
Abstract
Background:
Vitamin D is essential for bone remodeling, muscle function, and immune regulation. Its deficiency is common among patients undergoing total knee arthroplasty (TKA) and has been linked to delayed recovery, higher complication rates, and an increased risk of periprosthetic joint infections (PJIs). However, the impact of perioperative vitamin D supplementation on TKA outcomes remains unclear.
Purpose:
To evaluate if perioperative vitamin D supplementation would correct hypovitaminosis D; improve early postoperative outcomes, including wound healing, rehabilitation, pain, and fall rates; and reduce the risk of PJIs and revision surgery after TKA.
Study Design:
Systematic review; Level of evidence, 2.
Methods:
Following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, PubMed, Embase, Scopus, and Web of Science were searched for articles published up to July 2025. The inclusion criteria encompassed studies having a vitamin D–supplemented arm in the TKA context, while case reports, editorials, and other study designs were excluded. A total of 562 studies were found initially. Data on correction of vitamin D deficiency, functional and patient-reported outcomes, complications, revisions, and infections were independently extracted. Methodological quality was assessed using the ROBINS-I (Risk of Bias in Non-Randomized Studies of Interventions) and RoB 2 (Cochrane Risk of Bias Tool) tools.
Results:
A total of 11 studies met the inclusion criteria. Among the fragmented evidence, vitamin D supplementation was linked to minimal rehabilitation improvements. It was also associated with lower overall complication and PJI rates but was not significantly associated with changes in pain scores. The considerable heterogeneity in study designs, supplementation protocols, and baseline vitamin D status limited the certainty of findings.
Conclusion:
Our study demonstrated that perioperative vitamin D supplementation may enhance early recovery and lower complication rates after TKA. However, current evidence is inconsistent and insufficient to support universal supplementation. High-quality randomized trials are needed to establish its clinical efficacy and optimal dosing strategies as well as to refine postoperative recovery protocols and infection prevention strategies.
Keywords
Vitamin D status is typically assessed by serum 25-hydroxyvitamin D (25(OH)D), whereas 1,25-dihydroxyvitamin D (1,25(OH)2D or calcitriol) represents the active hormonal metabolite. Calcitriol functions as a key regulatory molecule in musculoskeletal health and function. 25 Vitamin D regulates calcium metabolism through adjustments in intestinal absorption and osteoclast maturation, which is crucial for bone mineralization and remodeling.10,25,52 Furthermore, vitamin D also improves muscle function by enhancing creatine phosphate metabolism and insulin responses.10,18 Vitamin D–deficient biopsies have shown a loss of type II muscle fibers, which could act as fall-preventing fibers; however, this loss was compensated when supplementation was performed.16,59 Vitamin D lowers inflammatory cytokines in neutrophils and suppresses T-cell proliferation. 4
Vitamin D deficiency is considered one of the most common nutritional deficiencies worldwide, affecting approximately 1 in 8 people globally. 28 In a Korean study by Jeon et al, 36 its rate among candidates for total knee arthroplasty (TKA) was 75.0% compared to 59.4% among controls, using a 20-ng/mL cutoff. Deficiency can impair the immune system and has been linked to higher rates of cancer, cardiovascular disease, and several musculoskeletal disorders, such as increased bone loss, osteoporosis, osteomalacia, and muscle weakness.14,33 Vitamin D deficiency is coupled with several autoimmune diseases, including systemic lupus erythematosus, 6 inflammatory bowel disease, 29 and multiple sclerosis. 24 Moreover, vitamin D deficiency is correlated with the pathogenesis of osteoarthritis because of its role in regulating chondrocyte extracellular matrix production. 15 Among orthopaedic procedures, low vitamin D levels are associated with delayed strength recovery after anterior cruciate ligament (ACL) reconstruction (ACLR), 7 fatty degeneration in rotator cuff repair, 49 and a lower Harris Hip Score in THA both preoperatively and postoperatively. 48
A high prevalence of vitamin D deficiency among patients with osteoarthritis who are candidates for total joint arthroplasty (TJA) has been reported in the literature. 19 In addition, several studies have suggested poor functional outcomes,34,35,47,58 postoperative complications,30,55,57,64 and periprosthetic joint infections (PJIs)1,31,41,65 in patients with vitamin D deficiency undergoing TKA. Increased attention toward enhanced recovery after surgery highlights the importance of evidence-based supplementation. Consequently, the optimization of nutritional status, specifically vitamin D, before TJA has gained the attention of orthopaedic surgeons as a possible way to reduce morbidity and mortality related to the surgical procedure.21,38,57
There is ongoing debate regarding the impact of vitamin D supplementation on outcomes after TKA in both the early and late postoperative periods. Key areas of interest include its influence on wound complications, rehabilitation speed, pain scores, and fracture rates in the early phase as well as revision and PJI rates in the late phase. Although several systematic reviews have attempted to clarify the relationship between vitamin D and TKA outcomes, particularly in relation to vitamin D status and preoperative supplementation,13,22,37,45,62,66 no standardized approach has yet been established regarding the efficacy or optimal timing of supplementation. The purpose of this study was to evaluate if perioperative vitamin D supplementation would correct hypovitaminosis D; improve early postoperative outcomes, including wound healing, rehabilitation, pain, and fall rates; and reduce the risk of PJIs and revision surgery after TKA. We hypothesized that vitamin D intake would improve both short- and long-term outcomes after TKA.
