
Abstract
Background:
Posterior cruciate ligament (PCL) injuries may lead to significant anteroposterior and rotational knee instability. Traditional reconstruction techniques, including single-bundle (SB) and double-bundle (DB) approaches, have limitations in terms of restoring full biomechanical function. A posterolateral tenodesis (PLT) augmentation associated with PCL reconstruction has been described, consisting of a nonanatomic bundle that shares the PCL tibial tunnel, courses along the posterior aspect of the lateral femoral condyle from an intra-articular to an extra-articular position, and is fixed at the lateral femoral epicondyle to provide additional control of tibial external rotation.
Purpose:
To determine the impact of adding a posterolateral tenodesis (PLT) to a PCL reconstruction to restore knee rotational and posterior stability.
Study Design:
Controlled laboratory study.
Methods:
In total, 24 embalmed cadaveric human knees were randomized into 3 main groups: intact (control), isolated PCL-deficient, and combined PCL + posterolateral corner (PLC)–deficient (Fanelli type A). Each group underwent sequential reconstructions using SB and DB PCL techniques, with and without the addition of PLT. Biomechanical testing included measurements of posterior tibial translation (PTT) and external tibial rotation (ER) at 30° and 90° of flexion using a custom-built robotic testing machine and inertial sensors. Porcine flexor tendons were used as grafts.
Results:
Sectioning the PCL significantly increased both PTT and ER, with values peaking in the combined PCL + PLC-deficient group (PTT: 10.3 ± 0.8 mm; ER: –30.4°± 0.8° at 90° of flexion). SB and DB reconstructions alone partially restored stability, but residual laxity persisted, especially in the rotational parameters. The addition of PLT significantly reduced both PTT and ER. In the DB + PLT group with combined PCL + PLC injury, the PTT and ER values (3.2 ± 0.3 mm and –12.5°± 0.3°, respectively) were statistically indistinguishable from the intact group (P > .05).
Conclusion:
Combined PCL and PLC injuries result in marked rotational and posterior instability. When added to SB or DB PCL reconstruction, PLT significantly improves biomechanical function, particularly regarding rotational control. These findings support the inclusion of PLT in surgical protocols addressing complex PCL-related instability.
Clinical Relevance:
Adding a posterolateral tenodesis to PCL reconstruction may reduce residual instability and improve outcomes in complex ligament injuries.
The posterior cruciate ligament (PCL) plays a fundamental role as the primary restrictor of posterior tibial translation. However, it also serves as a secondary stabilizer of external rotation (ER) and of excessive varus or valgus angulation at the knee, in conjunction with the structures that make up the posterolateral corner (PLC) of the knee.30,36 The PLC of the knee comprises several key structures: the fibular collateral ligament (FCL), the popliteus tendon (PT), and the popliteofibular ligament (PFL). These components function collectively to stabilize the knee against varus forces and external rotational stresses.15,18 Specifically, the FCL acts as the primary restraint to varus angulation, while the PT and the PFL contribute significantly to controlling the ER of the tibia relative to the femur.18,20 Secondary stabilizers, such as the mid-third lateral capsular ligament and the fabellofibular ligament, support the PLC by reinforcing resistance to varus and rotational forces, particularly when the primary structures are compromised. 14
The PCL originates in the anterolateral portion of the medial femoral condyle and attaches below the posterior joint line in a depression between the posterior edges of the medial and lateral tibial plateaus, which is known as the PCL facet. Its distal attachment is located above a shallow ridge called the champagne glass drop-off. 38 It is approximately 32 to 38 mm long. 26 This ligament is composed of 2 bundles of functional fibers that tighten at different degrees of knee flexion, the anterolateral (AL) bundle and the posteromedial (PM) bundle. Each bundle serves a distinct function. The AL bundle tightens during flexion, and the PM bundle tightens during extension. 26 The PCL serves as the primary barrier against posterior tibial displacement at all degrees of flexion, except near full extension. 5
There is currently some controversy as to whether sectioning the PCL increases ER. Some studies describe no increase in ER.27,29,36,49 Yet, other authors state that ER does increase.41,50 The PCL reconstruction can be performed using a single-bundle (SB) or double-bundle (DB) reconstruction technique. 44 However, neither has been shown to be significantly superior in terms of mid- and long-term functional clinical outcomes.34,52,59 Despite this, DB reconstruction is superior to SB reconstruction for biomechanical restoration.32,40 The DB technique is the only one that allows reproduction of PCL physiology, with an anterolateral bundle that tightens in flexion and a posteromedial bundle that tightens in extension. 48
Current PCL reconstruction techniques aim to restore normal knee biomechanics and kinematics, ideally preventing symptomatic anteroposterior laxity and rotational instability contributing to postoperative residual instability.3,10,35,37,58 Posterior or posterolateral instability is the most frequently reported complication.25,61
The addition of lateral extra-articular tenodesis (LET) has been used as a complementary method in anterior cruciate ligament (ACL) reconstruction to address rotational instability and yields favorable results.2,21,31,60 Clinical studies have demonstrated restoration of side-to-side differences in anteroposterior translation in the knee, a higher return-to-sport rates, and overall increased patient satisfaction following combined ACL reconstruction and LET.1,21,47,54
Applying a similar concept as a complement to PCL reconstruction may enhance knee joint rotational stability. A technique recently described by Alvarez-Salinas et al 4 proposes a posterolateral tenodesis (PLT) technique to address the problem of residual instability. The PLT consists of a nonanatomic graft bundle that shares the PCL tibial tunnel, courses along the posterior aspect of the lateral femoral condyle from an intra-articular to an extra-articular trajectory, and is fixed at the lateral femoral epicondyle to provide additional restraint to tibial ER.
