
Abstract
Background:
Humeral retrotorsion (HRT) has been linked to several throwing-related adaptations in baseball athletes, including glenohumeral range of motion, posterior capsule extensibility, throwing velocity, and injury risk. Studies have shown that rotational strength deficits can be linked to risk of injury, yet no studies have addressed the effect of side-to-side differences in HRT (relative HRT [rHRT]) and its relationship to rotational strength profiles.
Purpose/Hypothesis:
The purpose of this study was to determine the relationship between rHRT and shoulder strength measures. It was hypothesized that there would be a significant association between shoulder external rotation (ER) and internal rotation (IR) strength and rHRT in a cohort of uninjured collegiate baseball athletes.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 182 uninjured male collegiate baseball athletes participated in this study. Bilateral isometric rotational shoulder strength was measured for each participant utilizing a handheld dynamometer, while diagnostic ultrasound was used to measure humeral torsion. Multiple hierarchal regression was conducted to determine whether rHRT significantly contributed to measures of shoulder strength; additionally, subanalyses were conducted to determine if playing position or limb dominance significantly contributed to model fit.
Results:
Relative HRT did not significantly contribute to prediction models for dominant limb ER, nondominant limb ER, and nondominant limb IR strength (P > .05). Relative HRT significantly improved the model for dominant limb IR strength (P = .018) but was not a significant independent predictor. The additions of playing position (P = .037) and limb dominance (P = .032) also significantly improved regression models, but only for dominant limb IR strength.
Conclusion:
Relative HRT is associated with dominant limb IR strength. Additionally, effects of playing position (pitcher) and limb dominance (left-handed) independently and positively contributed to these strength prediction models, demonstrating an association between shoulder IR strength and rHRT, playing position, and limb dominance.
Humeral torsion, or the relative rotational difference between the orientation of the proximal humeral head and the epicondylar axis at the distal humerus, has garnered attention in the assessment of baseball athletes.19,27,42 Anatomic humeral retrotorsion (HRT) describes the morphological change at the humeral head typically observed in the throwing limb, in which the orientation is shifted in a posterior-medial direction and is associated with changes in transverse plane rotation. 27 This de-rotation process results in a relative posterior rotation compared to the nonthrowing limb and occurs most rapidly up to the age of 8 years and ceases to change once physis have closed. 32 Anatomic HRT has been described to increase with increasing age and baseball participation,32,37 with well-established normative values previously published. 31
The side-to-side difference in humeral torsion, or relative HRT (rHRT), has been referenced at a range of 10° to 20° when accounting for the difference between the dominant and nondominant limbs. 55 The larger side-to-side difference between limbs suggests a greater adaptive change to the dominant arm from the normal, theoretically unaffected, nondominant limb. 66 Combined with evidence that both greater dominant limb HRT and greater nondominant limb humeral torsion (ie, the genetic contribution) have been linked to throwing-related injury,46,66 understanding the effects this nonmodifiable risk factor has on other modifiable musculoskeletal risk factors is a clinical necessity.
