
Abstract
Background:
Young individuals with exercise-induced lower leg pain (ELP) may occasionally have rare entities such as functional popliteal artery entrapment syndrome (fPAES) or deep posterior chronic exertional compartment syndrome (dp-CECS). Diagnostic gold standards are absent for these syndromes, which share common symptoms like pain, tightness, and cramps, leading to significant treatment delays.
Purpose:
To determine whether the severity and frequency of typical symptoms in fPAES and dp-CECS are different.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Between January 2013 and February 2024, frequency and severity of leg pain, tightness, cramps, muscle weakness, and foot paresthesias were scored using a 5-point Likert scale (not severe, mild, moderate, severe, or very severe and never, sometimes, half of the time, most of the time, or all of the time) at rest and during exercise in patients with fPAES or dp-CECS before and after invasive therapy (surgery or botulinum toxin-A injection for fPAES, fasciotomy for dp-CECS). Only patients with fPAES and dp-CECS who reported success (cure or substantial relief) following a tailored treatment were studied. Nonnormally distributed data were presented as median (range or IQR), and normally distributed data were presented as mean ± SE. Nominal variables were compared using the χ2 test, and ordinal and continuous variables were compared with Mann-Whitney U tests. Binomial logistic regression was used to evaluate associations between fPAES or dp-CECS and symptom scores at rest and during exercise (95% confidence interval).
Results:
Data of 69 patients were available for analysis (fPAES, n = 24; dp-CECS, n = 45). Frequency and severity of pain, cramps, and muscle weakness were not different between groups. However, high foot paresthesias scores at rest (P = .009; odds ratio [OR], 1.17; 95% CI, 1.04-1.32) and during exercise (P = .008; OR, 1.193; 95% CI, 1.05-1.36) were associated with fPAES. Conversely, high tightness scores during rest pointed toward dp-CECS (P = .003; OR, 0.801; 95% CI, 0.69-0.93). Bilateral complaints were more common in fPAES (92%) compared to dp-CECS (40%; P = .001).
Conclusion:
Our study showed that patients who reported success after tailored treatment showed that standardized history taking may aid in distinguishing patients with exercise-induced lower leg pain due to fPAES from those with dp-CECS.
Keywords
The differential diagnosis of exercise-induced leg pain (ELP) in young individuals includes relatively uncommon syndromes such as popliteal artery entrapment syndrome (PAES) and deep posterior chronic exertional compartment syndrome (dp-CECS). PAES is caused by compression of the popliteal artery, most often due to hypertrophic lower leg muscles (functional PAES [fPAES]). In contrast, dp-CECS is thought to result from inappropriately elevated lower leg muscle compartment pressures. Both syndromes are characterized by exertion-induced calf pain and tightness.18,19 Findings at physical examination are nonspecific. Elevated muscle compartment pressures strongly point toward the presence of dp-CECS. 15 However, the role of imaging and functional tests is also to exclude other ELP syndromes such as medial tibial stress syndrome or stress fractures. As diagnostic gold standards for fPAES and dp-CECS are lacking, the identification of both entities is per exclusionem. As a consequence, treatment delays of up to 3 years in these young and active patients are not uncommon.
Simple tests distinguishing fPAES from dp-CECS are needed. 18 A recent study on ELP patients >50 years of age found that detailed history taking yielded characteristic symptom patterns associated with dp-CECS. 4 A detailed history may aid in reducing diagnostic delays of these ELP syndromes. The purpose of this prospective study was to determine whether severity and frequency of typical symptoms in fPAES and dp-CECS are different. It is hypothesized that meaningful differences in symptoms exist between the 2 syndromes.
Methods
Design and Setting
Patients were recruited from a specialized referral center for patients with ELP in the Netherlands. At present, approximately 700 new patients with ELP are evaluated yearly by the departments of sports medicine and surgery of this center. Specifics of the study were approved by the local medical ethical review board (NL82601.015.22). Minors completed the questionnaire in the presence of parents who granted consent.
Study Criteria
Each patient possibly having ELP was asked prior to a first outpatient evaluation to complete a questionnaire tabulating symptoms related to ELP. Eligible for study were patients aged between 15 and 40 years who were treated for fPAES or dp-CECS between January 2013 and February 2024. Inclusion criteria were a completed baseline questionnaire (Appendix 1) and a follow-up questionnaire containing a patient-reported outcome graded as an excellent or good treatment result 3 to 12 months after surgery (fPAES or dp-CECS; Appendix 2, question 4) or 6 weeks after a botulinum toxin-A injection (fPAES). The diagnosis of fPAES or dp-CECS was considered highly likely if patients reported an excellent or good outcome after this tailored treatment. Patients were excluded if they reported a reasonable, same, or poor outcome following treatment or if vascular, neurologic, or orthopaedic comorbidities emerged during the 1-year follow-up period.
Workup of fPAES and dp-CECS
A suspicion of fPAES is based on a history of lower leg pain during exertion that greatly diminishes within minutes after standing still, as in vascular intermittent claudication. 9 Pedal pulses may disappear following provocative plantar flexion. Duplex ultrasound analysis during provocative tests (defined as a patient positioned prone while exerting plantar foot flexion against fixed resistance) often reveals entrapment, as reflected by arterial narrowing and increased peak systolic velocity (PSV, m/s). 2
A case of dp-CECS is suspected on the basis of calf pain and tightness that often lasts for hours following exertion. 18 Palpation may reveal a tender medial leg compartment. Dynamic intracompartmental pressure (ICP) measurements often find increased muscle pressures after provocation. 20 A positive ICP was defined as a preexercise pressure ≥15 mm Hg, a 1-minute postexercise pressure ≥30 mm Hg, or a 5-minute postexercise pressure ≥20 mm Hg. 15 Diagnostic criteria suggestive of both entities are depicted in Table 1.