Methods
This systematic review adhered to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 2020 statement. To enhance the rigor of this study, we followed the Cochrane Handbook for Systematic Reviews of Interventions (Version 6.5) guidelines. Likewise, this study was registered with PROSPERO (No. CRD420251126160). 56
Search Strategy
For this study, we searched MEDLINE/PubMed, Scopus, Web of Science, and Embase for studies published up to July 2025. A systematic method combining keywords and Medical Subject Headings terms was used to identify relevant studies, encompassing TKA and vitamin D synonyms. The complete database-specific search strategy is provided in Appendix Table A1.
Eligibility Criteria
English- and non–English-language articles comprising cross-sectional, case-control, cohort, and clinical trial studies that evaluated the supplementation of vitamin D in candidates for TKA were considered for inclusion. Likewise, case reports, case series, finite analyses, cadaveric studies, letters, biomechanical studies, cost-effectiveness analyses, and reviews were excluded.
Study Selection and Data Extraction
There were 2 reviewers (A.A.F. and A.A.) who screened the retrieved records independently based on our eligibility criteria. A predefined data extraction spreadsheet (Google Sheets) was developed. The detailed outlines included first author, publication year, country, number of supplemented and nonsupplemented patients, age, follow-up, and assessed outcomes. The same 2 authors (A.A.F. and A.A.) independently extracted the data according to the predefined spreadsheet. In cases of a conflict regarding the extracted data and identified concepts, the reviewers attempted to resolve the issue through a discussion, and if required, a third reviewer (F.V.) mediated an agreement.
Risk-of-Bias Assessment
To evaluate the risk of bias in the included studies, we employed 2 validated tools: RoB 2 (Cochrane Risk of Bias Tool) for randomized controlled trials (RCTs) and Risk of Bias in Non-Randomized Studies of Interventions (ROBINS-I; Version 2) for observational studies. Again, 2 independent reviewers (A.A.F. and A.A.) performed the assessments, with a third reviewer (F.V.) stepping in to resolve any disagreements through a discussion and consensus. Results were visualized via robvis-generated traffic light and summary plots. 44
Data Synthesis
A quantitative meta-analysis was not feasible because of the heterogeneity in outcome definitions, supplementation regimens, and follow-up periods. Instead, we conducted a structured narrative synthesis, grouping results by outcome categories (vitamin D levels, revision and complication rates, objective functional outcomes, and patient-reported outcomes). We first tabulated the data to provide an overview of study characteristics, supplementation methods, and outcomes (Tables 1 and 2). Then, we compared findings within and across these categories to identify similarities and differences. We also factored in the risk of bias when interpreting results, giving more weight to findings from studies rated as having a low risk. Subgroup analyses or sensitivity analyses were not performed because of the limited number of studies in each outcome domain and the variety of supplementation methods.