It has been shown that when glenohumeral range of motion is interpreted within the context of rHRT, there is an observed shift in the total arc of motion, with a noted increase in external rotation (ER) and decrease in internal rotation (IR) on the throwing arm.13,18,20,53,55,56 A relationship between increased dominant limb HRT and posterior capsule extensibility has also been established.9,49,50,62 While not directly associated, increased anatomic HRT may indirectly affect throwing velocity through its relationship with ER gain, as increased shoulder ER has been positively correlated with pitching velocity.10,23,33,54 Cumulatively, these observations are notable, as alterations in total arc of motion, posterior capsule extensibility, and increased throwing velocity have each been independently linked to injury risk.6,8,10,33,45,51
These clinical objective measures related to HRT and rHRT should be screened for when attempting to elucidate injury risk profiles, as anatomic HRT is nonmodifiable. However, given that relationships have been shown between anatomic HRT (or rHRT) and other modifiable risk factors, further investigations are warranted to continue to understand the relationship between osseous adaptation and modifiable measures. Currently, there is a gap in the present literature to indicate if rHRT affects rotational shoulder strength profiles in baseball athletes. In theory, the relative displacement of the humeral head on the throwing limb may affect muscle strength and force production through alterations in the optimal length-tension relationships of shoulder musculature. Shoulder strength and its relation to injury risk development have been measured across all levels of baseball, and studies have delineated rotational strength deficits as a potential modifiable risk factor for injury.63,65 To date, no studies have addressed the relationship between rHRT, or the side-to-side difference in anatomic HRT, and its relationship to rotational strength profiles. As shoulder strength deficits have been postulated as an injury risk factor in overhead throwing athletes,25,39,65 a study investigating the association of rHRT on shoulder strength profiles is warranted to further explain the relationship between these rotational strength measures and osseous adaptations in overhead throwing athletes. Therefore, the purpose of this study was to identify whether relationships exist between shoulder rotational strength measures and rHRT. We hypothesized that rHRT would significantly contribute to a prediction model for bilateral shoulder ER and IR strength in a cohort of uninjured baseball athletes. Additionally, we sought to determine if playing position (pitcher vs position player) and limb dominance (right-handed vs left-handed) would contribute to these models. We hypothesized that playing position and limb dominance would significantly improve regression models for shoulder ER and IR strength. Given the exploratory nature of this work, we generated the primary and secondary hypotheses without perceived directionality.
Methods
Study Design
The protocol for this study was approved by our institutional review board through the University of Texas Health Science Center and Memorial Hermann Hospital System (HSC-MM-22-0537). Data for this study were retrospectively collected from the records of uninjured baseball players within a prospective registry established to monitor the musculoskeletal health of overhead athletes. Prospective data collection started in January 2022 and is currently ongoing; data utilized in this study were analyzed in May 2025. All data utilized for this study were taken at a spring preseason measurement before the commencement of the competitive season. All data were collected and stored in REDCap (Research Electronic Data Capture).29,30 Informed consent was provided by all participants before study enrollment.
Study Participants
Participants were considered eligible for this study if they were a currently uninjured collegiate baseball player (1) between 18 and 24 years of age, (2) with no history of elbow or shoulder surgery within the previous year, (3) with no current elbow or shoulder injury or pain that was limiting or restricting participation in all baseball activities at the time of testing, and (4) participating in baseball at the National Collegiate Athletic Association (NCAA) Division I, II, or III level. Participants were excluded from the study if they were experiencing an active, ongoing injury. No data regarding prior injury status and timing of prior injuries were available for this study. The study staff confirmed participant eligibility status at the time of enrollment. All data utilized for this study were collected at a spring preseason measurement before the commencement of the competitive season.
Clinical Evaluation
Participant characteristics, measures of shoulder ER and IR strength, bilateral humeral torsion, and Kerlan-Jobe Orthopaedic Clinic (KJOC) scores were collected during the initial evaluation. Objective measures of ER strength, IR strength, and HRT were obtained by 2 examiners (N.L.M. and S.M.K.). The examiners were not blinded to the throwing arm or the measured values for HRT in this study. Before data collection, the reliability for each measure was established. Intraclass correlation coefficients with 95% confidence intervals and standard error of measurement were calculated for the objective measures of ER strength, IR strength, and HRT and were found to be excellent for both intra- and interrater reliability for all measures (Table 1).
Intra- and Interrater Reliability for Clinical Measures a

ER, external rotation; HRT, humeral torsion; ICC, intraclass correlation coefficient; IR, internal rotation; SEM, standard error of measurement.
Data are presented as range for intrarater reliability values.
