
Abstract
Background:
Osteochondral lesions of the talus (OLTs) are a common cause of disability and chronic ankle pain. Many surgical treatment methods are currently used to treat OLTs, including particulated autologous cartilage transplantation (PACT). Nonetheless, the relative outcomes of PACT for OLTs are unclear.
Purpose:
To compare the short-term efficacy of bone marrow stimulation (BMS) and PACT in patients with OLTs.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Consecutive symptomatic patients with OLT who underwent BMS or PACT from March 2015 to December 2022 were retrospectively evaluated for at least 2 years. Preoperative radiography and magnetic resonance imaging (MRI) were performed in all patients. Follow-up second-look arthroscopy and MRI were performed approximately 1 year postoperatively. Clinical outcomes were assessed using the pain visual analog scale (VAS), American Orthopaedic Foot & Ankle Society (AOFAS) score, and Foot and Ankle Outcome Score (FAOS). The quality of regenerated cartilage was evaluated using Magnetic Resonance Observation of Cartilage Repair Tissue (MOCART) scores and International Cartilage Repair Society (ICRS) grades and scores. Continuous variables were compared using independent t tests. A P value <.05 was considered statistically significant.
Results:
A total of 48 and 16 patients (48 and 16 ankles) were enrolled in the BMS and PACT groups, respectively. No significant differences existed in demographic characteristics between the groups. Preoperatively, some clinical parameters were significantly worse in the PACT group (VAS 5.2 ± 2.3 vs 6.4 ± 0.8, P = .003; AOFAS score 70.0 ± 7.1 vs 62.1 ± 11.0, P = .015; FAOS symptom 64.7 ± 17.1 vs 53.3 ± 17.9, P = .036). However, 1-year FAOS quality of life scores (55.8 ± 21.1 vs 75.5 ± 23.1, P = .006) and 2-year AOFAS scores were significantly higher in the PACT group (84.9 ± 11.4 vs 91.4 ± 8.6, P = .021). Postoperative MOCART scores were significantly higher in the PACT group (55.3 ± 24.0 vs 66.3 ± 20.6, P = .048). Moreover, second-look arthroscopy revealed that ICRS scores (9.7 ± 0.5 vs 10.0 ± 0.5, P = .037) and grades (P = .001) were significantly better in the PACT group.
Conclusion:
Our study demonstrated that PACT achieved significantly superior morphologic cartilage regeneration compared with BMS in OLTs at 1-year follow-up. However, the differences in clinical outcomes between the 2 treatments were not significant. Notwithstanding, additional follow-up studies are needed to assess the effects of PACT on long-term outcomes.
Keywords
Osteochondral lesions of the talus (OLTs) are a frequent cause of chronic ankle pain and functional impairment. Conservative treatment involves rest, immobilization, and the use of anti-inflammatory medications. The success rate of nonoperative management for OLTs is approximately 45%. 31 If conservative approaches fail, surgical interventions such as bone marrow stimulation (BMS), osteochondral autograft transplantation, autologous chondrocyte implantation, and osteochondral allograft transplantation may be considered.15,16,24,30 However, these procedures have limitations, including variable clinical and biological outcomes, donor site complications, suboptimal integration, and high costs.
Surgical techniques for OLTs have evolved considerably over the past decade. Among emerging treatments, autologous cartilage chip transplantation has gained attention because of promising preclinical and clinical results and the demand for cost-effective solutions for articular cartilage repair.9-12,21 First introduced by Lu et al 20 in 2006, this transplantation method involves mincing autologous cartilage and transplanting it into an animal model with chondral defects. The treatment achieved chondrocyte migration and proliferation, suggesting that cartilage chips could be used in cartilage restoration. Later, Christensen et al 12 compared autologous cartilage chip transplantation and BMS in a minipig model and found that the former was more effective at improving hyaline cartilage regeneration and histologic scores and reducing fibrous tissue formation. This technique entails harvesting autologous hyaline cartilage from the trochlear border or intercondylar notch of the knee and implanting it into the lesion site. In alignment with this approach, clinical studies have used cartilage harvested from healthy sites.14,21,32,35
However, chondrocytes derived from damaged cartilage are viable and could be used in transplantation.4,7 Damaged cartilage tissue is used for particulated autologous cartilage transplantation (PACT) in the knee and ankle joints.3,26,28 However, the comparative outcomes of PACT and BMS for OLTs have not been investigated. Therefore, we aimed to compare the short-term efficacy of BMS and PACT in patients with OLTs. We hypothesized that PACT would be superior to BMS.
