
Abstract
Background:
Synovial fluid biomarkers reflect the inflammatory response after joint injury and surgery. Previous studies have identified synovial fluid biomarker concentrations in the knee after both anterior cruciate ligament (ACL) injury and ACL reconstruction (ACLR).
Purpose:
To systematically review the literature to summarize reported changes in synovial fluid biomarkers and their concentrations after acute ACL injury/ACLR.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
Studies published in the PubMed, EMBASE, and the Cochrane Library databases reporting in English on humans sustaining ACL tears and undergoing ACLR from inception to August 2025 were identified and included if postinjury/preoperative and/or postoperative concentrations of synovial fluid biomarkers were reported. Study quality, risk of bias, and heterogeneity were evaluated.
Results:
A total of 44 studies were identified, comprising 2428 patients and 4721 synovial fluid profiles. Postinjury (pre-ACLR) biomarker concentrations were reported across 38 studies (N = 2101 patients). Nineteen studies (N = 676 patients) reported mean biomarker concentrations post-ACLR. Interleukin-6 (IL-6), tumor necrosis factor-alpha (TNF-α), interleukin-1 beta (IL-1β), interleukin-8 (IL-8), interleukin-10 (IL-10), and interleukin-1 receptor antagonist (IL-1Ra) were reported in ≥10 studies (22 studies postinjury; 11 studies post-ACLR). Mean concentrations of all 6 biomarkers were elevated immediately after both injury (pre-ACLR) and surgery (post-ACLR), followed by progressive decrease. Increased mean concentrations for TNF-α and IL-8 were reported from 3 to 6 months after ACL injury (pre-ACLR), with IL-6, TNF-α, and IL-8 remaining elevated over 1 year after injury. Increased mean concentrations of IL-6 and IL-8 were reported from 3 to 6 months after ACLR, with IL-6 and IL-8 remaining elevated over 1 year post-ACLR. Methodological quality was moderate based on Methodological Index for Non-Randomized Studies scores (overall mean, 17.3 [range, 10-23]). Randomized studies demonstrated low to moderate risk of bias according to the Risk of Bias 2 assessment. Considerable heterogeneity in biomarker concentrations was observed.
Conclusion:
Immediate elevation of synovial fluid levels of proinflammatory biomarkers occurs after ACL injury and ACLR, followed by a progressive, yet variable, decrease over 1 year. These biomarkers reflect the underlying inflammatory and healing responses within the knee. However, their correlation with subjective and objective measures of knee function, as well as with the risk of secondary osteoarthritis, is unknown.
Keywords
Anterior cruciate ligament (ACL) tears are among the most common knee injuries, often resulting in short-term disability and long-term implications for knee health and longevity. 67 While treatment options after ACL rupture are subject to ongoing debate, ACL reconstruction (ACLR) remains the gold standard of care for young and active patients, improving quality of life and functional outcomes when compared with nonsurgical management.5,46 Despite the restoration of knee stability after ACLR, a substantial proportion of patients experience progressive degenerative changes within the joint, with a reported 3-fold increase in the prevalence of osteoarthritis (OA) when compared with healthy controls without ACL injury. 6
Synovial fluid biomarkers have garnered increased attention in sports medicine, reflecting the biochemical environment of the knee after ACL injury and ACLR.8,41,44,54,57,77 Specifically, the joint undergoes a complex inflammatory response characterized by the release of various cytokines and other biomarkers into the synovial fluid after ACL injury.41,44,54 Key biomarkers, such as interleukins (IL-6, IL-8, IL-10, IL-1β), tumor necrosis factor-alpha (TNF-α), and interleukin-1 receptor antagonist (IL-1Ra), play pivotal roles in the inflammatory and healing processes within the knee, 54 reflecting the acute inflammatory response mediating tissue repair. Other catabolic proteins, such as periostin (POSTN), which is closely associated with cartilage damage and inflammation, are elevated in the subacute phase after ACL injury. 65 However, prolonged or excessive inflammation is detrimental, leading to adverse outcomes such as chondral damage and compromised joint function.43,57 The modulation of these biomarkers post-ACL injury and reconstruction may help optimize recovery and minimize long-term joint damage.
This study aimed to systematically review and consolidate the present data on commonly reported synovial fluid biomarkers after ACL injury and ACLR. A more comprehensive description of the biochemical milieu of the knee after this common injury will guide further research into how these biomarkers relate to the risk of progressive joint damage,41,44,54,77 potentially leading to more targeted and effective treatment strategies to mitigate this risk.
Methods
Search Strategy and Eligibility Criteria
A systematic review was conducted in accordance with the 2020 PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement. 62 A literature search identifying studies reporting on synovial fluid biomarkers in patients sustaining ACL rupture and subsequent ACLR was conducted on August 5, 2025. Three authors (S.T., T.B., D.C.T.) independently conducted a systematic review of the literature, utilizing the PubMed, Cochrane Database for Systematic Reviews, Cochrane Central Register of Controlled Trials, and Embase databases from inception to August 2025. The search was performed using the following search terms with Boolean operators: “anterior cruciate ligament rupture”; “ACL rupture”; “anterior cruciate ligament injury”; “ACL injury”; “anterior cruciate ligament reconstruction”; “ACL reconstruction”; “synovial fluid collection”; “synovial fluid biomarkers”; and “biomarkers.”