Characteristics of Included Studies a
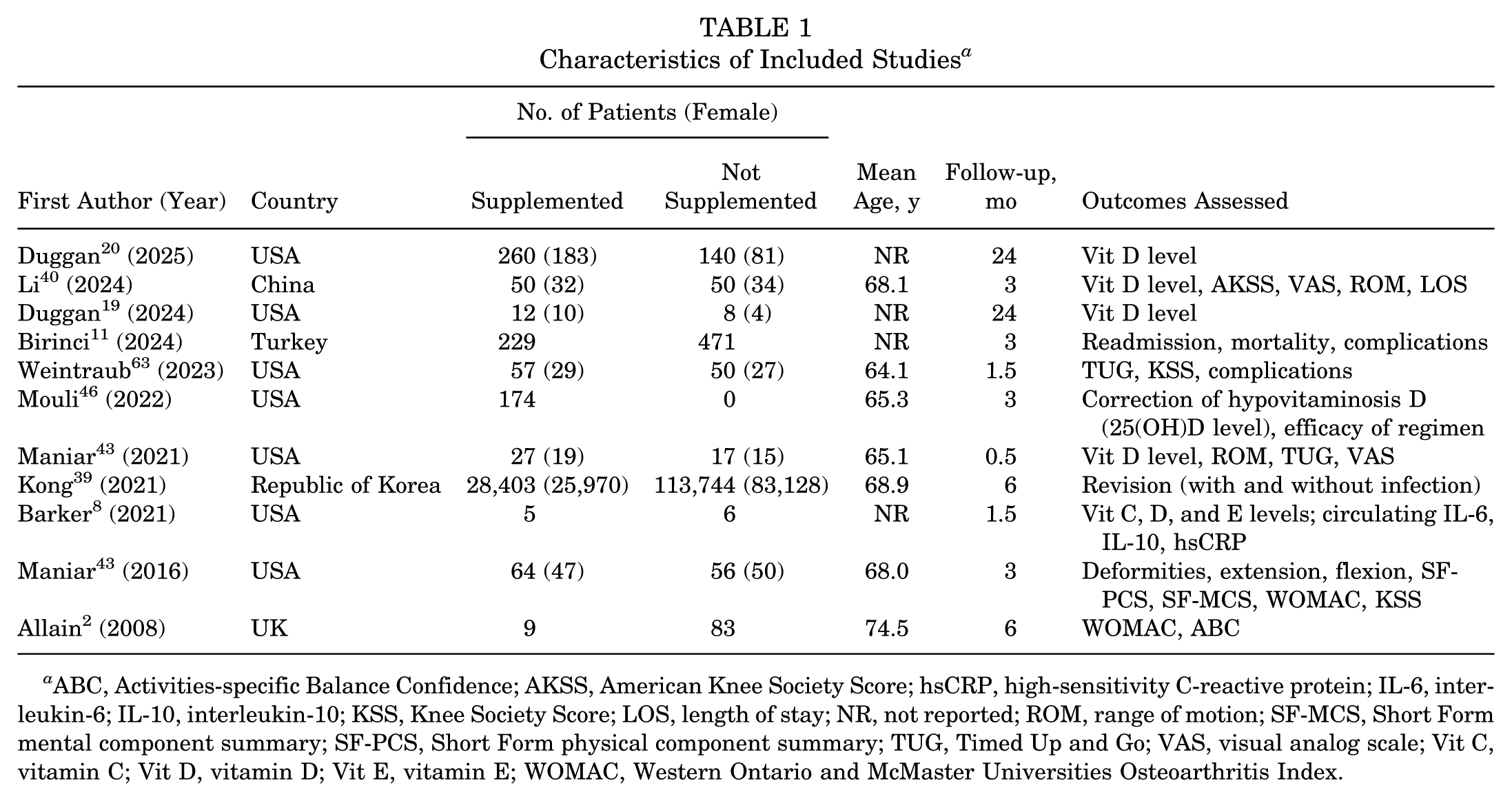
ABC, Activities-specific Balance Confidence; AKSS, American Knee Society Score; hsCRP, high-sensitivity C-reactive protein; IL-6, interleukin-6; IL-10, interleukin-10; KSS, Knee Society Score; LOS, length of stay; NR, not reported; ROM, range of motion; SF-MCS, Short Form mental component summary; SF-PCS, Short Form physical component summary; TUG, Timed Up and Go; VAS, visual analog scale; Vit C, vitamin C; Vit D, vitamin D; Vit E, vitamin E; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Vitamin D Supplementation Methods a

NR, not reported.
Results
In total, 562 studies were found by implementing the search strategy. After duplicate removal and title-abstract screening, 18 studies entered the full-text screening phase. There were 7 articles excluded: 5 studies did not perform vitamin D supplementation, 1 did not encompass TKA specifically, and 1 was considered a cost-effectiveness analysis. Ultimately, 11 studies were included in the current systematic review. This process is summarized in Figure 1.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram for the inclusion of studies.
Study Characteristics
A total of 11 articles were included: 8 were observational studies,2,11,20,39,42,43,46 and 3 were RCTs.8,40,63 In addition, 7 studies were performed in the United States,8,20,42,43,46,63 while China, 40 Turkey, 11 the Republic of Korea, 39 and the United Kingdom 2 each contributed 1 study. A mean age ranging from 64 to 75 years was noted, although 4 studies reported stratified age categories rather than mean values.8,11,20 Follow-up durations varied from 2 weeks in the study by Maniar et al 42 to 24 months in the studies by Duggan et al. 20 Key data from each study are presented in Table 1, while details of the vitamin D supplementation protocols, which varied considerably across studies, are summarized in Table 2.
