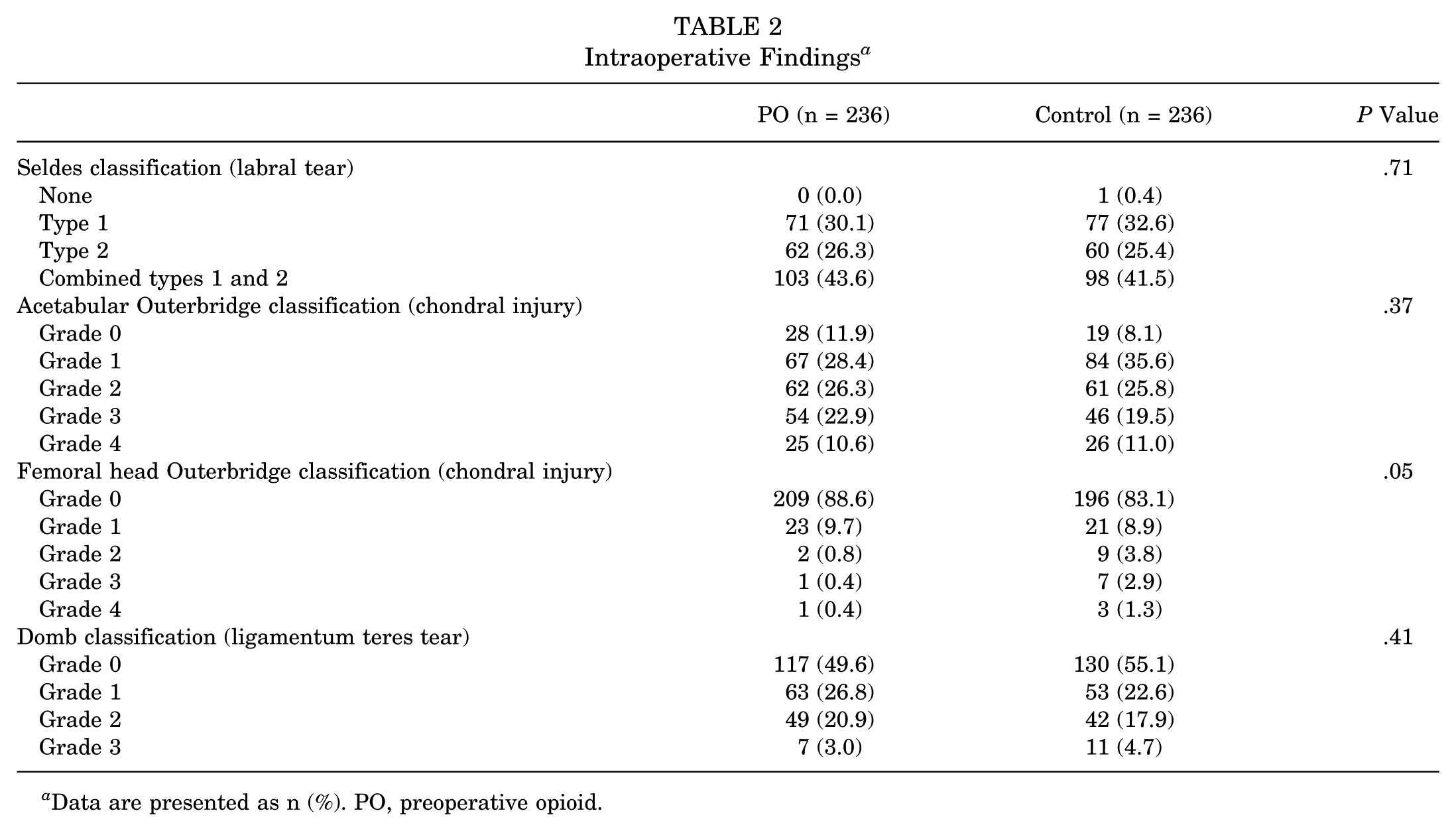
Data are presented as n (%). PO, preoperative opioid.
Intraoperative procedures are summarized in Table 3. No significant differences in intraoperative procedures were observed between the groups (P > .05).
