
Abstract
Background:
Anterior cruciate ligament (ACL) injuries are among the most common sports-related injuries worldwide. Primary ACL reconstruction (PACLR) is the standard treatment, but graft failure may necessitate revision ACLR (RACLR). Even though RACLR restores knee stability, outcomes such as return to sport (RTS) and patient-reported measures are thought to be inferior compared with PACLR. While RACLR is widely recognized as resulting in inferior clinical outcomes compared with PACLR, there remains a need for an updated, head-to-head meta-analysis to precisely quantify the magnitude of these disparities in terms of RTS and specific patient-reported outcomes (PROs) across larger patient populations.
Purpose/Hypothesis:
This study aimed to compare RTS and PROs between PACLR and RACLR. It was hypothesized that RACLR would result in significantly lower RTS rates and inferior PROs compared with PACLR.
Study Design:
Systematic review; Level of evidence, 3.
Methods:
A systematic search was conducted in PubMed and Cochrane Library (August 26, 2025) using terms related to “primary,”“revision,”“anterior cruciate ligament,”“reconstruction,” and “outcome.” Inclusion criteria included (1) comparative studies between PACLR and RACLR, (2) reporting of RTS or PROs through outcome measures (subjective International Knee Documentation Committee [IKDC], Knee injury and Osteoarthritis Outcome Score [KOOS], Lysholm, and Tegner), and (3) randomized controlled trials, cohort, cross-sectional, or case-control studies. Exclusion criteria comprised duplicates, reviews, case reports, abstracts, or letters. Two independent reviewers performed study selection, data extraction, and quality assessment using the Newcastle-Ottawa Scale and Joanna Briggs Institute checklist. Data on RTS (categorical) were analyzed using risk difference (RD) and PROs (continuous) using mean difference (MD). Random- or fixed-effects models were applied based on heterogeneity. Analyses were conducted with RevMan Web.
Results:
A total of 22 studies were included, comprising a total of 24,773 patients (22,767 PACLR and 2006 RACLR). While no significant difference was observed between groups in overall RTS rates (RD, 0.09; 95% CI, –0.02 to 0.19; P = .11), the PACLR group demonstrated significantly higher rates of returning to the same level of sports (RTS-S) compared with the RACLR group (RD, 0.17; 95% CI, 0.08 to 0.27; P = .0002). Regarding PROs, PACLR was found to be superior in all assessed metrics, including the IKDC (MD, 5.21; 95% CI, 2.41 to 8.00; P = .0003), Lysholm (MD, 4.62; 95% CI, 3.58 to 5.66; P < .00001), and Tegner activity scores (MD, 0.30; 95% CI, 0.13 to 0.48; P = .0005). Furthermore, PACLR showed significantly better results across all 5 domains of the KOOS, with the most pronounced disparities observed in the Sport and Recreation and Quality of Life subscales.
Conclusion:
Compared with PACLR, RACLR demonstrated similar overall RTS rates but significantly lower RTS-S and consistently worse PROs. While revision surgery can restore function for daily living, substantial limitations remain in sports performance and quality of life.
Keywords
Anterior cruciate ligament (ACL) injuries are very common in sports, with approximately 250,000 cases occurring annually in the United States. 27 ACL reconstruction (ACLR) is currently considered the gold standard treatment for ACL injuries and has become a very common orthopaedic procedure worldwide. However, postoperative ACL reinjury remains a potential adverse outcome for the injured population. A meta-analysis in 2016 indicated that the total ACL reinjury rate was found to be 15%, which could be affected by multiple risk factors, such as age, participating in high-risk exercise, incomplete healing, or inadequate rehabilitation. 42 For those patients whose grafts fail, a revision ACLR (RACLR) is necessary to reestablish knee stability to enable a return to daily and athletic activities while reducing the likelihood of cartilage and meniscal injuries. 25 Therefore, the level of recovery after revision surgery becomes a crucial concern for both health care professionals and patients.
In the field of sports medicine, it is a clinical consensus that RACLR generally yields less favorable results than primary ACLR (PACLR).9,10,26,44 Factors such as concomitant meniscal and chondral pathology, previous tunnel malposition, and compromised graft options contribute to the increased complexity and poorer prognosis associated with revision procedures.40,44
When it comes to assessment of surgical outcomes, the condition of return to sport (RTS) is extremely important, because the majority of surgical recipients are young individuals with regular exercise habits, who have high expectation for RTS. 39 However, only a few studies have discussed the results regarding RTS. A previous study analyzed the difference of RTS rate between primary and revision surgery, but it did not include studies that analyzed both types of surgeries simultaneously. 11
Therefore, we aim to bridge the gap in current literature by providing a robust, head-to-head comparison to clarify the functional and subjective differences between PACLR and RACLR. In this systematic review, we aim to evaluate the differences in RTS rate between primary and revision surgeries through a meta-analysis. Additionally, we plan to update patient-reported outcomes (PROs) based on previous research.10,45 Our hypothesis is that revision surgery will be inferior to primary surgery in terms of RTS and PROs.
Methods
Study Design
This systematic review with meta-analysis was performed according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines 2020. The study protocol is registered on PROSPERO (ID No. 1134578).
Search Strategy
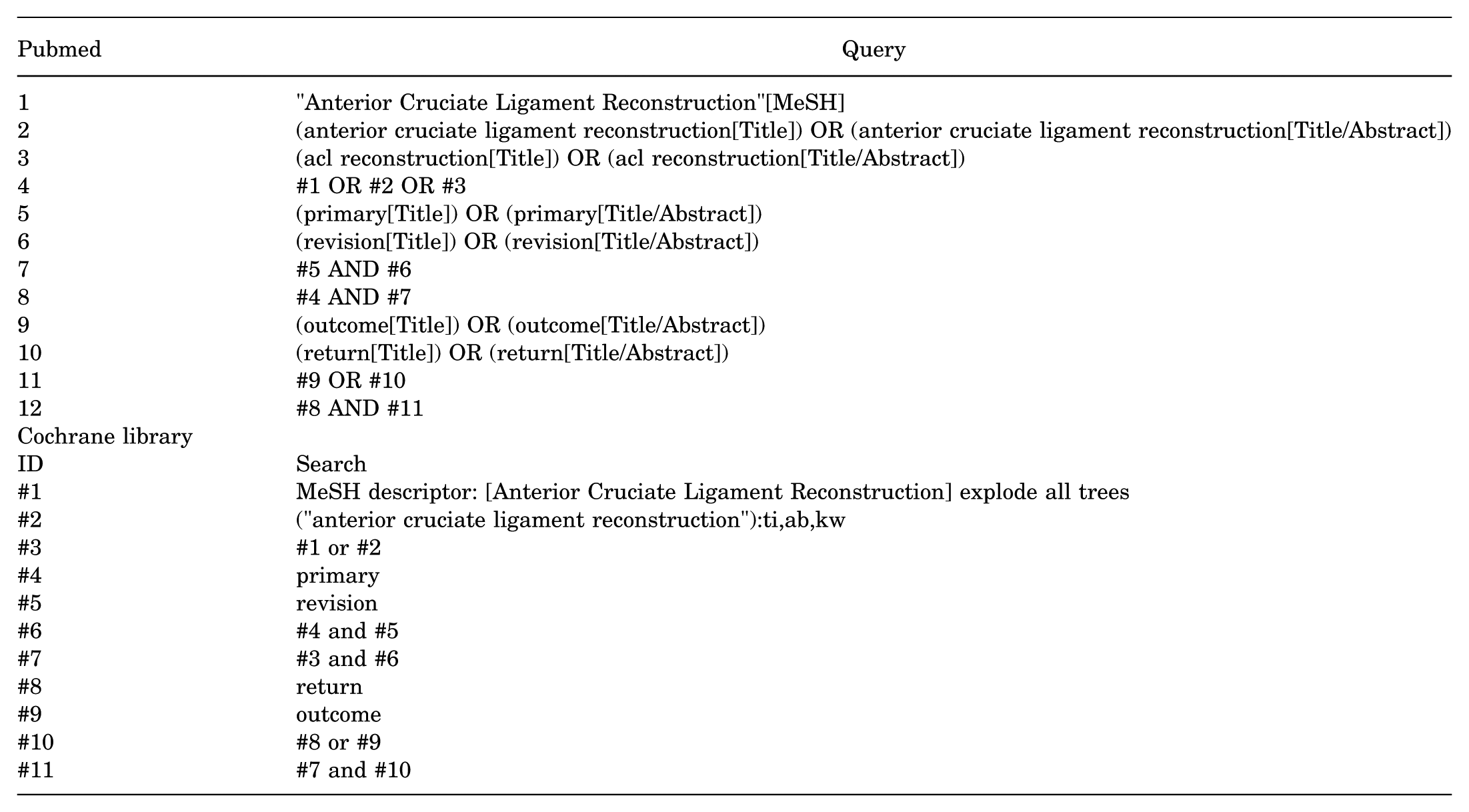
The systematic search was conducted on PubMed and Cochrane Library on August 26, 2025. Both sets of searches were performed in subject term and free term using keywords of “primary,”“revision,” anterior cruciate ligament,”“reconstruction,” and “outcome.” The details of search strategy are presented in the Appendix. Following the initial search, reference lists of the selected articles were manually searched for additional studies that might satisfy study criteria.
Inclusion and Exclusion Criteria
The final selection of included studies was based on the following criteria: (1) studies comparing the outcomes between the recipients of PACLR and those of RACLR; (2) studies reporting ≥1 of the following results: RTS rate, RTS at the same level (RTS-S) rate, or PRO measures (PROMs) including subjective International Knee Documentation Committee (IKDC), Knee injury and Osteoarthritis Outcome Score (KOOS), Lysholm Knee Scoring Scale, and Tegner Activity Scale2,3,12 (3) study designs including randomized controlled trials or cohort, cross-sectional, or case-control studies; and (4) studies published in English. We did not impose restrictions on graft types, surgical techniques, nor involvement of meniscal injury. Exclusion criteria were as follows: (1) duplicated studies, (2) studies lacking detailed data, (3) studies of review articles, case reports, conference abstracts, or letters to the editor.
Selection of Articles
All identified articles were independently reviewed by 2 authors (M.-H.S. and Y.-C.K.) based on the titles and abstracts for further screening. For those articles with potential applicability, full texts were viewed in compliance with the inclusion and exclusion criteria to identify the final target articles. When encountering disagreements, thorough discussion was had by the 2 authors to achieve a complete consensus. A third, more senior researcher (C.-P.Y.) was consulted to resolve the issue when necessary.
Quality Assessment of Included Studies
The Newcastle-Ottawa Scale (NOS) was applied to assess the methodological quality (risk of bias) of cohort studies and case-control studies of the included studies. The scale is a 9-point system, composed of the following 3 domains: selection, comparability, and outcome, each containing 3 subitems.21,33 For the assessment of cross-sectional studies, we applied the Joanna Briggs Institute (JBI) critical appraisal checklist. This tool evaluates the methodological quality of studies by examining potential biases in design, conduct, and data analysis through 8 specific criteria. 21 The assessment was conducted by the 2 authors individually, and discussion was conducted to achieve consensus when disagreements arose.