The inclusion criteria consisted of studies written in English or with an English-language translation that reported mean synovial fluid biomarker concentrations at 1 or 2 time points after ACL injury (pre-ACL reconstruction) and/or after ACLR. The exclusion criteria consisted of cadaveric, biomechanical, and animal studies; studies reporting only median biomarker concentrations; case reports; previous meta-analyses and systematic reviews; review articles; and editorial commentaries.
Title and abstract screening were independently performed by 2 authors (S.T., T.B.), followed by a full-text review to determine whether studies met the inclusion and exclusion criteria (Figure 1). A third author (D.M.K.) was assigned to consult whether any disagreements arose among the 2 authors, of which none were encountered. References from the included studies were reviewed to ensure that no additional studies meeting the inclusion criteria had been overlooked; none were identified.

PRISMA diagram. PRISMA, Preferred Reporting Items for Systematic Review and Meta-analysis.
Data Extraction
In the studies included for full analysis, the following study characteristics from each article were recorded and entered in a Microsoft Excel (Version 16.89; Microsoft ) spreadsheet: study title, year published, first author, level of evidence, patient characteristics (ie, mean age at the time of presentation, sex, BMI [body mass index]), concomitant injuries (eg, meniscal injury), concomitant procedures (eg, meniscal repair, meniscectomy), graft type utilized in ACLR, timing of synovial fluid collection post-ACL injury and/or post-ACLR, synovial fluid biomarkers assessed, and mean concentration of synovial fluid biomarkers at each collection timepoint. Only those biomarkers that were assessed in ≥10 previous studies were included for further analysis of post-injury/pre-ACLR and/or post-ACLR levels. Baseline biomarker concentrations were defined as low/undetectable levels consistent with those in healthy, uninjured knees (0-10 pg/mL).42,59,69
Study Quality Assessment
To minimize bias, methodological quality assessments were performed by 2 independent authors (D.C.T., T.B.) using the Cochrane Risk-of-Bias Tool for Randomized Trials, Version 2 (RoB2),35,71 to assess randomized studies, and the Methodological Index for Non-Randomized Studies (MINORS) 70 criteria to evaluate nonrandomized studies. If any disagreements were encountered, a third author (D.M.K.) was consulted, but none were reported. The Cochrane RoB tool assigns scores to randomized studies, categorizing them as high-, moderate- (unclear), or low-risk across 5 domains: randomization process, deviations from the intended intervention, missing outcome data, outcome measurement, and selection of reported results. The MINORS criteria consist of 8 questions for nonrandomized, noncomparative studies and 12 questions for nonrandomized, comparative studies, with each question scored as follows: 0, not reported; 1, reported but inadequate; or 2, reported and adequate. The highest achievable MINORS score for a nonrandomized, noncomparative study is 16, while the highest score for a nonrandomized, comparative study is 24. Because measures of dispersion were inconsistently reported across studies, formal statistical heterogeneity measures (I2, Cochran's Q) could not be calculated. Heterogeneity was therefore assessed descriptively by examining the distribution and ranges of reported biomarker concentrations, comparing sample-size–weighted means with median study means, and evaluating consistency across time intervals (Appendix Tables 4 and 5).
Data Analysis
Patient and study characteristics were compiled and analyzed in Microsoft Excel (Version 16.89; Microsoft). Because of the heterogeneity in synovial fluid collection after ACL injury and ACLR, collection times (T) were grouped into 6 intervals: T ≤ 1 week; 1 week < T ≤ 1 month; 1 month < T ≤ 3 months; 3 months < T ≤ 6 months; 6 months < T ≤ 1 year; and >1 year. Synovial fluid biomarker concentrations were compiled and calculated as a weighted mean. Biomarkers reported in a minimum of 10 studies were further analyzed and plotted as weighted mean concentrations based on timing intervals after ACL injury (pre-reconstruction) and after ACLR (Excel Version 16.89; Microsoft) and included for further analysis.