Criteria Suggestive of fPAES or dp-CECS a
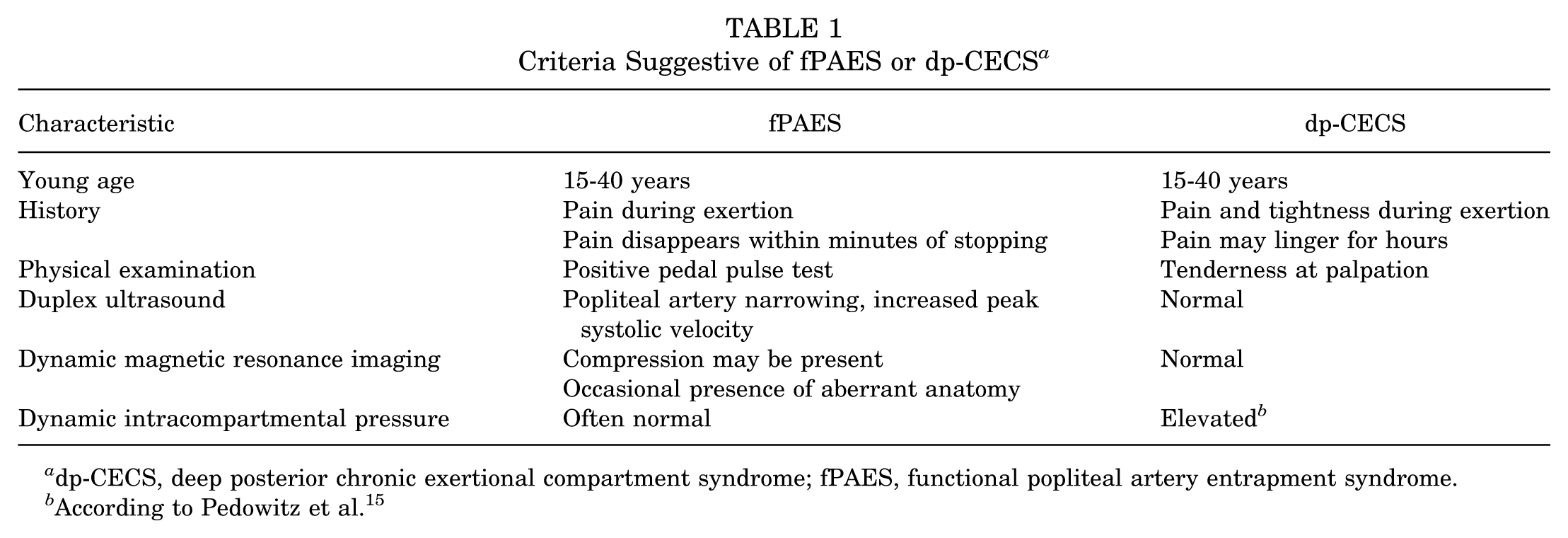
dp-CECS, deep posterior chronic exertional compartment syndrome; fPAES, functional popliteal artery entrapment syndrome.
According to Pedowitz et al. 15
Management of fPAES and dp-CECS
Between January 2013 and February 2023, all patients with symptomatic fPAES not responding to conservative treatment underwent plantar muscle resection and opening of the soleal tunnel via an infragenual approach according to Turnipseed (n = 14).10,18 After February 2023, treatment with fPAES was initiated with an ultrasound-guided injection of 50 IU botulinum toxin-A (BTX) in the medial head of the gastrocnemius muscle, as well as in the plantar muscle (if present) (n = 10).
Invasive management of symptomatic dp-CECS was offered following a failed conservative treatment regimen after multidisciplinary evaluation and included a fasciotomy of all 3 deep posterior muscles (long digital, hallucis, and posterior tibial) via a medial approach. Specifics of the operation were published previously. 21 Surgery was performed in a day care setting by 3 different surgeons with ample exposure to these patient populations. All patients were informed of the nature of the syndrome and consented verbally to all treatment specifics.
Questionnaires
ELP questionnaires were designed in 2012 and introduced in our facility in 2013 (Appendix 1). The aim was to standardly assess patient history using a set of questions, including time of onset of symptoms following initiation of exercise and relief after discontinuation. Five characteristic symptoms (pain, tightness, cramps, muscle weakness, and lower leg/foot paresthesias) are described by the patient. Symptom severity is scored as not severe (1 point), mild (2 points), moderate (3 points), severe (4 points), or very severe (5 points). Symptom frequency is tabulated as never (1 point), sometimes (2 points), half of the time (3 points), most of the time (4 points), or all of the time (5 points). Multiplying both scores allows calculation of a symptom score for each symptom. For instance, if a patient has mild pain (2 points) most of the time (4 points), 2 × 4 = 8 points for pain are obtained. A total symptom score is calculated as the sum of each of these 5 symptom scores and ranges from 5 points (“none of the 5 symptoms”) to 125 points (“each symptom always very severe”). Scores are obtained during rest as well as during exercise. Follow-up questionnaires scoring residual symptoms and outcomes are completed after 6 weeks (patients with fPAES receiving BTX, n = 10) or after 3 or 12 months (all other 59 operative patients, Appendix 2).