The objective of PLT is to enhance rotational stability and potentially reduce residual instability following PCL reconstruction. It is to be used in isolated reconstructions of the PCL for grade III ruptures associated with or unassociated with low-grade PLC injuries. It can be done using 2 preparation methods: (1) 2 separate tendon grafts for PCL reconstruction and PLT or (2) a Y-shaped Achilles tendon allograft. 4 The femoral and tibial tunnels are created following standard techniques. 22 The PLT femoral tunnel is prepared through a lateral incision made proximally and anteriorly to the lateral epicondyle.
The main purpose of this study was to determine whether an isolated and complete injury of the PCL causes a significant increase in ER, as well as to determine whether the addition of PLT to conventional reconstruction techniques (SB and DB) for the PCL restores ER to its native values. Additionally, the study aimed to determine the value of using PLT in a complete PCL injury combined with PLC injuries of the knee, classified as Fanelli type A. The latter involves injury to the PT and the PFL, resulting in increased ER of the knee in an experimental biomechanical model using human knees. 28
Our hypothesis posits that sectioning the PCL increases both ER and posterior translation of the tibia, with these values increasing further when a Fanelli type A injury is present. Similarly, we hypothesize that the inclusion of a PLT in combination with an SB or DB PCL reconstruction can significantly reduce the degree of ER and posterior translation to native values. This can be done in both a model of an isolated complete PCL injury and in combination with a Fanelli type A injury of the PLC.
Methods
An experimental biomechanical study was conducted on 24 nonpaired, nonarthritic, embalmed human cadaveric knees from 2 anatomy departments of the UANL. Each had been amputated 25 cm proximally and distally from the joint line. The study was approved by the Ethics Committee of the School of Medicine and University Hospital of the Universidad Autónoma de Nuevo León (UANL) under approval number #FI23-00001. The use of embalmed specimens instead of fresh-frozen tissue was required to comply with national biosafety regulations and legal frameworks regarding the handling of unclaimed cadaveric remains. To ensure the validity of the biomechanical assessment, embalming was performed by injecting a sequential mixture of commercial reagents (Metasyn, Rectifian, Introfiant, Syn Cav, Metaflow, Restaorative, and formaldehyde at 4%) (Dodge Co.) designed to preserve tissue with minimal stiffness (Walter Thiel's method). 51 The anatomic specimens had a mean age of 46 ± 6 years and were predominantly male (20 males and 4 females), with a mean body weight of 80.5 ± 13 kg.
Knees were excluded if they exhibited visible scars on the skin upon macroscopic inspection. Anteroposterior and mediolateral radiographic and fluoroscopic images were obtained to exclude knees with orthopaedic implants, severe osteoarthritis and evidence of prior surgeries, deformities, or fractures (all specimens had a tibial slope within the normal range, between 7° and 10°). The integrity of the meniscal structures and cruciate ligaments was assessed via arthroscopy to identify injuries that would contraindicate the use of the anatomic specimens. No specimens were excluded due to meniscal or ligamentous injuries.
Description of Study Groups
Following the preparation, the 24 cadaveric knees underwent initial biomechanical testing to obtain the baseline measurements (group A). Posterior tibial translation (PTT) and ER were recorded at 30° and 90° of knee flexion. After taking the baseline measurements, the 24 knees were randomized into 2 primary groups of 12 specimens each:
Groups C and D were subsequently subdivided into 2 subgroups (n = 6 each) that underwent SB and DB PCL reconstruction. Following the biomechanical assessments in each subgroup, a PLT was subsequently performed on all the specimens (Figure 1).