Intraoperative Procedures a
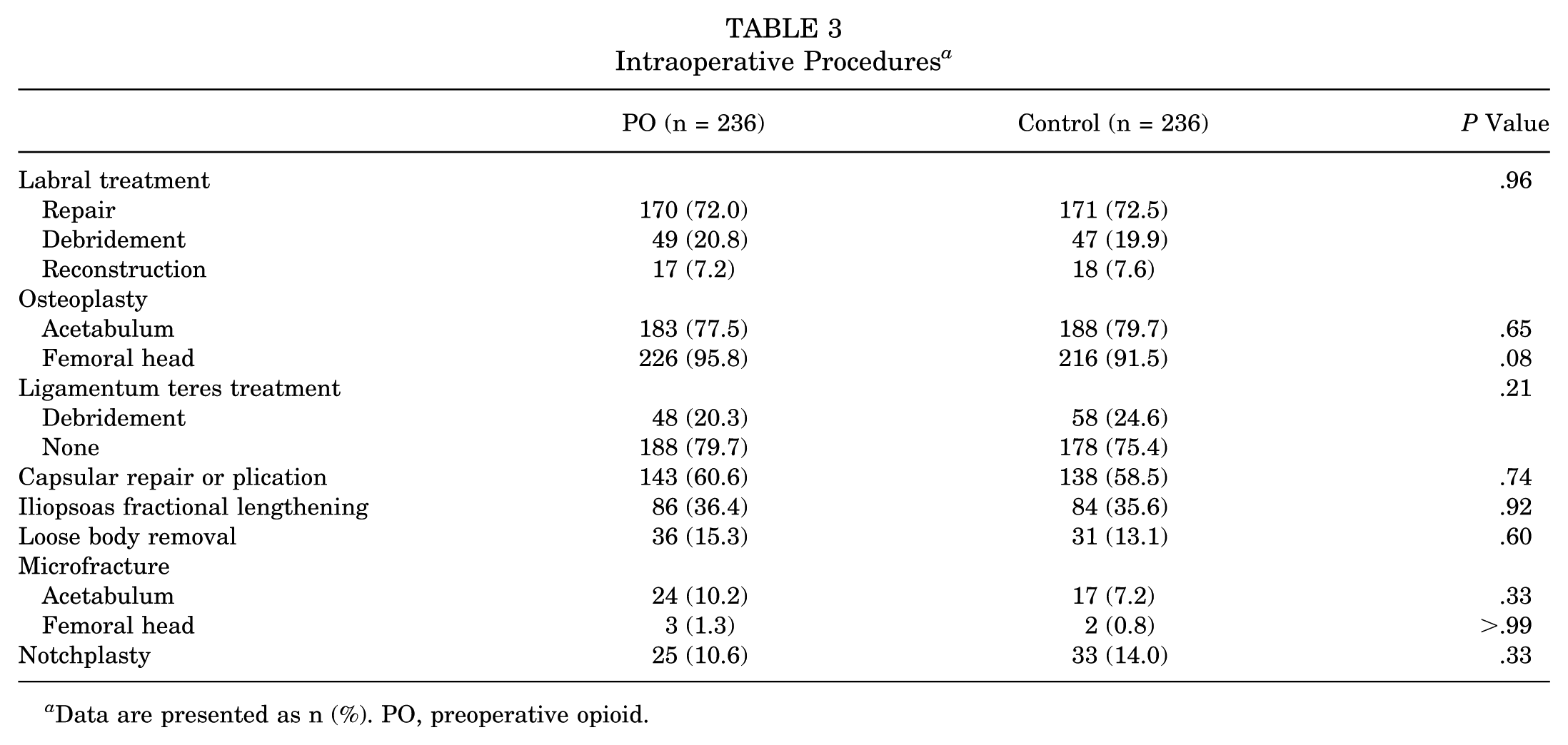
Data are presented as n (%). PO, preoperative opioid.
Patient-Reported Outcomes
PROs are summarized in Table 4. The PO group demonstrated significant improvements on all PRO measures, with a mean patient satisfaction at 2-year follow-up of 6.29 ± 2.55. Compared to the control group, the PO group had lower preoperative scores for the mHHS, NAHS, and HOS-SSS. Additionally, at 3-month follow-up, the PO group exhibited significantly lower scores for the mHHS and HOS-SSS (P < .05). Similarly, at the 1-year mark, the PO group showed lower scores for the mHHS, NAHS, and HOS-SSS (Figure 2).