Data Extraction
Detailed information of the included studies was extracted under the following categories: (1) study information, including first author, publication year, study design; (2) patient information, including number, sex, age, follow-up period, graft, accompanied meniscal and cartilage damage; (3) clinical information, including graft selection of reconstruction, additional damage (cartilage or meniscus) if reported, and surgical techniques; (4) postsurgical RTS-related information, including the number of achievers and nonachievers of RTS or RTS-S; and (5) postsurgical PROs, including the mean and standard variation of subjective IKDC, KOOS, Tegner, and Lysholm. If the provided data didn't meet our requirements, reasonable estimation was completed through Meta-Analysis Accelerator, which was built based on the research of Abbas et al.1,38
Statistical Analysis
All data on postsurgical RTS status and PROs were collected to compare between the RACLR and PACLR groups. For RTS status, which is an item of categorical data, we collected the pooled numbers and found risk difference (RD) to conduct a comparison. On the other hand, the PROs, including subjective IKDC, KOOS, and other scores, were composed of continuous scores. Therefore, we calculated the mean difference (MD) of the 2 groups for evaluation. To minimize potential bias introduced by data transformation, a sensitivity analysis was performed afterward by excluding studies that originally reported outcomes as medians and IQRs. This analysis aimed to determine whether the pooled effect sizes remained consistent when only studies providing direct mean and standard deviation data were included, thereby ensuring the robustness of our conclusions against potential nonnormal distribution of the primary data. Statistical significance was established when the 2-sided P value was <.05. We used I2 to evaluate heterogeneity. When I2 > 50%, a random-effects model was applied to conduct a meta-analysis. On the contrary, a fixed-effects model was applied when I2 < 50%. All data were processed through Revman Web.
Sensitivity Analysis
Sensitivity analysis was performed for PROs by excluding studies that reported data as medians and IQRs to ensure the robustness of the pooled estimates derived from mean and standard deviation transformations.
Results
Study Selection
We processed the selection under the guidance of the PRISMA 2020 flowchart, and the detailed process is presented in Figure 1. At the initial search, 478 articles were identified. Among those records, 10 articles were duplicates and the remaining 468 articles were screened based on their titles and abstracts. A total of 437 articles were excluded at this stage, and the full texts of 31 articles were assessed based on the inclusion and exclusion criteria. Finally, 22 articles fulfilled the criteria and were included for meta-analysis. ‡‡
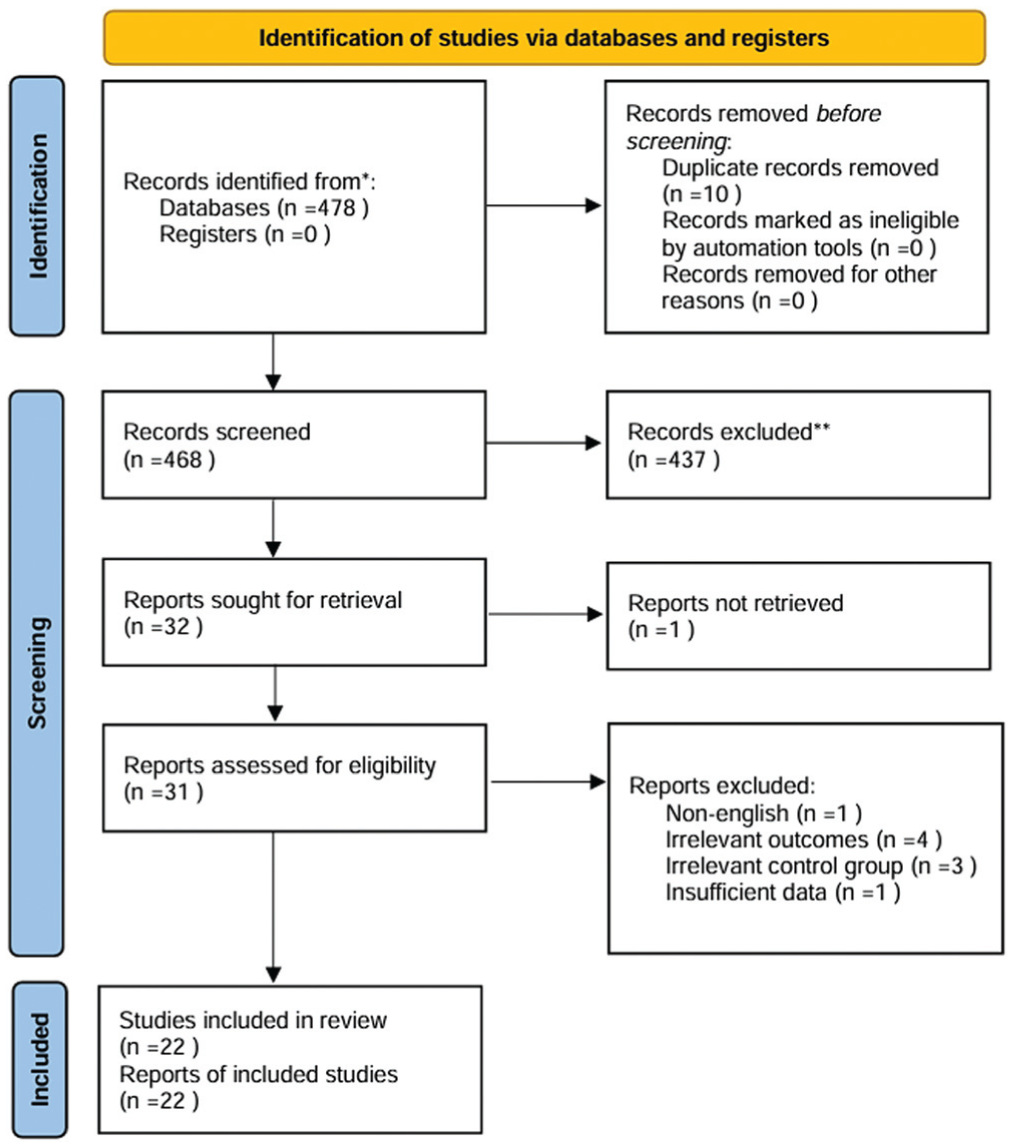
Flowchart of study selection following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.
Study Characteristics and Assessment of Risk of Bias
The characteristics of the included studies are summarized in Table 1. Among the 22 included articles, 13 were cohort studies, §§ 5 were case-control studies,8,28,29,35,36 and the remaining 4 were cross-sectional studies.15-17,22 Four studies were prospective in design,4,35,41,43 while the remaining 18 were retrospective. For the assessment of risk of bias, all studies achieved high methodological quality. The 18 cohort and case-control studies scored between 6 and 9 on the NOS scale (mean ± SD, 7.72 ± 0.83), with only 1 article receiving a score of 6, while the others scored ≥7. Among the 9 items of the NOS scale, “Comparability of cohort on basis of design or analysis” was where all the articles performed the worst. The remaining 4 cross-sectional articles, according to the JBI checklist, 1 received a score of 8, while the other 3 received a score of 7; all were deemed eligible for inclusion. The detailed information is presented in Table 2. Among all the included studies, 13 studies matched participants for primary and revision groups. In 8 studies, the number of participants in both groups was exactly the same.6,16,17,20,22,29,35,41 In 3 studies, the participant numbers were similar due to loss to follow-up or being outside the inclusion criteria.8,15,46 In 1 study, the primary-to-revision ratio was 1:2 because the authors included participants separately for 2 different types of grafts in the revision group. 14 In another study, the study design predetermined a primary-to-revision participant ratio of 2:1. 36
Detailed Quality Assessment of Included Studies Using Newcastle-Ottawa Scale
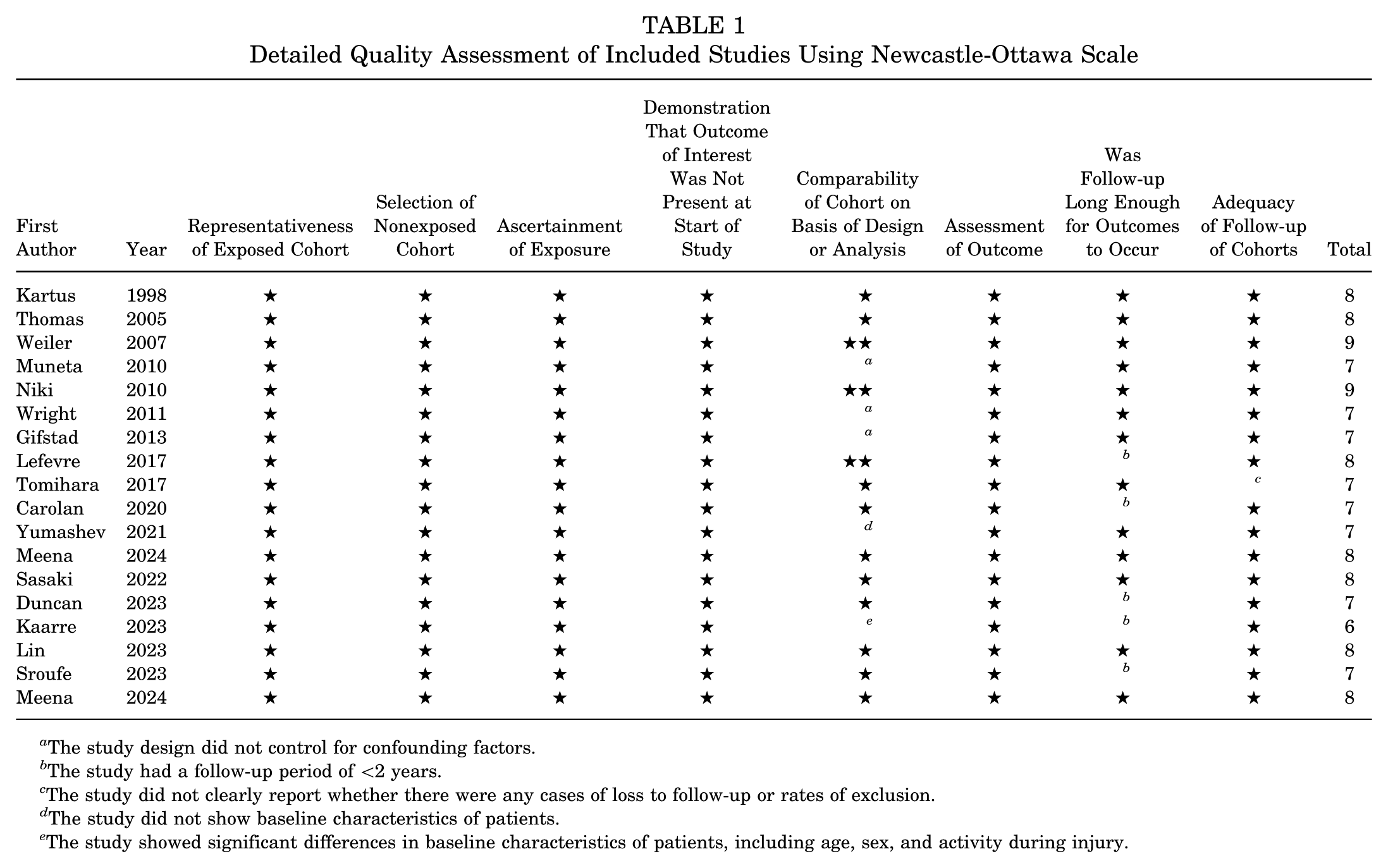
The study design did not control for confounding factors.
The study had a follow-up period of <2 years.
The study did not clearly report whether there were any cases of loss to follow-up or rates of exclusion.
The study did not show baseline characteristics of patients.
The study showed significant differences in baseline characteristics of patients, including age, sex, and activity during injury.
