
Abstract
Background:
Knee injuries account for 25% to 30% of running-related injuries (RRIs). Patellofemoral pain syndrome (PFPS), iliotibial band syndrome (ITBS), and patellar tendinopathy (PT) are the most commonly reported knee injuries. The literature focuses on biomechanical factors, whose predictive value is inconsistent, and exposure-related factors remain underexplored.
Purpose:
To systematically review and synthesize the evidence on risk factors associated with knee injuries in endurance runners with a focus on both biomechanical and exposure-related factors.
Study Design:
Systematic review; Level of evidence, 3.
Methods:
A systematic search of the Medline (PubMed), Embase, and Web of Science was conducted for studies before November 19, 2024. Studies were included if they investigated risk factors for knee injuries in adult endurance runners. Studies were excluded if they were case reports, non-English studies, review articles, studies focusing on nonendurance athletes, or studies focusing on athletes >30 years old. Twenty studies were selected from 1883 articles after screening. Risk factors were categorized as biomechanical or exposure-related.
Results:
Across PFPS, ITBS, and PT, the strongest and most recurrent risk factors were a history of previous injury (odds ratio [OR] range, 1.36-10.19), increased training load or volume (OR range, 1.07-8.94), and structural malalignment (OR range, 1.89-4.12). For general knee injuries, previous injury was the most frequently reported risk factor, associated with a 12.9% higher incidence of reinjury. PFPS was linked to training load and structural malalignment, indicating small to moderate associations between deviations from optimal load and injury risk. For ITBS, kinematic variables (OR range, 3.02-5.62; Cohen's d range, 1.24-2.21) and kinetic variables (OR, 8.88; Cohen's d, 0.82) were most commonly reported, reflecting moderate to very large effects linked to abnormal pelvic motion and impaired shock absorption. For PT, increased training load and volume (OR range, 1.27-8.94) and demographic factors (OR range, 1.06-1.43) were most frequently reported, with runners training >20 hours per week demonstrating a 15% to 20% higher injury incidence.
Conclusion:
Knee injuries in endurance runners are influenced by a history of injury, training load, and biomechanical factors. Future injury prevention strategies should integrate biomechanical and contextual factors, including individualized kinematic profiles and conservative training management.
Endurance running, defined here as running upwards of 10 km, has become increasingly popular in recent years because of its accessibility, relatively low prior experience requirements, and numerous mental and physical health benefits.18,28 However, the repetitive nature of the sport places substantial stress on the joints of the lower extremities. Musculoskeletal injuries, often secondary to overuse, affect up to 90% of individuals training for, competing in, or recovering from endurance running events, thereby highlighting a significant health concern within this population. 36 Specifically, of the joints of the lower extremity, studies have shown that knee injuries account for 25% to 30% of all running-related injuries (RRIs), with the majority of runners experiencing such injuries as patellofemoral pain syndrome (PFPS), followed by iliotibial band syndrome (ITBS), meniscal injuries, and patellar tendinopathy (PT).18,19,28
PFPS is the most common knee injury among endurance runners, with an incidence of 19% to 30% in female and 13% to 25% in male runners. 25 PFPS typically presents as gradually worsening pain in the anterior or retropatellar region of the knee and is commonly triggered by loading and compression. 25 ITBS is relatively less common, 20 with a prevalence of 8%, and is characterized by pain localized to the lateral knee, particularly with extension. 25 Although previous research has identified both biomechanical and training-related contributors to these conditions, findings across studies remain inconsistent, and injury mechanisms appear to vary by population, injury type, and running characteristics.2,30,44 However, much of the literature has focused narrowly on biomechanical risk factors, given the ease and accessibility of measuring interventions as well as the practicality of study design.8,23,33 Not only are such factors difficult to modify, but the evidence correlating these variables with injury is often inconsistent. Furthermore, even when biomechanical factors are associated with an increased risk of injury, there are consistent gait patterns across both healthy and injured running populations, indicating that a specific injury may be a result of a variety of movement patterns. 1
Focusing solely on biomechanical factors to explain injury risk does not fully address the multifactorial nature of running overuse injuries. Qualitative and exposure-related factors, such as demographic characteristics, injury history, and training load and volume, must be considered. The systematic reviews on this topic have important limitations: some focus on very elite populations,6,20 others address only exposure-related factors,5,9 or biomechanical factors,8,23,33 while others examine a broad range of lower-limb injuries rather than concentrating specifically on the knee, the joint most frequently affected by RRIs. 14 No recent review has integrated biomechanical and exposure-related risk factors exclusively for knee injuries in endurance runners across both amateur and elite populations. Addressing this gap may improve understanding of the causes of running-related knee injury and inform more targeted prevention efforts. Therefore, this systematic review aims to identify and synthesize the current evidence on biomechanical and exposure-related risk factors for knee injuries in adult endurance runners, defined here as individuals running distances of >10 km, to determine which factors are most consistently associated with knee injury development in this demographic.