Twenty-four human cadaveric knees (group A) were allocated into sequential posterolateral corner (PLC)/posterior cruciate ligament (PCL) injury or isolated PCL injury models. Specimens underwent either single-bundle (SB) or double-bundle (DB) reconstruction, followed by the addition of a posterolateral tenodesis (PLT) in the final stage.
Following surgical reconstruction, each specimen underwent the same biomechanical testing protocol as in the baseline phase. PTT and ER were measured again at both 30° and 90° of knee flexion.
Sample Preparation
Controlled knee dissection was performed to preserve structural integrity. The legs were amputated, and dissection was done proximally and distally to the joint line, extending 25 cm in each direction. During this process, the skin and fat tissue were meticulously removed, while ensuring the preservation of the articular capsule, all adjacent muscle groups, and the knee extensor apparatus.
Two segments of polyvinyl chloride (PVC) tubing were fixed at the proximal and distal ends of each specimen. Each measured 2.5 cm in length and 5 cm in diameter. A high-strength fiberglass resin (Resin PP250) (Poliformas) was used to secure the samples to the PVC. The resin was mixed with a reaction accelerator at a ratio of 10 drops of activator per 10 mL of resin to ensure homogeneous polymerization. The mixture was carefully poured into the space between the PVC and bone to ensure complete encapsulation and eliminate air bubbles that might compromise system integrity. To optimize the curing process, warm air was applied for 10 minutes.
Once the resin had fully hardened, the samples were carefully positioned in a custom-designed machine. It had been previously employed in our earlier biomechanical knee studies.45,46
The machine is equipped with 3 motors: 2 NEMA 23 stepper motors (Model 57HS112; Wantai) for quadriceps and hamstring traction in the upper part of the device and 1 NEMA 34 stepper motor (Model 57HS76, Wantai, China) for the inferior part of the device. The latter is responsible for generating rotational forces. The individual tendons from the hamstrings and quadriceps were securely attached using suture tape, reinforced with multiple passes of mediolateral rip-stop suture No. 2 (Orthocord), and connected to cables. Those cables were then connected to the motors to generate the ground reaction force during testing (Figure 2).

Custom-designed device used for biomechanical assessment. (A) Central motor for tibial rotation. (B) Motors for quadriceps and hamstrings traction. (C) Central motor for compression and flexion.
Graft Selection and Preparation
For the preparation of the PCL reconstruction tissues, porcine flexor tendons were used, as previous studies have demonstrated that they exhibit stiffness and high-load resistance.12,23 The anterior region of the pig leg was dissected to obtain the flexor tendon group. These specimens were surplus tissues from pigs originally sourced for commercial consumption and were not obtained or sacrificed specifically for this study. Human grafts were not used, as embalmed tissues lose their biomechanical properties.24,55
Distinct graft configurations were used. They were designated to replicate both isolated SB PCL reconstruction and PCL reconstruction combined with PLT. For the isolated SB PCL reconstruction, 12-cm-long monoband grafts with a diameter of at least 8 mm were used. For the DB PCL reconstruction, a 12-cm-long Y-shaped graft with at least a 9-mm diameter in the common trunk of the graft (tibia tunnel) and a bifurcated end with at least 9 mm for the AL bundle and 7 mm for the PM bundle. For the PCL reconstruction using the PLT, Y-shaped bifurcated grafts were used, measuring 12 mm in diameter at the tibial portion, 9 mm in diameter for the PCL, and at least 6 mm for the PLT. The total length of the grafts was 16 cm (Figures 3 and 4).

Graft used for the monofascicular reconstruction of the posterior cruciate ligament.

Y-shaped graft used for the monofascicular reconstruction of the posterior cruciate ligament for additional posterolateral tenodesis.
Both graft types were prepared using high-strength, nonabsorbable sutures (FiberWire; Arthrex) and underwent hydration with a 0.9% NaCl solution before implantation to preserve their biomechanical properties. Porcine grafts were chosen due to their high similarity to human ligaments.8,11
Surgical Technique for PCL Reconstruction and PLT
The classic technique for tibial tunnel preparation in PCL reconstruction was followed,4,22 with slight modifications to perform the procedure in an open manner. It began with the preparation of the graft, including sutures at both ends. The tibial tunnel was then drilled from the anteromedial tibial cortex to the anatomic insertion of the PCL under direct vision while aiming for a slightly lateral exit point over the tibial PCL footprint. Using a conventional instrument system for PCL reconstruction (Arthrex), selective capsulotomies were performed to allow for adequate visualization. This was followed by the creation of the femoral tunnel in the lateral cortex of the medial femoral condyle using an outside-in system. Proper tunnel orientation and positioning were confirmed through direct observation. In the group in which the PLT was performed, the tibial tunnel diameter was adjusted to 12 mm to adequately accommodate both graft ends. Then the graft was passed through the tunnels and secured in place with interference screws. They had a diameter equal to that of the tunnel made and were 20 mm in length.