Methods
Consecutive patients who underwent OLT with either BMS or PACT from March 2015 to December 2022 were retrospectively enrolled. The study was approved by our institutional review board (INHAUH 2025-03-001) and complied with the Declaration of Helsinki. All surgeries were performed by a senior surgeon (B.S.K.), and all patients were followed up for at least 2 years. BMS was conducted from March 2015 to July 2020, and PACT was performed from August 2020 to December 2022. The inclusion criteria were patients aged ≥18 years, those with unilateral lesions, patients with ankle cartilage defects classified as International Cartilage Repair Society (ICRS) grade 4, patients with persistent ankle pain and stiffness unresponsive to at least 3 months of nonoperative treatment (analgesic medications, physical therapy, and muscle-strengthening exercises, etc), and those who underwent magnetic resonance imaging (MRI) and second-look arthroscopy evaluation at follow-up. The exclusion criteria included patients with degenerative ankle arthritis (Kellgren-Lawrence grade II or higher), those with acute ligament injuries or chronic ankle instability, patients who had previously undergone surgical treatment for the same condition, those who had received injection therapy (eg, steroids, hyaluronic acid, or platelet-rich plasma) within 6 months for the same condition, patients with chronic inflammatory joint diseases (eg, rheumatoid arthritis) or infectious arthritis, and those with deformity of the ankle or foot.
All patients underwent standard preoperative radiography and MRI. The area of the lesion was measured on MRI, as previously described. 30 Follow-up evaluations, including second-look arthroscopy and MRI, were conducted approximately 1 year postoperatively with patient consent. An independent radiologist reviewed the images. Cartilage repair was assessed using Magnetic Resonance Observation of Cartilage Repair Tissue (MOCART) scores ranging from 0 (worst) to 100 (best). 27 Additionally, an independent orthopaedic surgeon assessed the quality of the regenerated cartilage using pre- and postoperative ICRS grades and postoperative ICRS scores.23,33 Clinical outcomes before and after surgery were evaluated based on the pain visual analog scale (VAS), American Orthopaedic Foot & Ankle Society (AOFAS) score, and Foot and Ankle Outcome Score (FAOS).
Surgical Technique
Patients were positioned supine, and standard anteromedial and anterolateral portals were established for arthroscopic visualization and instrumentation. Gentle ankle distraction was achieved using noninvasive traction with a foot strap applying approximately 15 pounds of force. A systematic arthroscopic evaluation of the ankle joint was performed to identify the lesion and assess its location and stability.
BMS was carried out using a conventional approach. 30 In contrast, in the PACT group, the cartilage covering the lesion was carefully detached using a grasper. The harvested cartilage was subsequently minced into approximately 1-mm3 fragments with a scalpel by an assisting surgeon. During this process, the senior author (B.S.K.) inspected the cartilaginous subchondral bone; unstable tissue was removed, and microfracture was performed to achieve a stable and even articular bed. Concomitant intra-articular pathologies identified during arthroscopy were addressed as appropriate through debridement, removal, or excision. Following the evacuation of saline from the joint, the minced cartilage was applied directly to the defect under dry arthroscopic visualization. A freer elevator was used to contour the implanted cartilage to match the surrounding articular surface, after which fibrin glue was applied to secure the construct. 28
Postoperatively, patients in the BMS group were permitted immediate weightbearing and unrestricted activities of daily living. In the PACT group, active range of motion exercises were initiated 2 to 3 days after surgery. The ankle was immobilized in a splint for 2 weeks, followed by use of a rigid walker boot after suture removal. Partial weightbearing with crutches was allowed until 6 weeks postoperatively.
Statistical Analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences version 26.0 (IBM Corp). Normally distributed continuous variables are presented as means ± standard deviations, and categorical variables are presented as numbers and percentages. The normality of the data was checked using the Kolmogorov-Smirnov and Shapiro-Wilk normality tests. Pre- and postoperative outcomes were evaluated using the Student t test or the Mann-Whitney test. The association between groups and ICRS grades was analyzed using linear-by-linear association analysis. The level of statistical significance was set at P < .05.
Results
A total of 48 and 16 patients (48 and 16 ankles) were enrolled in the BMS and PACT groups. No significant differences existed in demographic data between the 2 groups (Table 1).