Statistical Analysis
Data are expressed as median (with range or interquartile range [IQR]) in case of a nonnormal distribution and as mean (with standard error) if normal. Chi-square test was used to assess potential differences in nominal variables. The Mann-Whitney U test was used for determining possible group differences in ordinal or continuous variables. Binomial logistic regression was executed to determine associations between fPAES or dp-CECS and symptom scores at rest and during exercise (95% confidence interval). Missing data are referred to in the tables. Datasets were evaluated for outlying values, identified using Tukey's fence of Q3 plus 1.5 times the IQR. Following this methodology, 1 outlying value for time of symptom onset was removed. Similarly, 2 outliers regarding the variable time of symptom relief were removed from a total of 25 values. Statistical analyses and presentation are consistent with the CHAMP statement. 14
Results
A total of 1427 patients with ELP syndromes were evaluated in our clinic over the 11 years of interest, and 69 patients fulfilled study criteria (fPAES, n = 24, 35%; dp-CECS, n = 45, 65%; Figure 1).

Patient flow diagram. dp-CECS, deep posterior chronic exertional compartment syndrome; fPAES, functional popliteal artery entrapment syndrome. *Diagnosis confirmed is defined as an excellent or good outcome after tailored treatment.
Characteristics of fPAES and dp-CECS Populations
Age, sex distribution, and diagnostic delay were not different (Table 2). Patients were previously evaluated by a physical therapist (99%), sports physician (97%), neurologist (41%), or orthopaedic surgeon (28%). Almost all (96%) received a combination of conservative treatments, including rest, physical therapy, massage, shockwave therapy, dry needling, prolotherapy, inlays, walking training, and/or compression stockings, prior to invasive treatments.
Characteristics of fPAES and dp-CECS Populations a
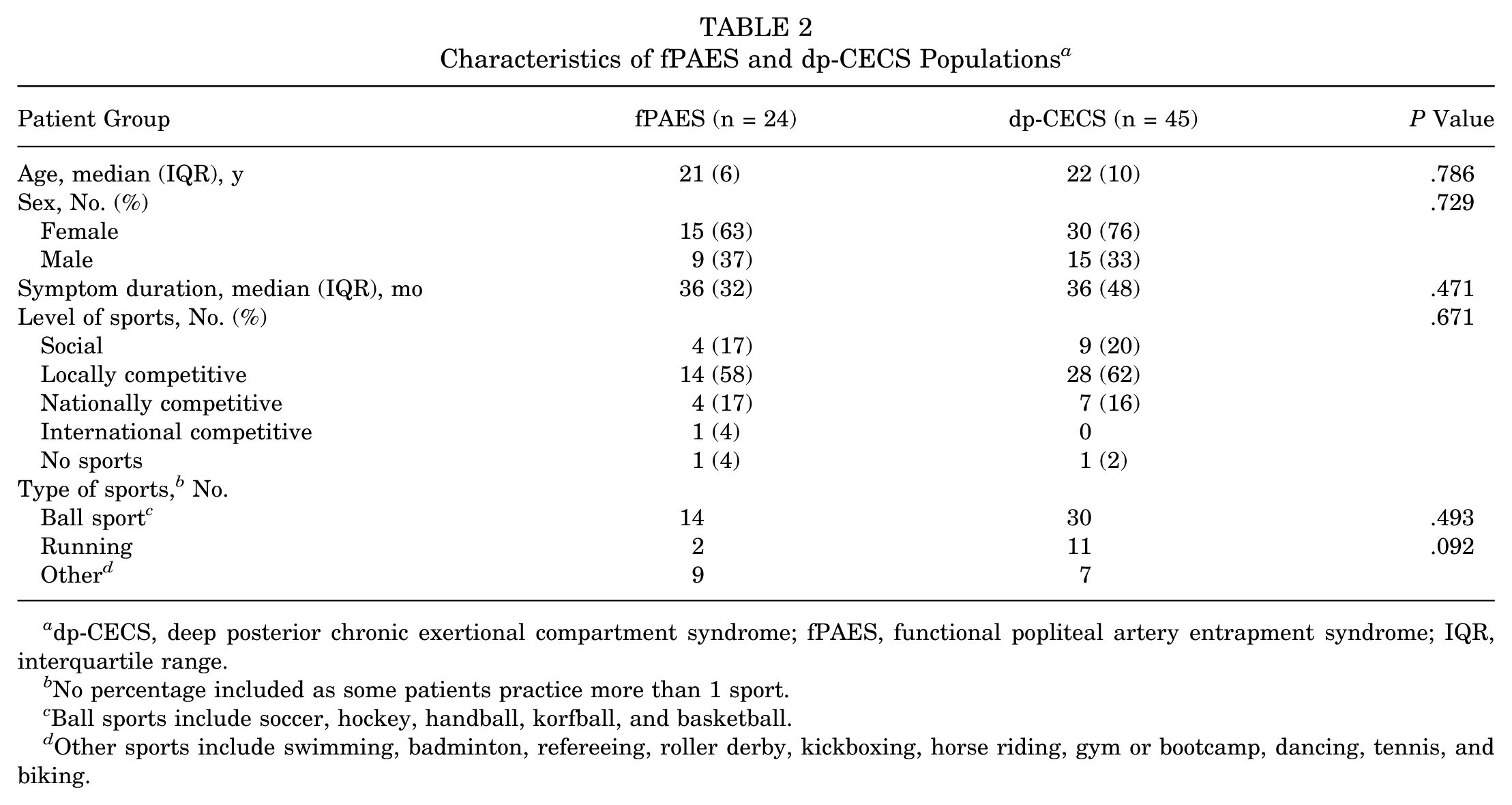
dp-CECS, deep posterior chronic exertional compartment syndrome; fPAES, functional popliteal artery entrapment syndrome; IQR, interquartile range.