Results
The initial literature search identified 172 articles (Figure 1). After a full-text review, 44 studies published between 1989 and 2023 were identified, met the inclusion/exclusion criteria, and were included for further analysis. The 44 included studies consisted of 6 studies7,22,45,47,49,72 of Level 1 evidence, 16 studies of Level 2 ‡ evidence, 8 studies4,38,41,42,51,52,60,64 of Level 3 evidence, and 14 studies of Level 4 § evidence. The mean MINORS score for the 36 studies that met the assessment criteria was 17.3 (range, 10-23). The mean score for the 11 noncomparative, nonrandomized studies ‖ was 12.3 (range, 10-14), while the mean score for the 25 comparative, nonrandomized studies was 19.5 (range, 16-23) (Appendix Figure 1). Eight randomized, comparative studies7,22,27,45,47,49,72 were evaluated according to RoB2 (Appendix Figure 2). A total of 5 studies23,27,45,47,72 revealed some concerns for risk of bias, while 3 studies7,22,49 possessed an overall low risk of bias. Considerable heterogeneity in reported biomarker concentrations was observed across studies, reflected by wide ranges in study means, differences between median study means and sample-size–weighted mean concentrations, and variability across postoperative time intervals (Appendix Tables 4 and 5).
Study and Patient Characteristics
A total of 2428 patients sustaining ACL injuries with subsequent postinjury and/or post-ACLR synovial fluid sample collection were identified from the 44 included studies (Table 1). The weighted mean patient age at the time of injury was 28 years (range, 12-62 years). Men comprised 68.1% (n = 1551/2279) of patients, while patient sex was not reported in 4 studies.11,14,23,42 The weighted mean patient BMI was 24.9 kg/m2, as reported in 589 patients across 14 studies. ¶
Overview of Included Studies and Patients With Biomarkers Reported in ≥10 Studies a

IL-10, interleukin-10; IL-1β, interleukin 1-beta; IL-1Ra, interleukin-1 receptor antagonist; IL-6, interleukin-6; IL-8, interleukin-8; LoE, level of evidence; NR, not reported; TNF-α, tumor necrosis factor-alpha.
Graft type and concomitant injuries are summarized in Appendix Table 1.
Synovial Fluid Biomarkers Analyzed
A total of 109 biomarkers were investigated, with each biomarker reported in a mean of 3 studies (Appendix Tables 2 and 3). Six biomarkers were found to be reported in a minimum of 10 studies overall, after ACL injury and/or ACLR. These included IL-6, TNF-α, IL-1β, IL-8, IL-10, and IL-1Ra. (Table 2)25,43,68,82,83
Biomarkers Reported in ≥10 Studies and Included for Analysis a
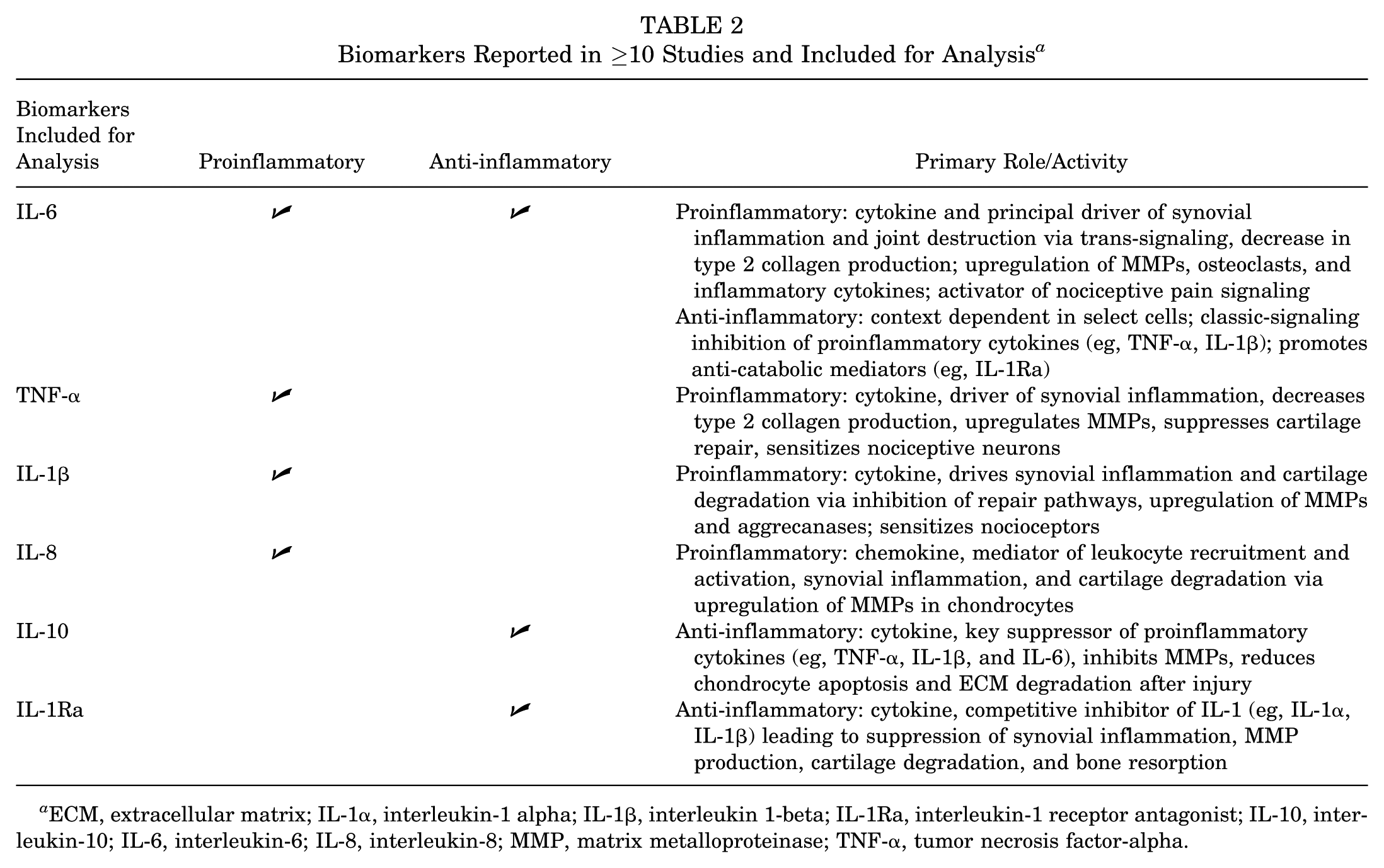
ECM, extracellular matrix; IL-1α, interleukin-1 alpha; IL-1β, interleukin 1-beta; IL-1Ra, interleukin-1 receptor antagonist; IL-10, interleukin-10; IL-6, interleukin-6; IL-8, interleukin-8; MMP, matrix metalloproteinase; TNF-α, tumor necrosis factor-alpha.