Patient-Reported Outcomes a
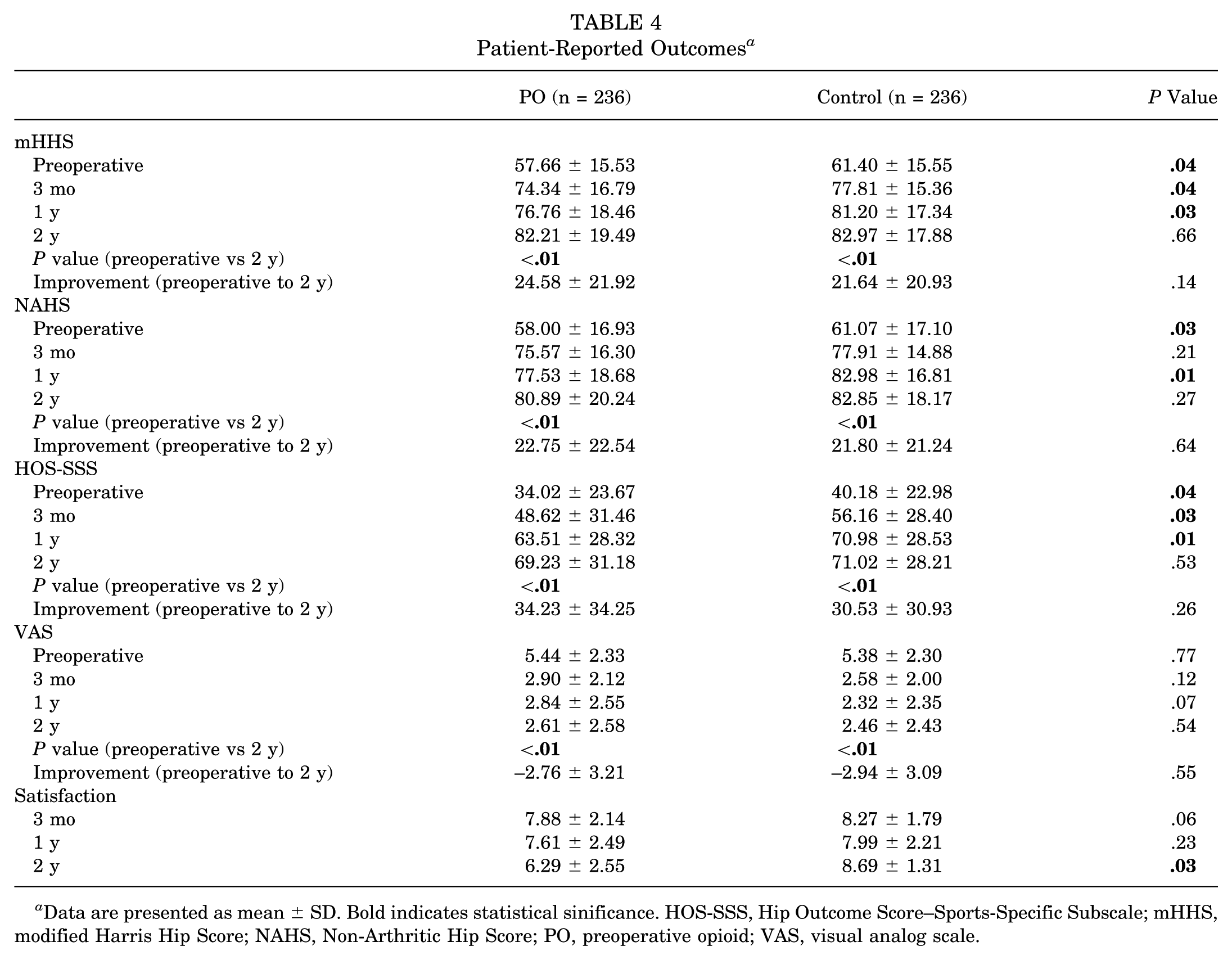
Data are presented as mean ± SD. Bold indicates statistical sinificance. HOS-SSS, Hip Outcome Score–Sports-Specific Subscale; mHHS, modified Harris Hip Score; NAHS, Non-Arthritic Hip Score; PO, preoperative opioid; VAS, visual analog scale.