Risk of Bias
Among the 8 included observational studies, 1 was assessed as having a high risk of bias, 5 had a moderate risk, and 2 were considered low risk. Most studies demonstrated a moderate risk, specifically in the first domain of the ROBINS-I tool. In contrast, the 3 RCTs were rated as having a low risk of bias. The risk of bias for the observational studies is presented in Figure 2, while the risk of bias for the RCTs is shown in Figure 3.
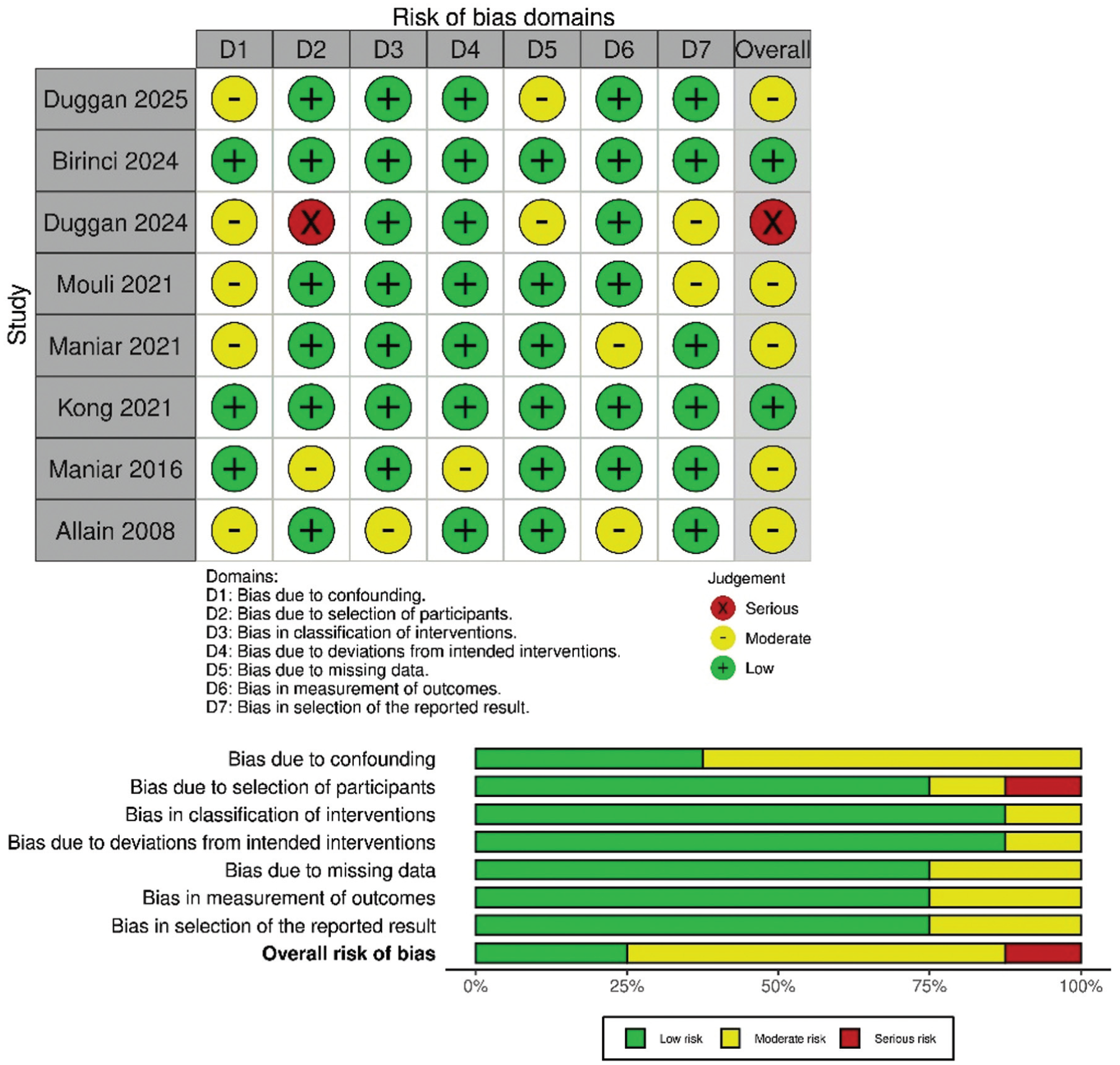
Traffic light plot and summary plot for the risk-of-bias assessment of observational studies.