Post-ACL Injury Synovial Fluid Biomarker Analysis
Synovial fluid biomarkers collected after ACL injury were reported in 38 studies consisting of 2101 patients. A total of 3618 samples were collected at a weighted mean of 55.2 weeks (range, 1 day-625 weeks) after injury. The most commonly reported postinjury synovial fluid biomarkers were IL-6, # followed by TNF-α, ** IL-1β, †† IL-8, ‡‡ IL-10, §§ and IL-1Ra ‖‖ (Figure 2).

Postinjury/pre-ACLR synovial fluid biomarkers. ACLR, anterior cruciate ligament reconstruction; post, post-reconstruction; pre, pre-reconstruction; sf, synovial fluid; sfIL-1β, synovial fluid interleukin-1 beta; sfIL-1Ra, synovial fluid interleukin-1 receptor antagonist; sfIL-10, synovial fluid interleukin-10; sfIL-6, synovial fluid interleukin-6; sfIL-8, synovial fluid interleukin-8; sfTNF-α, synovial fluid tumor necrosis factor-alpha.
The weighted mean concentrations of the 6 biomarkers were immediately elevated after injury (Figure 3). Specifically, the concentration of TNF-α increased from >1 week to 1 month (17.8-28.9 pg/mL), and again from 1 to 3 months (3.8 pg/mL) to 3 to 6 months (14.9 pg/mL), while the remaining biomarker concentrations steadily decreased until 6 months after injury. From 6 months to 1 year after injury, IL-6 and IL-8 displayed increased mean concentrations relative to their 3-to-6-month values, while the concentrations of the remaining 2 reported biomarkers (TNF-α and IL-10) steadily declined. At over 1 year after injury, the concentration of TNF-α increased from its 6-month-to-1-year value, while remaining biomarker concentrations continued to decrease, with IL-6, TNF-α, and IL-8 remaining elevated above baseline levels beyond 1 year (Table 3).

Post-ACLR synovial fluid biomarkers. ACLR, anterior cruciate ligament reconstruction; post, post-reconstruction; pre, pre-reconstruction; sf, synovial fluid; sfIL-1β, synovial fluid interleukin-1 beta; sfIL-1Ra, synovial fluid interleukin-1 receptor antagonist; sfIL-10, synovial fluid interleukin-10; sfIL-6, synovial fluid interleukin-6; sfIL-8, synovial fluid interleukin-8; sfTNF-α, synovial fluid tumor necrosis factor-alpha.