No percentage included as some patients practice more than 1 sport.
Ball sports include soccer, hockey, handball, korfball, and basketball.
Other sports include swimming, badminton, refereeing, roller derby, kickboxing, horse riding, gym or bootcamp, dancing, tennis, and biking.
Most patients practiced a ball sport such as soccer, field hockey, handball, korfball, or basketball (Table 2). The percentage of runners did not differ among groups. Level of sport was also similar (P = .671). Bilateral complaints were more common in fPAES (92%) compared to dp-CECS (40%; P = .001).
Imaging and Tests in fPAES and dp-CECS
Tables 3 and 4 depict imaging and tests for both entities. The increase in PSV following provocation is significantly higher in fPAES. Occlusion of the popliteal artery during provocation also occurs more often in the fPAES group (46% vs 0, P = .004).
Duplex Ultrasound in fPAES (n = 24) and dp-CECS (n = 45) a
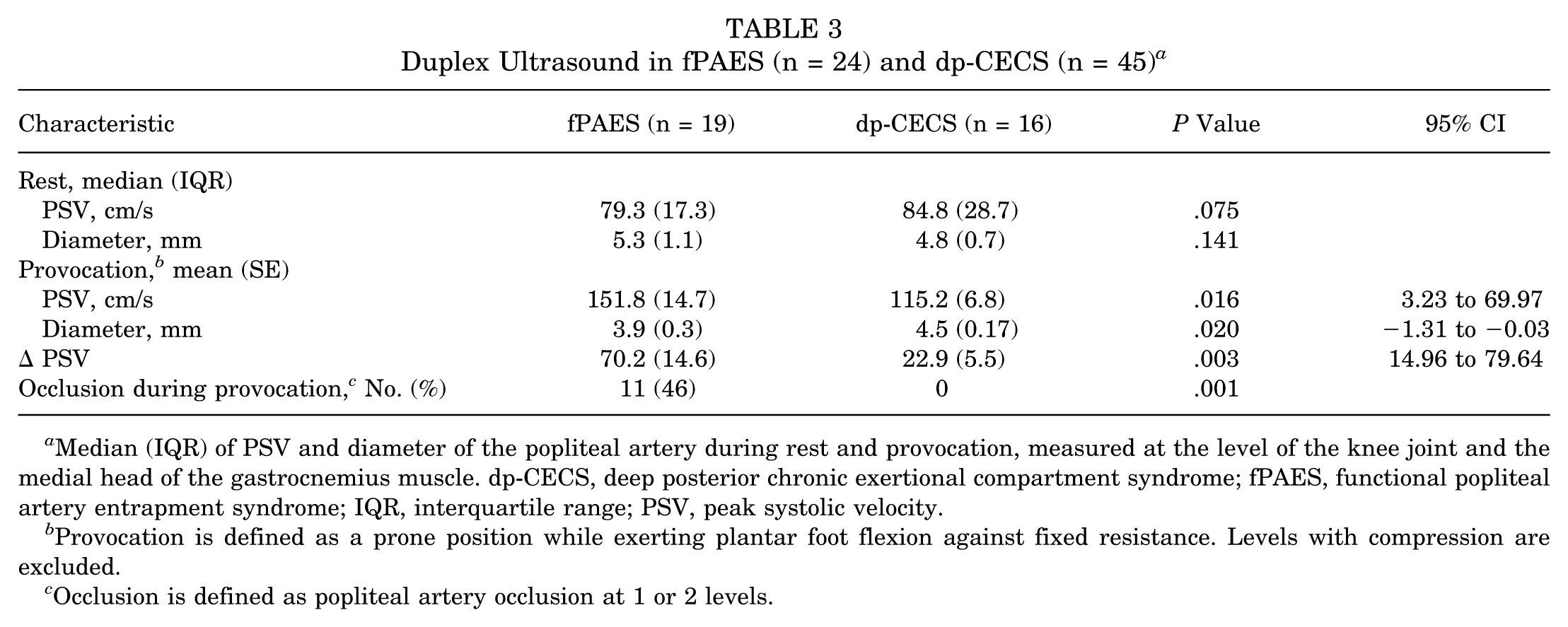
Median (IQR) of PSV and diameter of the popliteal artery during rest and provocation, measured at the level of the knee joint and the medial head of the gastrocnemius muscle. dp-CECS, deep posterior chronic exertional compartment syndrome; fPAES, functional popliteal artery entrapment syndrome; IQR, interquartile range; PSV, peak systolic velocity.
Provocation is defined as a prone position while exerting plantar foot flexion against fixed resistance. Levels with compression are excluded.
Occlusion is defined as popliteal artery occlusion at 1 or 2 levels.
