
Abstract
Background:
Chronic anterior shoulder instability affects young, athletic patients linked to activities involving external rotation (ER) and abduction. Some intrinsic patient characteristics may influence clinical presentation and bony lesions.
Purpose:
To analyze the association between sex, hyperlaxity, and number of dislocations in a cohort of patients with chronic anterior instability.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Between January 2022 and January 2025, patients >15 years of age with chronic anterior shoulder instability who had not been operated on were included in a cohort. Clinical data evaluated included age, sex, hyperlaxity (combined ER and internal rotation [IR] hyperlaxity), and subjective assessment of the shoulder. Regarding the number of dislocations, 4 groups were formed in this cohort: subluxation (ie, partial loss of contact between the humeral head and the glenoid, n = 10), 1 dislocation (ie, complete loss of contact between the humeral head and the glenoid, n = 20), 2 to 3 dislocations (n = 36), and >3 dislocations (n = 34). Bony lesions were assessed by radiographs and computed tomography scan using a semiautomatic method for humeral bone loss (HBL; size, volume, and location) and glenoid bone loss (GBL; percentage of bone loss).
Results:
In this cohort of 100 patients, 86% of patients had GBL and 83% had HBL. Although there were fewer women (n = 25) in the cohort than men (n = 75) (P = .01), women more frequently exhibited multidirectional (ER + IR) hyperlaxity (56% for women vs 36% for men; P = .04), narrower glenoid cavities (23.5 vs 26 mm; P < .001) and less GBL (10% for women vs 13% for men; P = .04). Hyperlax patients (n = 41) had smaller bipolar bone lesions than nonhyperlax patients (n = 59): GBL (8% vs 12%; P = .02), Hill-Sachs lesion length (26.7 ± 6.6 mm vs 30.4 ± 9.4 mm; P = .03), Hill-Sachs width (13.0 ± 4.2 mm vs 16.5 ± 5.5 mm; P = .045), and Hill-Sachs volume (2924 ± 2177 vs 5023 ± 4396 mm3; P = .04). In the >3 dislocations group, HBL was larger (length: 32 mm, P = .045; width: 17 mm, P < .001), with a greater volume (5409 mm3; P = .008), deeper (2.4 mm; P = .01), and with a specific location close to 12 o'clock in 3-dimensional analysis.
Conclusion:
This predominantly male cohort with chronic anterior instability demonstrated that women had narrower glenoid cavities and smaller glenoid bony lesions than men and were more often hyperlax than men. Hyperlax patients, regardless of sex, had smaller bipolar bony lesions, while the number of dislocations increased the size and severity of the HBL. Studies with larger patient samples are needed to confirm these results.
Chronic anterior shoulder instability is a common condition that often affects young, athletic patients. 16 Contact sports often carry a risk of chronic anterior shoulder instability.1,10,26,29 It would be interesting to know whether sex, hyperlaxity, and the number of dislocations are responsible for differences in clinical presentation. These are intrinsic characteristics of the patient that cannot be modified. Regarding sex, the literature has put forward hypotheses of differences in clinical presentation between women and men.2,9,14,20,21,23,28 Chronic anterior shoulder instability may present differently between the 2 sexes because men and women do not have the same muscle mass, hormones (relaxin), or sporting habits,5-8 but also have different bone and soft tissue lesion characteristics.2,20,28 However, from a strictly physiopathological point of view, there is no reason why the clinical presentation should differ between men and women. External rotation (ER) hyperlaxity of the shoulder with the elbow at the side and generalized joint hypermobility are associated with chronic anterior shoulder instability. 4 However, shoulder hyperlaxity is not associated with first episode of dislocation. One question that may arise is whether the clinical presentation and, above all, bone loss are comparable between hyperlax and nonhyperlax patients. The same question can also be asked in relation to the number of dislocations and subluxations and the effect this has on bipolar bony lesions. It appears that dislocations cause more humeral bone lesions than subluxations with a similar clinical presentation. The question is whether there are specific clinical presentations and bipolar bony lesions depending on sex, hyperlaxity, and number of dislocations. The aim of this study was to analyze the effect of sex, hyperlaxity, and number of dislocations in a cohort of patients with chronic anterior instability who had undergone a computed tomography (CT) scan.