Post-ACL Injury Synovial Fluid Biomarker Concentrations a
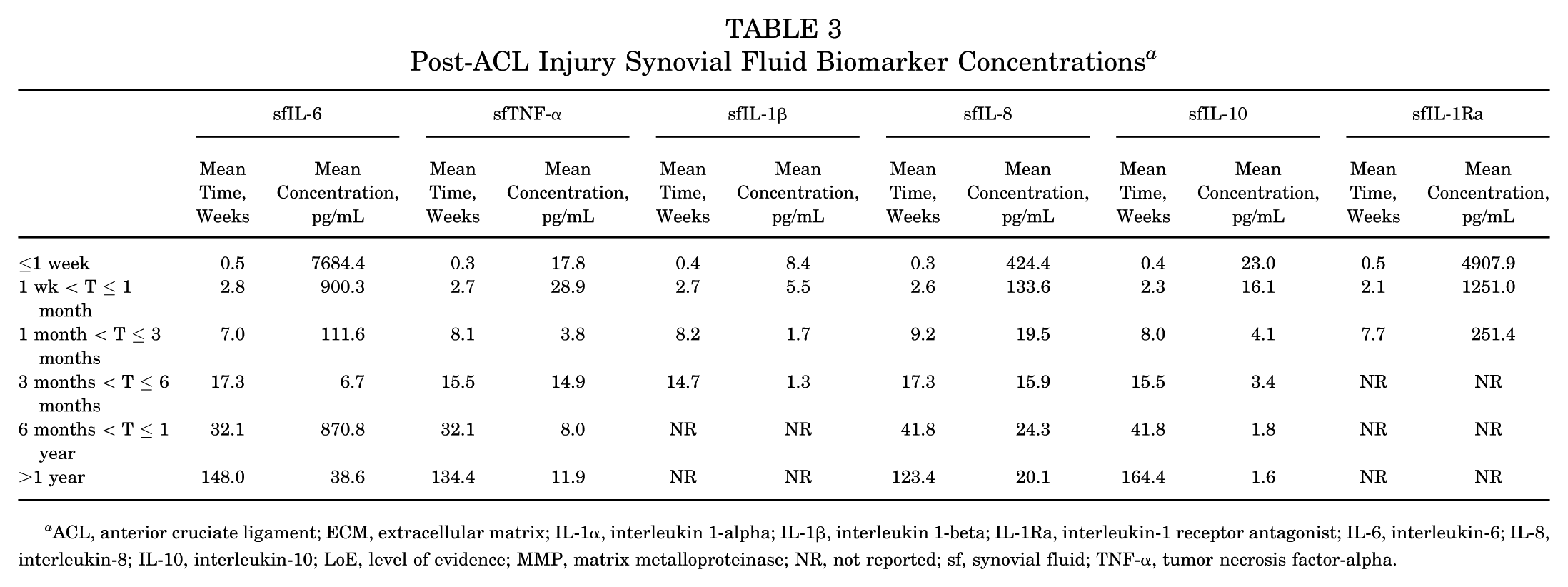
ACL, anterior cruciate ligament; ECM, extracellular matrix; IL-1α, interleukin 1-alpha; IL-1β, interleukin 1-beta; IL-1Ra, interleukin-1 receptor antagonist; IL-6, interleukin-6; IL-8, interleukin-8; IL-10, interleukin-10; LoE, level of evidence; MMP, matrix metalloproteinase; NR, not reported; sf, synovial fluid; TNF-α, tumor necrosis factor-alpha.
Post-ACLR Synovial Fluid Biomarker Analysis
Synovial fluid biomarkers collected after ACLR were reported in 19 studies involving 676 patients. A total of 1103 samples were collected at a weighted mean of 35.6 weeks (range, 0 days-411 weeks) after reconstruction. Biomarkers commonly collected after ACLR included IL-6,1,9,14,33,38,60,85 TNF-α,1,2,9,14,33,60,85 IL-1β, ¶¶ IL-8,9,14,27,60 IL-10,9,60 and IL-1Ra. 33
The weighted mean concentrations of the 6 biomarkers were immediately elevated after ACLR. The concentration of IL-1β increased further at 1 week to 1 month, while the concentrations of the remaining four reported biomarkers (ie, IL-6, TNF-α, IL-8, and IL-10) steadily decreased. At 3 to 6 months after ACLR, the concentration of TNF-α increased from its 1-week-to-1-month value. From 3 to 6 months to 1 year post-ACLR, all reported biomarker concentrations steadily decreased, with IL-6 and IL-8 remaining elevated above baseline levels beyond 1 year (Table 4).
Post-ACLR Synovial Fluid Biomarker Concentrations a

ACLR, anterior cruciate ligament reconstruction; ECM, extracellular matrix; IL-1β, interleukin 1-beta; IL-1Ra, interleukin 1 receptor antagonist; IL-6, interleukin 6; IL-8, interleukin 8; IL-10, interleukin 10; NR, not reported; sf, synovial fluid; TNF-α, tumor necrosis factor alpha.
Discussion
The most commonly reported synovial fluid biomarkers collected post-ACL injury and post-ACLR were IL-6, TNF-α, IL-1β, IL-8, IL-10, and IL-1Ra. Mean concentrations of the 6 biomarkers were elevated after injury and after ACLR. The concentration of TNF-α further increased from 1 week to 1 month after injury, while the concentration of IL-1β increased from 1 week to 1 month post-ACLR. The concentration of TNF-α increased from 3 to 6 months after injury and post-ACLR, while IL-6 increased from 6 months to 1 year post-injury/pre-ACLR. After 1 year, IL-6, TNF-α, and IL-8 concentrations remained elevated post-injury/pre-ACLR, while IL-6 and IL-8 concentrations remained elevated beyond 1 year after ACLR.