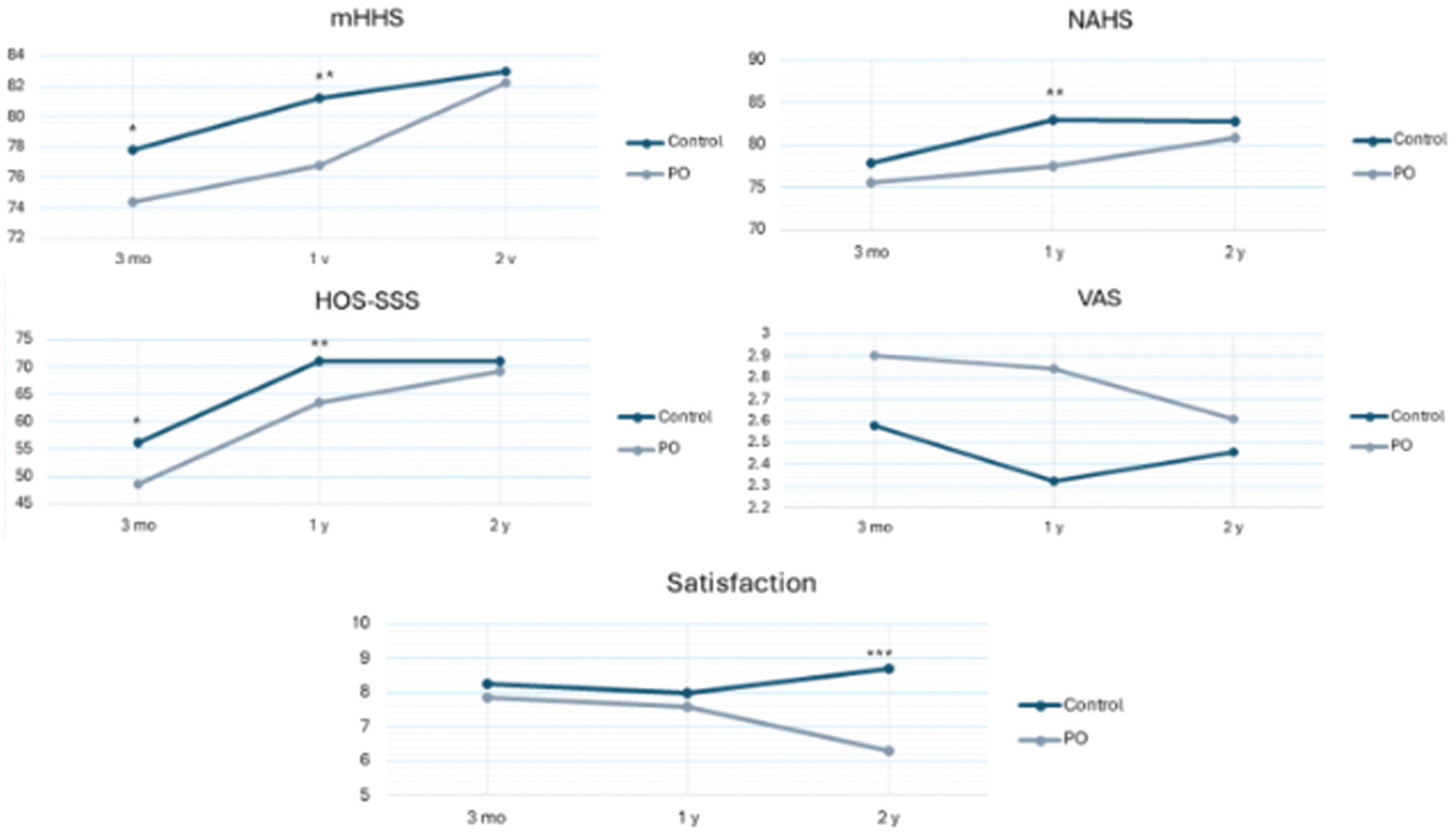
Patient-reported outcomes at 3 months, 1 year, and 2 years. HOS-SSS, Hip Outcome Score–Sports-Specific Subscale; mHHS, modified Harris Hip Score; NAHS, Non-Arthritic Hip Score; PO, preoperative opioid; VAS, visual analog scale. *Statistical significance (P < .05) at 3 months. **Statistical significance (P < .05) at 1 year. ***Statistical significance (P < .05) at 2 years.
Despite these differences, the magnitude of improvement from preoperatively to 2-year follow-up was comparable between groups for the mHHS, NAHS, HOS-SSS, and VAS, ultimately reaching similar postoperative scores. However, the PO group reported significantly lower patient satisfaction at the latest follow-up (P = .03) compared to the control group in which patient satisfaction increased from the 1- to 2-year time points.