Isometric Strength Testing
Isometric shoulder ER and IR strength testing was performed using a handheld dynamometer (HHD) (MicroFET 2; Hogan Scientific LLC) by 2 examiners (N.L.M. and S.M.K.). A make test methodology was performed similar to previous work utilizing isometric strength testing. 7 Each participant was positioned at the edge of a treatment table. The arm of the participant was positioned at 90° of elbow flexion with neutral rotation about the shoulder with a towel roll positioned between the trunk and elbow of the participant at the medial epicondyle (Figure 1). The participant was given verbal instructions to perform scapular stabilization and to remain in an upright posture with a neutral spine position to avoid excessive thoracic kyphosis. The primary examiner positioned the HHD approximately 2 cm proximal to the styloid process on the dorsal (ER strength) or ventral (IR strength) aspect forearm. 17 The participant was then instructed to push the HHD into either ER or IR, exerting maximal effort over a 5-second period while maintaining proper testing position and avoiding compensatory motions. Tactile cueing at the lateral aspect of the elbow was given to further avoid compensations, and a member of the study staff observed all testing procedures to ensure no compensations were noted. The peak force in pounds was recorded for 2 trials on both arms. The data in pounds were then converted to newtons utilizing the following formula: strength measure (lb) × 4.4482216153. The mean of the recorded values was then used for the final analysis. A third trial was performed if there was a discrepancy >5 lb between the first 2 trials; in these instances, the mean of the closest 2 trials was utilized for analysis.

Isometric shoulder (A) external and (B) internal rotation strength testing.
Humeral Torsion
Humeral torsion was assessed utilizing an indirect ultrasonographic technique described and validated by previous researchers.20,46,52 Each participant was placed supine on a treatment table in a hook-lying position. Ultrasound gel (Cardinal Health) was placed on a straight ML16-15 probe connected to a Venue Go R3 (GE HealthCare) ultrasound machine. Examiner 1 placed the participant's shoulder at 90° of abduction with the elbow at 90° of flexion and positioned the probe over the anterior aspect of the participant's glenohumeral joint. A rolled towel was placed under the participant's humerus to maintain a neutral position of the scapula in the coronal plane. The probe was then aligned perpendicular to the long axis of the humerus in the front plane. With the probe level (verified by a bubble level placed at the face of the probe), examiner 1 rotated the humerus until the deepest part of the bicipital groove was visualized and the apexes of the greater and lesser tuberosities were parallel to the horizontal plane (Figure 2). Examiner 2 then placed a digital inclinometer (Baseline Evaluation Instruments) just below the shaft of the ulna and recorded the degrees of inclination. The digital inclinometer was zeroed to the vertical plane before the measurement was obtained. The measurement from the digital inclinometer was recorded as the degrees of inclination observed from an anatomic reference 0° to the vertical plane. The mean of 2 values was used for data analysis, and a third was performed if there was a wide discrepancy (>3°) between the first 2 measurements; the closer of 2 trials in these instances was utilized for analysis. Relative HRT was utilized in the final analysis and was calculated using the following formula: dominant limb torsion – nondominant limb torsion. For clarity, when measuring humeral torsion, values with a positive denotation represent humeral torsion, while negative values represent true HRT; interpretationally, when considering the side-to-side difference in humeral torsion, or rHRT, a negative number represents a smaller degree of humeral torsion of the throwing limb compared to the nonthrowing limb.
