
Abstract
Background:
Changes in joint contact force distribution after injury are 1 factor driving tissue degeneration. Although clinical interventions aim to restore forces to their uninjured state, inconsistent outcomes suggest that patient variability in joint contact mechanics remains poorly understood, despite the use of patient-specific computational models that are too labor-intensive to be widely adopted. A more practical solution may involve grouping knees by commonalities in force distribution, enabling recognition of heterogeneity without requiring fully individualized models.
Hypothesis/Purpose:
The objective of this study was to determine whether human cadaveric knees can be grouped based on differences in joint contact force distribution across the tibial plateau during the stance phase of simulated gait. We hypothesized that a subset of knees would heavily rely on the meniscus (“meniscal-dominant loaders”) and another subset of knees would distribute more force through cartilage-to-cartilage contact (“cartilage-dominant loaders”). Our secondary hypothesis was that cartilage-dominant loaders would have their peak contact stress in the cartilage-cartilage contact region, and those with meniscal-dominant loading would have peak contact stress primarily located in the meniscus footprint.
Study Design:
Descriptive laboratory study.
Methods:
Cartilage-cartilage and meniscal footprints were identified on contact force data across the tibial plateaus of cadaveric knees (n = 44) subjected to simulated gait. Knees were grouped based on force distribution on the medial or lateral plateaus using K-means clustering. They were characterized as meniscal dominant loaders if >50% of the compartment load was acting through the meniscus for >50% of the simulated gait cycle. Knees were characterized as cartilage-dominant loaders if >50% of the compartment load was acting through the cartilage-to-cartilage contact zone for most of the gait cycle.
Results:
On the medial plateau, 4 clusters were identified. These clusters ranged from cartilage-dominant loaders (Cluster 1 [7% of knees]) to meniscal loaders (Cluster 4 [48% of knees]). Knees in Cluster 2 (20% of knees) and 3 (25% of knees) were meniscal-dominant loaders in early stance and switched to cartilage-dominant loading in late stance. The peak contact stress shifted from the cartilage-cartilage region in cartilage-dominant loaders to the meniscus footprint in meniscal-dominant loaders. On the lateral plateau, 3 clusters were identified. These clusters again ranged from cartilage-dominant loaders (Cluster 1 [11% of knees]) to meniscal-dominant loaders (Cluster 3 [72% of knees]). Knees in Cluster 2 (17% of knees) equally shared load between the cartilage and meniscus. No differences were found in peak stress between cartilage-dominant loaders and meniscal-dominant loaders on the lateral plateau.
Conclusion:
We confirmed that human cadaveric knees can be stratified based on the distribution of load through menisci and that peak pressures were higher in the cartilage-dominant loading knees.
Clinical Relevance:
This study identifies heterogeneity in how human cadaveric knees distribute forces during simulated gait. This information is fundamental to understanding and improving upon the biomechanical variability in the knee's response to injury and repair.
Changes in joint contact force distribution have been implicated as a key mechanical factor driving tissue degeneration and posttraumatic osteoarthritis (PTOA).7,18,19,24 Many clinical techniques leverage this conceptual underpinning to reduce the risk of joint degeneration in injured knees. Some clinical examples include tibial osteotomy to redistribute knee joint loads away from painful, damaged regions of the joint4,22,27; reduction of knee laxity after anterior cruciate ligament (ACL) reconstruction with lateral extra-articular tenodesis to reduce ACL forces14,32,37; and clinical evaluation of scaffolds prioritized for use in the medial meniscus, which is less mechanically demanding than the lateral meniscus.20,23 However, the success of these techniques in delaying progression of joint degeneration is variable,19,30 suggesting that we do not adequately understand knee-to-knee variability in joint contact mechanics.