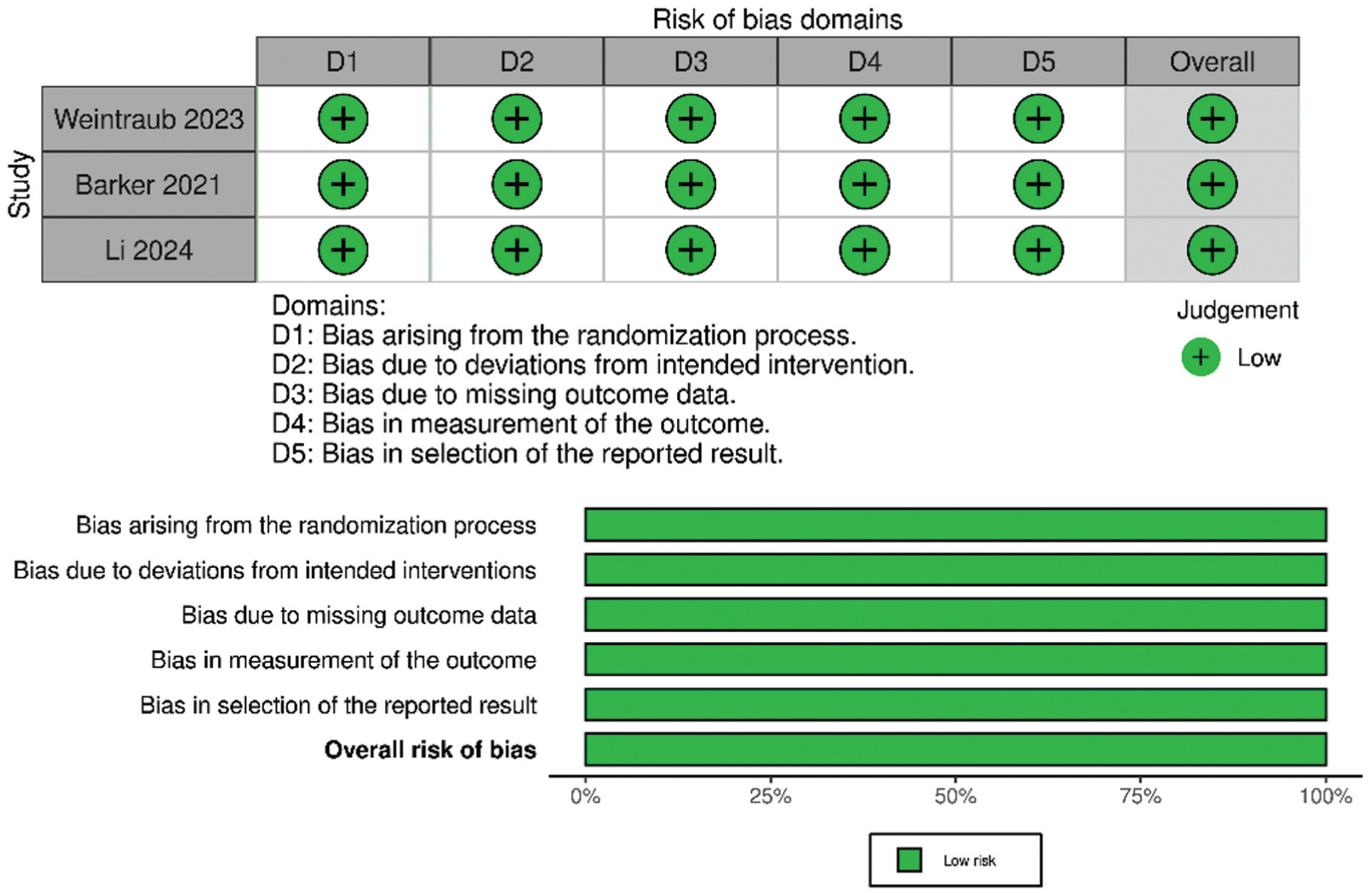
Traffic light plot and summary plot for the risk-of-bias assessment of randomized controlled trials.
Vitamin D Levels
Overall, 5 studies assessed vitamin D levels; supplementation consistently raised serum levels, particularly with oral dosing (Appendix Table A2).20,40,42,46 Maniar et al 42 reported significantly increased vitamin D levels in all supplemented groups at the final postoperative time point (day 14) compared to preoperatively. The highest vitamin D level was observed in the orally supplemented group compared to the intramuscularly supplemented and nonsupplemented groups across all time points (P < .01). Mouli et al 46 retrospectively evaluated preoperative vitamin D levels in 2 groups of supplemented, vitamin D–deficient patients undergoing TKA with different protocols. Levels were significantly higher in the loading-dose supplemented group than the sliding-dose supplemented group at 1 month preoperatively (P < .01).