Detailed Quality Assessment of Included Studies Using Joanna Briggs Institute Checklist
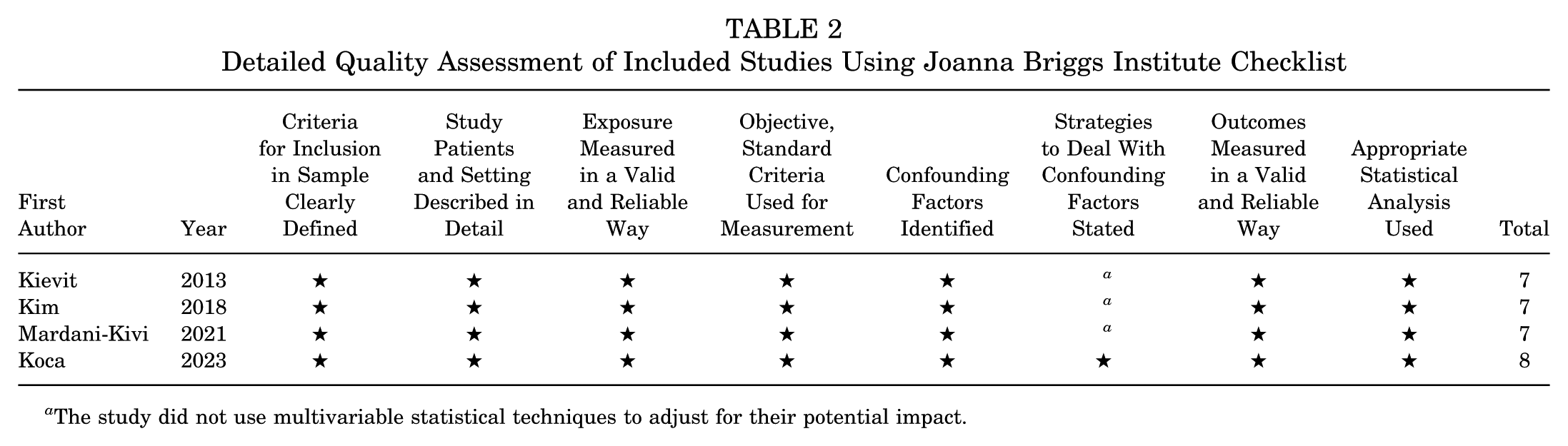
The study did not use multivariable statistical techniques to adjust for their potential impact.
Patient and Surgical Characteristics
This study analyzed a total of 24,773 individuals, comprising 22,811 who underwent PACLR and 2,032 who received RACLR. The sex distribution showed a male predominance in both groups, with male patients accounting for 54% in the PACLR group and 60% in the RACLR group. Patients in the PACLR cohort had a mean age of 29.04 years at the time of surgery, while those in the RACLR group had a mean age of 27.96 years. The mean follow-up durations for the PACLR and RACLR groups were 8.55 years and 5.31 years, respectively. Detailed information is summarized in Table 3.
Detailed Characteristics of Included Studies a
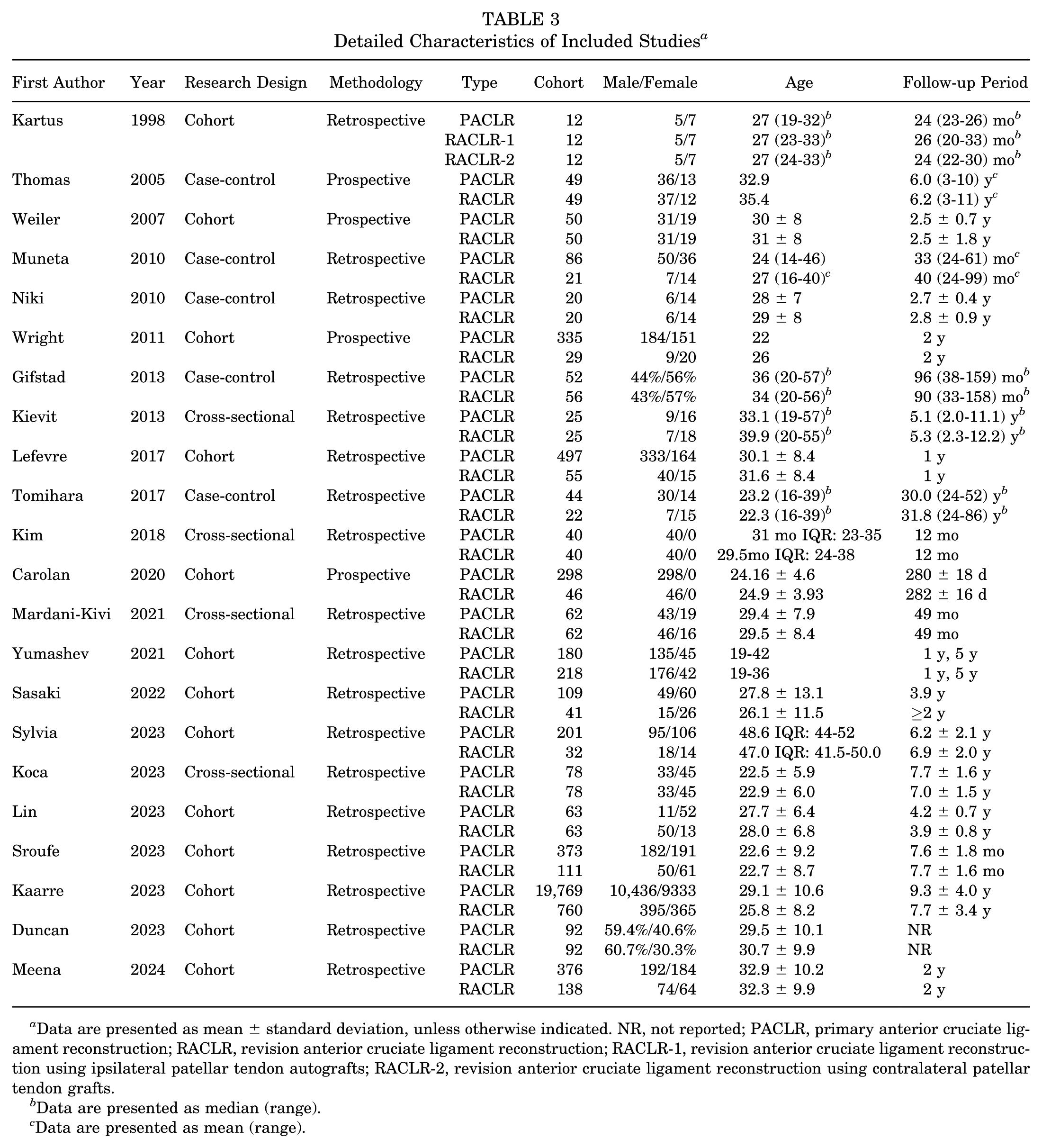
Data are presented as mean ± standard deviation, unless otherwise indicated. NR, not reported; PACLR, primary anterior cruciate ligament reconstruction; RACLR, revision anterior cruciate ligament reconstruction; RACLR-1, revision anterior cruciate ligament reconstruction using ipsilateral patellar tendon autografts; RACLR-2, revision anterior cruciate ligament reconstruction using contralateral patellar tendon grafts.
Data are presented as median (range).
Data are presented as mean (range).
In terms of surgical intervention, autograft tissue was utilized universally for PACLR cases, most frequently involving hamstring tendons, bone–patellar tendon–bone grafts, and quadriceps tendons at rates of 87.2%, 8.3%, and 2.9%, respectively. In contrast to the PACLR group, the most commonly selected graft type in the RACLR group was bone–patellar tendon–bone grafts (43.1%), followed by hamstring tendons (26.1%) and then quadriceps tendon (19.5%). In addition, allografts were more frequently utilized in the RACLR group than in the PACLR group (8.9% vs 1.2%). Detailed information is presented in Table 4. In most of the studies that reported surgical staging, the included RACLRs were performed in a single stage, ‖ ‖ with only 1 study adopting a 2-stage procedure. 35
Detailed Surgical Characteristics a
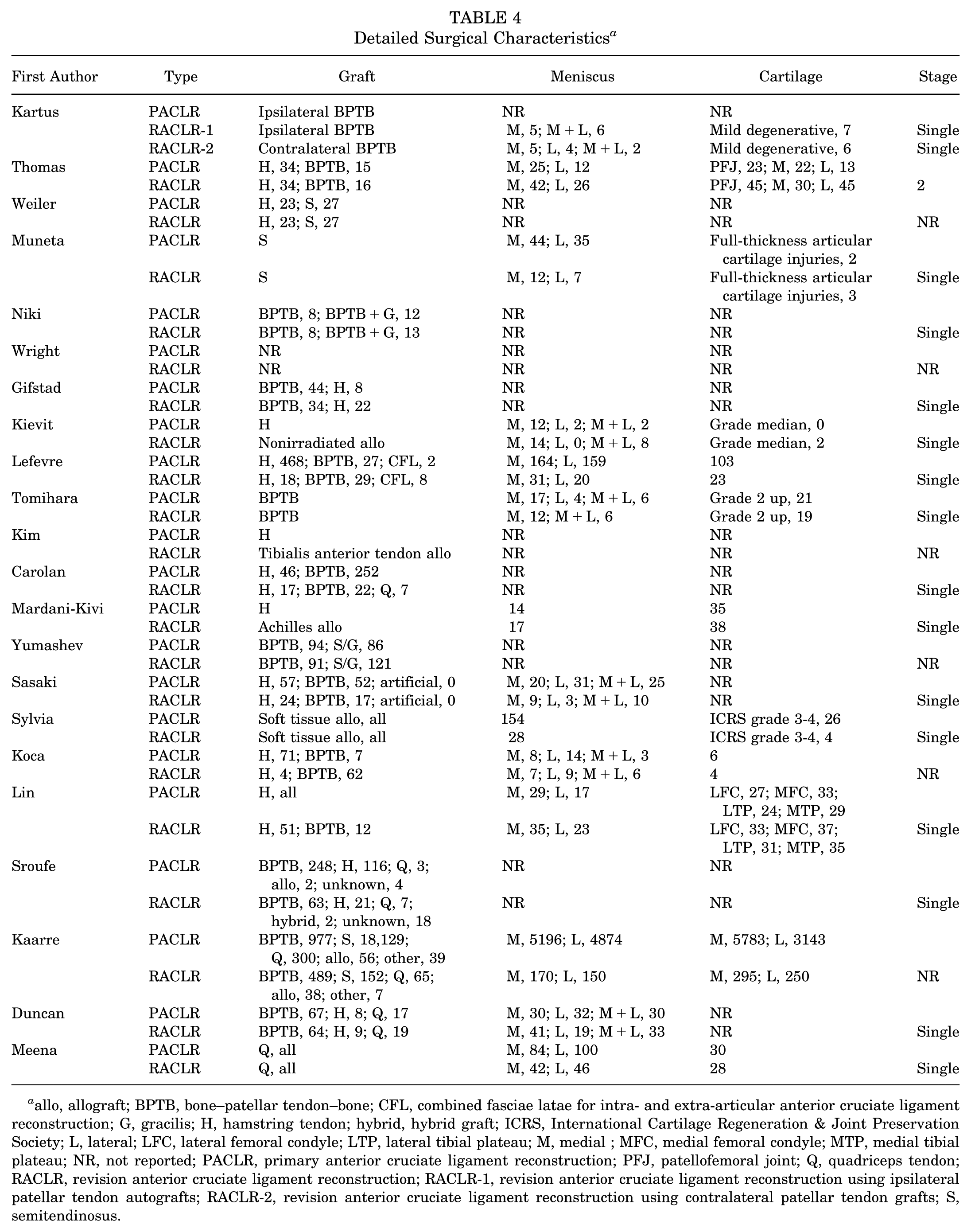
allo, allograft; BPTB, bone–patellar tendon–bone; CFL, combined fasciae latae for intra- and extra-articular anterior cruciate ligament reconstruction; G, gracilis; H, hamstring tendon; hybrid, hybrid graft; ICRS, International Cartilage Regeneration & Joint Preservation Society; L, lateral; LFC, lateral femoral condyle; LTP, lateral tibial plateau; M, medial ; MFC, medial femoral condyle; MTP, medial tibial plateau; NR, not reported; PACLR, primary anterior cruciate ligament reconstruction; PFJ, patellofemoral joint; Q, quadriceps tendon; RACLR, revision anterior cruciate ligament reconstruction; RACLR-1, revision anterior cruciate ligament reconstruction using ipsilateral patellar tendon autografts; RACLR-2, revision anterior cruciate ligament reconstruction using contralateral patellar tendon grafts; S, semitendinosus.