To address variability in outcomes, patient-specific models are being built from magnetic resonance imaging scans and motion analysis data.16,17,34 These models are labor-intensive to build, validate, and incorporate into clinical workflows; therefore, it remains unclear whether “one-off” personalized models will ever become mainstream. There may be a balanced approach between generalizing to the population and using patient-specific models. This balanced approach could utilize deep learning approaches to group specimens based on defining features, such as joint load distribution. This approach could avoid the need for one-off, resource-intensive, personalized models while recognizing the heterogeneity that exists. Exploring heterogeneity in intact uninjured knees during a simulated activity of daily living is a necessary step in this direction.
This study aimed to determine whether human cadaveric knees can be grouped based on differences in joint contact force distribution across the tibial plateau during the stance phase of simulated gait. Given the key role of the meniscus in distributing loads across the knee joint 1,9,15 we hypothesized the existence of a subset of knees that rely heavily on the meniscus (“meniscal-dominant loaders”) and a subset of knees that distribute more force through cartilage-to-cartilage contact (“cartilage-dominant loaders”). Our secondary hypothesis was that cartilage-dominant loaders would have their peak contact stress in the cartilage-cartilage (C-C) contact region, and those with meniscal-dominant loading would have peak contact stress primarily located in the meniscus footprint.
Methods
Gait Simulator
Data from 44 human cadaveric knees (16 female, 28 male; mean 56 years [range 29-76 years]) (Hospital for Special Surgery Institutional Review Board approval No.: 2016-0071) were used in this study. Knees were excluded if donors had a history of osteoarthritis (OA), osteoporosis, or rheumatoid arthritis; previous knee surgery to either side; or any history of cartilage or meniscal defects. A further visual inspection was performed before testing; if evidence of arthritis or meniscal/cartilage damage was present, the knee was excluded from testing. The data were extracted from a combination of previously published studies6,9 (n = 18) and from unpublished studies (n = 26), all of which quantified contact forces across the tibial plateau under simulated gait on a VIVO knee gait simulator (AMTI) using identical sample preparation, testing, and data analysis protocols. In brief, cadaveric knees were prepared and run through simulated gait as previously described in Chastain et al 9 using inputs from 36 International Organization for Standardization standard No. 14243-1. The knees were prepared by removing the skin, muscle, and patella, while preserving all soft tissues (eg, ACL, posterior cruciate ligament, medial collateral ligament, lateral collateral ligament, and posterolateral corner) around the joint capsule except for the patellar tendon. An electronic pressure sensor (Model 4011; Tekscan Inc), augmented with plastic tabs, was sealed between 2 layers of Tegaderm adhesive dressing (3M), equilibrated using a Tekscan pressure bladder, and calibrated on a mechanical testing system to 1.5 times the expected loads for the intact knee, placed across the tibial plateau under the menisci, and secured to the posterior capsule and ACL with sutures. The contact stress on the tibial plateau of the medial and lateral compartments of all knees was collected throughout the stance phase of simulated gait (0%-60%), at a frequency of 100 Hz (Figure 1A). A custom MATLAB program (Mathworks Inc) 11 was used to manually segment the C-C contact region from each specimen through the stance phase of gait on the medial and lateral plateaus (Figure 1A). The meniscal footprint (M) contact region was taken as the inverse of the identified C-C contact region on the corresponding plateau. The total stress in the C-C and M contact regions was exported for further analysis.