The knee microenvironment after ACL injury is characterized by elevated levels of both proinflammatory and anti-inflammatory markers immediately after injury for at least 1 year. Postinjury concentrations were highest for IL-6, reaching 100-fold the reference values in the first week, and remaining the highest among proinflammatory markers at 1 year. IL-6 is associated with increased pain levels, MMP-induced cartilage degradation, and an increased risk for posttraumatic osteoarthritis (PTOA).50,74,79 As IL-6, TNF-α, and IL-8 were elevated at >1 year after injury, these results demonstrate that the ACL-deficient knee exhibits persistent proinflammatory biomarkers that may contribute to progressive joint injury.
Interleukin-1 receptor antagonist (IL-1Ra) decreased significantly from the acute-injury phase (>1 week) to 3 months after injury. This finding aligns with those of Bigoni et al, 8 who reported IL-1Ra levels after ACL injury to be significantly lower than those in noninjured knees starting in the acute (ie, 48-hour) phase, with no subsequent recovery to reference values at 3 months after injury. IL-1Ra provides natural protection against the proinflammatory cytokine IL-1β,13,29 which was detected at low levels (<10 pg/mL) for up to 6 months after injury. Bigoni et al postulated that trauma associated with ACL injury may induce a long-term imbalance in IL-1Ra and that, without its protective effects, even relatively low unopposed levels of IL-1β may be sufficient to incur lasting consequences—including increased risk profiles for joint space narrowing, subchondral bone erosion, ultimate loss of joint function, and chronic pain.21,31
The synovial microenvironment >1 month after ACLR was characterized by high levels of inflammatory markers, which correspond with postsurgical healing. Although relatively few studies report biomarker concentrations beyond 1 month post-ACLR, Larsson et al 47 reported that patients treated with early reconstruction (up to 6 weeks after injury) had significantly higher cytokine concentrations at 4 months (IL-6, IL-8, IL-10, and TNF-α), 8 months (IL-6, IL-8, and TNF-α), and 5 years (sfIL-6) compared with rehabilitation alone. Patients who underwent delayed ACLR (median of 59 weeks after injury) had higher concentrations at 4 months (IL-10 and TNF-α), 8 months (TNF-α), and 5 years (IL-6). 47 Åhlén et al 1 examined synovial fluid collected from post-ACLR and contralateral knees at 8 years after reconstruction and reported no significant differences in the concentrations of IL-1β, IL-6, and TNF-α. However, ACLR knees showed greater degenerative changes, including significantly more meniscal and cartilage damage compared with contralateral knees, as evidenced by higher Fairbanks scores and greater meniscal and cartilage injury and thinning on magnetic resonance imaging (MRI). 1
Posttraumatic OA after ACL injury is reported to result from the injury event itself,17,75 as well as the resultant chemical microenvironment.12,15,37 Proinflammatory markers play crucial roles in the inflammatory response, leading to increased synovial inflammation and the development of fibrosis. Over time, this response impairs tissue repair by upregulating MMPs and generating free radicals, contributing to cartilage degradation, knee pain, and stiffness. Changes in commonly reported synovial fluid biomarkers (IL-6, TNF-α, IL-1β, IL-8, IL-10, and IL-1Ra) after ACL injury and reconstruction reflect underlying inflammation and healing within the knee. Consequently, long-term resolution of proinflammatory cytokines after ACLR may afford additional joint protection and long-term health. Further investigations examining cytokine profiles in ACL-deficient versus post-ACLR knees at long-term follow-up are necessary to better understand the long-term benefit of ACLR on joint health based on the joint microenvironment. Moreover, a thorough understanding of the synovial environment in the knee may help clinicians and researchers forecast patient outcomes after ACL injury and reconstruction, as well as design therapeutic targets to decrease inflammation and cartilage degradation.
Several key molecular biomarkers have been identified specifically after ACL injury. Rai et al 64 identified 2 key inflammatory markers (TNF-α and beta nerve growth factor) and 4 anti-inflammatory markers (IL-4, IL-5), placental growth factor-1, and IL-13 that were higher in knee synovial fluid after ACL injury compared with OA. A follow-up study identified specific catabolic proteins, including cysteine-rich protein 1, S100A11,
POSTN, and vimentin, which were significantly elevated in the subacute phase (mean, 53.7 days) after ACL injury and closely associated with cartilage damage and inflammation. 65 Conversely, chondroprotective proteins, including chitinase-3-like protein 2, tumor necrosis factor–inducible gene-6 protein, neutrophil defensin-1, osteopontin, and cartilage intermediate layer protein-1, were significantly lower in the subacute phase, 65 suggesting that restoring their levels may be beneficial. The potential therapeutic targeting of POSTN is especially noteworthy, as Brophy et al 11 reported ACL remnants induce POSTN expression in chondrocytes, which, in turn, upregulate MMP13 and a disintegrin and metalloproteinase with thrombospondin motif 4, key enzymes involved in cartilage matrix breakdown. While POSTN knockdown inhibited both anabolic and catabolic gene expression and slowed cell migration in vitro, 15 its central role in the metabolic imbalance leading to OA underscores its importance as a key candidate biomarker and potential therapeutic target. Further research is needed to develop consistent and effective diagnostic and therapeutic protocols, which may lead to more personalized treatment strategies to improve postoperative outcomes and minimize long-term disability after ACL injury.