A technique described in the literature for DB PCL reconstruction 39 consists of preparing the graft into 2 distinct bundles (AL and PM), each sized appropriately for individual tunnel placement. The tibial tunnel is created first, following the same technique previously described. In it, a tibial aiming guide is used to establish a tunnel trajectory of approximately 55° to 65° to the tibial plateau. The femoral tunnels are then created with outside-in drilling techniques for independent AL and PM bundle fixation, with conventional ACL guides to ensure anatomic placement within the medial femoral condyle. The AL bundle tunnel is positioned higher and anteriorly, while the PM bundle tunnel is placed lower and more posteriorly to replicate native fiber orientation. Once the tunnels are prepared, the grafts are passed while ensuring each bundle follows its designated pathway. They are tensioned sequentially, typically fixing the PM bundle first at 90° of knee flexion, followed by AL bundle fixation at 40°. Fixation is achieved using interference screws. 22
Femoral-Side Preparation for PLT
To create the femoral-side fixation point for PLT reconstruction, a longitudinal skin incision of approximately 4 to 5 cm was made at the level of the lateral femoral epicondyle. The iliotibial band was also incised longitudinally until the bone plane was reached. A utility clamp was used to pass a suture from the extra-articular space into the joint, which was then retrieved through the anteromedial portal. This suture served as a shuttle to pass the proximal limb of the PLT.
Graft Passage and Insertion
The tail of the graft was passed from the anteromedial portal through the tibial tunnel using a retrograde technique. Initially, a posteromedial portal was created to provide access to the posterior compartment via a cannula. A wire loop was then inserted into the tibial tunnel from the posterior side and retrieved through an anteromedial portal using a suture retriever. Both ends of the graft were introduced into the tibia tunnel in a retrograde fashion. Once inside the tibia, the proximal end of the PCL graft was directed toward the femoral tunnel using the guide loop and then secured in place with an interference screw (Figure 5). The proximal limb of the PLT was passed in a retrograde manner with direct observation from the anterolateral portal. Then, a thread was passed from the extra- to the intra-articular space in an “over-the-top” fashion. The PLT graft was pulled retrogradely and fixed on the femoral epicondyle using a staple or interference screw, with the knee in full extension. For any of the PCL techniques used (SB or DB), the graft fixation sequence is as follows: proximal fixation of the PCL on the femur, followed by tibial fixation of the common graft, and, finally, fixation of the PLT at the described point with the knee in extension. The femoral fixation point for the PLT was established 3 mm distal and 3 mm anterior to the lateral femoral epicondyle (at the level of the popliteal groove). Optionally, a low-profile staple can be used at the referenced point to fix the PLT.

(A) Single-bundle posterior cruciate ligament (PCL) reconstruction. (B) Double-bundle PCL reconstruction. (C) Single bundle + posterolateral tenodesis. (D) Double-bundle PCL reconstruction + posterolateral tenodesis. LFC, lateral femoral condyle; MFC, medial femoral condyle.
Biomechanical Assessment
Testing was performed under standard laboratory conditions at an ambient room temperature of approximately 22°C. Prior to mounting, specimens were thawed from –20°C using a warm air flow and allowed to equilibrate/come to room temperature to ensure consistency in tissue behavior. The cadaveric specimens were mounted on a custom-built biomechanical testing machine and subjected to a 150-N load for 20 flexion-extension cycles with a range of motion from 0° to 90° at a frequency of 1 Hz.7,9 The objective was to eliminate the initial stiffness of the tissues. During the mounting process, the tibial portion was secured using a 4.5-mm cortical screw inserted through the PVC tube to improve structural stability. This portion was positioned perpendicular to the ground and connected to a NEMA 34 stepper motor (Model 57HS112; Wantai), which allowed for controlled free rotation. Meanwhile, the femoral portion was fixed to a loading head that facilitated translational compressions and was attached to a NEMA 34 stepper motor (Model 57HS76; Wantai) along a central axis.