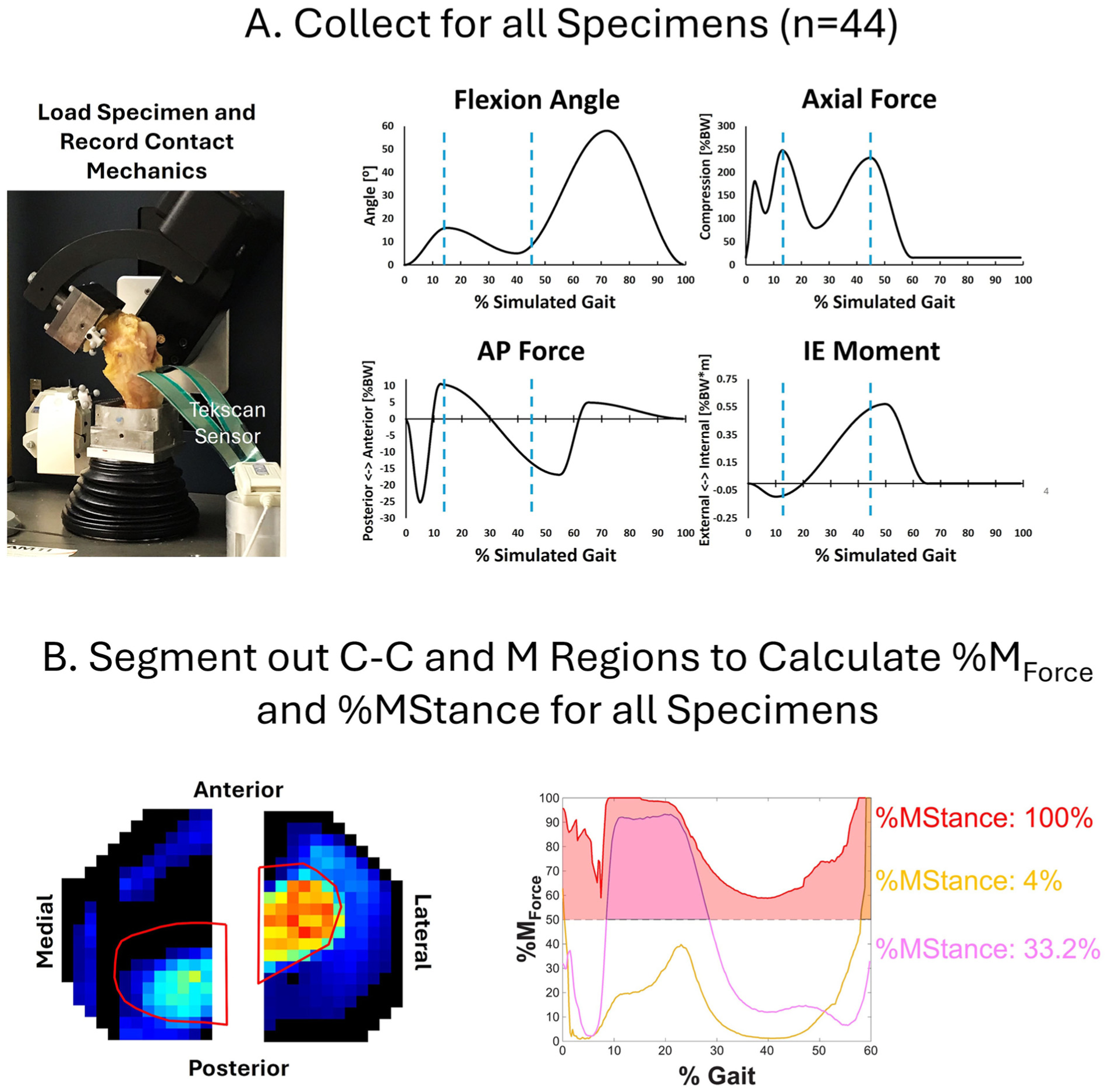
Workflow for clustering analysis. (A) Contact mechanics data were collected for simulated gait using a Tekscan sensor. Gait was performed using the specimen's BW according to ISO 14243-1. (B) Regions of interest were segmented for the C-C contact region on the medial and lateral plateau (red outlines). The %MForce was calculated for all specimens and further reduced to %MStance. AP, anteroposterior; BW, body weight; C-C, cartilage-cartilage; IE, internal-external rotation; ISO, International Organization for Standardization.