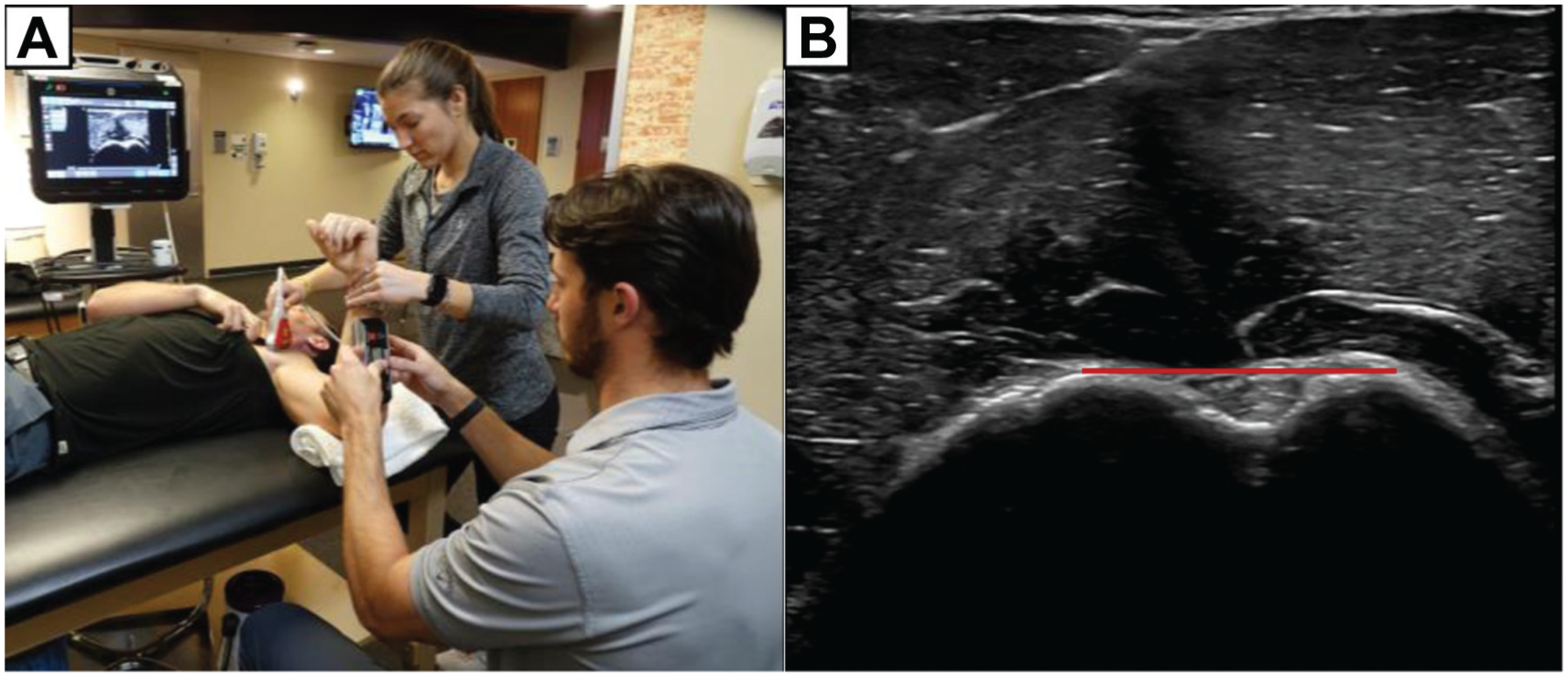
(A) Measurement of humeral retrotorsion using a linear ultrasound probe placed over the anterior shoulder. (B) Visualization of the deepest portion of the bicipital groove while the lesser and greater tubercle remain parallel (red line).
KJOC Score
After objective testing, participants completed the KJOC questionnaire. The following verbal instructions were provided in a standardized script by one member of the study staff: “The following questions concern your physical functioning during game and practice conditions. Unless otherwise specified, all questions relate to the function of your shoulder and/or elbow at the present time. For each question, please indicate your self-perceived current level of function by placing an ‘x’ along the line” (0-10 scale). The KJOC score is a numeric score representing self-reported function of the shoulder and elbow specifically designed and validated for overhead populations, with a score of 100 representing excellent self-perceived shoulder and elbow health. 2 A range of scores across varying levels of play have been reported in the literature to discriminate between healthy and injured populations24,41 and are commonly used to subjectively measure self-reported throwing arm function in overhead throwing athletes.
Statistical Analysis
A priori power analysis was performed using G*Power Version 3.1 (G*Power, Franz Faul, Universität Kiel, Germany) with power set at 0.80 (1 –b) and an alpha level of .05. A conservative small effect size (f2 = 0.06) was utilized. A total of 125 participants were required in this study to identify statistically significant interactions between one predictor variable (rHRT), 3 control variables (age, height, and weight), and shoulder strength.