Meniscal pathology was frequently documented in both surgical groups. In the PACLR population with detailed records regarding meniscal status (n = 21,144), injuries to the medial meniscus occurred in 6817 cases (32.2%), while lateral meniscal damage was identified in 5280 patients (25.0%). The RACLR group with detailed record of meniscal status (n = 1348) presented with medial meniscal tears in 425 cases (31.5%) and lateral meniscal tears in 307 cases (22.8%). Statistical comparisons revealed no significant difference between the prevalence of medial meniscal injuries (χ2 = 0.27; P = .61) and lateral meniscal injuries (χ2 = 3.16; P = .08) in the 2 groups. The reporting of chondral lesions varied among studies, with some describing its location, others its severity, and some its involvement with ligaments. Consequently, these data could not be pooled for meta-analysis and are summarized qualitatively in the tables.
RTS-Related Outcomes
RTS Rates. Four studies provided statistical results on RTS with a total of 958 patients (PACLR, 700; RALCR, 258).17,19,20,22 Among these 4 studies, 2 reported that the RTS rate did not differ significantly between the primary and revision groups,17,22 while the other 2 indicated significantly higher RTS rates in the primary group.19,20 According to the extracted data, the result of meta-analysis indicated no significant difference in RTS rate between the 2 groups as shown in Figure 2 (RD, 0.09; 95% CI, –0.02 to 0.19; P = .11; I2 = 52%).
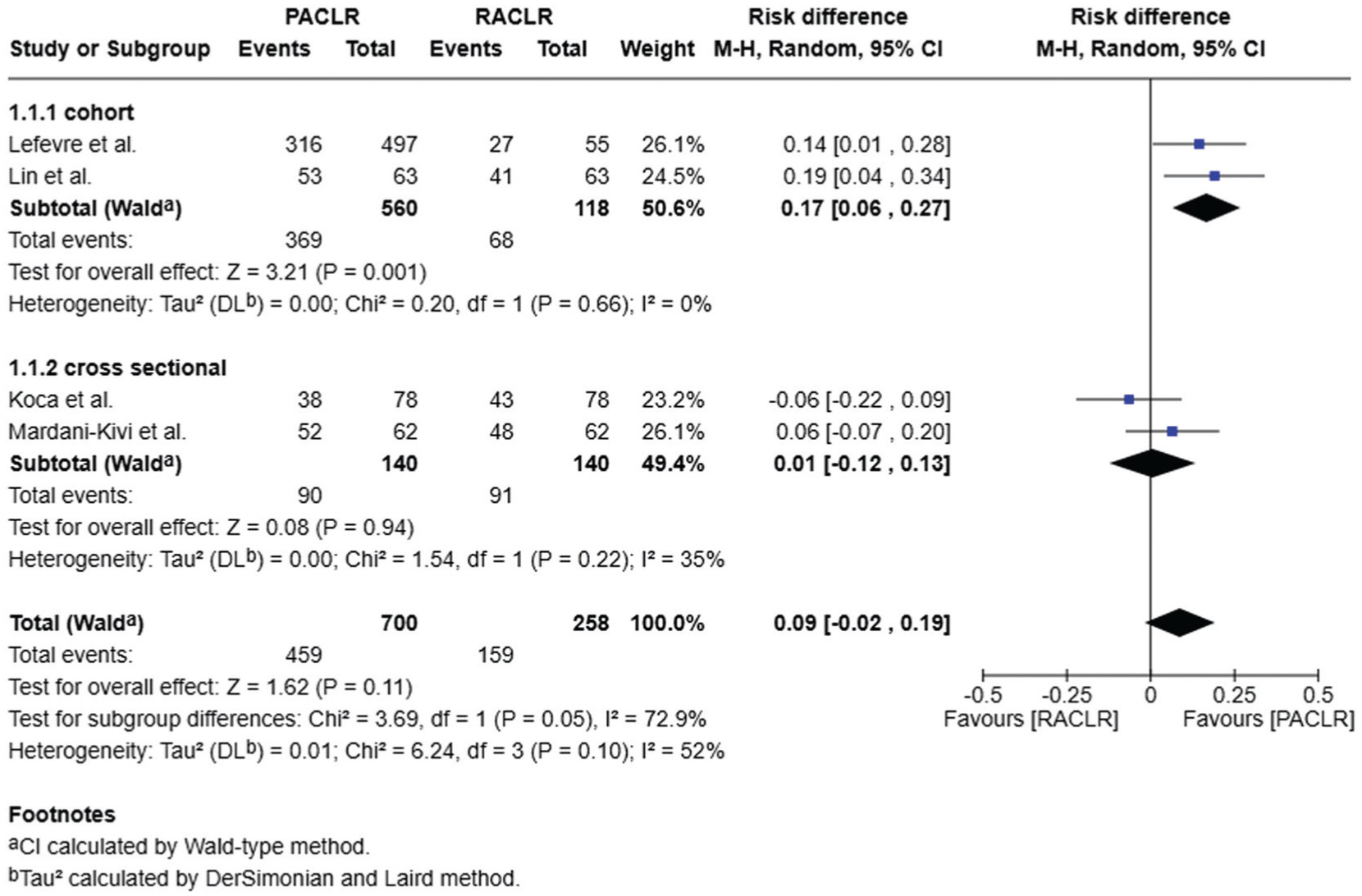
Forest plot of return-to-sport rates. M-H, Mantel-Haenszel; PACLR, primary anterior cruciate ligament reconstruction; RACLR, revision anterior cruciate ligament reconstruction.
RTS-S Rates. Six studies provided statistical results on RTS-S with a total of 1368 patients (PACLR, 1042; RACLR, 326). Among these 6 studies, 3 reported that the RTS-S rate did not differ significantly between the primary and revision groups,20,22,36 while the other 3 indicated a significantly higher RTS-S rate in the primary group.4,17,19 According to the extracted data, the meta-analysis revealed that PACLR had a significantly higher RTS-S rate compared with RACLR as shown in Figure 3 (RD, 0.17; 95% CI, 0.08-0.27; P = .0002; I2 = 53%).
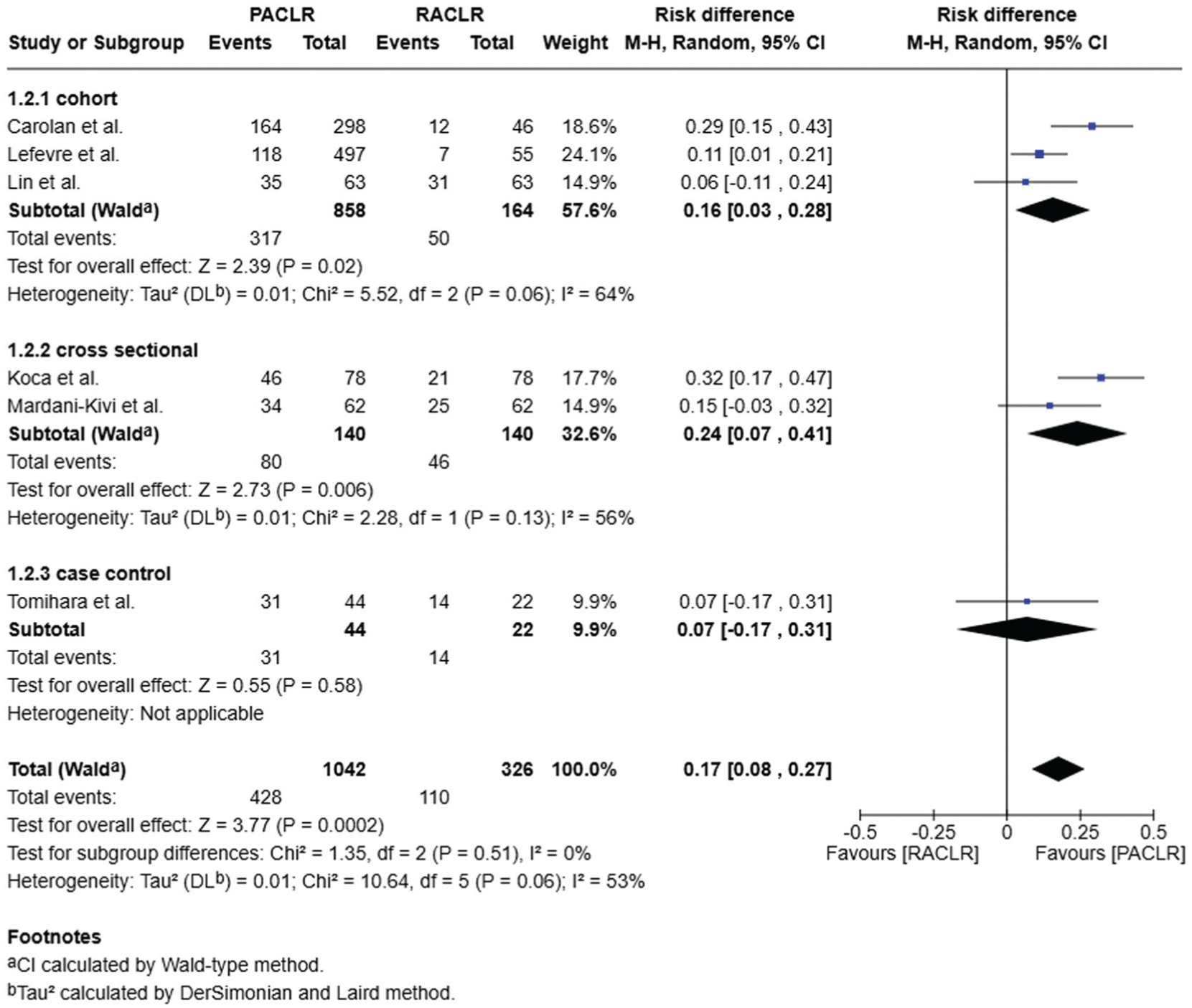
Forest plot of return to sport at the same level rates. M-H, Mantel-Haenszel; PACLR, primary anterior cruciate ligament reconstruction; RACLR, revision anterior cruciate ligament reconstruction.