Data Dimensional Reduction
The percent meniscal loading at each point of the stance phase of the gait cycle was calculated as

where FM is the sum of the forces within the M, and FC-C is the sum of the forces within the C-C region during the stance phase. The total percentage of the stance phase during which >50% of compartment force was through the M (%MStance) was then calculated and used as input for unsupervised clustering (Figure 1B).
K-means Clustering
K-means clustering was used to group knees by %MStance. K-means clustering is an unsupervised clustering algorithm that assigns each specimen to clusters (k) based on the proximity of the specimen %MStance to the determined %MStance data cluster center. The algorithm attempts to minimize the distance between the specimen data and the data center location of its assigned cluster. MATLAB was used to perform the clustering analysis. The initial number of clusters, kinit, was chosen by minimizing the sum of squared errors for each specimen to its cluster centroid for all possible cluster numbers, kn, via the elbow method. 35 For each kn, 50 replicate runs were performed, and the run with the lowest total sum of distances value was used for each cluster centroid. Further optimization of the cluster number was performed by using silhouette plots. 29 See Supplement 2 for more details on the clustering approach. For each cluster, the mean and standard deviation of the specimens’ %M values were plotted across the stance phase of gait (0%-60%).
Cluster Descriptive Statistics
Data analysis of the clustered data was performed at 14% and 45% of gait, which correspond to the 2 peaks of axial load during the gait cycle (Figure 1A, blue dotted lines). Three metrics were analyzed: (1) total force; (2) contact area; and (3) peak pressure in 3 regions of interest on either the medial or lateral compartments: (1) whole compartment; (2) C-C contact region; or (3) M contact region.
Statistical Analysis
A multiple linear regression was run in GraphPad Prism Version 10.6.1, with %MStance as the dependent variable. Independent variables include age, sex, laterality (right/left knee), height, and weight. Since only 44 knees were available for this study, the study model used only main effects within a least-squares approach. For the data collected at 14% and 45% of gait, a 1-way analysis of variance was performed between clusters. A Tukey post hoc test was performed to determine significant differences between groups (P < .05, α = .95).