Previous investigations have attempted to correlate biomarker concentrations with subjective and objective outcomes after ACL injury and reconstruction.48,73,74 Struglics et al 73 reported that in a series of 116 ACL-injured patients, each log10 unit elevation of serum TNF concentration at the 2-year follow-up was associated with a 35-point (95% CI, 7%-63%) increase in the knee-related quality of life Knee Injury and Osteoarthritis Outcome Score at the 5-year follow-up after ACL injury. Similarly, Lattermann et al 48 found that in 22 patients undergoing ACLR, higher concentrations of IL-1α, IL-1Ra, and MMP-9 were associated with a lower odds of meeting the International Knee Documentation Committee Patient Acceptable Symptom State threshold. Markus et al 58 reported that concentrations of monocyte chemoattractant protein-1, vascular endothelial growth factor, and IL-1Ra correlated with the development of PTOA at 8 years postoperatively in 18 patients undergoing ACLR. However, other studies have reported that inflammatory biomarker concentrations demonstrate poor correlation with predicting OA progression after ACL injury and reconstruction at 12-month (ACLR, n = 30), 51 5-year (ACL injury, n = 113), 66 8-year (ACLR, n = 11), 1 and 16-year (ACL injury, n = 88) 61 follow-up. Further research is necessary to determine the utility of synovial fluid biomarker concentrations in predicting long-term patient outcomes and OA development.
This study has several limitations. There is variability among studies in laboratory protocols and analysis methods of synovial fluid biomarkers, which can affect the reported biomarker concentration levels. Standardized protocols for collection,19,30 measurement,64,81 and reporting16,19 have been published. However, not all included studies followed the same methodology or provided a detailed description of individual techniques—including whether ultrasound guidance and/or saline lavage were used, particularly when collection times exceeded 1 year. Although many studies meeting the inclusion criteria were included, our pooled analysis was limited to a small subset of studies reporting only those biomarkers reported in a minimum of 10 studies. Mean time intervals between injury and surgery were infrequently reported and varied widely across studies included in the post-ACLR analysis, making this data unusable. This deficiency obviously has the potential to impact pooled long-term biomarker profiles post-ACLR. While degenerative changes, including cartilage damage and meniscal lesions, may be detected on MRI in up to 17% of patients as early as 1 to 5 years post-ACLR,20,63 radiographic evidence of OA is present in approximately 12% to 21% of patients at 5 years post-ACLR. 10 Few studies analyzed biomarker concentrations at >1-year follow-up, which limited analysis at postoperative time points necessary to establish a correlation with OA progression. Moreover, in the post-ACLR biomarker analysis, relatively few studies reported concentrations between 3 and 12 months after surgery. Because of heterogeneity in the study designs, including substantial variability in synovial fluid collection timing relative to ACL injury and ACLR, as well as incomplete or insufficient sample sizes at multiple time intervals, it was not feasible to perform formal comparative analysis, such as postinjury versus postsurgery, ACL-injured versus contralateral knee, and correlation with objective (eg, graft type, performance of concomitant procedures) and patient-reported outcome measures. This study did not analyze patient-reported outcomes or note whether they were collected. Studies reporting only median values were excluded. However, including these studies with appropriate transformations could potentially increase sample sizes and power. Finally, the use of pooled weighted mean biomarker concentrations may not fully capture inter-patient variability nor accurately reflect biochemical processes occurring throughout the knee synovial microenvironment at the individual patient level. Future research is necessary to determine the clinical implications of inflammatory biomarker concentrations on long-term knee joint health and prognosis after ACL injury and reconstruction.
Conclusion
The knee microenvironment after ACL injury and ACLR is characterized by the immediate elevation of synovial fluid levels of proinflammatory biomarkers (IL-6, TNF-α, IL-1β, IL-8, IL-10, and IL-1Ra), followed by a progressive yet variable decrease over 1 year. These biomarkers reflect the underlying inflammatory and healing responses within the knee. However, more research is needed to determine whether they correlate with subjective and objective measures of knee function or with the risk for secondary OA.