To measure ER, a digital gyroscope (Model MOT0110; Phidget) was placed at the level of the tibial tubercle and firmly secured with a strap. Simultaneously, the tibial motor applied a 1-N traction until the physical limit of the anatomic specimen was reached. 19 For the posterior translation measurement, a force transducer cable (Model 9363; Revere) was fixed below the tibial tubercle and pulled posteriorly by a NEMA 34 stepper motor (Model 86HS156; Wantai) until the physical limit of the specimen was reached. 19
In both cases, 3 rotations were performed to calibrate the sensor before measurements, and data were later recorded using the Phidget Control Panel software. Displacement was determined using a pretest calibration curve in which the electrical output was correlated with physical distance (millimeters) measured with a digital caliper. External rotation was assessed based on changes in the y-axis, while posterior translation was evaluated using x-axis changes, with the software converting the transducer's voltage signals into linear displacement values. Negative numbers indicate the axis is lateral to the center (Figure 6). Each specimen underwent 3 consecutive measurements, which were independently reviewed and validated by 3 authors (R.M.A., C.F.O.G., C.C.C.).

Rotational changes along the y-axis captured by the Phidget gyroscope in the tibial segment.
A traction force of 1000 N was applied to the distal tibia via the central axis motor acting on the femoral portion. 19 Additionally, adjusted loads of 88 N and 67 N were applied to the quadriceps and hamstrings, respectively, at flexion angles of 30° and 90°. 43 Each degree of flexion was verified using a goniometer and defined as the angle formed between the anatomic axes of the femur and tibia on their lateral surfaces.
Data Analyses
The specimens were distributed between PCL repair without tenodesis and with tenodesis using intentional nonprobabilistic sampling in a homogeneous manner. For descriptive statistical analysis, the Kolmogorov-Smirnov test was employed to assess the normality of the data distribution. The results are expressed using measures of central tendency (mean) and dispersion (standard deviation). For the inferential analysis, a repeated-measures analysis of variance (ANOVA) was applied, with a significance level set at P < .05. To assess intraobserver and interobserver reliability, 3 trained observers were selected. Each observer independently performed repeated measurements of the variables of interest on 3 consecutive occasions. For each variable, the average of the 3 measurements was used as the representative value for each observer to reduce random measurement error and improve precision.
The intraclass correlation coefficient (ICC) was calculated for continuous variables using a 2-way mixed-effects model with absolute agreement. An ICC value ≥0.75 was considered indicative of good reliability. It is based on the classification proposed by Cicchetti, 17 which categorizes ICC values as follows:
<0.40 = poor
0.40-0.59 = fair
0.60-0.74 = good
≥0.75 = excellent
All analyses were performed using IBM SPSS Statistics, version 25 (2020). 33
Results
No specimen was excluded, which resulted in all 24 tested knees being available for final analysis. In the control group (group A), PTT measured 2.1 ± 0.5 mm at 30° of knee flexion and 3.5 ± 0.6 mm at 90°, while ER was –12.2°± 1.5 at 30° and –13.2°± 1.6 at 90°.
Posterior Tibial Translation
The PTT increased significantly in knees with PCL deficiency compared with the control group. At 30° of knee flexion, group C (PCL-deficient) showed a mean PTT of 6.8 ± 0.8 mm, while it was 2.1 ± 0.5 mm in the control group (group A) (P < .001). At 90°, the difference was even more pronounced, with values of 10.1 ± 1.2 mm in group C versus 3.5 ± 0.6 mm in group A (P < .001). Group D (PCL-PLC deficient) showed similar values (6.9 ± 0.7 mm at 30°, 10.3 ± 0.8 mm at 90°), indicating that PLC injury does not further increase posterior tibial displacement when the PCL is already deficient.
In contrast, the isolated PLC deficiency group (group B) did not demonstrate significant changes in posterior translation compared with the controls (2.7 ± 0.4 mm at 30°, 3.7 ± 0.8 mm at 90°; P > .05). This finding suggests that the PLC plays a limited role in posterior stabilization of the tibia.
In the SB PCL reconstruction group (group C2), PTT was reduced to 3.2 ± 0.6 mm at 30° and 4.2 ± 0.7 mm at 90° (P < .001 vs control), while the DB PCL reconstruction group (group C3) saw better results (2.8 ± 0.3 mm and 3.7 ± 0.5 mm), with no significant difference from the control group (P > .05). In combined PCL-PLC injury scenarios, reconstruction without addressing the PLC (group D2 and D3) led to residual posterior laxity. However, the addition of PLT in groups D4 and D5 significantly reduced PTT to values statistically indistinguishable from the intact knee. Group D5 (PCL-PLC + DB + PLT) reached 1.9 ± 0.6 mm at 30° and 3.2 ± 0.3 mm at 90°, indicating successful restoration of posterior stability (Table 1).
Changes in Posterior Tibial Translation by Groups at 30° and 90° of Flexion a

Values are presented as mean ± standard deviation. DB, double-bundle; PCL, posterior cruciate ligament; PLC, posterolateral corner; PLT, posterolateral tenodesis; PTT, posterior tibial translation; SB, single-bundle.