Methods
Study Design
A retrospective and comparative observational, single-center study was conducted at the Toulouse University Hospital between January 2022 and January 2025. The inclusion criteria were patients (1) aged >15 years 18 with (2) ≥1 episode of anterior shoulder dislocation or (3) subluxation with (4) no history of surgical bony procedures on the humerus or glenoid and with (5) a CT scan without injection. Exclusion criteria were patients who had already been operated on for osteosynthesis, infections, posterior instability, voluntary dislocation, and chronic dislocation, as well as shoulder dislocation with chronic rotator cuff lesion. Patients who had undergone preoperative arthro-CT scan and/or magnetic resonance imaging were also excluded because segmentation using software cannot be performed with this type of examination. Patients were informed about the use of their clinical data and CT scan. They gave their consent after receiving clear, honest, and appropriate information. Clinical and radiological data were collected and analyzed by a single fellowship-trained surgeon.
Population
From January 2022 to January 2025, we analyzed the medical records of 359 patients with shoulder instability (Figure 1). After excluding 259 patients, the analysis was performed on 100 patients.
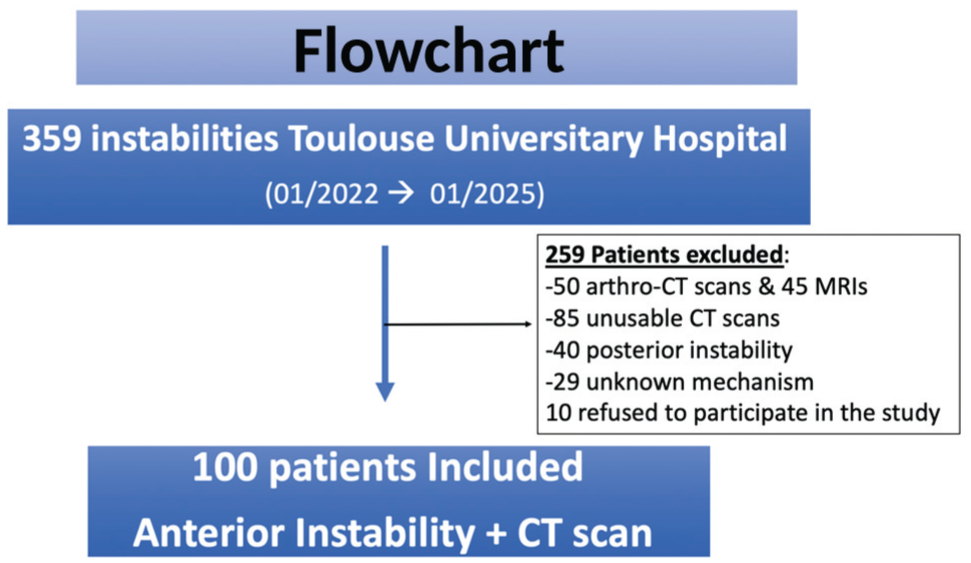
Flowchart of patient inclusion in the study. CT, computed tomography; MRI, magnetic resonance imaging.
Clinical Evaluation
For each patient, the following clinical criteria were evaluated: age, sex, and dominant side. The number of dislocations (complete loss of contact between the humeral head and the glenoid cavity of the scapula with reduction by external maneuver by another person) and subluxations (partial loss of contact between the humeral head and the glenoid cavity of the scapula with spontaneous reduction) were assessed. 18 Anterior hyperlaxity was defined as ER of the shoulder, elbow at side, >85°. 38 Multidirectional hyperlaxity, which corresponds to hyperlaxity in internal rotation (IR) and external rotation, was defined as a combination of shoulder hyperlaxity with the elbow at the side as defined by Walch, plus internal hyper-rotation >T8. 19 The practice of a sport, the type of sport, and the level of practice were also assessed (leisure, competition, and professional) in association with the Instability Severity Index Score (ISIS) 1 score. A subjective assessment of the shoulder was also carried out using the Subjective Shoulder Value (SSV) and SSV Sport scores.6,11 Any surgery and the type of surgery were recorded. The number of dislocations was divided into 4 groups: 0 dislocations with subluxation (n = 10), 1 dislocation (n = 20), 2 to 3 dislocations (n = 36), and >3 dislocations (n = 34). Regarding age, 3 groups of patients were formed: <20 years of age (n = 32), between 20 and 30 years of age (n = 34), and >30 years of age (n = 34).