MRI, ABI, and ICP in fPAES (n = 24) and dp-CECS (n = 45) a
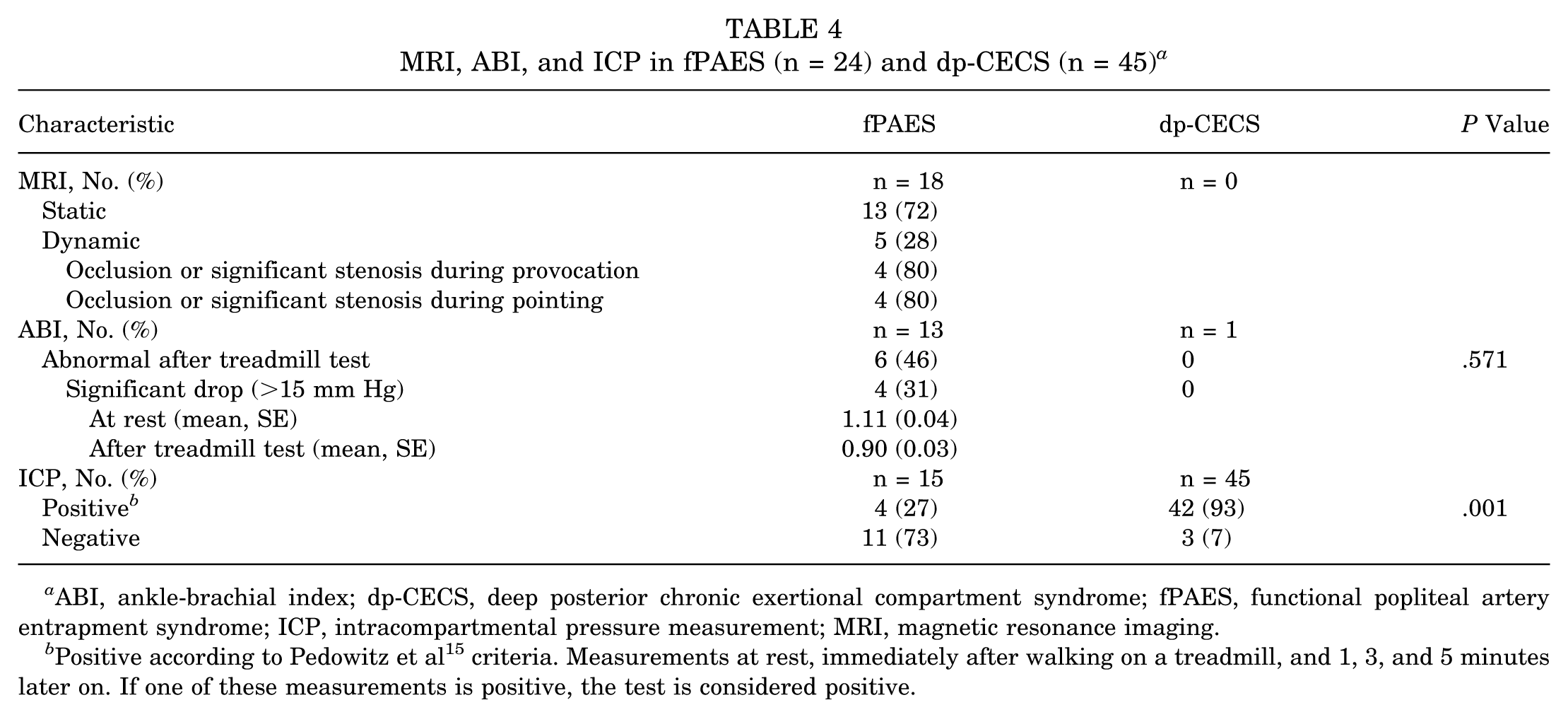
ABI, ankle-brachial index; dp-CECS, deep posterior chronic exertional compartment syndrome; fPAES, functional popliteal artery entrapment syndrome; ICP, intracompartmental pressure measurement; MRI, magnetic resonance imaging.
Positive according to Pedowitz et al 15 criteria. Measurements at rest, immediately after walking on a treadmill, and 1, 3, and 5 minutes later on. If one of these measurements is positive, the test is considered positive.
Symptom Onset and Relief in fPAES and dp-CECS
Patient-reported time of symptom onset (median, in minutes) after starting exercising is similar (fPAES 5 minutes, IQR 9 [n = 23] versus dp-CECS 5 minutes, IQR 10 [n = 44]; P = .390). However, significantly fewer patients with fPAES experience persisting symptoms postexercise (fPAES 38% vs dp-CECS 71%; P = .007). Median time until symptom relief after an exercise is 10 minutes in both groups, although the variation tends to be larger in dp-CECS (fPAES 10 minutes, IQR 9 [n = 12] vs dp-CECS 10 minutes, IQR 650 [n = 13]; P = .087). The ratio of time until symptom relief/time of symptom onset is <5 in 11 of 12 patients with fPAES compared to 5 of 13 patients with dp-CECS (P = .052).
Daily Life Symptoms in fPAES and dp-CECS
No differences in symptom presence are found in daily life, at work, and at night (Table 5). Striking is the high nighttime frequency of symptoms in both patient groups.