For descriptive characteristics and clinical and self-reported clinical measures, continuous data are expressed as means and standard deviations, while ordinal data are presented as counts. To test the hypothesis of this study, 4 separate hierarchal multiple regressions using an entry method were conducted to assess the relationship between rHRT and bilateral shoulder ER and IR strength. Age, height, and weight were entered in the first block for each regression together to first determine the effects of potential confounding variables on the model fit. For each regression, rHRT was entered in a second block to independently determine if the addition of this variable significantly improved the model. Dominant limb ER and IR strength and nondominant limb ER and IR strength were entered as the dependent variable in the second block of each regression. Assumption testing, including assessments of linearity and normality, multicollinearity, homoscedasticity, and normality of residuals, was conducted before analyses for all continuous independent and dependent variables included in the analyses. The assumption of normality was confirmed using the Shapiro-Wilk test; dominant limb HRT and rHRT violated the assumption of normality (P < .05). As the Shapiro-Wilk test can be sensitive to even minor deviations in a distribution, the decision was made to move forward without changes, particularly as the central limit theorem suggests that in larger samples (≥30 participants) the sampling distribution tends to be normal, regardless of the shape of the data. 22 All other assumptions were met.
Subanalyses were performed using similar statistical methods to determine changes in model significance by including playing position (pitchers and position players) and limb dominance (right-handed and left-handed athletes). The same statistical methods were used to determine whether each entry significantly improved the prediction model and estimations of variance were explained; these were conducted by again regressing confounding variables of age, height, and weight in model 1, rHRT in model 2, and either position or limb dominance in model 3, respectively. Playing position was transformed into dummy codes, where a value of 0 represented pitchers and a value of 1 represented position players; similarly, limb dominance was transformed where a value of 0 represented right-handed throwers and a value of 1 represented left-handed throwers. These models were regressed on the 4 dependent variables of bilateral rotational strength to determine if and to what extent these variables improved the model. All data were analyzed using statistical package SPSS Version 29 (IBM). An alpha level of P < .05 was considered significant for all statistical analyses.
Results
A total of 182 male collegiate baseball athletes met inclusion criteria for this study (Figure 3).

CONSORT (Consolidated Standards of Reporting Trials) flow diagram of participant inclusion.
Athletes included were pitchers (50.0%) and position players, with a majority of the athletes (78.6%) participating at the NCAA Division I level. Participant baseline characteristics are presented in Table 2.
Participant Baseline Characteristics a

Data are presented as n or mean ± SD. KJOC, Kerlan-Jobe Orthopaedic Clinic; NCAA, National Collegiate Athletic Association.
Dominant and nondominant limb anatomic HRT, rHRT, and shoulder rotational strength measures are presented in Table 3.
Objective Measures a

Data are presented as mean ± SD. ER, external rotation; HRT, humeral retrotorsion; IR, internal rotation.
Relationship Between rHRT and Dominant Limb ER Strength
The primary analyses used a 2-step hierarchal approach, introducing age, height, and weight in the first model (to address potential confounding variables), followed by rHRT in the second model, to determine if this addition significantly improved the model. The first model did not significantly explain dominant limb ER strength (R2 = .028; adjusted R2 = .011; F[3,178] = 1.684; P = .172). The addition of rHRT in the second model did not significantly improve the model (R2 = .030; adjusted R2 = .008; F[1,177] = 1.384; P = .241). Body weight emerged as a significant predictor in model 1 (β = .192; P = .030) and model 2 (β = .195; P =.028)
Relationship Between rHRT and Dominant Limb IR Strength
The first model significantly explained dominant limb IR strength (R2 = .046; adjusted R2 = .030; F[3,178] = 2.865; P = .039). No significant predictors emerged in this model (P > .05). The addition of rHRT in the second model significantly improved the model (R2 = .065; adjusted R2 = .044; F[1,177] = 3.061; P = .018). Height emerged as a significant predictor in this model (β = .175; P =.039); while the addition of rHRT improved the model, it was not a significant predictor in model 2 (β = .139; P =.061).
Relationship Between rHRT and Nondominant Limb ER Strength
The first model did not significantly explain nondominant limb ER strength (R2 = .030; adjusted R2 = .013; F[3,178] = 1.819; P = .145). The addition of rHRT in the second model did not significantly improve the model (R2 = .037; adjusted R2 = .016; F[1,177] = 1.722; P = .147). No individual predictors emerged as significant predictors (P > .05).