Revision and Complications
The outcomes regarding complication rates were fragmented but in favor of a beneficial effect of vitamin D. Evidence suggesting decreased rates of revision primarily came from the study by Kong et al 39 involving more than 140,000 patients undergoing TKA. That study compared patients who received calcium and vitamin D supplementation with those who did not. Regular supplementation for >6 months and >12 months was associated with a reduced risk of revision TKA (adjusted hazard ratios [aHRs], 0.56 and 0.65, respectively). Notably, combined calcium and vitamin D use for >1 year was linked with lower rates of revision for PJIs (aHR, 0.63) and noninfectious reasons (aHR, 0.70). Additionally, supplementation for >1 year significantly improved overall implant survival (P < .01). 39
Complications reported by Birinci et al 11 consisted of acute kidney injuries, pneumonia, deep vein thrombosis, acute pulmonary edema, acute myocardial infarction, periprosthetic fractures, dislocations, acute PJIs, superficial wound problems, cellulitis, 90-day readmission, and mortality. Rates of acute pulmonary edema (0.3% vs 1.4%, respectively; P = .04), superficial wound problems (0.2% vs 2.5%, respectively; P < .01), and cellulitis (0.0% vs 2.2%, respectively; P < .01) were significantly lower in the supplemented group than in the nonsupplemented group. Li et al 40 compared cryotherapy alone with combined cryotherapy and vitamin D supplementation and reported deep vein thrombosis as the only postoperative complication, with a statistically nonsignificant difference in favor of the supplemented group (6% vs 4%, respectively; P = .86).
Objective Functional Outcomes
There were 4 studies that evaluated vitamin D supplementation on functional outcomes after TKA, including range of motion and the Timed Up and Go (TUG) test.40,42,43,63 Li et al 40 found that vitamin D supplementation combined with cryotherapy significantly improved range of motion compared with cryotherapy alone at 1 and 3 months postoperatively as well as compared with controls at 3 days, 7 days, 1 month, and 3 months. These outcomes were not reproduced in the observational studies by Maniar et al42,43 in which the authors reported no differences in flexion changes between groups. Li et al 40 used a higher dose than the study by Maniar et al 43 in 2016 but not in 2021. 42 For the TUG test, Maniar et al 42 observed greater postoperative improvements on days 3 and 14 in the supplemented group, whereas the outcomes were not reproduced in the RCT by Weintraub et al 63 at longer follow-up time points of 3 and 6 weeks.
Patient-Reported Outcomes
Overall, 5 included studies evaluated patient-reported outcomes.2,40,42,43,63 Knee function measured by the Knee Society Score was similar between supplemented and control groups in 2 studies.43,63 The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) showed minimal effects: Allain et al 2 reported greater improvements on the stiffness subscale at 6 months but no other changes, while Maniar et al 43 observed no differences at 3 months. Li et al 40 found improved American Knee Society Score values at 1 and 3 months in the supplemented group. Other patient-reported outcome measures, including the Short Form Health Survey physical component summary and the Activities-specific Balance Confidence scale, showed no significant changes.2,43 Pain outcomes, assessed by the visual analog scale and WOMAC pain subscale, were not significantly influenced by supplementation in any of the 3 studies that evaluated them.2,40,42
Discussion
The principal finding of this systematic review is the absence of consistent, high-certainty evidence supporting a clinically meaningful benefit of vitamin D supplementation on outcomes after TKA; however, when interpreted cautiously, vitamin D supplementation may positively influence various outcomes after TKA both in the early and late postoperative periods.