Symptoms in Daily Life, During Work, and at Night in fPAES and dp-CECS a
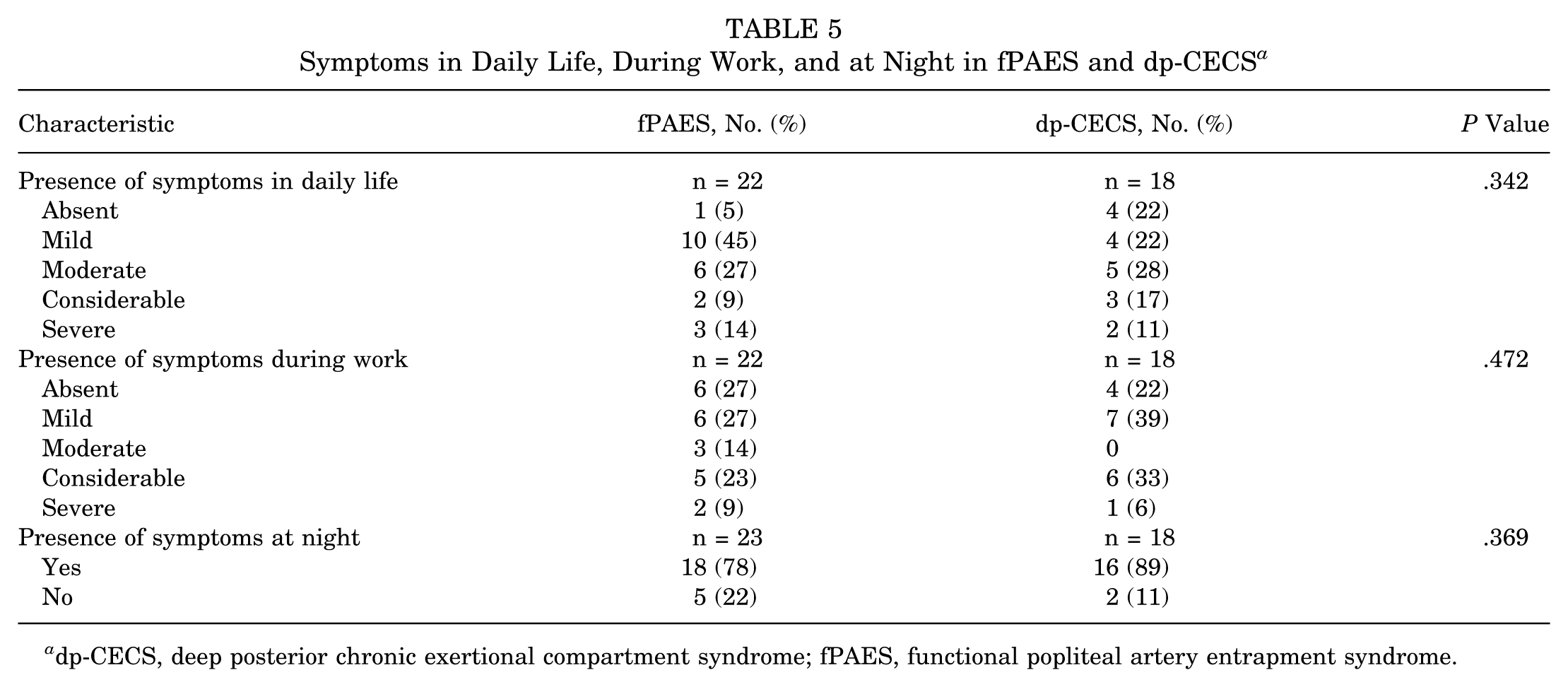
dp-CECS, deep posterior chronic exertional compartment syndrome; fPAES, functional popliteal artery entrapment syndrome.
Symptoms During Exercise and Rest in fPAES and dp-CECS
Symptom scores are depicted in Figure 2. During exercise, scores of pain, weakness, cramps, and tightness are not different between groups. However, patients with fPAES report significantly higher foot paresthesias scores (fPAES 12, IQR 12 vs dp-CECS 2, IQR 8; P = .011).
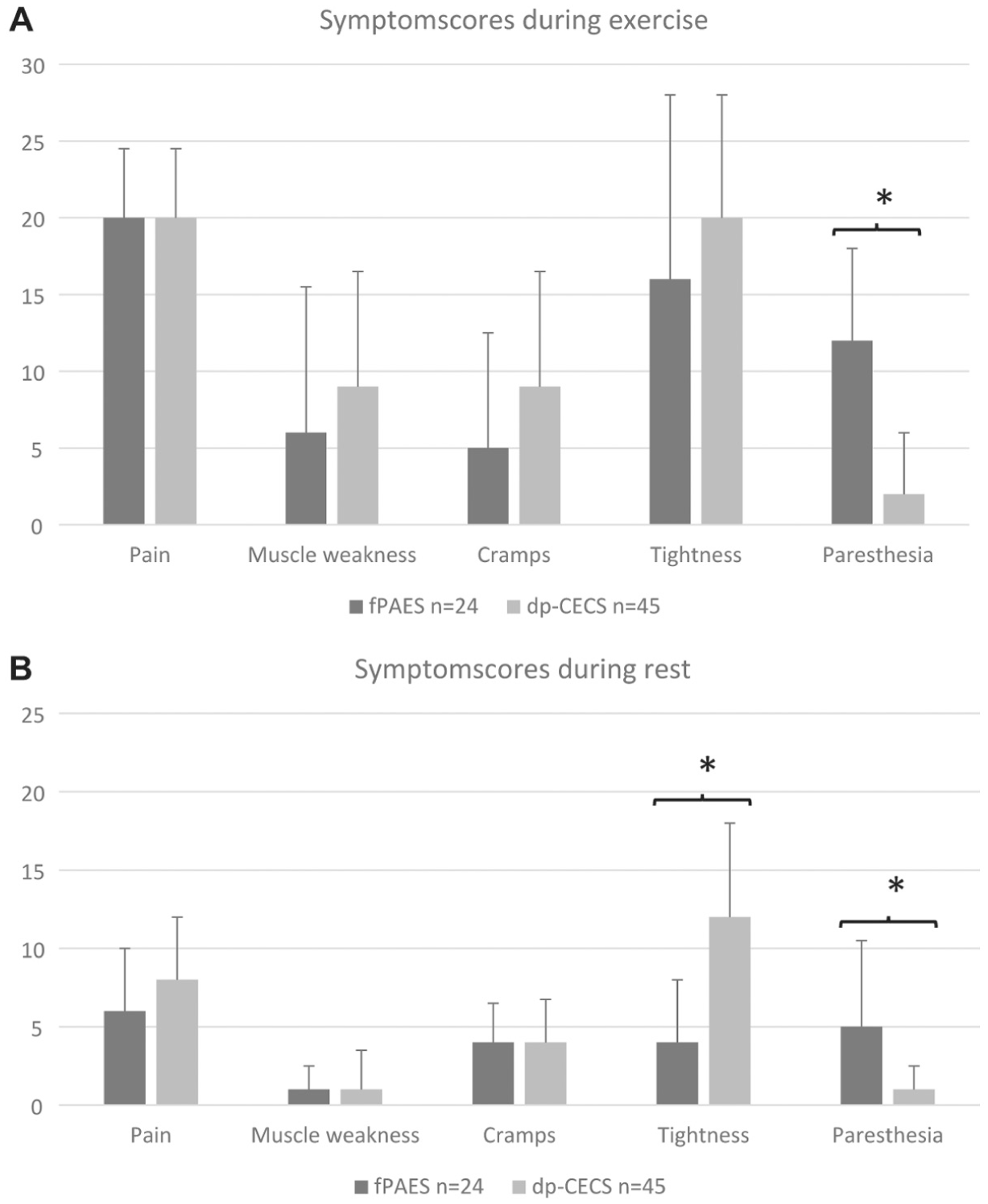
Symptom scores during (A) exercise and (B) rest in functional popliteal artery entrapment syndrome (fPAES) and deep posterior chronic exertional compartment syndrome (dp-CECS). Data expressed as median, IQR. *P < .05.
During rest, scores of pain, weakness, and cramps are not different. Again, patients with fPAES report significantly higher foot paresthesias scores (fPAES 6, IQR 11 vs dp-CECS 1, IQR 3; P = .024). In contrast, patients with dp-CECS score significantly higher regarding tightness (fPAES 4, IQR 8 vs dp-CECS 12, IQR 12; P = .002).
A multivariable logistic regression was used to assess whether foot paresthesia during exercise, tightness at rest, and bilateral symptoms predicted the presence of fPAES. These were selected for inclusion in the logistic regression based on prior univariate analyses, which demonstrated significant differences between patients with dp-CECS or fPAES. The overall model was significant compared with the null model (χ2 = 36.2, df = 3, P < .001). Model fit was good (Hosmer-Lemeshow P = .975 with Nagelkerke R2 = 0.572). High foot paresthesia scores during exercise predicted a greater likelihood of fPAES (OR, 1.193; 95% CI, 1.05-1.36; P = .008). Conversely, a high score of tightness during rest indicated a higher probability of a patient having dp-CECS (OR, 0.801; 95% CI, 0.69-0.93; P = .003). Interestingly, bilaterality of symptoms strongly suggested fPAES (OR, 10.88; 95% CI, 1.94-60.97; P = .007). Demographics, history, and symptom patterns of treatment responders and nonresponders in fPAES and dp-CECS were not statistically different. Therefore, these clinical parameters do not predict success after tailored treatment.
Discussion