Methods
This study is a systematic review of studies published before November 19, 2024, that investigated potential risk factors for knee injuries in endurance runners. A protocol for this study was prospectively registered on an international registry and complied with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines (Figure 1).

PRISMA flow diagram.
One author conducted an electronic search in Medline (PubMed), Embase (Ovid), and Web of Science (Clarivate) on November 19, 2024. The search was performed using a combination of the following 51 terms: (("Running"[Mesh] OR runn* OR runner*) AND ("Risk Factors"[Mesh] OR "Risk"[Mesh] OR "risk factors"[tiab] OR predict*[tiab] OR risk*[ot] OR "risk factors"[ot] OR predict*[ot])) AND (("Knee Joint"[Mesh] OR "Hamstring Tendons"[Mesh] OR "Hamstring Muscles"[Mesh] OR "Quadriceps Muscle"[Mesh] OR "Patellar Ligament"[Mesh] OR "Cartilage, Articular"[Mesh] OR "Lower Extremity"[Mesh] OR knee OR patellae OR patella OR patellar OR patellofemoral OR "iliotibial band" OR menisc* OR "medial collateral" OR "anterior cruciate" OR chondromalacia OR osteoarthritis OR arthritis OR quadriceps OR semitendinosus OR semimembranosus OR "biceps femoris" OR cartilage OR "lower extremity" OR "lower extremities" OR "lower limb" OR "lower limbs") AND ("Knee Injuries"[Mesh] OR "Tendon Injuries"[Mesh] OR injury OR injuries OR tear OR tears OR torn OR rupture* OR pain OR overuse OR stress OR osteoarthriti* OR arthriti*)). No restrictions were placed on the search in terms of language or publication date.
Three reviewers (K.S., M.N., S.W.) independently screened 1883 articles from the initial search using predetermined inclusion and exclusion criteria. Studies were first screened for inclusion based on title and abstract. Articles that passed abstract screening were advanced to full-text review. Conflicts were resolved by majority decision. Articles were included if they were observational/interventional studies or clinical trials observing runners aged ≥18 years who reported risk factors for knee injuries. Articles were excluded if they were case reports, non-English studies, review articles, studies focusing on nonendurance athletes (defined here as individuals running distances of <10 km), or studies focusing on athletes >30 years. Studies >30 years were excluded to preserve clinical and methodological relevance, given major changes in footwear technology, training practices, biomechanical assessment tools, and injury definitions.
Risk of bias was assessed using the Joanna Briggs Institute Methodological Quality Assessment Tool. All studies were evaluated against the appropriate critical appraisal checklists to determine the study's methodological quality. One reviewer (K.S.) independently assessed each included study. Studies judged to be at high risk of bias were excluded. Further details of the screening process are described in Figure 1.