External Rotation
The ER was significantly affected by injuries to both the PLC and PCL. Group B (PLC-deficient) showed a substantial increase in ER compared to the control group, with values of –25.4°± 0.4° at 30° and –27.0°± 0.8° at 90° versus –12.2°± 1.5° and –13.2°± 1.6° in the control group (P < .001). The PCL deficiency alone group (group C) also had an increased ER (–17.3°± 0.8° at 30°, –19.1°± 1.2° at 90°; P < .001), although to a lesser extent than PLC deficiency. The combined injury group (group D) exhibited the greatest rotational laxity, with ER reaching –27.3°± 0.7° and –30.4°± 0.8° (P < .001 vs control).
PCL reconstruction alone partially restored rotational control. The DB technique group (group C3) had an improved ER of –14.9°± 0.3° at 30° and –16.1°± 0.5° at 90°, while the SB technique group (group C2) reached –16.4°± 0.5° and –17.2°± 0.7°. However, reconstruction without PLC repair (groups D2 and D3) failed to restore normal rotation in cases of combined PCL-PLC deficiency, with residual values still significantly higher than those of controls.
The addition of PLT markedly improved outcomes. Group D5 (PCL-PLC + DB + PLT) showed ER values of –11.8°± 0.6° at 30° and –12.5°± 0.3° at 90°, statistically comparable to the control group (P > .05) (Table 2).
Changes in External Rotation by Group at 30° and 90° of Knee Flexion a
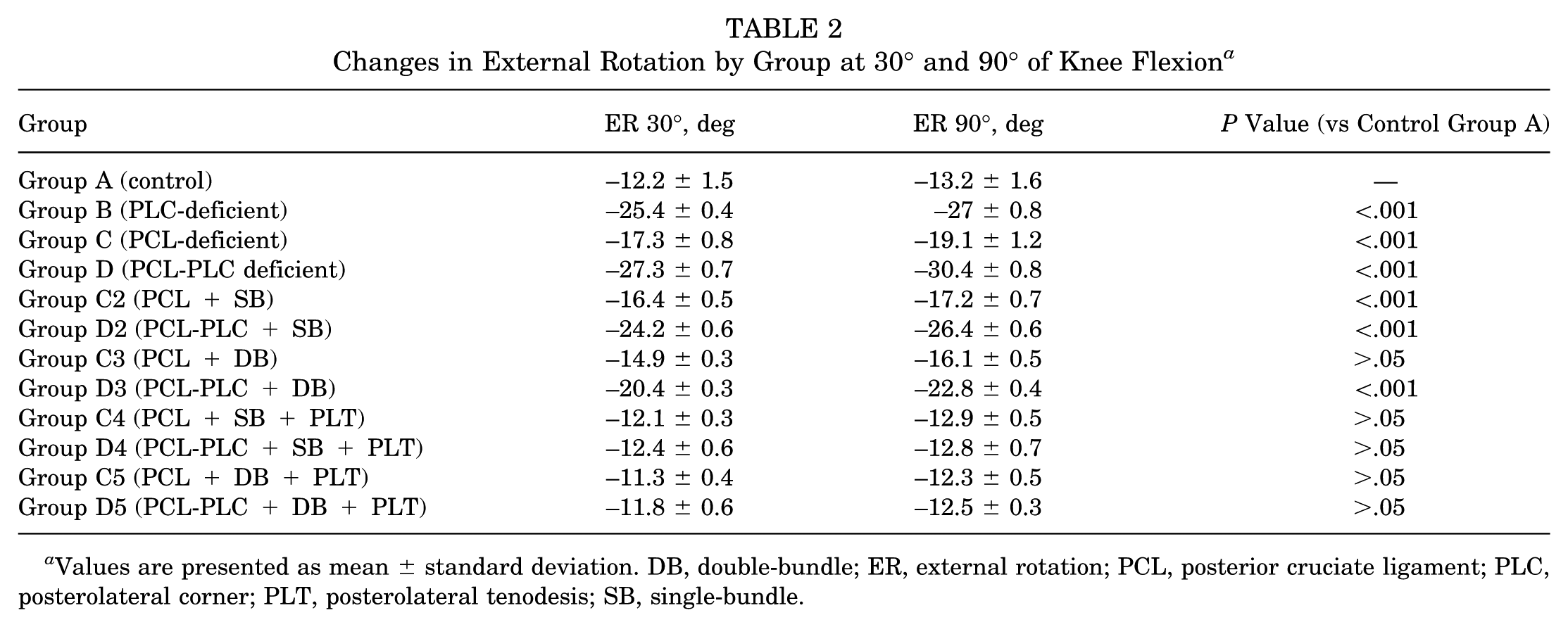
Values are presented as mean ± standard deviation. DB, double-bundle; ER, external rotation; PCL, posterior cruciate ligament; PLC, posterolateral corner; PLT, posterolateral tenodesis; SB, single-bundle.