Functional Hip Outcome Thresholds
The PO group met the MCID at similar rates for the mHHS, NAHS, VAS and HOS-SSS compared to the control group. Furthermore, both groups met the PASS at similar rates for the mHHS, NAHS, and HOS-SSS. However, the PO group met the PASS for the VAS at a lower rate (P = .03) (Figure 3).
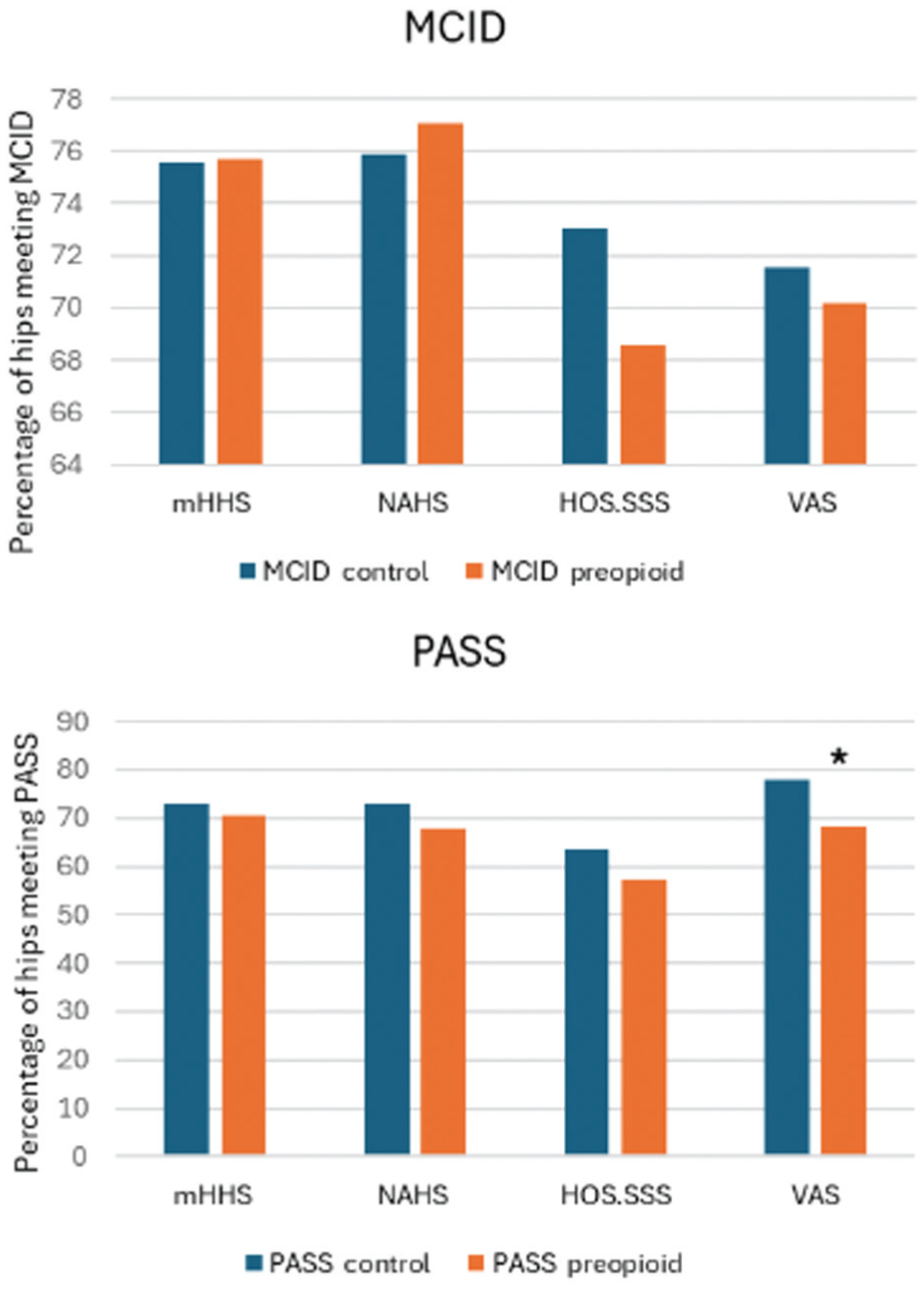
There were no significant differences between the groups in meeting the minimal clinically important difference (MCID) for the modified Harris Hip Score (mHHS), Non-Arthritic Hip Score (NAHS), Hip Outcome Score–Sports-Specific Subscale (HOS-SSS), or visual analog scale (VAS) or in meeting the patient acceptable symptom state (PASS) for the mHHS, NAHS, or HOS-SSS (P > .05). The preoperative opioid (PO) group reached the PASS for the VAS at a lower rate compared to the control group (P = .03).