Radiographic Assessment of Bipolar Bone Lesions
First, a radiographic analysis was performed. The assessment of glenoid bone lesions was performed on a 3-rotation (ER, IR, and neutral rotation), anteroposterior and lateral radiographs. The assessment of Hill-Sachs lesions in the posterosuperior part of the humerus, which corresponds to humeral bone loss (HBL), was also analyzed on anteroposterior radiograph with ER. The Bernageau view was often difficult to perform due to patient apprehension and therefore was not used for assessment.
CT Scan Evaluation of Bipolar Bone Lesions: Glenoid Bone Loss (GBL)
For the CT scan assessment of bony lesions, a manual analysis was performed by a single observer (H.B.), quantifying bone loss on a frontal view using the Sugaya circle method 37 and a report on bone loss according to Hailong et al. 13 The right shoulder scapulae were analyzed and reoriented using 3-Matic Medical software (Version 15.0; Materialise). An adjustment was also performed at the exact point of bone loss and at the “healthy” points at 3 o'clock and 9 o'clock (Figure 2).

Assessment of glenoid bone loss. 3D, 3-dimensional. The colors on the glenoid allow depth to be highlighted using color coding: red for the most superficial edges of the glenoid. On the gray glenoid, the yellow anterior inferior part of the glenoid symbolizes simulated glenoid bone loss.
CT Scan Evaluation of Bipolar Bone Lesions: HBL
Regarding the assessment of HBL known as a Hill-Sachs lesion, the radiographic image was first analyzed for screening purposes. The Hill-Sachs lesion was then assessed on an axial slice of CT scan. The classification initially used was that developed by surgeons, based on the Calandra classification modified and adapted to axial CT scans 3 : stage 0: no lesion, the head is spherical; stage 1: minimal cartilage lesion with loss of sphericity; stage 2: subchondral lesion with true notch; and stage 3: large lesion. We then used a 3-dimensional method known as the clock method to locate the posterosuperior lesion of the humerus (Figure 3). The width and length of the humeral bone lesion were characterized using the Ozaki method. 27 The depth of the lesion was calculated automatically using computer software (3-matic; Materialise), as was the volume.

(A) Measurement of the length and width of a Hill-Sachs lesion. (B) The 3-dimensional clock method is used to measure the radial angle of the lesion with its starting point (red dot at red arrow) and its end point (red dot below). The maximal depth of the lesion are also measured (double blue arrow). The starting angle (green line) between the 12 o'clock and 6 o'clock line (green arrow) and the starting point (red arrow) is measured.
Statistical Analysis
Numerical variables were expressed as mean ± SD and discrete results as absolute and relative frequencies (%). We created 2 groups based on sex and hyperlaxity values, 3 groups based on age of patients, and 4 groups based on the number of dislocations. The comparability of the groups was assessed by comparing the basic demographic data. The normality and heteroscedasticity of continuous data were assessed using the Shapiro-Wilk and Levene tests, respectively. For comparisons between ≥3 groups, an analysis of variance was performed followed by a t test with adjustment for multiple pairwise comparisons if there was a difference between groups. Discrete results were compared using the chi-square test or Fisher exact test, as appropriate. The alpha risk was set at 5%, and 2-tailed tests were used. Statistical analysis was performed using EasyMedStat software (Version 3.42; www.easymedstat.com).