Patient Characteristics a
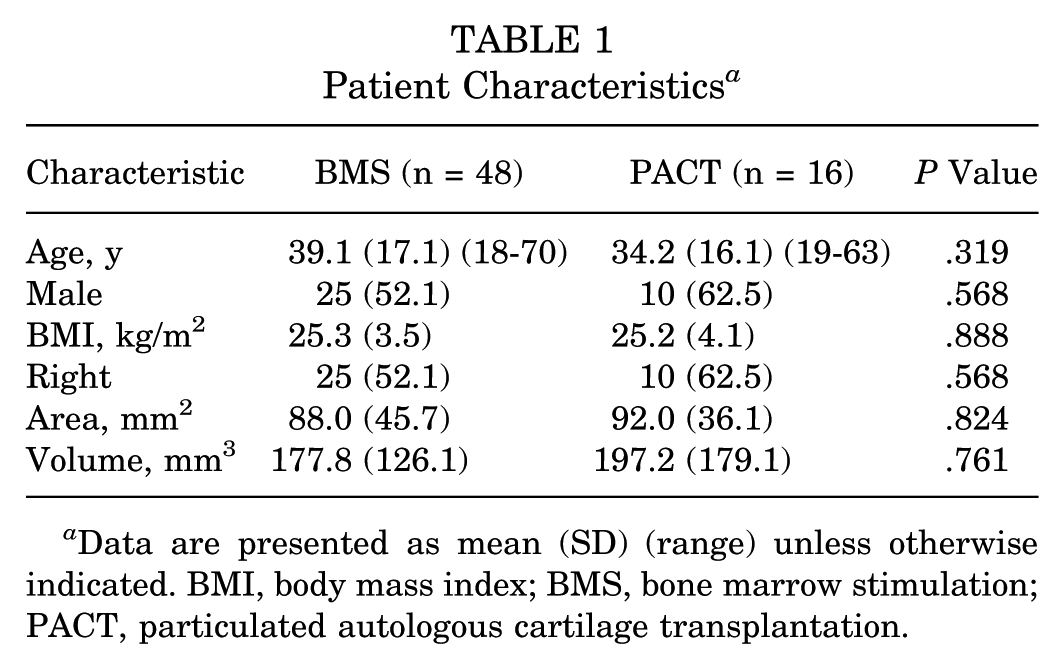
Data are presented as mean (SD) (range) unless otherwise indicated. BMI, body mass index; BMS, bone marrow stimulation; PACT, particulated autologous cartilage transplantation.
Clinical outcomes are presented in Table 2. Both groups showed significant improvements in all clinical parameters postoperatively compared to preoperative values (P < .001). Preoperatively, pain VAS and AOFAS scores, FAOS symptom scores, and FAOS sum were significantly lower in the PACT group than in the BMS group (P≤ .039). At a 1-year follow-up, FAOS quality of life scores were significantly higher in the PACT group (P = .006). In turn, no significant between-group differences were observed in the other outcome parameters. At a 2-year follow-up, AOFAS scores were significantly higher in the PACT group (P = .021), whereas other parameters showed no significant differences.
Clinical Outcomes of Bone Marrow Stimulation and Particulated Autologous Cartilage Transplantation a

Data are presented as mean (SD) (range). Bold values indicate statistical significance at p < 0.05. AOFAS, American Orthopaedic Foot & Ankle Society; BMS, bone marrow stimulation; FAOS, Foot Ankle Outcome Score; PACT, particulated autologous cartilage transplantation; QoL, quality of life; VAS, visual analog scale.
MRI and arthroscopic findings are summarized in Table 3. MOCART scores significantly improved postoperatively in both groups (P < .001). No significant differences existed in preoperative MOCART scores between the groups. In turn, postoperative MOCART scores were significantly higher in the PACT group (P = .048) (Figure 1).