Results
Simulated Gait: Cluster Analysis
Medial Plateau. Four unique clusters of knees were identified based on how force was distributed across the medial tibial plateau throughout the stance phase of simulated gait. Also, 7% of knees were in Cluster 1, in which knees were cartilage-dominant loaders; 48% of knees were in Cluster 4, in which knees were meniscal-dominant loaders; and 45% of knees had variable levels of meniscal and cartilage loading throughout the stance phase of the simulated gait cycle (Figure 2A and Figure 3). The overall mean waveform was predominantly within the meniscal-loading region (Figure 2B), with a pattern following the same trend as Clusters 2 and 3 (meniscal-dominant loading around 14% and cartilage-dominant loading at 45%).
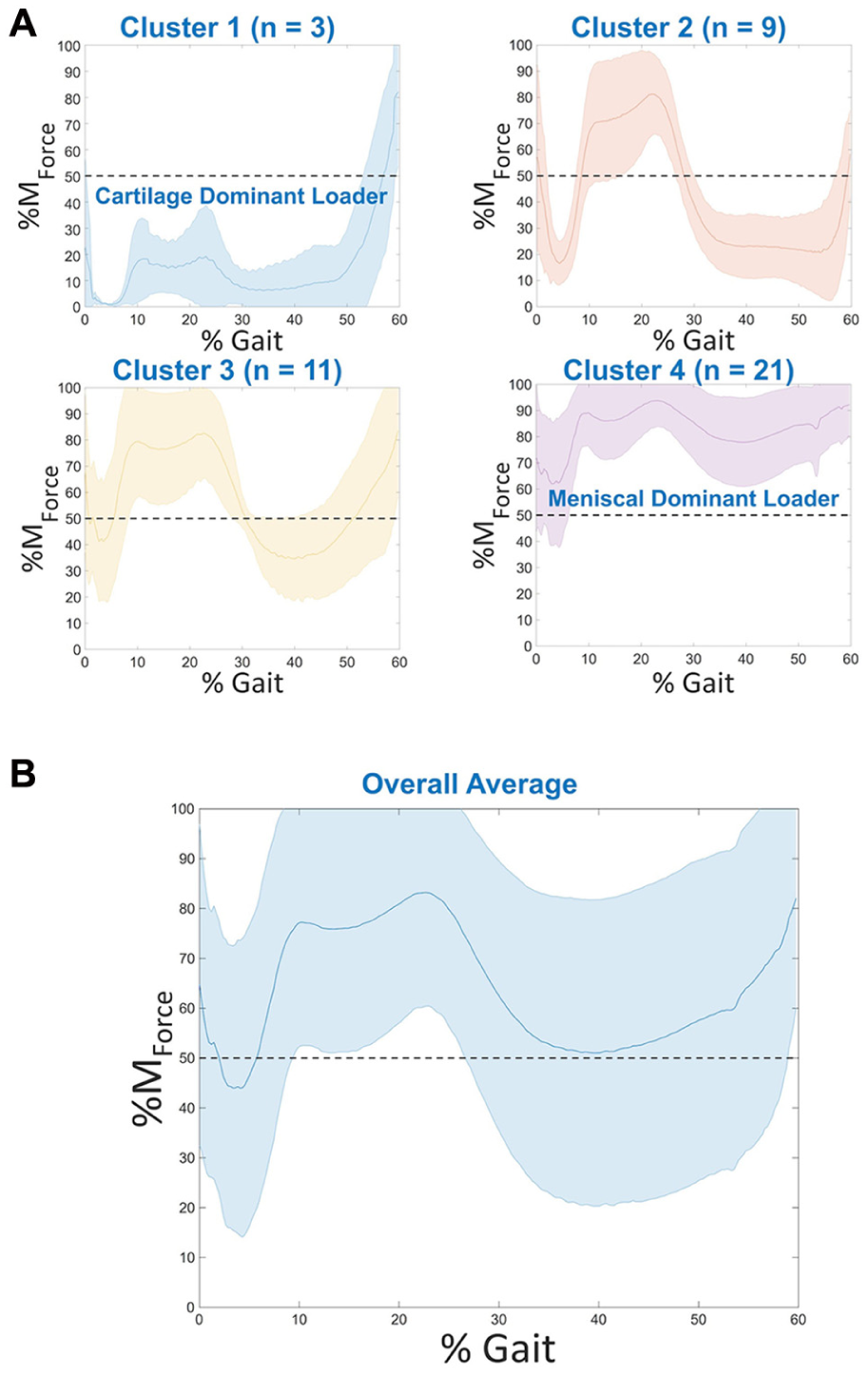
%MForce on the medial plateau through stance. (A) The medial %MForce with mean (solid line) and standard deviation (shaded regions) for identified clusters. (B) The mean (solid line) and standard deviation (shaded regions) across all specimens (overall mean) for the medial %MForce. Cluster 1 includes the cartilage-dominant loaders, and Cluster 4 includes the meniscal-dominant loaders.

Representative heat maps of the medial compartment are shown. The red-outlined region indicates the location of the cartilage-cartilage contact. Cluster 1 is a cartilage-dominant loader, while Cluster 4 is a meniscal-dominant loader.
Lateral Plateau. Three distinct knee clusters were identified based on how force was distributed across the lateral tibial plateau throughout the stance phase of simulated gait. Also, 11% of knees were in Cluster 1, in which knees were cartilage-dominant loaders; 72% of knees were in Cluster 3, in which knees were meniscal-dominant loaders; and 17% of knees had approximately equal levels of meniscal and cartilage loading throughout the stance phase of the simulated gait cycle (Figures 4 and 5).

%MForce on the lateral plateau through stance. (A) The lateral %MForce with mean (solid line) and standard deviation (shaded regions) for identified clusters. (B) The mean (solid line) and standard deviation (shaded regions) across all specimens (overall mean) for the lateral %MForce.