PRO Measures
Subjective IKDC. Subjective IKDC is a PROM primarily used to assess an individual's subjective perception of knee joint function. 12 It consists of 3 sections: symptoms, sport activities, and function. The total score is then converted into a standardized score ranging from 0 to 100, with a higher score indicating better knee joint function. Ten studies reported relevant data for subjective IKDC, involving a total of 2816 patients (PACLR, 2120; RACLR, 696).4,6,16,19,20,32,34,35,43,46 Among the 10 studies, 6 reported that the subjective IKDC score did not differ significantly between the primary and revision groups,4,6,16,19,20,32 while the other 4 indicated significantly lower scores in the RACLR group.34,35,43,46 According to the extracted data, the meta-analysis revealed significantly lower subjective IKDC scores in the RACLR group compared with the PACLR group, as shown in Figure 4 (MD, 5.21; 95% CI, 2.41-8.00; P = .0003; I2 = 80%).
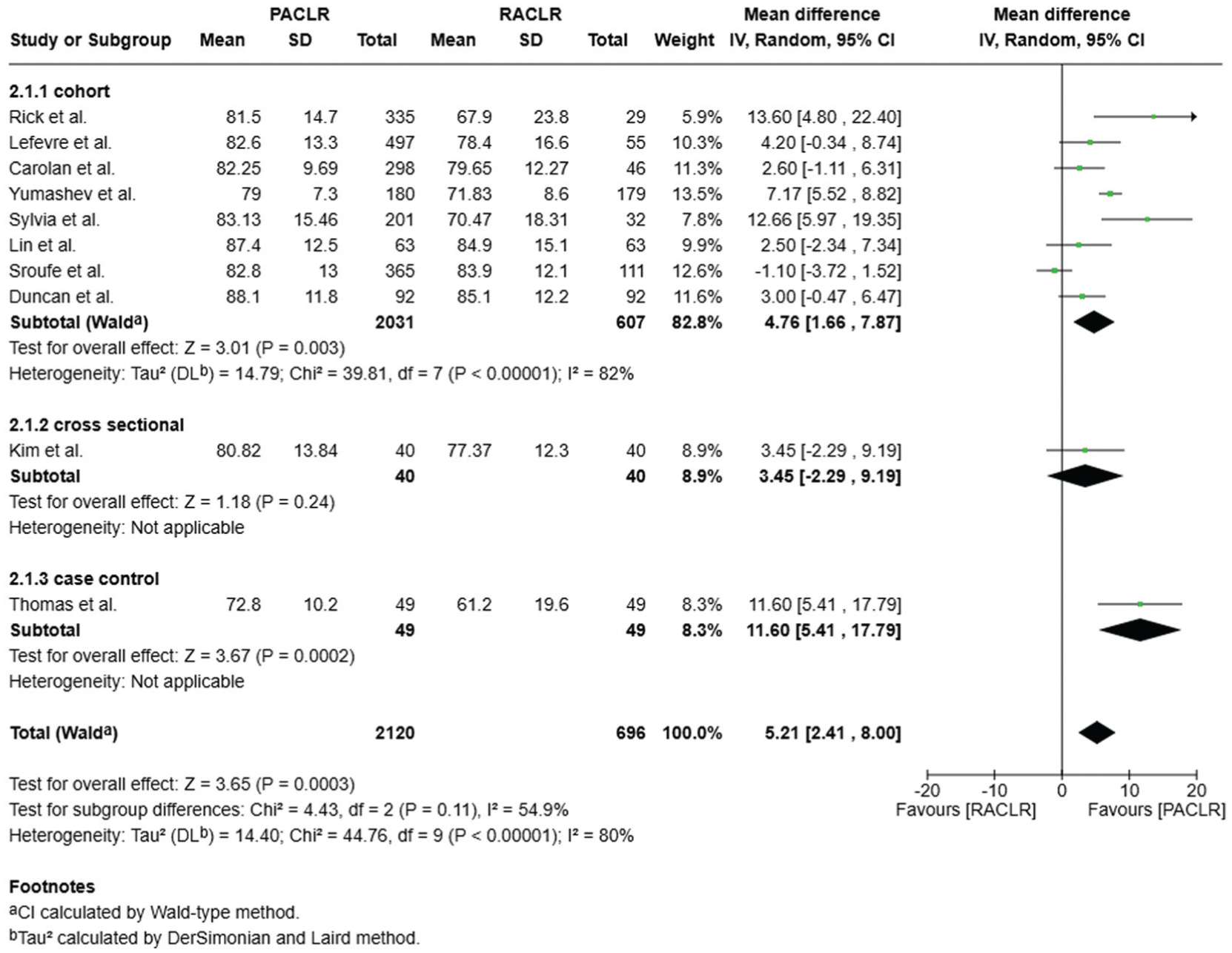
Forest plot of subjective International Knee Documentation Committee. IV, inverse variance; PACLR, primary anterior cruciate ligament reconstruction; RACLR, revision anterior cruciate ligament reconstruction.
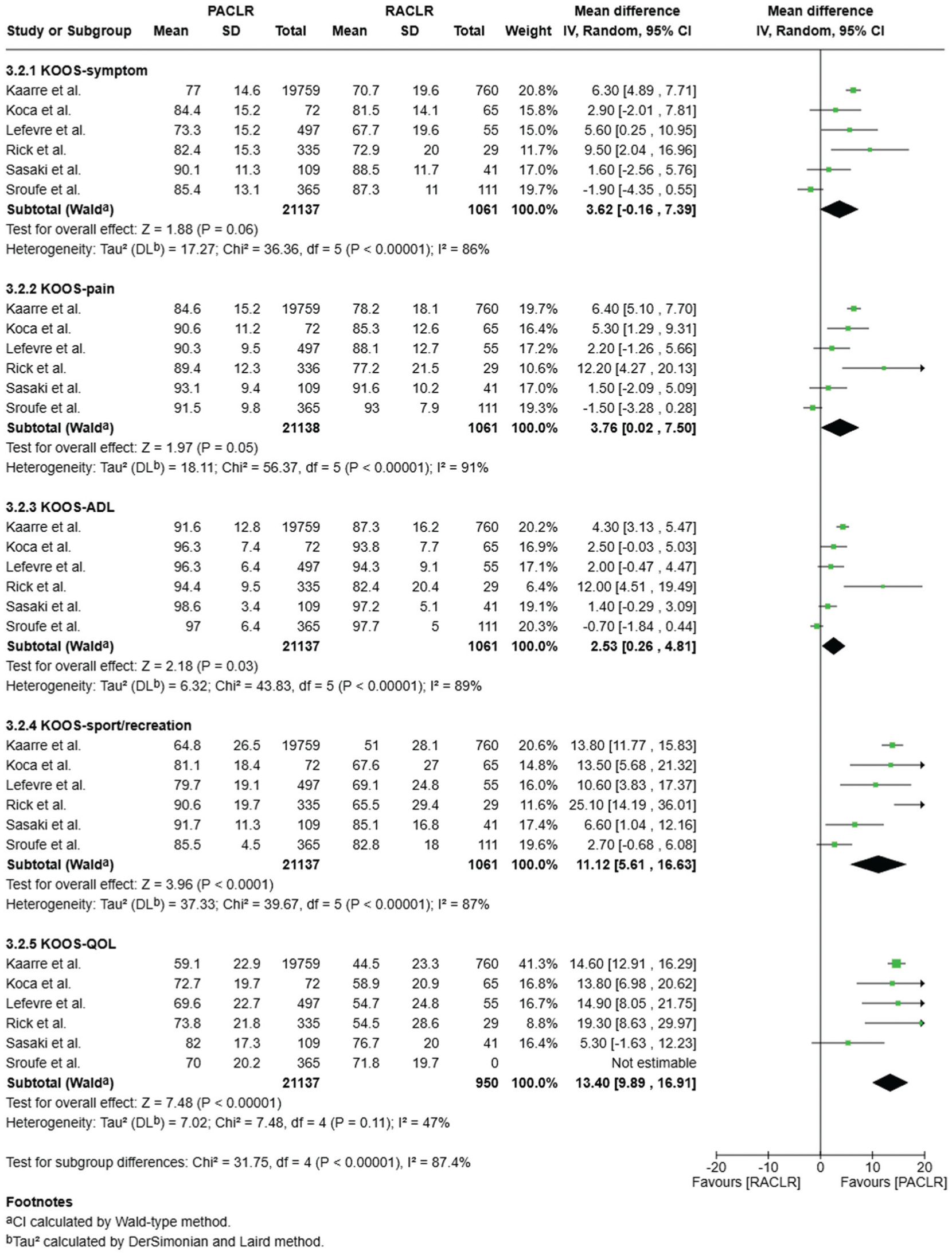
Knee Injury and Osteoarthritis Outcome Score. KOOS is a PROM containing questions in 5 domains: Pain, other Symptoms, Activities of Daily Living (ADL), function in Sport and Recreation, and knee-related Quality of Life (QOL). 2 The scores of each domain are converted into a standardized score ranging from 0 to 100 and presented separately, with lower scores indicating worse knee function. Seven studies reported relevant data for KOOS, involving a total of 22,250 patients (PACLR, 21,164; RACLR, 1086).13,15,17,19,31,32,44 According to the extracted data, the meta-analysis revealed significantly lower scores across all 5 domains in the RACLR group compared with the PACLR group. The MD in Symptoms, Pain, ADL, Sport and Recreation, and QOL were 4.68 (95% CI, 0.99-8.36), 4.66 (95% CI, 1.03-8.29), 3.52 (95% CI, 1.08, 5.96), 11.88 (95% CI, 7.30-16.45), and 11.34 (95% CI, 5.02-17.67), respectively. The detailed comparisons are shown in Figure 5.