Results
Epidemiological Data
The clinical characteristics of the patients in the cohort were summarized in Table 1. This was a young (mean ± SD age, 29 ± 15 years) and active population, with all patients (N = 100) reporting previous apprehension in the abduction ER position. Most patients (90%) played a sport, with more than a third competing and/or playing at a professional level. Rugby was played by 20% of patients in this series. The mean ISIS score was >4. The group aged <20 years old participated in more competitive sports (60% vs 34% and 15%; P < .001) with no other significant differences between groups.
Epidemiological Data a

Data are presented as n or mean ± SD, unless otherwise indicated. ER, external rotation; ISIS, Instability Severity Index Score; SSV, Subjective Shoulder Value.
Radiological Results
There was a difference between the number of patients with GBL found on radiograph versus CT scan (55% vs 86%, respectively; P = .01) and between the number of patients with HBL found on radiograph versus CT (30% vs 84%; P < .001) (Table 2). CT scans identified, among this cohort, bipolar bone lesions with the following frequencies: 86% of glenoid bony lesions and 83% of humeral bony lesions.
Humeral and Glenoid Bone Loss a

Data are presented as n or mean ± SD, unless otherwise indicated. CT, computed tomography.
Sex Differences
The population in our cohort was predominantly male (25 women vs 75 men; P = .01) (Table 3). ER hyperlaxity and multidirectional hyperlaxity were more common in women (56% vs 36%, P = .04; 16% vs 4%; P = .045, respectively). The SSV and SSV Sport scores were lower in women than in men. Women had a smaller glenoid than men (23.50 ± 2.36 mm vs 26.00 ± 2.38 mm; P < .001). The amount of GBL was lower in women than in men (10.00% ± 8.15% in women vs 13.00% ± 7.78% in men; P = .04).
Comparison of Characteristics by Sex a

Data are presented as mean ± SD or n (%). The P-values in bold indicate statistically significant values p < 0.05. ER, external rotation; IR, internal rotation; ISIS, Instability Severity Index Score; SSV, Subjective Shoulder Value.
ER Hyperlaxity
Two groups were established in this cohort based on hyperlaxity: hyperlax (n = 41) and nonhyperlax (n = 59) (P = .07) patients (Table 4). GBL was lower in the hyperlax group (8% vs 12%; P = .02) than in the nonhyperlax group. The length, width, and volume of HBL were lower in the hyperlax group compared with the nonhyperlax group, respectively (26.6 vs 30.43 mm, P = .03; 13.00 vs 16.48 mm, P = .045; 2924 vs 5023 mm3, P = .04).
Comparison of Patients With Hyperlaxity and Without Hyperlaxity

Data are presented as mean ± SD or n (%). The P-values in bold indicate statistically significant values p < 0.05. ISIS, Instability Severity Index Score; SSV, Subjective Shoulder Value.
See Figure 3 for time locations.
Number of Dislocations
On the humeral side, the Hill-Sachs lesion was longer and wider in the group with the most dislocations (31.7 and 17.3 mm, respectively; P = .045 and P < .001). The volume of the Hill-Sachs lesion was greater in the group with >3 dislocations (5409 mm3; P = .008), as was the maximal depth of the lesion (2.39 mm; P = .01). The radial angle of the clock was greater in the group with >3 dislocations (P = .03). In the >3 dislocations group, the upper limit of the lesion was closest to 12 o'clock (27.4°; P = .04) (Table 5).
Comparison of Characteristics According to Number of Subluxations or Dislocations a

Data are presented as mean ± SD. The P-values in bold indicate statistically significant values p < 0.05. HS, Hill-Sachs lesion.