Radiological and Second-Look Arthroscopy Outcomes of Bone Marrow Stimulation and Particulated Autologous Cartilage Transplantation a
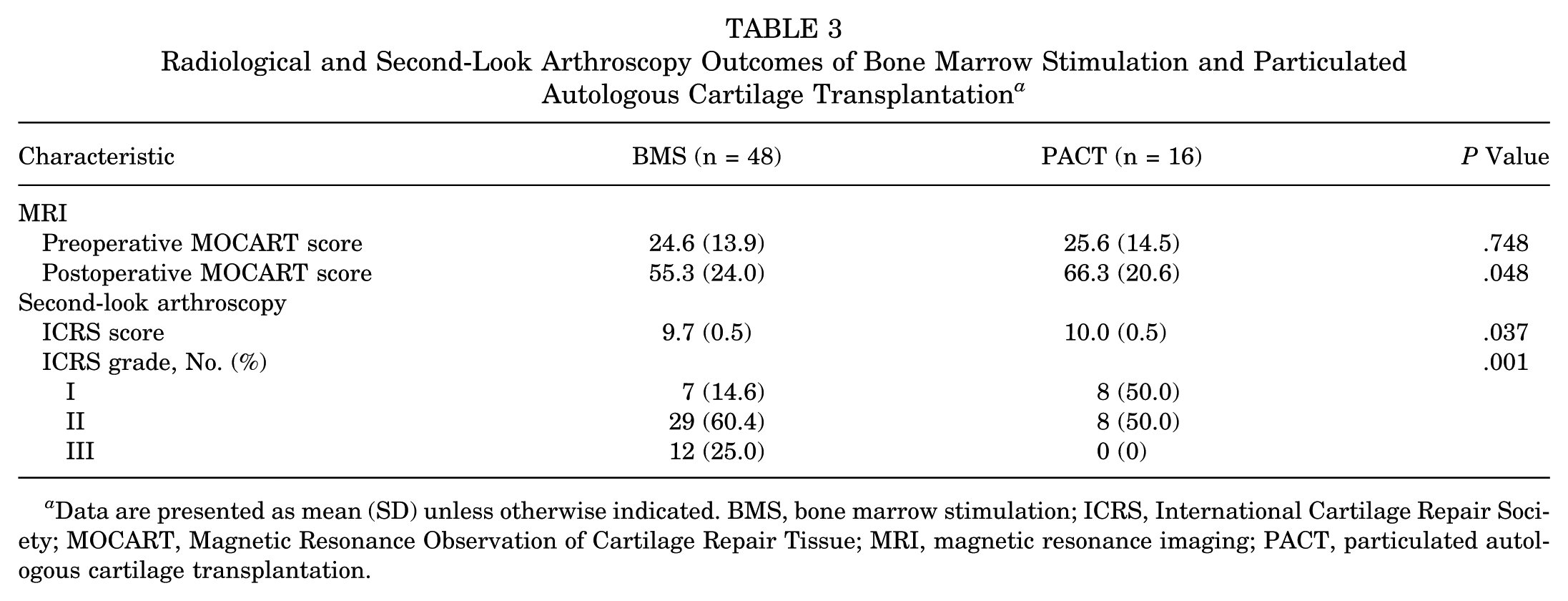
Data are presented as mean (SD) unless otherwise indicated. BMS, bone marrow stimulation; ICRS, International Cartilage Repair Society; MOCART, Magnetic Resonance Observation of Cartilage Repair Tissue; MRI, magnetic resonance imaging; PACT, particulated autologous cartilage transplantation.

Representative coronal T2 fat-suppressed magnetic resonance imaging (MRI) images of bone marrow stimulation (BMS) and particulated autologous cartilage transplantation (PACT). (A, B) Preoperative and 1-year postoperative MRI images of a 52-year-old man who received BMS. (C, D) Preoperative and 1-year postoperative MRI images of a 20-year-old woman who received PACT.
Second-look arthroscopy revealed that ICRS scores and grades were significantly better in the PACT group (P = .037, P = .001) (Figure 2).

Representative arthroscopic images of the medial talus showing bone marrow stimulation (BMS) and particulated autologous cartilage transplantation (PACT). (A, B) Arthroscopic images obtained during the first operation and at the 1-year postoperative second-look arthroscopy of a 40-year-old man who received BMS. (C, D) Arthroscopic images obtained during the first operation and (E) at the 1-year postoperative second-look arthroscopy of a 21-year-old man who received PACT.
Discussion
The major findings of the present study were that PACT demonstrated superior morphologic cartilage regeneration compared with BMS in the treatment of OLTs. Postoperative MOCART scores were significantly higher in the PACT group than in the BMS group (P = .048), and second-look arthroscopy showed significantly better ICRS scores and grades in the PACT group (P = .037 and P = .001, respectively). Although preoperative clinical scores were worse in the PACT group, postoperative clinical outcomes were comparable between groups, with significantly higher FAOS quality-of-life scores at 1 year (P = .006) and AOFAS scores at 2 years (P = .021) in the PACT group. BMS is simple to perform and cost-effective. However, BMS is less effective in larger and noncontained lesions. 8 Additionally, in the long term, BMS can cause fibrocartilage formation, articular surface damage, incomplete integration, and degenerative changes, potentially leading to suboptimal long-term outcomes.2,18 In contrast, PACT, which involves mincing autologous hyaline cartilage and transplanting it to fill articular defects, can potentially replace BMS in treating OLT.