One author (K.S.) extracted data from the eligible studies. The extracted data included study design, sample size, demographic characteristics, follow-up period, runner level (eg, recreational vs professional), injury type, and reported risk factors. Data were grouped first by all identified risk factors and then by knee injury subtype. Risk factors were first categorized into conceptual groups. For this review, biomechanical factors were defined as characteristics of movement patterns and forces during running, including kinematic factors (eg, peak hip adduction, pelvic drop, forward trunk lean) and kinetic factors (eg, ground-reaction forces, joint moments, joint loading patterns). Exposure-related factors were defined as variables related to training characteristics or runner background, including demographic characteristics, injury history, weekly mileage, running frequency, and footwear characteristics. Risk factors were also grouped by subtype. Subtypes included demographic characteristics, previous injury history, kinematic factors (defined as biomechanical characteristics related to the movement patterns of the body during running; eg, peak hip adduction, pelvic drop, forward trunk lean), kinetic factors (defined as biomechanical characteristics related to the forces acting on the body during running; eg, ground-reaction forces, joint moments, joint loading patterns), muscle strength and activation, structural malalignment, soft tissue flexibility and tightness, training load and volume, and footwear and equipment.
When available, odds ratios (ORs) were extracted. For studies that did not report this metric, standardized effect sizes (Cohen’s d or Pearson's r) were reported using available data. Effect sizes were extracted to allow comparisons across studies that reported different statistical measures. Because of substantial heterogeneity in study design, injury definitions, follow-up duration, and outcome reporting, statistical pooling was not feasible, and therefore, a meta-analysis was not attempted, thereby significantly limiting the generalizability of this study.
Results
The initial search produced 2587 studies, of which 704 were duplicates and were removed. Of the remaining 1883 studies, 1693 were excluded during title and abstract screening and full text review, leaving 26 studies that proceeded to risk of bias assessment and data extraction. Of these, 20 studies met the inclusion criteria and were included in the final review. Seven studies were case-control studies5,9,14,17,26,29,38, 4 studies21,22,27,43 were cross-sectional studies, 8 studies were cohort studies,7,13,15,24,31,37,39,45 and 1 study 34 was a randomized controlled trial. The mean follow-up ranged from 2 weeks before an endurance running event to 12 months. However, 10 studies did not report a follow-up period. Study characteristics are summarized in Table 1.
Identified Risk Factors for Running-Related Injuries a

AKP, anterior knee pain; BMI, body mass index; F, female; ITBS, iliotibial band syndrome; LoE, level of evidence; M, male; PFPS, patellofemoral pain syndrome; PT, patellar tendinopathy; RRI, running-related injury; SI, sacroiliac.
The included studies investigated risk factors for running-related knee injuries overall (n = 6), PFPS (n = 9), ITBS (n = 3), and PT (n = 2) (Table 1). Risk factors clustered into 2 categories: biomechanical (eg, kinematic and kinetic variables) and exposure-related (eg, training load, prior injury, demographic characteristics).
Across all injury types, the strongest risk factors were a history of previous injury, defined as any previous injury to either knee resulting in a change to knee function (reported OR range, 1.36-10.19), training load (defined as overall physiologic stress secondary to the training) or training volume (defined as weekly mileage) (OR range, 1.07-8.94), and structural malalignment (OR range, 1.89-4.12). Previous injury consistently emerged as the most powerful predictor, with odds of reinjury up to 10 times higher in runners with a previous RRI. Excessive or irregular training load also demonstrated moderate to strong associations with knee injury risk, while lower limb malalignments—such as varus knee alignment, pes planus, and abnormalities in patellar tracking or alignment (eg, lateral patellar tilt or subluxation)—were consistently linked to increased knee joint stress.
For general knee injuries, the strongest predictors of future injury risk were again a history of injury (reported OR range, 1.36-4.80), structural malalignment (OR range, 1.89-4.12), and higher training load or volume (OR range, 1.35-1.78). These estimates were primarily derived from Benca et al 5 (previous injury: OR, 1.36), Fokkema et al 15 (previous injury, OR, 4.80), Benca et al 5 (malalignment: OR, 1.89-4.12), 24 Fokkema et al 15 (training load: OR, 1.35), and Burke et al 7 (training load: OR, 1.78). Previous injury was the most frequently reported risk factor (study n = 5), with previously injured runners demonstrating a 12.9% higher incidence of new knee injuries. Additional risk factors for all knee injuries, along with the exact reported effect estimates, are summarized in Table 2. Effect estimates are ORs unless explicitly specified as Cohen's d or r.