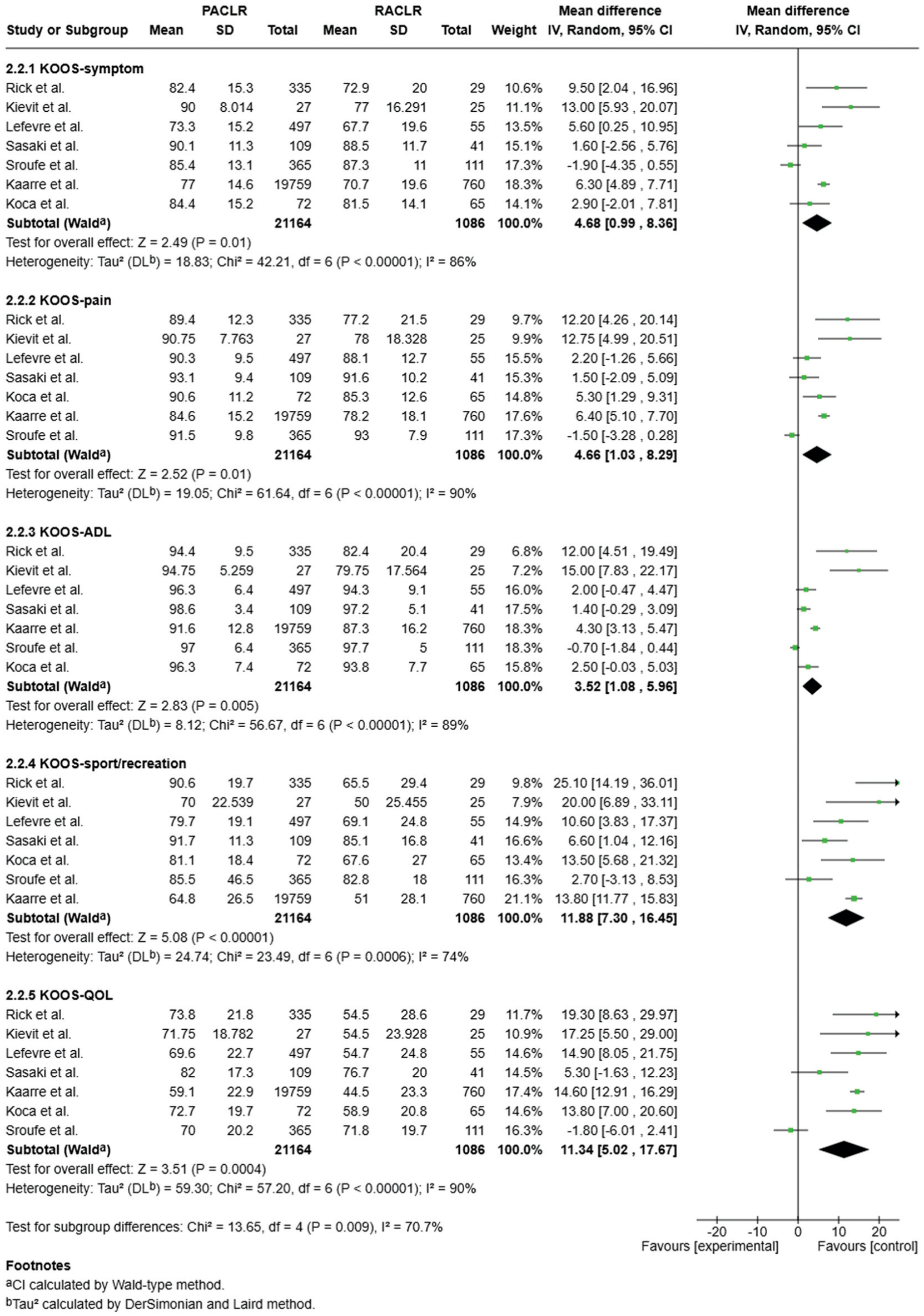
Forest plot of Knee injury and Osteoarthritis Outcome Score (KOOS). ADL, Activities of Daily Living; IV, inverse variance; PACLR, primary anterior cruciate ligament reconstruction; QOL, Quality of Life; RACLR, revision anterior cruciate ligament reconstruction.
Lysholm Knee Scoring Scale. The Lysholm scale is a patient-reported instrument comprising 8 subcomponents, including limp, support, locking, instability, pain, swelling, stair climbing, and squatting. Its raw score is 100 points, so standardization is not required, and it primarily focuses on walking and basic functions. Ten studies reported relevant data for Lysholm, involving a total of 1926 patients (PACLR, 1329; RACLR, 597).14-16,19,20,24,28,36,41,46 Among the 10 studies, 6 reported that Lysholm score did not differ significantly between the primary and revision groups,14-16,19,20,36 while the other 4 indicated significantly lower scores in the RACLR group.24,28,41,46 According to the extracted data, the meta-analysis revealed significantly lower Lysholm scores in the RACLR group compared with the PACLR group, as shown in Figure 6 (MD, 4.62; 95% CI, 3.58-5.66; P < .00001; I2 = 10%).
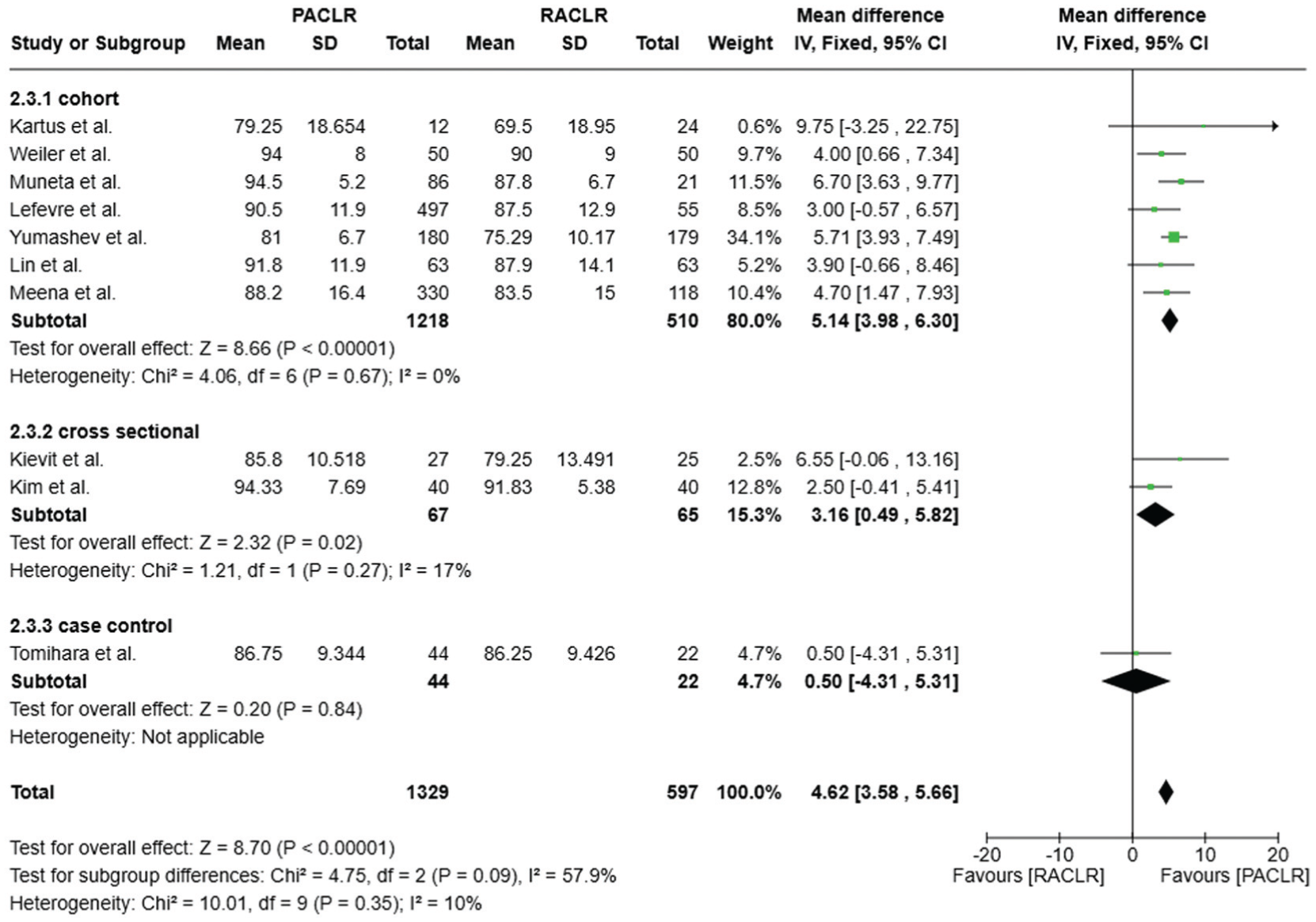
Forest plot of Lysholm Knee Scoring Scale. IV, inverse variance; PACLR, primary anterior cruciate ligament reconstruction; RACLR, revision anterior cruciate ligament reconstruction.
Tegner Activity Scale. The Tegner Activity Scale is a numerical scale with scores ranging from 0 to 10, representing the activity level of patients with knee injuries. 3 Higher scores indicate higher activity levels, where 0 represents disability or sick leave and 10 represents participation in competitive elite sports such as soccer, football, or rugby (national elite). Eleven studies reported relevant data for Tegner, involving a total of 1765 patients (PACLR, 1186; RACLR, 579). ¶¶ Among the 11 studies, 9 reported that the Tegner score did not differ significantly between the primary and revision groups, ## while the other 2 indicated significantly lower scores in the RACLR group.17,24 According to the extracted data, the meta-analysis revealed significantly lower Tegner scores in the RACLR group compared with the PACLR group, as shown in Figure 7 (MD, 0.30; 95% CI, 0.13-0.48; P = .0005; I2 = 48%).
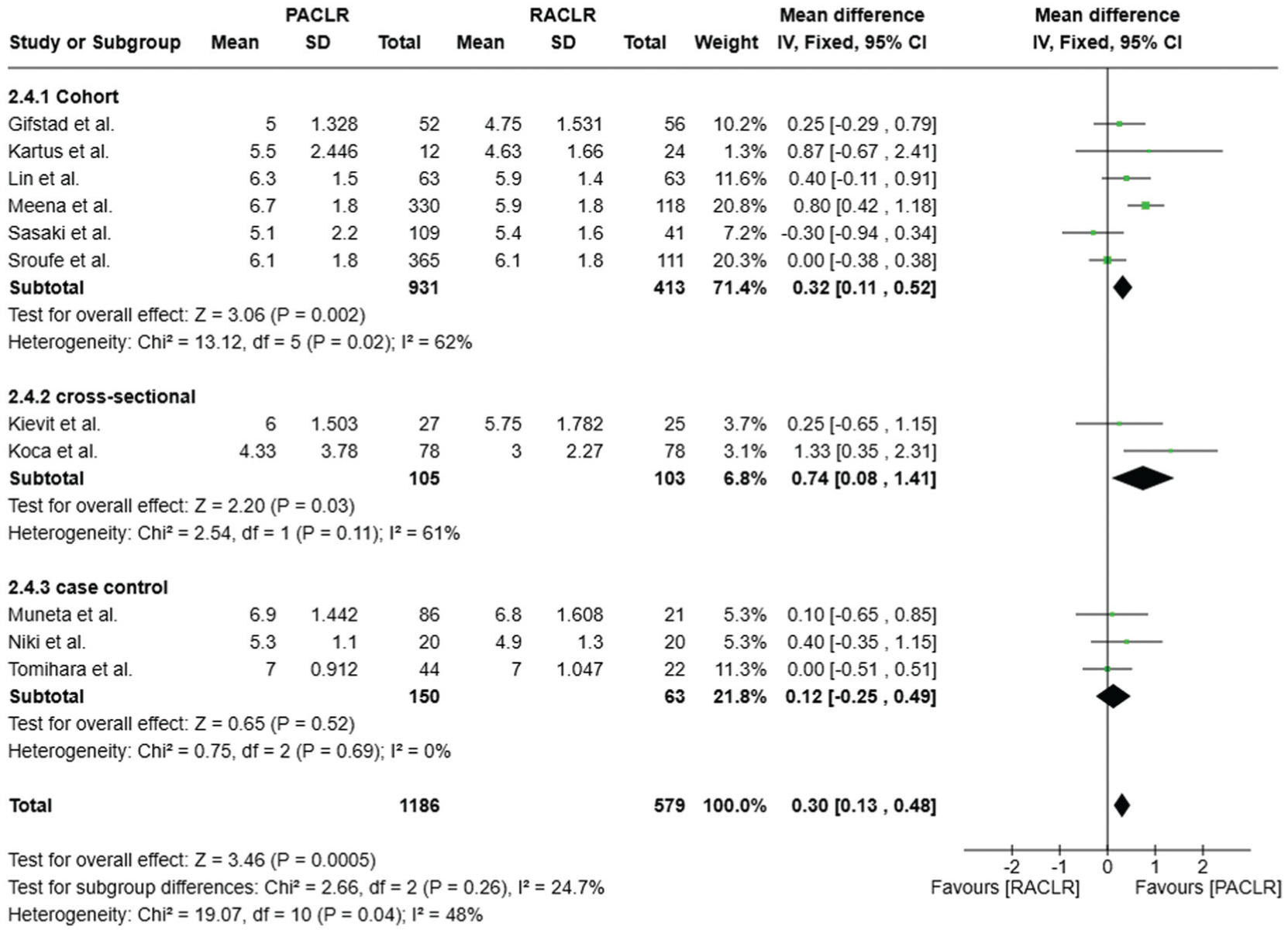
Forest plot of Tegner Activity Scale. IV, inverse variance; PACLR, primary anterior cruciate ligament reconstruction; RACLR, revision anterior cruciate ligament reconstruction.