Relationship Between rHRT and Nondominant Limb IR Strength
The first model did not significantly explain nondominant limb IR strength (R2 = .020; adjusted R2 = .004; F[3,178] = 1.225; P = .302). The addition of rHRT in the second model did not significantly improve the model (R2 = .030; adjusted R2 = .008; F[1,177] = 1.377; P = .244). No individual predictors emerged as significant predictors (P > .05).
Pitchers Versus Position Players
The subanalyses used a 3-step hierarchal approach, introducing age, height, and weight in the first model, followed by rHRT in the second model, and lastly, either playing position or limb dominance into the third model to determine if these additions significantly improved the model. For dominant limb ER strength, the addition of playing position in the third model did not significantly improve the overall model (R2 = .031; adjusted R2 = .003; F[1,176] = 1.113; P = .355). Body weight remained a significant predictor in this model (β = .193; p =.031). For dominant limb IR strength, the addition of playing position in the third model significantly improved the overall model (R2 = .065; adjusted R2 = .038; F[1,176] = 2.435; P = .037); however, no significant predictors emerged from this model. The addition of playing position indicated that a primary position of pitcher significantly and positively improves predicted dominant limb IR strength. For nondominant limb ER strength, the addition of playing position in the third model did not significantly improve the overall model (R2 = .041; adjusted R2 = .013; F[1,176] = 1.493; P = .194); body weight emerged as a significant predictor in model 3 (β = .178; P =.045). For nondominant limb IR strength, the addition of playing position in the third model did not significantly improve the overall model (R2 = .031; adjusted R2 = .003; F[1,176] = 1.110; P = .357); no significant predictors emerged from this model.
Right-Handed Versus Left-Handed Players
For dominant limb ER strength, the addition of limb dominance in the third model did not significantly improve the overall model (R2 = .033; adjusted R2 = .011; F[1,176] = 1.220; P = .302). Body weight remained a significant predictor in this model (β = .196; P =.028). For dominant limb IR strength, the addition of limb dominance in the third model significantly improved the overall model (R2 = .066; adjusted R2 = .040; F[1,176] = 2.500; P = .032); height remained as a significant predictor in this model (β = .176; P = .039). The addition of limb dominance indicates that left-handedness significantly and positively improved predicted dominant limb IR strength. For nondominant limb ER strength, the addition of limb dominance in the third model did not significantly improve the overall model (R2 = .038; adjusted R2 = .011; F[1,176] = 1.406; P = .224); no significant predictors were included in the final model. Lastly, for nondominant limb IR strength, the addition of limb dominance in the third model did not significantly improve the overall model (R2 = .040; adjusted R2 = .013; F[1,176] = 1.461; P = .205); no significant predictors emerged from this model. Table 4 demonstrates the regression coefficients for the final model for each strength measure.
Regression Coefficients for Final Models a

B, unstandardized beta; ER, external rotation; IR, internal rotation; rHRT, relative humeral retrotorsion; SE B, standard error of beta. Boldface type indicates statistical significance.
Entered into third step to independently determine contribution of playing position and limb dominance to model.
Discussion
This study contributes to the current literature describing the adaptive changes that occur with rHRT development regarding shoulder strength between the dominant and nondominant limbs. We found that the addition of rHRT significantly contributed to the model predicting dominant limb shoulder IR strength, although rHRT was not a significant independent predictor. Relative HRT did not significantly improve the prediction models for dominant limb ER strength, nondominant limb ER strength, or nondominant limb IR strength. These results complement previous studies regarding the effects of rHRT on modifiable objective measures in baseball players13,18,20,50,53-56; however, this is the first identifiable work to investigate whether a relationship between osseous adaptation and shoulder strength in baseball athletes exists.