Representative heat maps of the medial compartment are shown. The red-outlined region indicates the location of cartilage-cartilage contact. Cluster 1 is a cartilage-dominant loader, while cluster 3 is a meniscal-dominant loader.
Multiple Linear Regression Analysis. A multiple linear regression was run on the demographic data versus %MStance. Male sex had a significant influence on %MStance of the knees (P = .02978), whereas the remaining variables did not. However, there was a weak correlation between demographic data and the %MStance with an R2 of 0.1332.
Total Force, Contact Area, and Peak Pressures at 14% and 45% of Gait. No differences were found in total force, area, or peak pressure on either the medial or lateral plateaus (data not shown). Differences between Clusters 1 and 4 were found in the total force, contact area, and peak pressure in the C-C region at both 14% and 45% of gait (Figure 6). Additionally, the total force and peak pressure at 14% of gait were significantly decreased from Cluster 1 to Clusters 2 and 3 in the C-C region. Cluster 2 was significantly different from Cluster 4 at 45% of gait in total force and peak force.
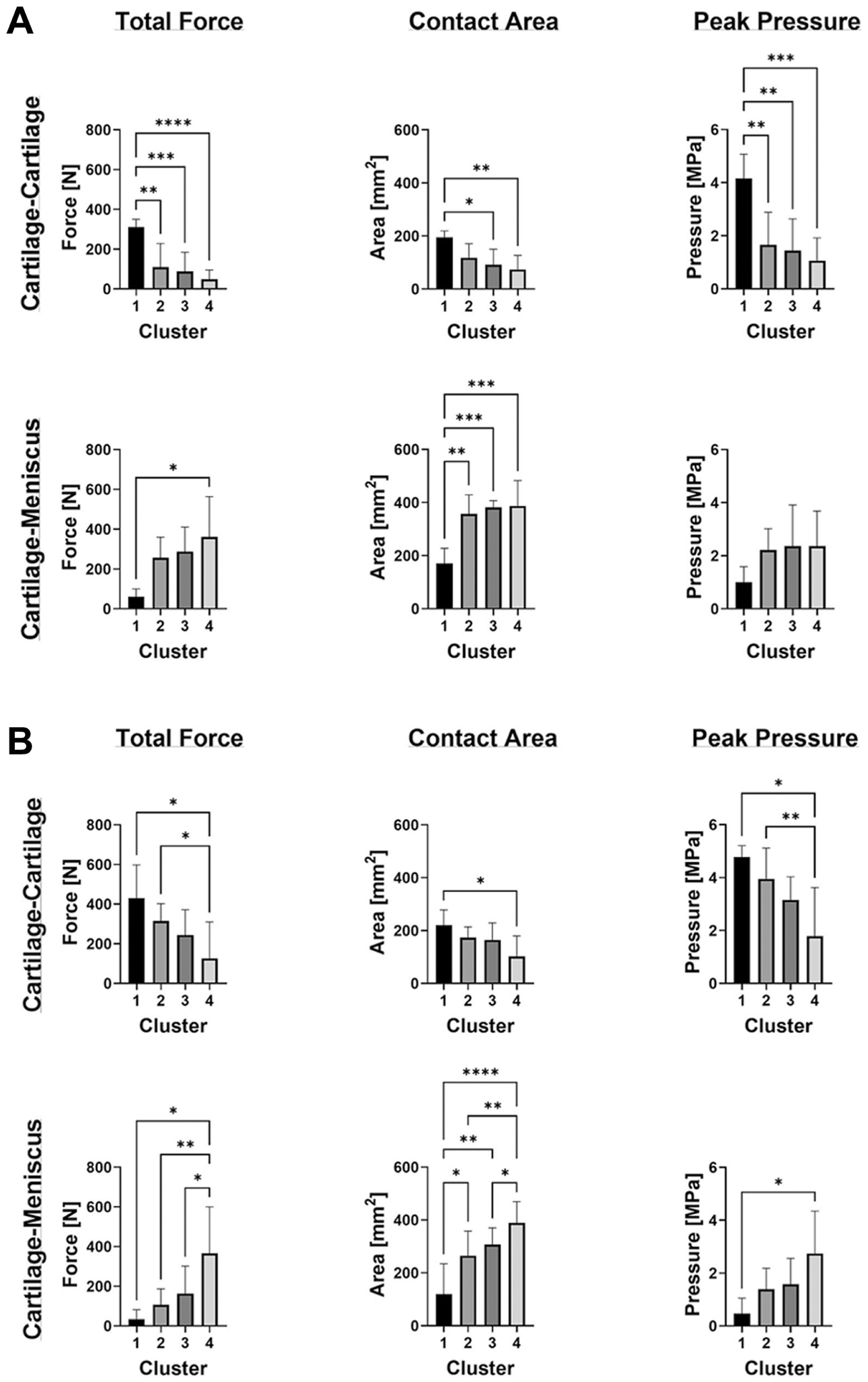
Total force, contact area, and peak pressure on the medial plateau. Total force, contact area, and peak pressure are shown at (A) 14% and (B) 45% of gait for the C-C and (M) regions. Bar graphs represent the mean and standard deviation for each cluster.
In the M region, the total force and contact area increased significantly between Clusters 1 and 4 at 14% of gait (Figure 6). At 45% of gait, the total force, contact area, and peak pressures in Cluster 4 were significantly increased from those in Cluster 1. There were also significant differences in total force and contact area at 45% of gait from Clusters 2 and 3 to Cluster 4.
On the lateral plateau, the total force decreased between Cluster 1 and Cluster 3 at 14% of gait in the C-C region (Figure 7). The contact area also decreased by 45% in the C-C region between Clusters 1 and 2, and between Cluster 3 and the others. No differences were found in the peak pressure at 14% and 45% in the C-C region. No differences in total force, contact area, or peak pressure were seen in the M region at 14% or 45% of gait.