Sensitivity Analysis
Subjective IKDC. After excluding studies that originally reported outcomes as medians and IQRs, 8 studies remained in the sensitivity analysis of subjective IKDC.4,6,19,20,32,35,43,46 Despite the adjustments, the result remained consistent with our primary finding: the results were consistent with our primary analysis, revealing significantly lower subjective IKDC scores in the RACLR group compared with the PACLR group. Details are presented in Figure 8 (MD, 4.7; 95% CI, 1.64-7.76; P = .003; I2 = 82%).
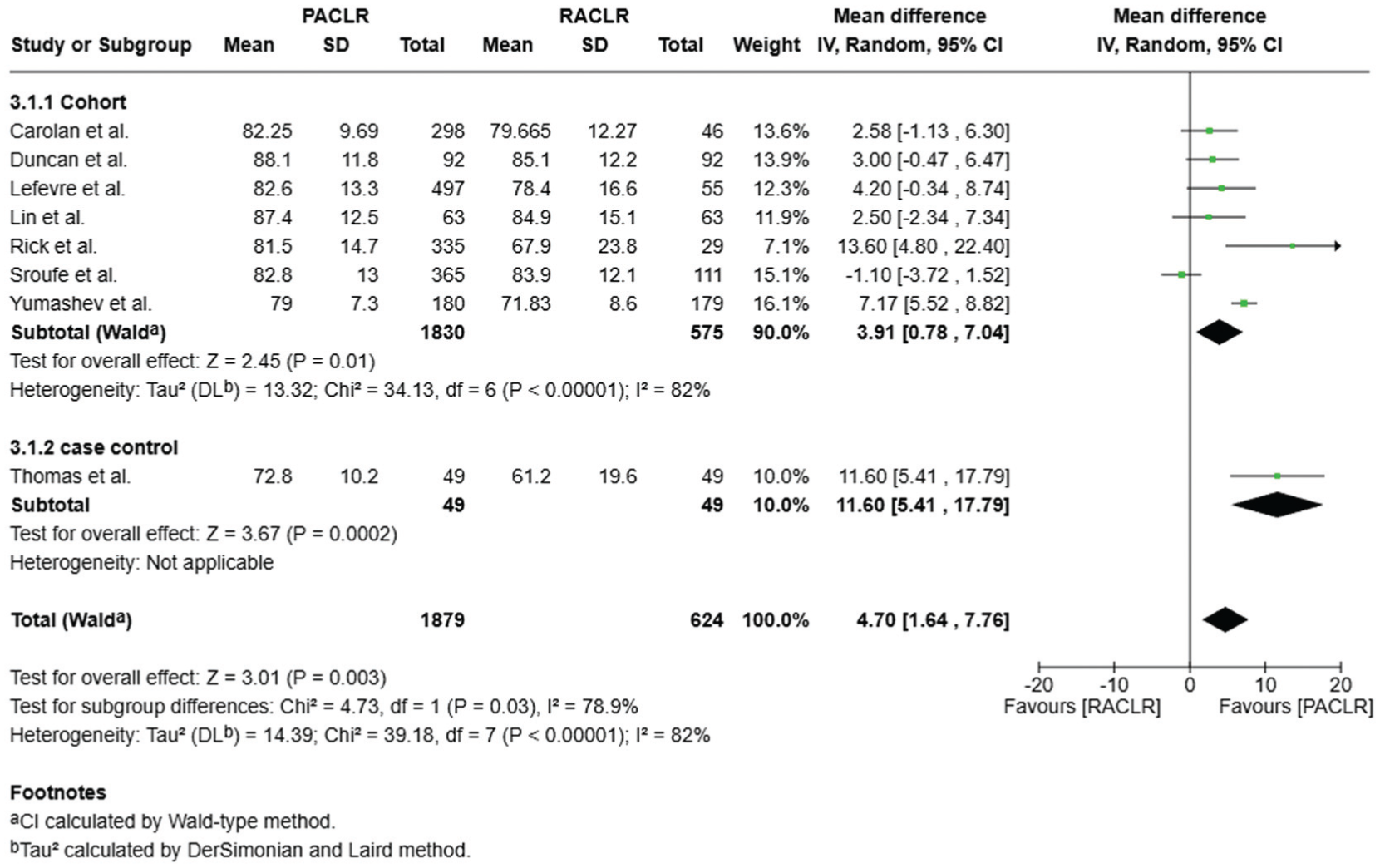
Forest plot of sensitivity analysis of subjective International Knee Documentation Committee. IV, inverse variance; PACLR, primary anterior cruciate ligament reconstruction; RACLR, revision anterior cruciate ligament reconstruction.
Knee Injury and Osteoarthritis Outcome Score. After excluding studies that originally reported outcomes as medians and IQRs, 6 studies remained in the sensitivity analysis of KOOS.13,17,19,31,32,43 After conducting the analysis, the results for the Pain domain differed from the primary analysis: pain scores showed no significant difference between the 2 groups (MD, 3.62; 95% CI, –0.16 to 7.39; P = .06), while the other domains yielded the same conclusions, with significantly lower scores in the revision group. Detailed data are presented in Figure 9.
Forest plot of sensitivity analysis of Knee injury and Osteoarthritis Outcome Score (KOOS). ADL, Activities of Daily Living; IV, inverse variance; PACLR, primary anterior cruciate ligament reconstruction; QOL, Quality of Life; RACLR, revision anterior cruciate ligament reconstruction.
Lysholm Knee Scoring Scale. After excluding studies that originally reported outcomes as medians and IQRs, 6 studies remained in the sensitivity analysis of the Lysholm scale.19,20,24,28,41,46 Despite the adjustments, the findings remained consistent with our primary analysis, indicating significantly lower Lysholm scores in the revision group compared with the primary group. Details are shown in Figure 10 (MD, 5.1; 95% CI, 3.93-6.27; P < .00001; I2 = 0%).
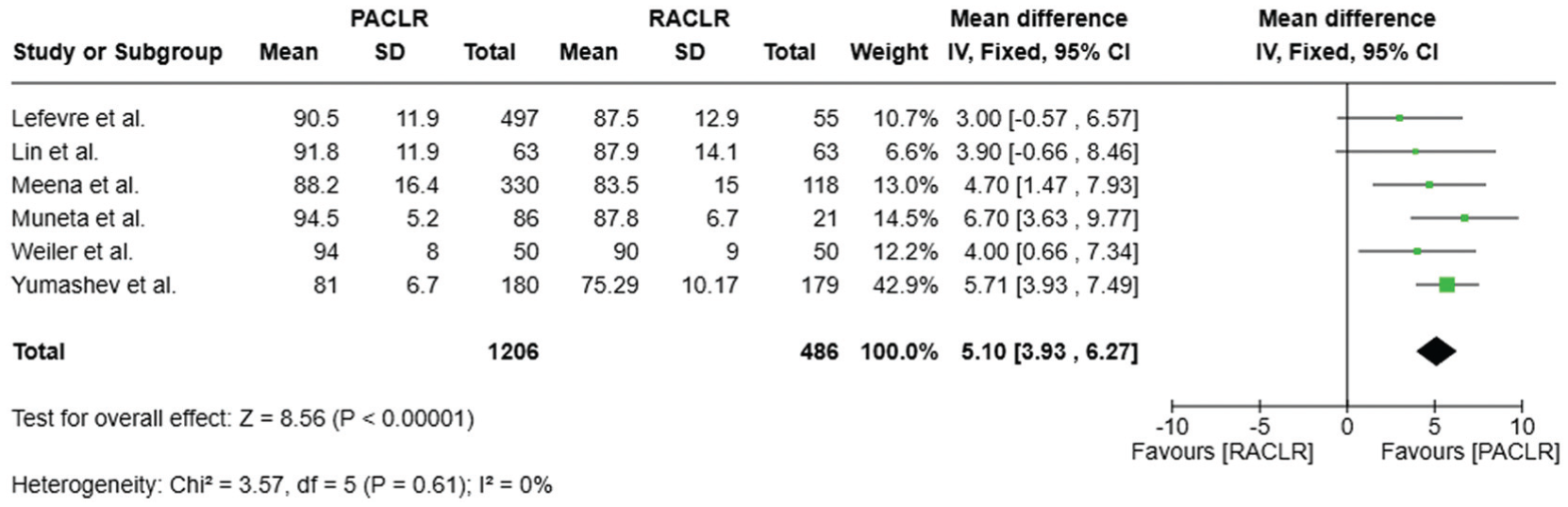
Forest plot of sensitivity analysis of Lysholm Knee Scoring Scale. IV, inverse variance; PACLR, primary anterior cruciate ligament reconstruction; RACLR, revision anterior cruciate ligament reconstruction.
Tegner Activity Scale. After excluding studies that originally reported outcomes as medians and IQRs, 6 studies remained in the sensitivity analysis for the Tegner scale.17,20,24,29,31,32 The sensitivity analysis yielded a different conclusion: no significant difference was observed between the 2 groups. Details are shown in Figure 11 (MD, 0.39; 95% CI, –0.02 to 0.79; P = .06; I2 = 70%).