The major findings of our study demonstrated that fPAES and dp-CECS are very similar and share fundamental symptoms, including pain, cramps, and muscle weakness. However, the current study shows that patients with fPAES more often report bilateral symptoms and foot paresthesias, whereas patients with CECS more often have muscle tightness during rest. These findings may aid in the diagnostic workup of future patients with ELP. Because responding patients with fPAES and dp-CECS exhibited symptom patterns comparable to nonresponders, these clinical features do not predict success after treatment.
Earlier studies have reported that demographic data or patient history do not allow for distinguishing fPAES from CECS.1,5,6 One study found that 30% patients who underwent surgery for fPAES reported an earlier dp-CECS fasciotomy, suggesting overlap. 11 In our fPAES group, 6 patients (25%) had an earlier fasciotomy. Our fPAES and dp-CECS populations did not differ with respect to age, sex, body mass index, athletic level, or type of sports. The only significant difference regarding patient history was the finding that most (92%) patients with fPAES reported bilateral symptoms compared to just 40% of patients with dp-CECS.
Most studies on fPAES and dp-CECS briefly discuss patient-reported symptoms but do not determine intensity and frequency.12,13 Serial symptom scoring potentially allows for objectively quantifying the burden to the patient and for monitoring treatment outcome. Our study found that pain, muscle weakness, and cramps were more frequent and severe during exertion compared to rest in both syndromes, as expected. Foot paresthesias were previously described in fPAES as well as in CECS.3,7,8,10,16 Turnipseed 18 described a higher prevalence of paresthesias in patients with fPAES, although a comparison was made with patients having CECS of the superficial (not the deep) posterior compartment (40% vs 4.2%). Interestingly, our patients with fPAES report more frequent and more intense foot paresthesias than patients with dp-CECS, both at rest and during exercise. The reason for this difference is unclear. It may be hypothesized that this is due to a proximal tibial nerve compression by the lower leg muscles in fPAES compared to a more distal nerve compression by the deep posterior muscles in dp-CECS. A neurologic analysis determining the extent of altered lower leg and foot skin sensation was not performed.