Secondary Surgery and Complications
The PO group (n = 30 [12.7%]) underwent revision hip arthroscopy at a comparable rate to the control group (n = 23 [9.7%]) (P = .38). All revisions were performed for the recurrence of symptoms after an asymptomatic interval. The time to revision hip arthroscopy was also comparable, with a mean of 26.24 ± 26.75 months for the PO group and a mean of 30.81 ± 27.68 months for the control group (P > .73). Comparable arthroplasty-free survivorship was also noted, with 214 patients (90.7%) not requiring arthroplasty over the study period in the PO group compared to 221 patients (93.6%) in the control group (P > .05). The complication rate between the 2 groups was similar (P > .05). In the PO group, 5 patients (2.1%) experienced a superficial infection. In the control group, 3 patients (1.3%) experienced a superficial infection, and 1 patient (0.4%) experienced heterotopic ossification.
Discussion
The main finding of this study is that patients in the PO group who underwent hip arthroscopy for the treatment of FAI and labral tears demonstrated significant improvements on all evaluated PRO measures at 2-year follow-up. Compared to the control group, the PO group had lower preoperative scores for the mHHS, NAHS, and HOS-SSS and experienced a longer recovery curve, as indicated by lower mHHS and HOS-SSS scores at 3-month follow-up and lower mHHS, HOS-SSS and NAHS scores at the 1-year mark. However, by 2-year follow-up, these differences normalized, with the PO group achieving similar magnitudes of improvement and comparable mean scores for the mHHS, NAHS, HOS-SSS, and VAS. Despite these improvements, the PO group reported significantly lower patient satisfaction, with a mean score of 6.29 compared to 8.69, and reached the PASS for the VAS at a lower rate at the latest follow-up.
Although limited data exist on preoperative opioid-based pain management in hip preservation, evidence from other orthopaedic fields provides insights.1-3 For instance, Lu et al 15 reported on 1242 patients who underwent shoulder arthroscopy, 184 of whom (14.8%) had a preoperative opioid pain management protocol. These patients showed significant improvements from preoperatively to postoperatively but started with significantly lower preoperative scores and achieved significantly lower postoperative outcomes. Similar to our findings, preoperative opioid use negatively impacted patient satisfaction with surgery.
Similarly, in hip arthroscopy, Westermann et al 26 evaluated 321 patients undergoing surgery for FAI to assess the impact of opioid use on preoperative functional scores. The authors included 55 patients (17%) who reported opioid use within 3 months of surgery, 89 patients (28%) had a history of opioid use but not within 3 months of surgery, and 177 patients (55%) reported nonopioid consumption before surgery. 26 Similar to the findings of the current study, the authors observed that patients who used opioids within 3 months reported significantly lower preoperative functional scores, as measured by the Hip Disability and Osteoarthritis Outcome Score pain subscale, University of California, Los Angeles activity score, and Veterans RAND 12-Item Health Survey mental component score, compared to the other 2 groups. 26 Furthermore, Maldonado et al 17 conducted a study involving 34 patients who underwent hip arthroscopy for FAI and labral tears. Patients were divided into 2 groups: opioid-naïve patients and those with a history of preoperative opioid consumption within 6 months of hip arthroscopy. The authors observed that the 17 patients in the preoperative opioid consumption group had lower preoperative scores on the NAHS. 17 Postoperatively, VAS scores were significantly higher at 1 and 6 months, while mHHS scores were significantly lower at the 2-year mark compared to the opioid-naïve group. It is important to note that because of the small sample size, the study was not fully powered to detect differences in PROs.