Interobserver and Intraobserver Reliability
Intraobserver consistency yielded an ICC of 0.91 (95% CI, 0.87-0.95), while interobserver agreement reached 0.88 (95% CI, 0.83-0.92), indicating excellent reliability. These results confirm that both ER and PTT measurements were performed consistently and reproducibly across evaluators.
Discussion
The primary finding of our study lies in the significant role the PCL plays in controlling ER, not only PTT. Sectioning of the PCL led to a measurable increase in ER, which was further exacerbated when the PLC was also deficient. While both SB and DB PCL reconstructions improved stability, neither technique alone was able to fully restore native ER values in combined PCL-PLC injuries. Only when a PLT was added (regardless of whether SB or DB PCL reconstruction was performed) were ER values restored to levels comparable to the intact knee. This highlights the key role of the PLC in rotational stability and the importance of addressing it surgically in combined injury patterns, as residual posterior instability and ER are challenges that the surgeon faces during the postoperative follow-up.16,40,42
Since this is a new technique, there are no similar studies in the literature to date. However, comparable techniques describe DB reconstruction as a proposal to improve stability in PCL reconstruction, as it is more effective than SB reconstruction in controlling posterior stability. 40
In a meta-analysis conducted by Lee et al 40 in 2012, 10 studies on the biomechanical properties of the knee after PCL reconstruction were compared. They evaluated the SB technique versus the DB technique. The results concluded that DB reconstruction offers better outcomes in terms of posterior stability, although there were no significant differences in the evaluation of ER between both techniques.
On the other hand, Apsingi et al 6 conducted a biomechanical study with 10 fresh-frozen knees, with a mean age of 78 years. In it, the effects of a DB reconstruction using cadaveric tendon-bone-tendon grafts were measured. Subsequently, the study was converted into an SB reconstruction by cutting the PM bundle. No statistically significant differences in PTT were found between the 2 techniques. Regarding ER, PCL sectioning produced a measurable increase. However, it was not greater than the PCL sectioning, suggesting that the PLC is responsible for stability in ER. These findings emphasize the need for addressing PLC structures in the surgical management of combined injuries to fully restore rotational stability.
Our study presents a lower mean age than 5 of the 10 studies included in the Lee et al 40 meta-analysis. We also evaluated a larger number of samples than 8 of the 10 studies in the meta-analysis, as well as those in Apsingi et al. 6 Contrary to previous studies, our findings demonstrate that adding tenodesis to SB PCL reconstruction significantly improves both PTT and ER, with values comparable to the control group. This result is particularly relevant, as previous studies failed to demonstrate a similar improvement in ER stability. The technique proposed in our study not only addresses PTT but also provides an effective solution for ER instability—a benefit that conventional SB and DB techniques have not been able to satisfactorily resolve.
There is a complete lack of evidence regarding the surgical management of low-grade PLC injuries such as Fanelli type A lesions. Our findings provide the initial evidence that even these low-grade injuries can result in increased external tibial rotation, highlighting their biomechanical relevance. Moreover, the use of a PLT technique may offer a viable surgical option to address this rotational instability.
To date, multiple reconstruction techniques have been described to address PLC instability of the knee. They include tibiofibular- and fibular-based procedures aimed at restoring native posterolateral structures. Chahla et al 13 introduced the tibiofibular-based technique to reconstruct the lateral collateral ligament (LCL), the popliteal tendon, and PFL, which are important structures of the PLC. Anatomic reconstructions of the PLC commonly aim to restore the PT and PFL to address varus and rotational instability. The tibiofibular-based technique seems to be advantageous since it allows for anatomic reconstruction of the 3 important structures. These techniques have been primarily described for higher-grade posterolateral injuries, whereas their role in lower-grade lateral-sided deficiency remains less clearly defined. The present study focused on Fanelli type A lateral collateral ligament injuries associated with PCL deficiency, a clinical scenario in which complete anatomic reconstruction of the posterolateral structures may not be routinely required. In this context, the proposed posterolateral tenodesis demonstrated a targeted stabilizing role that may complement PCL reconstruction without the added complexity of reconstructing the PT or PFL.