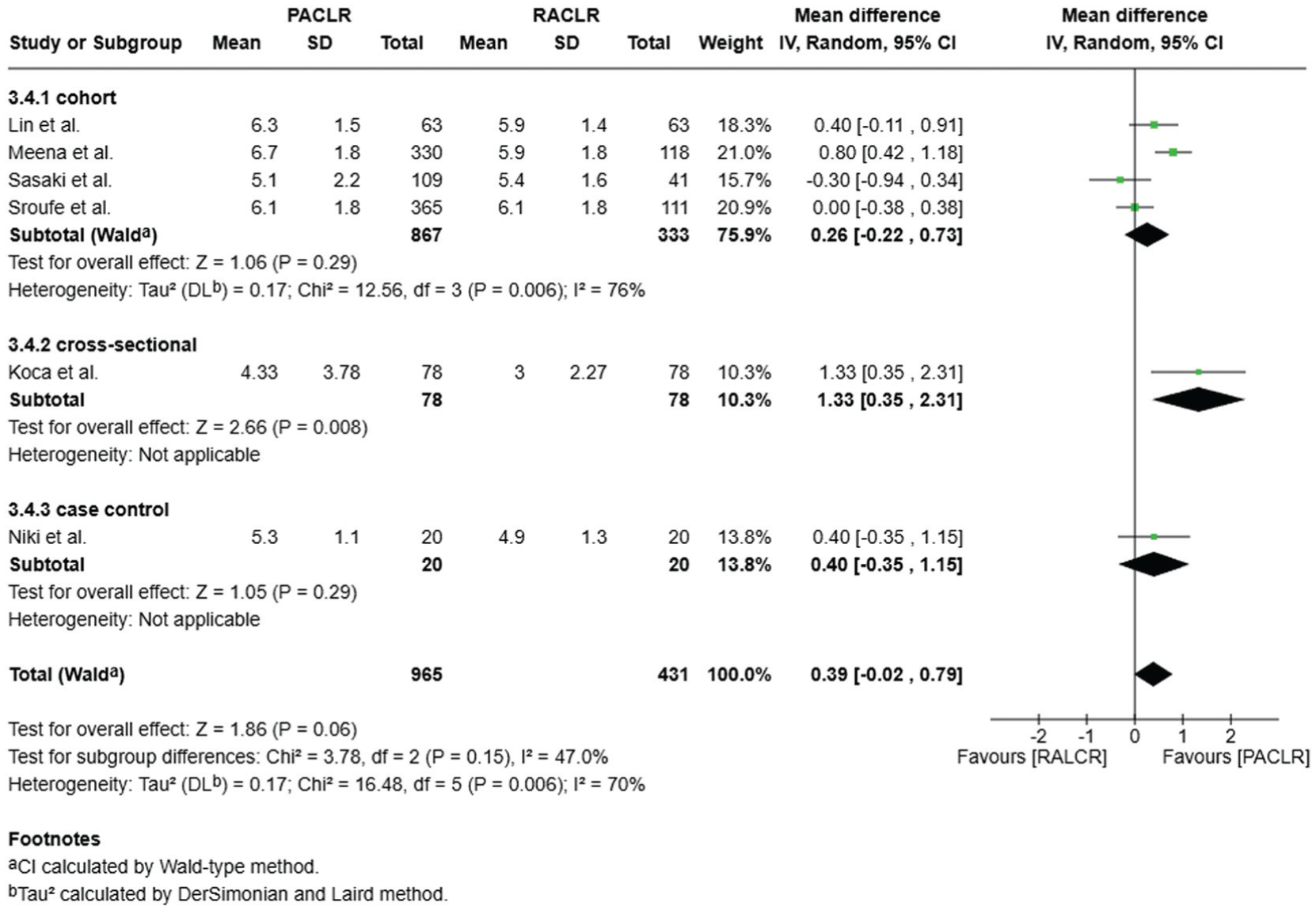
Forest plot of sensitivity analysis of Tegner Activity Scale. IV, inverse variance; PACLR, primary anterior cruciate ligament reconstruction; RACLR, revision anterior cruciate ligament reconstruction.
Discussion
Our meta-analysis demonstrated that while there was no significant difference in the overall RTS rate between PACLR and RACLR, the rate of returning to the same preinjury level was significantly lower in the RACLR group. Additionally, significant differences were found in several commonly used—KOOS, Lysholm score, and Tegner Activity Scale—with PACLR consistently showing better results. Subjective IKDC scores also showed a significant difference favoring PACLR, indicating broader disparities in postoperative function.
When focusing specifically on RTS outcomes, our meta-analysis found that although the overall RTS rate did not differ significantly between PACLR and RACLR, patients undergoing RACLR were less likely to return to the same preinjury level of sport. The pooled RTS rate across studies was approximately 62%, which is comparable with prior large cohort data by the MARS Group (RTS, 63%). 23 However, considerable heterogeneity was observed, as some studies reported significant differences while others did not. This inconsistency likely reflects small sample sizes, variability in surgical techniques, and differences in study design, underscoring the need for larger, high-quality investigations to clarify the true effect of RACLR on sport-specific recovery. A previous meta-analysis provided a related conclusion of RTS 11 ; however, the primary distinction of our study is that it aggregated all available studies on RACLR and calculated an overall RTS rate for the revision group, then compared it with the cumulative RTS rate of PACLR from previous research. In contrast, our research specifically included studies that directly compared the RTS rates between PACLR and RACLR groups in a head-to-head manner, allowing for a more precise and direct comparison. Despite methodological differences between our head-to-head approach and Grassi et al’s pooled analysis, both studies reached the same conclusion, reinforcing the robustness of the finding that RACLR patients are less likely to return to the same pre-injury level. 11 This consistency in findings suggests that the limitation in RTS-S after RACLR is a real and consistent phenomenon.
Several studies have discussed the possible reasons for this phenomenon, including psychological readiness, accompanied meniscal or cartilage damage, and rehabilitation plans.7,30,37 A study by Webster et al 40 indicated that International Cartilage Regeneration & Joint Preservation Society 3 or 4 chondral pathology could lead to significantly lower scores on all PROs and lower rate of RTS-S of preinjury sport. Additionally, Duncan et al 6 found that patients with RACLR had poorer psychological readiness than PACLR (ACL Return to Sport after Injury scale: 85.3 ± 17, 77.4 ± 19.4), which could be a critical factor in rehabilitation. As another aspect of psychological factors, compliance has been found to be related to the rate of RTS, as research showed that higher compliance in rehabilitation has a significant positive effect on rate of RTS and RTS-S. 5 Therefore, more studies need to be conducted to establish a thorough and intact protocol for rehabilitation of patients undergoing RACLR.
Our results reinforce the findings of Mohan et al, 26 who demonstrated that while RACLR is effective, its functional improvements are more modest than those achieved in primary settings. Our study builds upon this by including a larger, updated sample size and additional subscale analysis. On the other hand, findings from Yan et al 45 indicated significant differences between PACLR and RACLR in KOOS and Lysholm scores, but not in the Tegner Activity Scale. However, our meta-analysis identified significant differences in all 3 measures, suggesting that with a larger data set, the conclusions may more accurately reflect the true impact of RACLR on PROs. Notably, the Tegner scale specifically evaluates the intensity of sports participation, further reinforcing our earlier finding that RTS-S is significantly lower after RACLR compared with PACLR. Furthermore, we found that in the 5 domains of KOOS, the highest and lowest scores were observed in the ADL and QOL domains, respectively. This indicates that after postoperative rehabilitation, most patients can recover sufficiently for daily activities such as walking or climbing stairs. However, they may still encounter challenges in high-demand sports or psychological aspects.
Our study also examined subjective IKDC scores, a composite measure encompassing symptoms, sports activities, and function. Unlike previous studies, which did not analyze subjective IKDC scores, our findings indicate a significant difference between PACLR and RACLR in this measure. A previous meta-analysis highlighted the objective IKDC scores in assessing knee function and noted their limitation is the lack of analysis on subjective IKDC. 10 Therefore, we addressed this unaddressed gap of the research and obtained results consistent with previous conclusions, as the IKDC scale captures multiple dimensions of knee function, further supporting the notion that RACLR patients experience greater limitations postoperatively. Furthermore, the subjective IKDC score was shown to correlate well with long-term outcomes and patient satisfaction in ACLR. 18
In our sensitivity analysis, which excluded studies requiring data transformation (from median [IQR] to mean ± SD), the differences in KOOS Pain and Tegner scores between PACLR and RACLR transitioned from statistically significant to nonsignificant. While the transition to nonsignificance in KOOS Pain and Tegner scores may be partially attributed to the reduced sample size in the sensitivity analysis, this finding provides a nuanced insight. It suggests that the disparity between PACLR and RACLR may be less pronounced in basic symptom relief and general activity. Conversely, the persistent significant differences in the other PROs across all analyses highlight that the true gap in overall satisfaction exists between RACLR and PACLR.
By integrating RTS outcomes and patient-reported measures, our findings contribute to a more comprehensive understanding of the differences between PACLR and RACLR. These results highlight the need for realistic preoperative counseling, individualized rehabilitation strategies, and continued efforts to improve RACLR techniques to optimize functional outcomes.
Limitations
Several limitations should be considered when interpreting our findings. First, while our "head-to-head" inclusion criteria ensure a more direct comparison than previous broad-scale reviews, the number of studies directly comparing PACLR and RACLR remains limited. The sample sizes for the RACLR groups were relatively small compared with PACLR, which could potentially lead to statistical imbalance. Second, significant heterogeneity was observed in several outcomes, likely attributable to variations in surgical techniques, rehabilitation protocols, and follow-up durations. Specifically, a subgroup analysis based on graft type was not performed because of inconsistent reporting and insufficient granular data across the included studies, which prevented a meaningful comparison of how different grafts might influence the outcomes. Third, the majority of the included studies were retrospective in design, which increases the risk of inherent selection bias. Fourth, critical confounding factors—such as psychological readiness, rehabilitation compliance, and concomitant meniscal or chondral injuries—were not uniformly reported and thus could not be fully adjusted for in the meta-analysis.
Furthermore, our reliance on data conversion for a subset of the literature represents a noteworthy limitation. Our sensitivity analysis revealed that after excluding converted data, the statistical significance for KOOS Pain and Tegner scores was not maintained. While this transition to nonsignificance may be attributed to a reduction in statistical power from smaller sample sizes, it also provides a nuanced insight into the clinical reality: the functional gap between PACLR and RACLR appears less pronounced in basic symptom management and routine activity levels. In contrast, the robust and persistent differences observed in RTS-S and KOOS QOL across all analyses suggest that the primary weakness of RACLR is specifically localized to high-demand athletic performance and long-term quality of life. Consequently, while RACLR is effective for fundamental recovery, results regarding elite-level sport return and subjective pain relief should be interpreted with caution. Finally, the relatively short- to midterm follow-up in many studies may not fully capture long-term differences, such as osteoarthritis progression or rerevision rates.
Future research with large-scale, prospective, and multicenter designs—utilizing standardized reporting of means and standard deviations—is required to validate these findings and optimize evidence-based strategies for patients undergoing RACLR.
Conclusion
This meta-analysis demonstrated that while the overall RTS rates after PACLR and RACLR were comparable, patients undergoing RACLR had a significantly lower likelihood of returning to their preinjury level of sport. Furthermore, all PROMs—including the subjective IKDC, KOOS, Lysholm, and Tegner scales—consistently favored the PACLR group. These findings suggest that although revision surgery successfully restores fundamental function for daily activities, patients may face substantial limitations in high-demand athletic performance and knee-related quality of life. Therefore, comprehensive preoperative counseling, individualized rehabilitation strategies, and continued refinement of revision techniques are essential to better align patient expectations with realistic postoperative outcomes.
Footnotes
Appendix
| Pubmed | Query |
|---|---|
| 1 | "Anterior Cruciate Ligament Reconstruction"[MeSH] |
| 2 | (anterior cruciate ligament reconstruction[Title]) OR (anterior cruciate ligament reconstruction[Title/Abstract]) |
| 3 | (acl reconstruction[Title]) OR (acl reconstruction[Title/Abstract]) |
| 4 | #1 OR #2 OR #3 |
| 5 | (primary[Title]) OR (primary[Title/Abstract]) |
| 6 | (revision[Title]) OR (revision[Title/Abstract]) |
| 7 | #5 AND #6 |
| 8 | #4 AND #7 |
| 9 | (outcome[Title]) OR (outcome[Title/Abstract]) |
| 10 | (return[Title]) OR (return[Title/Abstract]) |
| 11 | #9 OR #10 |
| 12 | #8 AND #11 |
| Cochrane library | |
| ID | Search |
| #1 | MeSH descriptor: [Anterior Cruciate Ligament Reconstruction] explode all trees |
| #2 | ("anterior cruciate ligament reconstruction"):ti,ab,kw |
| #3 | #1 or #2 |
| #4 | primary |
| #5 | revision |
| #6 | #4 and #5 |
| #7 | #3 and #6 |
| #8 | return |
| #9 | outcome |
| #10 | #8 or #9 |
| #11 | #7 and #10 |
Final revision submitted February 28, 2026; accepted March 3, 2026.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.