Risk Factors for General Knee Injuries a
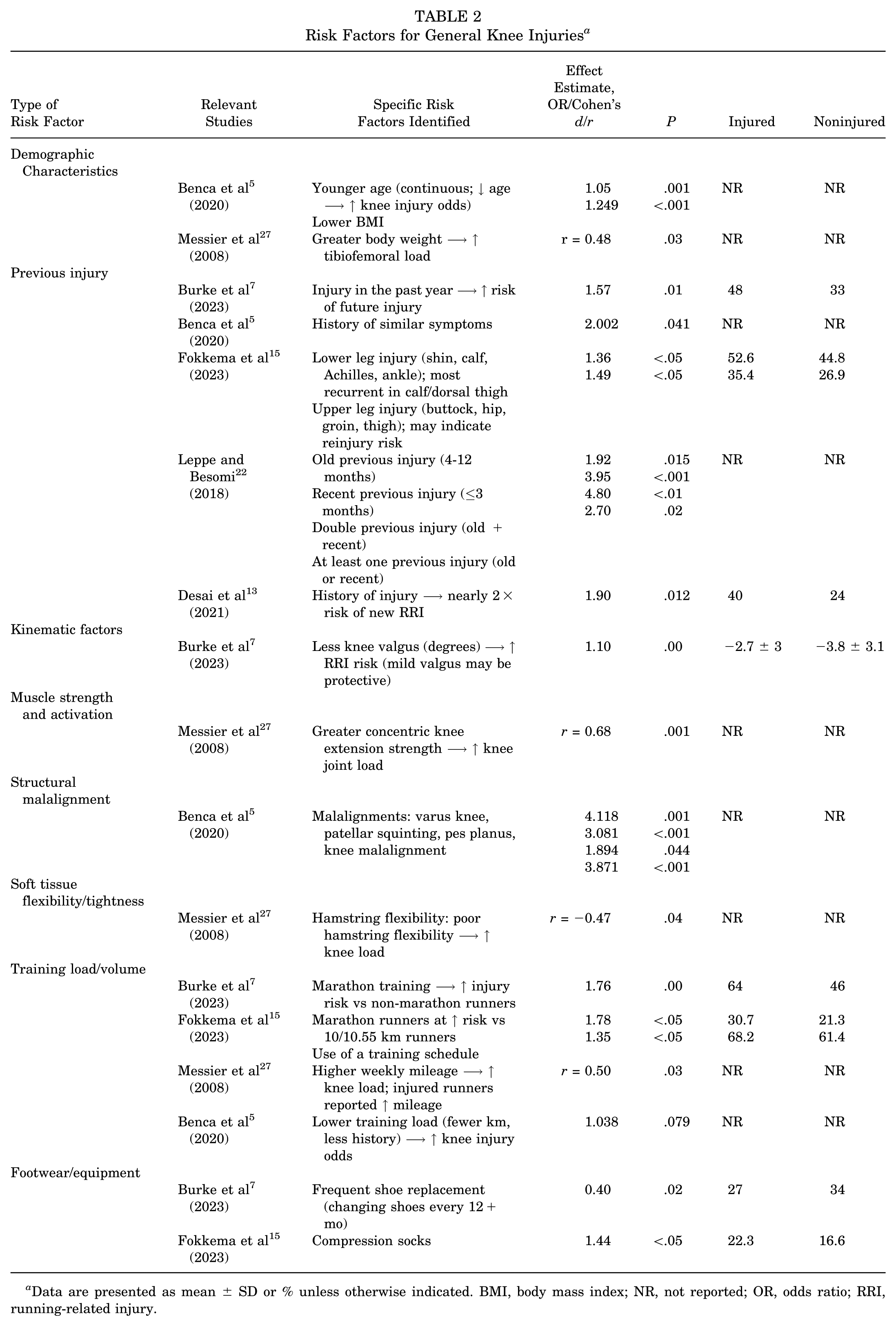
Data are presented as mean ± SD or % unless otherwise indicated. BMI, body mass index; NR, not reported; OR, odds ratio; RRI, running-related injury.