A number of studies report on calf muscle tightness in various types of ELP.4,7,20 Tightness in dp-CECS is hypothesized to occur as a result of an increased compartmental pressure of the 3 deep posterior muscles due to an unknown cause. 17 Our data indicate that patients with dp-CECS experience significantly more calf muscle tightness compared to those with fPAES during rest. We hypothesize that the effect of reperfusion following intermittent and repetitive ischemia in patients with fPAES might be less intense and shorter. Anyhow, it may be that the 2 syndromes are 2 sides of the same coin. This hypothesis is supported by the observation that 27% of patients with fPAES exhibited elevated compartment pressures and that several patients with dp-CECS demonstrated abnormal findings on popliteal artery ultrasound imaging.
Limitations
This study is not without limitations. One limitation of this study are different treatments and incomplete data sets. A number of questions may have been unclear to some patients. For instance, the question “Do symptoms subside after exercise?” was not concise enough. If the answer was “no,” patients were not asked how long the symptoms lingered. Since our center is a national referral center for patients with ELP, individuals with socioeconomic disadvantages may not be able to travel to the clinic. Therefore, the study population might be biased. Another limitation is the small number of study participants in both patient populations. This is also because the study protocol dictated that only patients who reported a successful treatment outcome (“responders”) were included. The aim of our study was to determine whether symptoms in fPAES and dp-CECS are different. We reasoned that patients with a history and physical examination consistent with dp-CECS, an ICP consistent with dp-CECS, who underwent surgery for possible dp-CECS, and who reported success after a fasciotomy were indeed likely to have dp-CECS. A similar line of reasoning was used for the fPAES population. Conversely, it was assumed that including treatment nonresponders in the study design potentially led to heterogeneity and bias. By this approach, both study populations only contained patients who were most likely having fPAES or dp-CECS, allowing for an optimally valid comparison. Another limitation is that imaging and functional assessments were not standardized across all participants in both cohorts. Future studies should aim to implement uniform diagnostic protocols across both groups to minimize bias.
Conclusion
This study of patients who reported success after tailored treatment showed that standardized history taking may help distinguish patients with exercise-induced lower leg pain due to fPAES from those with dp-CECS.
Footnotes
APPENDIX 1—Dutch National Network for Exercise-Induced Pain Syndromes (NIAPS) Questionnaire Regarding Exercise-Induced Pain Syndromes in the Lower Leg. Translated from Dutch to English
APPENDIX 2—Dutch National Network for Exercise-Induced Pain Syndromes (NIAPS) Follow-up Questionnaire After Surgery for Exercise-Induced Pain Syndromes in the Lower Leg. Translated from Dutch to English
Study Number:
Please check the appropriate answer for each question.
□ 1 week
□ 2 weeks
□ 4 weeks
□ 6 weeks
□ Other, namely:
□ No
□ Yes, a hematoma
□ Yes, an infection
□ Yes, a sensory disturbance in or around the operated area
□ Other, namely:
□ No
□ Yes
□ Other, namely:
□ Fully resolved
□ Improved a lot
□ Improved a little
□ Stayed the same
□ Worsened a little
□ Worsened a lot
□ Worse than ever
□ Absolutely satisfied
□ Very satisfied
□ Somewhat satisfied
□ Neither satisfied nor dissatisfied
□ Somewhat dissatisfied
□ Seriously dissatisfied
□ Absolutely dissatisfied
□ Yes, I am back at my previous level
□ Yes, I am back, but less intensively than before the symptoms started
□ Yes, but I have chosen a different sport
□ No
□ Other, namely:
________________________________________
□ None
□ Recreational
□ Local competitive
□ National competitive
□ International competitive
□ Not at all
□ A little
□ Moderately
□ A lot
□ Very much
□ Not at all
□ A little
□ Moderately
□ A lot
□ Very much
The following questions concern the symptoms you have experienced during the past month.
Severity: □ None □ Mild □ Moderate □ Severe □ Very severe
Frequency: □ Never □ Sometimes □ Half of the time □ Often □ Always
Severity: □ None □ Mild □ Moderate □ Severe □ Very severe
Frequency: □ Never □ Sometimes □ Half of the time □ Often □ Always
Severity: □ None □ Mild □ Moderate □ Severe □ Very severe
Frequency: □ Never □ Sometimes □ Half of the time □ Often □ Always
Severity: □ None □ Mild □ Moderate □ Severe □ Very severe
Frequency: □ Never □ Sometimes □ Half of the time □ Often □ Always
Severity: □ None □ Mild □ Moderate □ Severe □ Very severe
Frequency: □ Never □ Sometimes □ Half of the time □ Often □ Always
Severity: □ None □ Mild □ Moderate □ Severe □ Very severe
Frequency: □ Never □ Sometimes □ Half of the time □ Often □ Always
Severity: □ None □ Mild □ Moderate □ Severe □ Very severe
Frequency: □ Never □ Sometimes □ Half of the time □ Often □ Always
Severity: □ None □ Mild □ Moderate □ Severe □ Very severe
Frequency: □ Never □ Sometimes □ Half of the time □ Often □ Always
Severity: □ None □ Mild □ Moderate □ Severe □ Very severe
Frequency: □ Never □ Sometimes □ Half of the time □ Often □ Always
Severity: □ None □ Mild □ Moderate □ Severe □ Very severe
Frequency: □ Never □ Sometimes □ Half of the time □ Often □ Always
Final revision submitted February 3, 2026; accepted March 14, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.H.G. received funding from Stichting Stimuleren Sportgeneeskunde ZOB, the Netherlands.
Ethical approval for this study was obtained from the Máxima MC medical ethical review board (NL82601.015.22).
Data Availability
Patient-level data and the full data set are available from the corresponding author upon reasonable request.