In the early postoperative period, Birinci et al 11 reported a significant reduction in wound complication and cellulitis rates. Vitamin D's role in modulating the immune system, with benefits for macrophages and dendritic cells, may account for these results.9,32 However, patients undergoing TKA experiencing higher rates of superficial wound issues and cellulitis may possibly be caused by thinner subcutaneous tissue, differences in tension between wound edges during flexion and extension, and skin dryness. 11 Also, the clinical translation of immunomodulation mechanisms into reproducible reductions in early complications after TKA remains uncertain because the rates of several other short-term complications did not change with vitamin D supplementation, such as acute myocardial infarction, periprosthetic fractures, and dislocations. 11
When discussing patient-reported outcomes, Maniar et al 43 and Allain et al 2 found no significant effect on outcome scores. Notably, Maniar et al 42 and Weintraub et al 63 observed improved and unimproved TUG test results in the supplemented groups, respectively. Data regarding the impact of vitamin D supplementation on the incidence of falls or early periprosthetic fractures were even more limited. While such evidence is incomplete in these contexts, several pathways have been proposed through which vitamin D may enhance musculoskeletal health. In addition to bone health, calcitriol plays a role in muscle fiber formation, morphology, and physiology. Vitamin D–deficient biopsies have shown a loss of type II muscle fibers, which could act as fall-preventing fibers.16,59 This loss was compensated when supplementation was performed. 5 Moreover, the modulatory effects of vitamin D in the immunological context are considered a mediator for less autoimmune and atrophic diseases. 53 Vitamin D also regulates calcium-related metabolism. Within the activity of fibers, cytosolic calcium activates calcium/calmodulin-dependent protein kinase signaling and up-regulates myocyte enhancer factors 2A and 2D, which improve glucose uptake and may have beneficial effects. 25 With a more orthopaedic perspective, in the ACLR context, Qiu et al 54 reported a significant positive correlation between vitamin D levels and neuromuscular function of the quadriceps in both injured and noninjured limbs in a cross-sectional study. However, in an earlier prospective cohort study of candidates for ACLR by Gupta et al, 26 no functional improvement was observed in the long term between various vitamin D levels. The preventive role of vitamin D in muscle loss was also confirmed in a study by Tomlinson et al. 61 Inconsistent functional outcomes may stem from varying supplementation and co-supplementation protocols as well as from techniques used to evaluate muscle function, such as questionnaires or tests.26,42,53,61,63
Evidence regarding long-term outcomes after TKA is limited. A large retrospective study by Kong et al, 39 including 142,147 patients, reported a significant reduction in revision TKA (aHR, 0.65). That study further analyzed the cause of revision procedures, revealing that regular vitamin D and calcium supplementation for >12 months was associated with decreased rates of revision for both PJIs (aHR, 0.63; P = .03) and aseptic issues (aHR, 0.70; P = .008), while acute PJI rates did not differ between the groups in the study by Birinci et al, 11 although with a smaller sample size. To examine vitamin D's immunomodulatory effects and its possible links with PJIs, it should be highlighted that vitamin D enhances innate and adaptive immunity. 17 Cathelicidins and defensins, 2 vitamin D–responsive antimicrobial peptides, may partially explain the role of vitamin D in enhancing innate immune defenses against PJIs, 17 particularly in relation to staphylococci, 12 the most commonly implicated pathogens. 23 Adaptive immunity may also be modified through dendritic cells and T-cell differentiation against PJIs.16,59 These insights align with an earlier study by Maier et al 41 in which an association was reported between low vitamin D levels and PJIs. While the immunomodulating effects of vitamin D may account for the septic side of this outcome, future studies may better explain the possible link between vitamin D supplementation and aseptic revision via a muscle-mediated mechanism, as summarized in the former paragraph.
In other orthopaedic/sports medicine fields, there are limited data regarding vitamin D supplementation. Haines et al 27 reported that the union rate was not associated with vitamin D supplementation after traumatic fractures, while Patel et al 51 recommended up to 4000-IU supplementation with calcium after stress fractures. Moreover, Bae et al 5 showed that vitamin D deficiency may be associated with a nearly 2-year earlier diagnosis of osteoporosis after ACLR. Pasquini et al 50 also suggested that hypovitaminosis D is associated with a higher risk of ACL injuries and delayed muscle recovery after ACLR. However, evidence regarding functional outcomes after ACLR, such as return to sport, was not consistent and conclusive based on their systematic review. 50
Within previously performed systematic reviews examining both vitamin D and TJA,13,22,37,45,62,66 3 did not evaluate the effects of vitamin D supplementation on TJA outcomes but reported the effect of hypovitaminosis D with relatively few included articles.13,22,66 In 2020, Kenanidis et al 37 reported the effects of preoperative vitamin D levels on TJA outcomes, suggesting that supplementation may alter postoperative vitamin D levels. Vivek et al 62 also conducted a systematic review, encompassing 10 articles, to elucidate the general association between vitamin D and TKA. However, a risk-of-bias assessment was not performed, and 2 articles evaluating vitamin D supplementation were included. 62 Finally, the study closest to the current study was a rapid systematic review, performed by Morrison et al 45 in 2022, which included 3 articles to evaluate the effects of vitamin D supplementation on TJA outcomes.