Across PFPS studies, the strongest predictors included measures of lower-extremity alignment (eg, forefoot varus [−0.5° to −0.4°], genu varum [−3;0.9° to −0.3°]) and patellofemoral biomechanics (eg, patellar maltracking; reported OR range, 3.09-3.60), kinematic variables such as pelvic obliquity (reported OR, 3.09), and higher training load or volume (reported OR range, 1.06-2.07). These estimates originated primarily from Benca et al 5 (malalignment: OR, 3.60; pelvic obliquity: OR, 3.09; training load: OR, 1.06-2.07). Training load and volume variables were the most frequently reported category of significant risk factors (study n = 4), with effect sizes (r range, 0.32-0.53; F-statistic range, 4.22-7.19) indicating small to moderate associations between increased or irregular training loads and the risk of knee overuse injuries. Runners with PFPS typically demonstrated 10% to 15% differences in weekly mileage or duration compared with their uninjured counterparts. Both undertraining 5 and overtraining 45 patterns were observed. Extrinsic load management factors, such as running frequency, surface, and footwear, also contributed to injury occurrence. 21
In ITBS, the strongest predictors were a history of injury (OR, 10.19), kinetic factors such as lower braking force (OR, 8.88), and higher training load or volume (reported OR range, 2.86-9.34). These values correspond to Benca et al 5 (previous injury: OR, 10.19) and Messier et al 26 (kinetic factors: OR, 8.88; training load: OR, 2.86-9.34). Kinematic (motion-related) variables were reported in 2 studies (reported OR range, 3.02-5.62; Cohen's d range, 1.24-2.21), as were kinetic (force-related) variables (reported OR, 8.88; Cohen's d: 0.819). Kinematic demonstrated large to very large effects. Kinetic demonstrated moderate to large effects. Cited kinematic factors included increased anterior pelvic tilt, increased hip flexion during stance, increased forward trunk lean over training, lower calcaneal to vertical touchdown angle, and higher supination velocity in injured runners compared with noninjured runners. Cited kinetic factors included increased hip adductor moment post-training and lower braking force in injured runners compared with noninjured runners. Taken together, these findings highlight the interplay between abnormal lumbopelvic control and altered force attenuation as key contributors to ITBS development.
Finally, for PT, the strongest predictors were higher training load or volume (reported OR, 8.94), structural malalignments, such as knee genu varum or genu valgum (reported OR, 3.15), and a history of injury (reported OR, 2.10). These effect estimates were drawn from Morton et al 27 (training load: OR, 8.94; previous injury: OR, 2.10) and Benca et al 5 (malalignment: OR, 3.15). The most frequently reported risk factors were increased training load/volume (study n = 2; reported OR range, 1.27-8.94) and demographic variables (study n = 2; reported OR range, 1.06-1.43). Effect estimates for training-related factors indicated moderate-to-very-large associations between excessive weekly training exposure and PT risk. Runners who trained >20 hours per week demonstrated a mean 15% to 20% higher incidence of PT compared with their uninjured counterparts. Among demographic variables, male sex and younger age were most consistently associated with PT, suggesting increased susceptibility for injury development in younger, high-volume male runners. Tables 3 to 5 detail risk factors for PFPS, ITBS, and PT, with the exact reported effect estimates, respectively. Effect estimates are ORs unless explicitly specified as Cohen's d or r.