Total force, contact area, and peak pressure on the lateral plateau. Total force, contact area, and peak pressure are shown at (A) 14% and (B) 45% of gait for the C-C and M regions. Bar graphs represent the mean and standard deviation for each cluster.
Discussion
By analyzing force distribution across the medial and lateral plateaus of 44 human cadaveric knees subjected to simulated gait, we accepted our hypothesis that human cadaveric knees can be stratified based on the percent of compartment force distributed through the meniscus. We identified knees that were meniscal-dominant loaders, knees that were cartilage-dominant loaders, and a combination thereof. We also found that the total force and peak pressures in the C-C contact region of the cartilage-dominant loaders (Cluster 1) were significantly higher compared with those in meniscal-dominant loaders (Cluster 4). Our study demonstrates that stratifying knees by the distribution of forces across the plateau is a feasible approach to unmasking differences obscured by averaging and represents a new paradigm for characterizing knee biomechanical behavior.
The concept of exploring the distribution of compartment loads between the M and the CC contact areas is not new.13,33 Nonetheless, cadaveric and computational models that quantify contact force distribution are predominantly based on sample sizes determined to have adequate power to detect significant differences caused by simulated injury or repair, with typical studies including 6 to 10 knees.1,2,6,9,10,15,31 Moreover, an analysis of the contact mechanics of uninjured knees has only been reported for 5 knees, 15 and as such did not capture inherent variability. The present study is unique—it reports upon one of the largest cohorts of cadaveric knees (n = 44), from a wide range of donors, all subjected to similar test conditions. Our key finding, that averaging contact data masks inherent variability in the role the meniscus plays, has implications for clinical care. One example of this is the current clinical practice for meniscal tears.