From a clinical standpoint, current evidence does not support routine vitamin D supplementation for all patients undergoing TKA. Although supplementation is inexpensive and generally safe, the lack of consistent benefits across outcomes and the predominance of low-certainty evidence preclude firm recommendations. Notably, no current orthopaedic society guidelines mandate routine vitamin D screening or supplementation before TJA, highlighting an area for potential clinical standardization and future research. High-level evidence supporting routine vitamin D supplementation for all candidates for TKA, irrespective of baseline status, remains limited. A cost-effectiveness analysis by Arshi et al 3 revealed that both selective (screening-based) and universal supplementation strategies can be cost-effective, given the potential reduction in PJIs and associated health care costs; however, selective supplementation proved more efficient. Designing a population-specific protocol requires the careful consideration of multiple factors, including the prevalence and severity of vitamin D insufficiency, ethnic and geographic differences in sun exposure, age, comorbidities, socioeconomic determinants, and overall cost-effectiveness.3,11,60
This review has limitations. Only 3 included studies were RCTs, while the remaining observational studies were carried with inadequate adjustments for confounding variables. Moreover, outcome reporting and supplementation protocols were highly heterogeneous. Future research should focus on large, multicenter randomized trials with standardized vitamin D dosing, consistent baseline measurements, strict adherence to supplementation protocols, and careful adjustments for confounding factors to better clarify the role of vitamin D supplementation in TKA outcomes.
Conclusion
Our study demonstrated that perioperative vitamin D supplementation may enhance early recovery and lower complication rates after TKA. However, current evidence is inconsistent and insufficient to support universal supplementation. High-quality randomized trials are needed to establish its clinical efficacy and optimal dosing strategies as well as to refine postoperative recovery protocols and infection prevention strategies.
Footnotes
Appendix
Serum Vitamin D Levels a

| First Author (Year) | Group | Preoperative | POD 1 | POD 3 | POD 7 | POD 14 | 1 mo | 3 mo | 6 mo | 1 y | 2 y |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Maniar 42 (2021) | Nonsupplemented | 48.3 ± 11.6 | NA | 40.4 ± 10.7 | NA | 38.9 ± 8.9 | NA | NA | NA | NA | NA |
| Intramuscularly supplemented | 21.5 ± 7.7 | NA | 31.2 ± 24.9 | NA | 38.9 ± 21.5 | NA | NA | NA | NA | NA | |
| Orally supplemented | 20.2 ± 6.6 | NA | 69.9 ± 16.4 | NA | 68.5 ± 17.9 | NA | NA | NA | NA | NA | |
| Duggan 19 (2024) | Supplemented | 45.33 ± 31.27 | NA | NA | NA | NA | 46.00 ± 12.73 | 28.33 ± 10.21 | 47.33 ± 14.98 | 25.67 ± 11.76 | 40.22 ± 19.43 |
| Nonsupplemented | 38.33 ± 12.70 | NA | NA | NA | NA | 12.00 | 22.00 ± 9.90 | NA | 43.00 ± 17.49 | 36.94 ± 9.16 | |
| Duggan 20 (2025) | Supplemented | 38.21 ± 14.75 | NA | NA | NA | NA | 36.11 ± 12.74 | 40.19 ± 16.36 | 44.93 ± 17.95 | 41.35 ± 14.54 | 38.89 ± 14.50 |
| Nonsupplemented | 37.21 ± 12.11 | NA | NA | NA | NA | 33.50 ± 14.66 | 37.14 ± 8.42 | 36.85 ± 14.26 | 36.77 ± 12.23 | 39.25 ± 13.31 | |
| Li 40 (2024) | Supplemented + cryotherapy | 55.22 ± 9.14 | 45.90 ± 8.06 | NA | 42.88 ± 7.11 | NA | 61.34 ± 6.86 | 84.20 ± 5.44 | NA | NA | NA |
| Nonsupplemented | 53.10 ± 7.32 | 43.90 ± 8.06 | NA | 40.22 ± 6.85 | NA | 44.56 ± 7.53 | 45.52 ± 6.69 | NA | NA | NA | |
| Nonsupplemented + cryotherapy | 53.66 ± 8.03 | 44.10 ± 7.47 | NA | 40.18 ± 6.82 | NA | 44.30 ± 7.20 | 45.14 ± 6.93 | NA | NA | NA | |
| Mouli 46 (2022) | Sliding dose supplemented | 3 mo preoperatively: 22.25 ± 5.16 1 mo preoperatively: 30.03 ± 10.85 |
NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Loading dose supplemented | 3 mo preoperatively: 23.23 ± 4.32 1 mo preoperatively: 35.00 ± 8.39 |
NA | NA | NA | NA | NA | NA | NA | NA | NA |
Data are shown as mean ± SD. NA, not applicable; POD, postoperative day.
Final revision submitted January 24, 2026; accepted February 15, 2026.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.