Discussion
Chronic anterior shoulder instability mainly affects young athletes who participate in contact sports and/or arm wrestling. It appears that certain intrinsic characteristics of the patient may alter clinical presentation. Regarding bipolar bony lesions in this cohort of 100 patients, 86% of patients had a glenoid lesion and 83% of patients had a humeral bone lesion. Few studies have analyzed the association between sex, hyperlaxity, number of dislocations, and clinical and CT scan characteristics of patients with anterior instability. Our series included one-quarter female and three-quarters male. Female patients had a smaller glenoid with less GBL compared with male patients. Women were more frequently hyperlax than men and had a lower subjective assessment of their shoulder before treatment than their male counterparts. The number of hyperlax and nonhyperlax patients in the series was comparable, with less severe bipolar bony lesions in the hyperlax patients. In this series, the number of dislocations was associated with humeral lesions that were larger in size and volume and located closer to the 12 o'clock position in 3D. It can be assumed that the more a patient dislocated one's shoulder anteriorly, the more significant the humeral bone lesions were, with a specific location.
The cohort population was young, athletic, and predominantly male, which is comparable with other cohorts in the literature. 20 This characteristic may be due to the location of our center, as contact and collision sports seem to be practiced mainly by men. However, more women are playing rugby in our regions, which would contradict older epidemiological studies. The study by Patzkowski et al 28 on a population of young female athletes found that playing rugby, a contact sport, was the leading cause of traumatic instability. In 1989, Krøner et al 17 found that male patients with a history of dislocation had a mean age of between 20 and 30, while women dislocated their shoulders on average between the ages of 60 and 80, probably due to rotator cuff injuries. The mechanism and pathophysiology were therefore different between men and women. Sports practices have evolved over the past 30 years. There is no physiological reason that can explain the difference in dislocation rates between women and men or the age at which they occur. 5 However, given the intrinsic characteristics, the clinical presentation and lesions may differ depending on sex.2,9,14,20,21,23,28,30 The sample sizes of some studies in the literature are unbalanced, which is also the case in our study. Studies on dislocation rates in men and women in a population of rugby players or students found no difference between the 2 sexes.10,29 In the same sport, there should therefore be no difference between women and men. Although the sample sizes are different in our series, it appears that ER hyperlaxity and multidirectional hyperlaxity are more prevalent in female than in male patients.19,38 These results were in line with the literature, as Borsa et al 2 and McFarland et al 21 demonstrated that women were less stiff and more hyperlax in the anterior part of the glenohumeral joint. This result also seems to be consistent with the studies by Remvig et al, 32 which reported greater ligament laxity in women. One of the physiological hypotheses, which has been particularly studied in anterior cruciate ligament ruptures, is the presence of higher levels of relaxin in women than in men.5,8 However, this theory has yet to be confirmed.
Our series also showed that women seem to be more affected by chronic anterior shoulder instability in their daily lives, whether in sports or in general, with lower SSV and SSV Sport scores. This point has never been addressed or found in the literature. Magnuson et al 20 demonstrated in a large cohort that women had lower scores (eg, American Shoulder and Elbow Surgeons, Western Ontario Shoulder Instability Index, and Single Assessment Numeric Evaluation) with no difference in the number of dislocations. It would be interesting to confirm this effect on daily life and sports participation by conducting further studies evaluating this effect. It remains to be seen whether, after treatment, the subjective assessment of women's shoulders will be as satisfactory as that of men.