Footnotes
Appendix
Post-ACLR Synovial Fluid Biomarker Concentrations

| Number of studies and patients (n) | Time (weeks) weighted mean, median mean, range | Concentration (pg/mL) weighted mean, median mean, range | |
|---|---|---|---|
|
|
|||
| ≤ 1 week | 6 (134) | 0.7, 0.8 (0.0–1.0) | 3519.6, 2820.6 (0.0–12823.1) |
| 1 wk < T ≤ 1 month | 3 (23) | 4.0, 4.0 (3.0–4.0) | 612.7, 502.0 (220.0–855.4) |
| 1 month < T ≤ 3 months | – | NR | NR |
| 3 months < T ≤ 6 month | 1 (38) | 17.3, 17.3 (17.3–17.3) | 255.6, 255.6 (255.6–255.6) |
| 6 months < T ≤ 1 year | 1 (77) | 43.7, 43.3 (34.7–52.0) | 107.5, 104.5 (29.6–179.5) |
| > 1 year | 2 (125) | 195.9, 260.0 (104.0–410.8) | 12.5, 8.0 (0.5–20.4) |
|
|
|||
| ≤ 1 week | 6 (136) | 0.6, 0.5 (0.0–1.0) | 12.4, 10.8 (2.4–40.8) |
| 1 wk < T ≤ 1 month | 1 (8) | 4.0, 4.0 (4.0–4.0) | 2.4, 2.4 (2.4–2.4) |
| 1 month < T ≤ 3 months | – | NR | NR |
| 3 months < T ≤ 6 month | 1 (38) | 17.3, 17.3 (17.3–17.3) | 8.9, 8.9 (8.9–8.9) |
| 6 months < T ≤ 1 year | 1 (77) | 43.7, 43.3 (34.7–52.0) | 5.5, 5.5 (5.5–5.5) |
| > 1 year | 2 (125) | 195.9, 260.0 (104.0–410.8) | 3.8, 3.8 (1.6–4.3) |
|
|
|||
| ≤ 1 week | 7 (210) | 0.5, 0.5 (0.0–1.0) | 1881.5, 9.5 (1.0–29330.0) |
| 1 wk < T ≤ 1 month | 4 (63) | 2.3, 2.7 (1.4–4.0) | 4045.7, 12.7 (0.6–25430.0) |
| 1 month < T ≤ 3 months | – | NR | NR |
| 3 months < T ≤ 6 month | – | NR | NR |
| 6 months < T ≤ 1 year | – | NR | NR |
| > 1 year | 1 (11) | 410.8, 410.8 (410.8–410.8) | 0.4, 0.4 (0.4–0.4) |
|
|
|||
| ≤ 1 week | 3 (81) | 0.8, 0.8 (0.5–4200.0) | 1239.0, 1701.1 (132.4–4200.0) |
| 1 wk < T ≤ 1 month | 2 (9) | 3.9, 3.5 (3.0–4.0) | 417.8, 453.7 (407.5–500.0) |
| 1 month < T ≤ 3 months | 1 (41) | 6.0, 6.0 (6.0–6.0) | 183.8, 183.9 (180.4–187.4) |
| 3 months < T ≤ 6 month | 1 (38) | 17.3, 17.3 (17.3–17.3) | 150.1, 150.1 (150.1–150.1) |
| 6 months < T ≤ 1 year | 1 (77) | 43.7, 43.3 (34.7–52.0) | 44.1, 44.1 (43.2–45.0) |
| > 1 year | 1 (114) | 175.2, 182.0 (104.0–260.0) | 19.2, 19.1 (18.0–20.3) |
|
|
|||
| ≤ 1 week | 2 (71) | 0.7, 0.5 (0.5–1.0) | 14.4, 1.6 (1.1–28.0) |
| 1 wk < T ≤ 1 month | 1 (8) | 4.0, 4.0 (4.0–4.0) | 11.2, 11.2 (11.2–11.2) |
| 1 month < T ≤ 3 months | – | NR | NR |
| 3 months < T ≤ 6 month | 1 (38) | 17.3, 17.3 (17.3–17.3) | 5.3, 5.3 (5.3–5.3) |
| 6 months < T ≤ 1 year | 1 (77) | 43.7, 43.3 (34.7–52.0) | 2.6, 2.6 (2.2–2.9) |
| > 1 year | 1 (114) | 175.2, 182.0 (104.0–260.0) | 1.7, 1.7 (1.7–1.8) |
|
|
|||
| ≤ 1 week | 1 (26) | 0.0, 0.0 (0.0–0.0) | 965.4, 925.0 (400.0–1450.0) |
| 1 wk < T ≤ 1 month | – | NR | NR |
| 1 month < T ≤ 3 months | – | NR | NR |
| 3 months < T ≤ 6 month | – | NR | NR |
| 6 months < T ≤ 1 year | – | NR | NR |
| > 1 year | – | NR | NR |
ACL = anterior cruciate ligament; IL-10 = Interleukin 10; IL-1Ra = Interleukin 1 receptor antagonist; IL-1β = Interleukin 1-beta; IL-6 = Interleukin 6; IL-8 = Interleukin 8; LOE = Level of evidence; NR = Not reported; sf = synovial fluid; TNF-α = Tumor necrosis factor alpha
Final revision submitted March 22, 2026; accepted March 28, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.V.S. has received research support from Elite Orthopedics LLC. M.J.M. has received consulting fees from Arthrex Inc, Osteosys, and Schwartz Biomedical; and fellowship support from Arthrex Inc, Bregg Inc, and Smith & Nephew.