The proximal humeral physis is considered the weakest part of the growing bone, which is susceptible to anterior rotation during skeletal immaturity and then ceases to change once the physis closes. 34 Because of the extreme glenohumeral ER required during the throwing motion, osseous changes are seen uniquely in the dominant throwing arm of skeletally mature baseball players. These adaptive changes strongly suggest that the osseous component of decreased humeral torsion contributes to the observed paradoxical shift in side-to-side differences of range of motion in collegiate baseball players, characterized by an increase in glenohumeral ER (8°-14°) and decrease in glenohumeral IR (10°-15°) on the throwing arm.13,18,20,53,55,56 Likewise, this observed increase in glenohumeral ER increases posterior capsule tightness, which limits the available IR.9,49,50,62 This soft tissue observation, derived in part from rHRT, has also delineated a relationship between osseous and soft tissue adaptations and scapular dyskinesis in overhead throwing athletes.48,58 Given the demonstrated effects that humeral torsion has on soft tissue structures about the glenohumeral joint, it is reasonable to suspect that rHRT may alter rotational strength profiles in baseball athletes. Furthermore, as rHRT is a nonmodifiable risk factor, particularly at the collegiate level when this osseous adaptation has ceased based on skeletal maturation, identifying relevant modifiable risk factors associated with rHRT is critically important for injury risk mitigation.
Shoulder strength profiles have been a key area of interest in injury risk mitigation in baseball athletes. The internal and external rotators play a crucial role throughout the throwing motion, eliciting high levels of rotator cuff muscle activation, garnering attention from sports medicine clinicians.21,35 Previous studies have demonstrated the relationship between shoulder strength measures and shoulder range of motion, specifically, deficiencies in shoulder rotational strength when clinical glenohumeral IR deficit is observed.3,28 A recent study has shown a meaningful relationship between shoulder IR strength and elbow varus torque, suggesting that shoulder IR strength may mitigate elbow loading while controlling for velocity. 5 Given the relationship observed from the results of the present study, an intimate relationship between rHRT and dominant limb shoulder IR strength may exist and ultimately affect the rate of loading during overhead throwing without detracting from performance.
While rHRT significantly improved the dominant limb shoulder IR strength model, it was not determined to be a statistically significant predictor. These findings offer support that the degree of rHRT may affect shoulder strength profiles, but the contribution of rHRT to shoulder IR strength should be interpreted with caution. Additionally, for the dominant limb shoulder IR strength model, both playing position and limb dominance independently improved the model without demonstrating statistical significance as a predictor. In essence, the regression coefficients garnered from this model suggest that a larger rHRT value (ie, a greater side-to-side difference in rHRT), a reported primary position as a nonpitcher, and right-handed limb dominance negatively affect predicted dominant limb IR strength; these conclusions must be interpreted with caution, as these independent predictors were not significant. Interestingly, body weight and height were retained as significant predictors for models predicting dominant and nondominant limb ER strength and dominant limb IR strength. Associations between anthropometric measures and strength have been demonstrated, and variations in body composition can influence strength measures at varying regions across the body.1,43 Strength measures in baseball athletes have been previously normalized by anthropometric variables, such as body mass and ulnar length, a derivative of height, in attempts to account for between-participant variability.4,36,47 Additionally, a recent study has demonstrated the appropriateness of utilizing a body mass normalization method for rotational strength measures in baseball athletes. 38 While no definitive conclusions can be drawn from the present data, future studies may work to identify how and to what degree anthropometric variability affects shoulder rotational strength profiles in baseball athletes.
When analyzing the results of our study, we anticipated that the increase in relative posteromedial rotation of the humeral head observed with increasing degrees of HRT would correlate to shoulder rotational strength through an alteration in the length-tension relationship of the posterior rotator cuff. The length-tension relationships of various musculature have been well established in other body regions in which alterations in strength and force production can be elucidated based on muscle length.11,12,40,44,59,67 This creates a phenomenon in which a given muscle will demonstrate its peak force producing capacity at midranges of motion, but as it approaches either maximally shortened or lengthened positions, the strength of the muscle is the weakest. Previous studies have suggested that 1-joint muscles, like the posterior muscles of the rotator cuff, demonstrate peak force–generating capacities in a shortened position. 16 However, an overwhelming majority of the literature demonstrates that during an isometric contraction, a muscle will exert less force at both its maximally shortened and maximally lengthened positions due to overextending and overlapping of sarcomeres.26,61,68 This has been demonstrated specifically in the internal and external rotators of the shoulder joint. 15 The results of the present study support the speculative notion that rHRT may negatively affect shoulder IR strength through an alteration in the displacement of the humeral head, altering the length-tension relationship and, ultimately, the force-generating capacity of the internal rotators; these premises were not studied directly in this study and thus should be interpreted with caution and treated as speculation at the present time.