The concept of using autologous cartilage chips for cartilage repair was first introduced in 1983 and has been the subject of ongoing research.1,10,12,20 Animal studies showed that when cartilage was precisely cut with a sharp scalpel, embedded chondrocytes remained largely intact and migrated from their original matrix to promote the formation of a new extracellular matrix.5,17,19,25,34 Additionally, chondrocytes in the surrounding matrix can resume proliferation, improving healing. This process has been observed in animal models where small cartilage defects regenerate spontaneously. 22 A preclinical study demonstrated that PACT effectively promoted cartilage repair in shallow osteochondral lesions without requiring bone grafting. 29 The extent of cartilage fragmentation also plays a critical role in the repair process. Larger cartilage chips promote the activation of fewer chondrocytes than smaller chips. Moreover, cartilage chips with a paste-like consistency can create an optimal environment for high-quality tissue regeneration. 6
Chondrocytes within osteochondral lesions reportedly remain viable and can be used in transplantation.4,7 The morphologic characteristics, cell density, proliferative capacity, and protein synthesis of damaged articular cartilage are similar to those of normal cartilage. 7 Similarly, no significant differences exist in the mean glycosaminoglycan concentration and DNA content in cell pellets derived from damaged and healthy cartilage. 4 Furthermore, these properties are similar to those of chondrocytes derived from autologous bone marrow cells. Case studies demonstrated the efficacy of PACT using cartilage harvested from lesions in knee and ankle joints.26,28
Several studies have compared the outcomes of PACT and BMS. A preclinical study revealed that PACT resulted in a greater proportion of hyaline cartilage (17.1%) and a lower percentage of fibrous tissue (23.8%) than BMS (2.9% and 41.1%) (P < .01 for both variables). 12 Furthermore, after 6 months, PACT achieved higher ICRS scores and type II collagen staining than BMS (P < .05 for both). A prospective study compared BMS with a cell-based cartilage repair technique using the Cartilage Autograft Implantation System (CAIS) over a 2-year follow-up and showed that the International Knee Documentation Committee scores and most subdomains of the Knee injury and Osteoarthritis Outcome Score were significantly higher in the CAIS group. 13 Additionally, the incidence of intralesional osteophyte formation was notably lower in the CAIS group than in the BMS group (25% vs 70%) at a 1-year follow-up. Our findings align with those of previous studies. Although between-group differences existed in clinical outcomes at the 2-year follow-up, surgical outcomes assessed through MRI and arthroscopic examinations were superior in the PACT group. This result suggests that PACT may yield better long-term results with extended follow-up.
This study has limitations. First, although all patients were evaluated using the same follow-up protocol, patients were not randomized to receive treatment, potentially introducing bias, such as differences in preoperative outcomes and surgical modalities. Second, the small number of patients decreased the statistical power of the results. Third, the short follow-up prevented the evaluation of cartilage repair and functional outcomes in the long term. Thus, a longer follow-up is needed to fully assess the durability of the regenerated cartilage and potential long-term complications, such as cartilage degeneration and clinical failure. Fourth, postoperative rehabilitation protocols differed between the BMS and PACT groups (eg, weightbearing exercises immediately after surgery vs splinting followed by weightbearing exercises). These differences may have influenced the healing process and clinical outcomes, making it difficult to base the results solely on the surgical technique. However, this effect may be temporary and may not have strongly affected the outcomes. Finally, although the ICRS score/grade and the MOCART score used in this study are widely accepted tools for evaluating cartilage repair, they do not represent direct histologic assessment of the regenerated tissue. Future studies including histologic evaluation with tissue samples would provide a more precise comparison between the 2 treatment groups.
Conclusion
Our study demonstrated that PACT achieved significantly superior morphologic cartilage regeneration than BMS in OLT at the 1-year follow-up. However, the differences in clinical outcomes between the 2 treatments were not significant. Notwithstanding, additional follow-up studies are needed to assess the effects of PACT on long-term outcomes.
Footnotes
Final revision submitted March 17, 2026; accepted March 21, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.W.S. has received funding from the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (RS-2025-16072043). Funding was used in the analysis, interpretation of data, and writing the manuscript.
Ethical approval for this study was obtained from the Inha University Hospital Institutional Review Board (INHAUH 2025-03-001).