Risk Factors for Patellofemoral Pain Syndrome a

Data are presented as mean ± SD, mean (range), or %, unless otherwise specified. BM, body mass; BMI, body mass index; BWS, body weight-supported; F, female; M, male; NR, not reported; OR, odds ratio; PFPS, patellofemoral pain syndrome; RF, rectus femoris; RRI, running-related injury; SI, sacroiliac; VMO, vastus medialis obliquus.
Risk Factors for Iliotibial Band Syndrome a

Data are presented as mean ± SD, unless otherwise indicated. BMI, body mass index; BW, body weight; ITB, iliotibial band; ITBS, iliotibial band syndrome; NR, not reported; OR, odds ratio; RRI, running-related injury.
Risk Factors for PT a

Data are presented as % or (range), unless otherwise indicated. NR, not reported; OR, odds ratio; PT, patellar tendinopathy.
Discussion
This systematic review identified 3 primary risk factors for running-related knee injuries in endurance runners: a history of injury, higher training load or volume, and selected kinematic variables, with variation by injury subtype. Across the 20 included studies, previous injury emerged as the most consistent predictor, training load demonstrated moderate associations with injury development, and kinematic findings were heterogeneous but relevant in specific subgroups. Together, these findings indicate that knee injury risk in runners reflects interactions between both biomechanical and exposure-related contributors rather than a single dominant factor. Notably, many of the strongest predictors identified, including previous injury history and certain biomechanical characteristics, are not directly modifiable. In contrast, training load represents a potentially modifiable factor. However, the extent to which modifying training load reduces injury risk remains uncertain.
Eight studies identified a previous history of RRIs as a predictor of future RRI, with up to a tenfold increased odds of subsequent injury.5,7,13,15,22,29,43,45 This finding is consistent with previous reviews. For example, Saragiotto et al 35 synthesized data from 4671 pooled participants and examined 60 different predictive factors and reported that a history of RRI within the previous 12 months was the most consistent risk factor. Similarly, van Poppel et al 41 reported that previous injury was the strongest risk factor across both short- and long-distance groups. This suggests that, regardless of distance, inadequate recovery after a previous RRI predisposes runners to develop future RRIs. 41 Expanding further, Correia et al, 10 in an umbrella review, identified previous musculoskeletal injury as one of the most consistently reported risk factors for RRIs across the umbrella evidence, further demonstrating that previous injury is a repeatable, cross-study finding, reinforcing its role despite heterogeneity in study designs and injury definitions.
Clinically, these findings underscore the value of consistently screening for previous injury when evaluating endurance runners. A history of injury may reflect incomplete tissue recovery, persistent neuromuscular deficits, or altered loading patterns, all of which may increase susceptibility to reinjury. Possible physiologic explanations for the increased risk include incomplete tissue healing, maladaptive movement patterns, or preexisting biomechanical deficits that may be exacerbated by a premature return to sport (RTS).3,4,16 However, as previous injury is not modifiable, its primary utility may lie in risk stratification rather than direct intervention. Runners with a history of RRI may benefit from close monitoring, individualized rehabilitation, and cautious RTS progression to reduce the likelihood of injury recurrence. Future research should aim to clarify these intertwined mechanisms while also standardizing definitions of previous injury. Doing so will both refine RRI risk prediction models and translate this well-established association into evidence-based interventions.
Eight studies identified training load and volume-related factors, such as greater weekly mileage and number of hours training, as contributors to RRI risk.5,7,14,15,26,27,29,45 This aligns with systematic reviews by Kakouris et al, 20 Damsted et al, 11 van der Worp et al, 40 and Nielsen et al, 32 which reported associations between higher overall training loads and increased injury risk. Although variability in study quality limits generalizability, the pattern across reviews supports an association between high training load and injury risk. 12 From a clinical perspective, these findings highlight an association between higher training loads and injury risk. However, the extent to which specific load-management strategies, such as gradual progression or avoidance of abrupt changes, reduce injury incidence remains unclear. While approaches such as gradual progression and avoidance of abrupt increases in training are commonly recommended, the current evidence base does not definitely establish their effectiveness in reducing injury incidence. As such, recommendations regarding training modification should be interpreted cautiously and tailored to the individual runner.