One interesting observation was that of the mean KJOC scores reported for this cohort, a mean score of 87.7 (88.4 for pitchers, 86.6 for position players) was found at a spring preseason baseline. The KJOC score measures self-perceived function of the throwing limb in baseball athletes, and a score between 90 and 100 has been suggested to represent excellent self-perceived function.41,64 However, the current literature on normative KJOC scores in collegiate athletes is mixed, as scores as low as 81.3 in uninjured athletes have been reported, ranging in the 80s and 90s in previously published studies.14,22,38,57,60,64 Our observations are in line with this in that, regardless of position, collegiate baseball athletes demonstrate preseason scores below the normal threshold. Further research is needed to better understand the utility of the KJOC score in classifying injured and uninjured populations in collegiate baseball athletes.
There are limitations associated with this study. First, our sample consisted of only collegiate baseball athletes; while this limits the generalizability of the findings, we intentionally chose a skeletally mature population (based on age) to demonstrate the ultimate effects of rHRT development on shoulder strength. The inclusion of skeletally immature athletes may alter these results by including athletes on a relative spectrum of rHRT development. Additionally, we were unable to gather data regarding prior injury status and timing of prior injuries in this cohort. Previous injury history may affect shoulder rotational strength profiles and should be considered in the interpretation of these results. Next, we chose to include both right-handed and left-handed throwing athletes. While this does not immediately seem like an immedieate limitation, previous work has demonstrated discrepancies in the development of rHRT by limb dominance and may affect the findings. Finally, the strength testing protocol chosen in this study does not represent functional throwing positions in baseball athletes. Testing positions for rotational shoulder strength vary across the literature. In this study, rotational shoulder rotational strength was measured isometrically in a seated position with the elbow flexed to 90° with the shoulder in neutral at 0° of abduction. This position allows for improved standardization (and, as demonstrated by Table 1, excellent intra- and interrater reliability) of the measurement position but may allow for increased recruitment of secondary muscle groups compared to other measurement positions. While the study staff continuously monitored the testing positions for substitutions (trunk lean, trunk rotation, shoulder abduction, etc) during isometric strength testing, the results could be impacted by the methodology used.
Conclusion
The results of this study demonstrated a significant association between IR strength and rHRT. Therefore, increased anatomic HRT (or decreased humeral torsion) on the dominant limb may result in alterations in muscle length-tension relationships, ultimately affecting the maximum force-generating capacity of shoulder IR strength. Additionally, effects of playing position (pitcher) and limb dominance (left-handed) independently and positively contributed to these strength prediction models, demonstrating an association between shoulder IR strength and rHRT, playing position, and limb dominance. Bony adaptations in the overhead throwing athlete, such as the degree of humeral torsion, are nonmodifiable risk factors for throwing-related shoulder and elbow injury. Continued work delineating the effects of humeral torsion on other modifiable risks is necessary to identify key objective performance indicators that can be manipulated through prescribed interventions to mitigate throwing-related injury risk. The clinical observation of large rHRT should prompt clinicians to diligently assess other known and modifiable musculoskeletal risk factors, such as glenohumeral range of motion, capsular adaptations, scapular dyskinesis, and, based on the results of the present study, shoulder strength profiles, in order to more accurately evaluate injury risk in the overhead throwing athlete.
Footnotes
Final revision submitted March 2, 2026; accepted March 9, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.E.C. has received payments from Arthrex, Medinc of Texas, and Stryker Corporation in the form of royalties or license and travel and lodging.
Ethical approval for this study was obtained from the institutional review board through the University of Texas Health Science Center and Memorial Hermann Hospital System (HSC-MM-22-0537).