Variability in outcomes after meniscal surgery is a clinical challenge that requires a solution. Partial meniscectomy of the lateral meniscus leads to rapid PTOA progression. 25 Our finding that a majority of knees (72%) were clustered in the meniscal-dominant phenotype (Cluster 3) on the lateral plateau gives credence to the idea that if patients biomechanically rely on their meniscus, they may be more affected by an injury to the meniscus. 8 In the medial compartment, we found that 48% of knees fell into the dominant meniscal loaders cluster (Cluster 4). According to clinical data, 50% of patients who undergo medial partial meniscectomy develop OA 10 to 20 years after treatment.3,19,24,28 Patients at risk of OA could be those who are “uninjured” meniscal-dominant loaders who are more detrimentally affected by an injury/removal of a portion of the meniscus. This understanding of intact knees can be used to study cadaveric knees after medial partial meniscectomy to understand the contribution of specimens in their intact state, being meniscal-dominant loaders versus cartilage-dominant loaders, on contact mechanics changes after partial meniscectomy.
Our finding that peak pressures in the C-C contact region of the cartilage-dominant loaders (Cluster 1) were significantly higher compared with those in meniscal-dominant loaders (Cluster 4) supports the concept that, in bypassing the meniscus, forces become concentrated in a smaller zone. It is possible that variations in cartilage thickness and modulus values in the C-C and M regions,5,12 are in response to the forces that these zones experience, highlighting the importance of better understanding the loading environment of each region. It is also possible that, in designing scaffolds or implants to replace and repair damaged menisci and cartilage, the intact knee's loading environment should be considered. For example, meniscal-dominant loaders may require higher modulus constructs for meniscal replacement than their cartilage-dominant counterparts.
This study is not without limitations. The Tekscan sensors used have inherent errors in measuring contact on curved surfaces 21 and under dynamic loads 26 ; however, as this study compares relative contact areas and measures the relative contribution of the meniscus in load distribution, the accuracy of the sensors is less critical to the study outcome. There can also be errors in sensor placement, especially in the lateral compartment, which could underreport meniscal contact, as seen in the heat maps in Figures 2C and 3C. Even with these placement errors, most knees were meniscal dominant on the lateral plateau, suggesting that these errors were not large enough to affect the meniscus's contribution to load-bearing in the lateral compartment. The meniscus and cartilage regions of interest were manually determined on the Tekscan maps, which could lead to inherent error in the identification of the cartilage and meniscal regions. This limitation was addressed by ensuring that all regions of interest were identified by individuals with proper training, as described in Chen et al. 11 With the limited number of cadaveric specimens in each cluster, it was not possible to perform appropriately powered statistical analysis to determine demographic or geometric (femoral and tibial) parameters that correlate with the specimen cluster. However, we have used the continuous data, %MStance, to define the clusters and determine any correlations with demographic data. From this analysis, there was a weak correlation between demographic data and %MStance, with male sex making a significant contribution. Future studies will leverage finite element modeling to vary the geometric and soft-tissue properties of a patient model to identify key factors that determine the mechanical loading phenotype.
The findings of this study suggest that taking a more specimen-specific approach to studying joint contact mechanics may improve understanding of how different patient populations respond to injury and treatments. This would ultimately help identify the most appropriate, least invasive treatment to ensure long-term joint health after injury intervention in these populations. Future work will investigate correlations between geometric (both bony and soft-tissue), demographic, and mechanical properties (eg, laxity) of the joints, as well as explore any correlations between changes in injury contact mechanics and intact specimen cluster membership.
Footnotes
Supplement 1:
Supplement 2:
Final revision submitted March 11, 2026; accepted March 24, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: The authors received National Institutes of Health funding for this study (R01 AR066635 and R01 AR075523) and support from the Russell Warren Chair in Tissue Engineering at Hospital for Special Surgery.
Ethical approval for this study was obtained from the Hospital for Special Surgery Institutional Review Board (No.: 2016-0071).