Finally, 6 of the included studies reported kinematic factors, such as asymmetrical loading and increased forward trunk lean, as predictors of future RRIs.4,7,14,26,37,45 This finding is partly consistent with existing literature, although prospective evidence remains sparse and heterogeneous. For example, Ceyssens et al 8 synthesized 16 prospective studies and found limited evidence linking peak hip adduction to PFPS and ITBS in female runners. Vertical loading rates and overall RRIs were inconsistent across the studies reviewed in this review, thereby leading the authors to conclude that kinematic risk factors appear to be injury and population-specific rather than universal. Vannatta et al 42 reported similar findings and argued that pooling across heterogeneous runner groups may obscure meaningful associations. The authors noted that hip adduction and rearfoot eversion appeared more relevant in certain subgroups, particularly female recreational runners. 42 Reviews by Peterson et al 33 and Lopes et al 23 also reported factors such as lower hip adduction velocity, reduced knee extension strength, and increased peak hip adduction angle as predictors of RRI incidence, but emphasized heterogeneity across the reviewed articles.
In the clinical context, variability in biomechanical findings across studies may reflect differences in runner characteristics, running conditions, and methodological approaches. This heterogeneity complicates direct comparison and may limit the generalizability of kinematic predictors. As many biomechanical characteristics are not easily modifiable, their primary role may be to identify at-risk individuals rather than serve as direct targets for intervention. Thus, individualized biomechanical assessments may be more clinically useful than relying on universal kinematic thresholds.
Thus, when examining trends in risk factors for knee injuries in endurance runners, our findings, along with the existing literature, suggest that clinicians should integrate 3 core elements when treating RRIs in this demographic: assessment of injury history, recognition of training load as a contributing factor, and individualized biomechanical evaluation rather than reliance on single generalized markers. Importantly, many identified risk factors may be better suited to risk stratification than to direct modification. Several identified predictors, including injury history and certain biomechanical characteristics, are not readily modifiable and may instead serve to identify runners at elevated risk. In contrast, training load represents a potentially modifiable exposure; however, optimal strategies for reducing injury risk through load modification remain unclear. Collectively, these findings support an individualized approach that emphasizes risk identification while acknowledging current limitations in evidence for targeted prevention strategies.
Limitations
This study had numerous limitations that warrant consideration. The predominance of observational study designs limits causal inference. Cross-sectional studies only capture a single time point, making it difficult to determine whether risk factors precede or follow injury. In addition, follow-up durations were inconsistent or unreported in half of the studies, potentially underestimating injury rates or obscuring true associations. Another important limitation is the heterogeneity in injury definitions and outcome measures across studies, which complicates direct comparison and may contribute to inconsistent findings. In particular, definitions of RRIs varied substantially, ranging from any musculoskeletal pain during running to injuries requiring medical consultation or time loss, making synthesis across studies less precise. Furthermore, the absence of high-quality studies with substantial sample sizes limits the generalizability of the association presented here. Publication bias is also a concern, as much of the current literature focuses on biomechanics rather than exposure-related factors, thereby potentially skewing the balance of evidence.8,23,33 In addition, this systematic review excluded non-English articles and gray literature, potentially omitting relevant but unpublished data. Finally, a formal meta-analysis was not performed due to substantial clinical and methodological heterogeneity across studies, which precluded meaningful statistical pooling.
Conclusion
The risk of knee injury remains high among endurance runners and is influenced by both biomechanical and exposure-related factors. This review found that previous injury, increased training load, and kinematic factors were the most commonly identified and strongest risk factors, with variation by injury type. These findings emphasize that knee injury susceptibility in endurance runners arises from multiple interacting factors rather than a single dominant mechanism.
Footnotes
Final revision submitted March 25, 2026; accepted March 30, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.G. is a reviewer for The American Journal of Sports Medicine. An immediate family member of S.W. is employed by Stryker in a non-orthopaedics division.