While tibiofibular-based reconstructions attempt an anatomic restoration of the PLC, they are technically demanding and may not be necessary in all injury patterns. In contrast, the proposed posterolateral tenodesis represents a technically simpler procedure that may provide meaningful rotational restraint. Moreover, this technique could be considered an adjunct to fibular-based reconstructions, with the potential to enhance rotational control without the need for additional anatomic reconstruction.
The PLT technique described by Alvarez-Salinas et al 4 has not yet been supported by published clinical outcome series. Consequently, its clinical effectiveness remains to be determined, and further clinical studies are required to validate its role as an adjunct to PCL reconstruction.
Vogrin et al, 56 in a biomechanical study, described the restrictive function of the PCL in ER. They observed a significant increase in ER after ligament sectioning, with the greatest rotational instability occurring at 30°. These results contrast with our findings, where maximum instability was observed at 90°.
In terms of techniques, Grotting et al 30 conducted a biomechanical study with 11 fresh-frozen cadaveric legs with a mean age of 63 years to compare knee biomechanics after reconstruction with the “all-inside” technique versus the transtibial technique. PCL sectioning did not significantly alter the degree of ER at any angle, and rotational trends were like the intact state. The mean ER peaked at 90° of flexion but was not significantly different from that of the intact state. The “all-inside” reconstruction improved PTT compared with the transtibial technique, although it did not reach intact state levels. In comparison, our technique with the addition of PLT reduced PTT and ER values to native levels.
This suggests that the PLT effectively complements PCL reconstruction and improves overall joint stability. The addition of an extra-articular reinforcement has been previously validated in ACL reconstruction and has shown favorable results for rotational stability.31,47 However, its application in PCL surgery is still an emerging research area with limited available literature.
Our findings suggest that the PLT contributes to reducing both PTT and external tibial rotation and may provide support in the management of low-grade PLC injuries. Further clinical trials are necessary to assess the impact of PLT on functional outcomes, as well as efforts to improve the clinical scoring systems and postoperative recovery.
Based on the biomechanical findings reported in the present study, future investigations should focus on direct biomechanical comparisons between posterolateral tenodesis and different PLC reconstruction techniques. Such studies may further clarify the relative contributions of various posterolateral stabilization strategies and help more precisely define the indications for each technique.
Study Limitations
This study had some limitations. As a cadaveric model, it is not possible to evaluate graft healing and remodeling over time. The use of Thiel-embalmed specimens instead of fresh-frozen cadavers was also a limitation. However, this method was chosen to comply with local biosafety and legal regulations within our country, while maintaining a high degree of joint flexibility and realistic tissue handling. Previous studies have supported the suitability of Thiel-embalmed tissues for biomechanical investigations involving joint kinematics.25,57
An a priori sample size calculation was not performed, and the number of specimens included in the study was determined by the availability of cadaveric knee specimens. The sample size was therefore limited by specimen availability, which might be a factor that affects the generalization of the results. Although a standardized protocol was used for graft preparation and fixation, technical variations could influence the observed results. Furthermore, porcine ligament allografts were used, which, while providing consistency in graft properties across groups, may not fully replicate the biological and biomechanical characteristics of human tissue.
Recommendations for Future Research
Future research might focus on evaluating the clinical and functional effects of combining PCL reconstruction with PLT in clinical studies, as well as comparing different graft configurations and fixation techniques. Long-term follow-up studies may also provide valuable information on the durability and sustained efficacy of this surgical strategy. An important strength of our study is its pioneering nature in the biomechanical analysis of this new technique. It has shown promising results in terms of postoperative stability after PCL reconstruction. While the proposed combined PCL reconstruction and PLT technique has been demonstrated to be biomechanically efficient in controlling both the posterior drawer test and excessive tibial ER, more clinical research with adequate follow-up is necessary to completely rule out any adverse effect on the knee joint.
Conclusion
Sectioning of the PCL and PLC significantly increased both ER and PTT when compared to the control group (native stability). An isolated injury to the PLC resulted in a marked increase in ER but did not affect PTT. In contrast, an isolated PCL injury led to both increased ER and a notable increase in PTT.
The addition of PLT significantly improved ER control by providing greater rotational stability than the standard isolated SB and DB techniques. While its effect on PTT was less pronounced, rotational stability was notably increased, with values lower than those of the nontenodesis groups.
Footnotes
Acknowledgements
The authors thank The Knee Society for their support with a grant that covered part of the financial expenses related to this research.
Final revision submitted March 8, 2026; accepted March 14, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was awarded the Knee Society’s 2024 Research Grant (registration number GRANT ID#: 01-2024) by The Knee Society's Research Committee.
Ethical approval for this study was obtained from the Institutional Review Board and Research Ethics Committee of the University Hospital of the Universidad Autónoma de Nuevo Leon (registration number #FI23-00001).