In terms of bone anatomy, women in our series have a smaller glenoid on average than men. However, bone loss appears to be lower in women than in men (10% in women vs 13% in men), even when considering the smaller size of the glenoid. Once again, this showed that the clinical presentation differs depending on sex.2,9,14,20,21,23,28 The shape of the glenoid in women has been described as more oval compared with the glenoid in men, which is more round according to Merill. 22 We did not specifically analyze the shape of the glenoid between the 2 groups, but the analysis of the size of the glenoid cavity in our series seems to agree with this study. In their series with few bone lesions (21% of patients with GBL and 53% with HBL), Hettrich et al 14 found that men had more bipolar bony lesions, as in our series and other studies in the literature, while women had more capsular laxity.2,20 However, the number of episodes and the age at which dislocations occur appear to be the main factors influencing glenoid bone injuries. 23 In female patients, it is essential to thoroughly evaluate the soft tissues before surgery, as bone injuries are significantly less common and mainly occur on the humeral side. 28 Soft tissue injuries, in female patients, can be bipolar: labral on the glenoid side, and ligamentous on the humeral side. Humeral avulsion of the glenohumeral ligament lesions account for up to 25% of cases in some series. 28
Two groups were formed in this cohort: hyperlax (n = 41) and nonhyperlax (n = 59), with no statistically significant difference between the groups. It is important not to confuse multidirectional hyperlaxity with multidirectional instability (MDI), which are 2 different concepts. Multidirectional instability is defined by anterior and posterior instability plus increased inferior translation and was not addressed in this study. 28 Although disputed, MDI characterizes a pathological clinical effect of a shoulder dislocating in 2 directions. 28 The 2 groups were comparable in terms of age, sports practice, and number of episodes of dislocation and/or subluxation. As seen previously, bone loss in the glenoid was smaller in size in the hyperlax group than in the nonhyperlax group. Sahu and Shah, 34 in their comparative series of Latarjet procedures in 2 groups of hyperlax and nonhyperlax patients, also found less bone loss in the glenoid side in the hyperlax group. GBL assessment is essential but must be combined with HBL assessment and clinical criteria such as hyperlaxity. In adolescents, Rosello et al 33 showed that the number of preoperative dislocations (>3) and hyperlaxity were criteria that contraindicated anatomic Bankart repair because of the very high recurrence rate. Analysis of HBL between hyperlax and nonhyperlax patients showed similar bone loss localization in both groups. However, the length, width, and volume of HBL was lower in the hyperlax group compared with the nonhyperlax group. These data seem to show that hyperlaxity should be analyzed precisely in the context of chronic anterior shoulder instability with bone loss rates that need to be adjusted. For example, the concepts of “critical or subcritical” GBL (13.5% bone loss at the glenoid) should probably be adapted in hyperlax patients.7,12,31,33,35
Regarding the number of dislocations, there were 4 groups of patients in this cohort: subluxations (n = 10 patients), 1 episode of dislocation (n = 20 patients), 2 to 3 episodes of dislocation (n = 36 patients), and >3 episodes of dislocation (n = 34 patients). The diameter of the humerus and the width of the glenoid cavity before injury did not differ between patients with subluxations, 1 dislocation, 2 to 3 dislocations, or >3 dislocations. On the humeral side, the Hill-Sachs lesion was longer and wider in the group with the highest number of dislocations. The volume of the Hill-Sachs lesion was greater in the group with >3 dislocations. In the group with >3 dislocations, the start of the lesion was closest to 12 hours. On the glenoid side, the lesions did not differ according to the number of dislocations. There was also no difference in off-track or peripheral track lesions. 15 In chronic anterior shoulder instability, Hill-Sachs lesions appear to be most common during the first episode of shoulder dislocation. 24 During subsequent episodes, glenoid bone lesions worsen and become more common than humeral bone lesions, which was not found in our series. 25 In fact, the number of dislocations was not correlated with more severe glenoid bone lesions, which may be due to the limited sample size of our study. However, no correlation between the size of the humeral and glenoid bone lesions has been found in the literature, which is also the case in our series.24,25,27,36
Limitations
This study has several limitations: it is a retrospective, single-center study with a small number of patients. Other data were studied but with unbalanced groups, such as sex. Furthermore, we did not take patient size into account when weighting the results for glenoid sizes. Then, radiological analysis was performed by a single fellowship-trained surgeon without multiobserver analysis. As mentioned above, the assessment of the shoulder in daily life and during sports was performed using a subjective score without an objective score.
Conclusion
This predominantly male cohort with chronic anterior instability demonstrated that women had narrower glenoid cavities and smaller glenoid bony lesions than men and were more often hyperlax than men. Hyperlax patients, regardless of sex, had smaller bipolar bony lesions, while the number of dislocations increased the size and severity of the HBL. Studies with larger patient samples are needed to confirm these results.
Footnotes
Final revision submitted February 21, 2026; accepted February 27, 2026.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from CHU Toulouse (RnIPH 2021-021).