Our results build on these previous findings. We observed that patients in the PO group started with significantly lower preoperative scores and had a longer recovery process to achieve comparable functional outcomes to a nonopioid consumption group at 2-year follow-up, reaching clinically important thresholds at similar rates. However, despite improving their functional outcomes, patients in the PO group displayed significantly lower patient satisfaction and achieved the PASS for the VAS at a lower rate at the latest follow-up. These findings reinforce the need for careful preoperative counseling regarding opioid use, as it may delay functional recovery and negatively impact patient satisfaction.
To our knowledge, this report is among the first to analyze the impact on functional outcomes of patients with preoperative opioid-based pain management who underwent hip arthroscopy for FAI and labral tears. The propensity score–matched comparison to a control group provides a perspective on the outcomes of this patient population. The sample size surpassed the required number by a priori power analysis, thus minimizing the likelihood of type II errors. The inclusion of validated cohort-specific thresholds for functional hip outcome measures, such as the MCID and PASS, adds a clinical context to the interpretation of mean PROs.
Limitations
This study was not a randomized controlled trial, but the propensity score–matched controlled study design sought to account for confounding variables. Analyses in this study were performed retrospectively. Additionally, because all procedures were conducted at a single institution, the generalizability of the results across institutions is uncertain. Furthermore, self-reported opioid consumption might introduce some selection bias. Some group differences might also exist, as patients taking daily opioids may have higher preoperative pain levels, heightened pain sensitivity, or comorbid mental health conditions. The duration of symptoms and the type of prescribed narcotic were not available for all patients.
Conclusion
Hip arthroscopy for the treatment of FAI and labral tears in patients using daily opioid-based pain control resulted in significant short-term improvements in PROs. Compared to a benchmark control group, patients using opioids preoperatively experienced a delayed functional recovery process but ultimately achieved comparable functional outcomes at 2-year follow-up. Despite these improvements, they reported lower patient satisfaction and met the PASS for the VAS at a lower rate. Preoperative opioid use delayed functional recovery and reduced patient satisfaction, despite comparable 2-year outcomes.
Footnotes
Final revision submitted December 10, 2025; accepted January 4, 2026.
One or more of the authors have declared the following potential conflict of interest or source of funding: R.Q.-J. and A.H.K.-R. have received travel reimbursement from Arthrex, Stryker, and Zimmer Biomet. B.D.K. serves on the editorial board for Arthroscopy and has received hospitality payments from Medical Device Business Services. B.G.D. reports a relationship with Arthrex, Inc. that includes: consulting or advisory, speaking and lecture fees, royalties, research funding, and travel reimbursement; reports a relationship with Smith & Nephew that include: research support; reports a relationship with DJO, LLC that includes: royalties; reports a relationship with Medacta USA, Inc. that includes: royalties and consulting or advisory; reports a relationship with Stryker Corporation that includes: consulting or advisory, research funding, and non-financial support; reports a relationship with Smith+Nephew, Inc. that includes: non-financial support; reports a relationship with Bioventus LLC that includes: non-financial support; reports a relationship with Heraeus Medical, LLC that includes: non-financial support; reports a relationship with Lightbody Medical Technologies Inc that includes: non-financial support; reports a relationship with Oak Med, Inc. that includes: non-financial support; reports a relationship with DePuy Synthes Sales Inc. that includes: non-financial support; reports a relationship with Shalby Advanced Technologies, Inc. that includes: non-financial support; reports a relationship with Medwest Associates that includes: non-financial support and debt forgiveness; reports a relationship with Intellijoint Surgical Inc. that includes: non-financial support; reports a relationship with Medtronic, Inc. that includes: non-financial support; reports a relationship with SI-BONE, Inc. that includes: consulting or advisory and non-financial support; reports a relationship with Xiros Inc. that includes: non-financial support; reports a relationship with Zimmer Biomet Holdings, Inc. that includes: non-financial support; reports a relationship with Electronic Waveform Lab, Inc. that includes: non-financial support; has patent #8920497 with royalties paid from Arthrex; has patent #2612625 with royalties paid from Orthomerica and DJO Global; has patent #RE47811 with royalties paid from Arthrex; has patent #0338177 with royalties paid from Orthomerica. B.G.D. is a Board Member of American Hip Institute Research Foundation, AANA Learning Center Committee, the Journal of Hip Preservation Surgery, the Journal of Arthroscopy, AOSSM Research Committee, ISHA Hip Preservation Society; has had ownership interests in the American Hip Institute and affiliates.
Ethical approval for this study was obtained from American Hip Institute Research Foundation (No. 20242189).