
Abstract
Background:
Ultrasound (US) screening for cam morphology in athletes is rarely performed. Conventional US imaging in the neutral hip position may overlook cam lesions in the anterolateral position, which is the most common location that exhibits cam morphology.
Purpose:
To investigate US-detected cam-related morphology and prominence in male collegiate soccer players using US with an additional 15° hip extension view and to examine their associations with groin symptoms and functional impairments.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
This voluntary screening study included 55 male collegiate soccer players (110 hips; mean age, 19.5 ± 1.1 years) from a single varsity team, all of whom were active and without hip or groin pain severe enough to limit soccer participation. US imaging of the femoral head-neck junction was performed in the neutral position and at 15° of hip extension using a linear probe. The femoral morphology on US was classified as normal, flattened, or prominent; and flattened or prominent findings were grouped as cam-positive for analysis. Groin pain and pinching sensations were assessed using questionnaires and flexion adduction internal rotation tests. Four functional parameters were evaluated, and logistic regression analyses were performed to identify factors associated with the current symptoms.
Results:
US-based cam-positive morphology was identified in 97 hips (88%) and prominence in 53 hips (48%). The detection rate of US-based cam-positive morphology increased from 79% at 0° to 88% at 15° of hip extension (P = .02), and that of prominence increased from 21% to 48% (P < .0001). Groin pain was present in 25 hips (19%), and pinching sensation was reported with 49 hips (45%). In cam-positive hips, having ≥3 functional deficits (odds ratio [OR], 5.0) and greater side-to-side internal rotation difference (OR, 1.2) predicted groin pain; the same variables (OR, 10.2 and 1.1, respectively) predicted pinching sensation. In prominence-positive hips, ≥3 functional deficits predicted groin pain (OR, 6.5) and pinching sensation (OR, 6.9).
Conclusion:
US screening with 15° hip extension improved the detection of anterolateral cam-related morphology in male collegiate soccer players. Current symptoms were more strongly associated with multiple functional impairments than with morphology alone.
Femoroacetabular impingement (FAI) is a well-recognized cause of hip and groin pain in athletes, and cam morphology is its predominant structural feature. 13 Prospective studies have shown that cam morphology often develops during skeletal maturation in young soccer players, suggesting a sport-specific adaptation to repetitive high-load movements.2,26 Cross-sectional studies on professional soccer players have confirmed a persistently high prevalence of cam morphology. 3 These findings suggest that early structural adaptations may persist into adulthood and contribute to hip-related symptoms or performance limitations during competition. Early detection of cam morphology in young athletes may be critical for preventive screening and load management, given that groin and hip injuries remain among the most frequent time-loss conditions in soccer.24,27
Radiographic evaluation, particularly the 45° Dunn view, is considered the most reliable method for detecting anterolateral cam morphology. 21 However, routine radiographic or magnetic resonance imaging (MRI) screening in large athletic populations may be impractical because radiographs involve radiation exposure, whereas MRI is more resource-intensive, costly, and less accessible. 16 Ultrasound (US) has recently gained attention as a practical alternative in sports medicine because it enables dynamic, radiation-free, bedside evaluation of the hip joint. 20 Several studies have reported that US can identify cam morphology with acceptable diagnostic accuracy and interrater reliability.14,15 Nonetheless, limitations remain: US cannot visualize intra-articular structures, and measurement standardization is lacking. 22 Moreover, conventional US imaging is typically performed in the neutral position, which may fail to capture the anterolateral aspect where cam deformities most commonly occur.14,20 Given these constraints, refining the US scanning positions could enhance detection sensitivity and make morphological screening feasible in on-field athletic settings.
The purpose of this study was to investigate US-detected cam-related morphology and prominence in male university soccer players and to examine their associations with groin symptoms and functional impairment. We hypothesized that US would allow feasible screening for cam morphology and that cam-positive players, particularly those with marked prominence, would exhibit a higher prevalence of impingement-related sensations and functional deficits in hip and pelvic control.
Methods
Study Design and Participants
Ethical approval was obtained from the institutional review board of Hokusuikai Kinen Hospital. All screening procedures, including ultrasound examinations, questionnaires, and functional assessments, were conducted on April 10, 2025, during the team's preseason period at the team's training facilities. This study involved a preseason voluntary screening program for male collegiate soccer players who were active and had no hip or groin pain severe enough to limit soccer participation. Participants were recruited by inviting all rostered players from a single university varsity soccer team competing in a top-tier collegiate division in Japan to participate in this cross-sectional observational study. The source population consisted of all registered members of the team, and all eligible players were approached for participation without additional selection procedures. The inclusion criteria were as follows: (1) enrollment in a university soccer club and (2) consent to participate. The exclusion criteria were as follows: (1) history of hip surgery or other conditions affecting hip morphology and (2) current hip or groin pain sufficient to limit participation in soccer activities.
US Examination
US examinations were performed using a SNiBLE2 system (Konica Minolta) equipped with a linear transducer (L11-3; frequency range, 3-11 MHz). All measurements were conducted in the supine position on a bed approximately 55 cm high. Two imaging positions were evaluated: 0° and 15° hip extension (Figures 1 and 2). At 0°, the hip was positioned in neutral rotation, with the toes pointing upward. In the 15° extension position, the examined leg was lowered off the bed with the foot flat on the floor, and the angle was confirmed using a goniometer. Neutral rotation was maintained whenever possible; however, when muscle tension made it difficult to sustain this position, minimal abduction and external rotation were permitted. Care was taken to avoid lumbar hyperextension during the image acquisition.
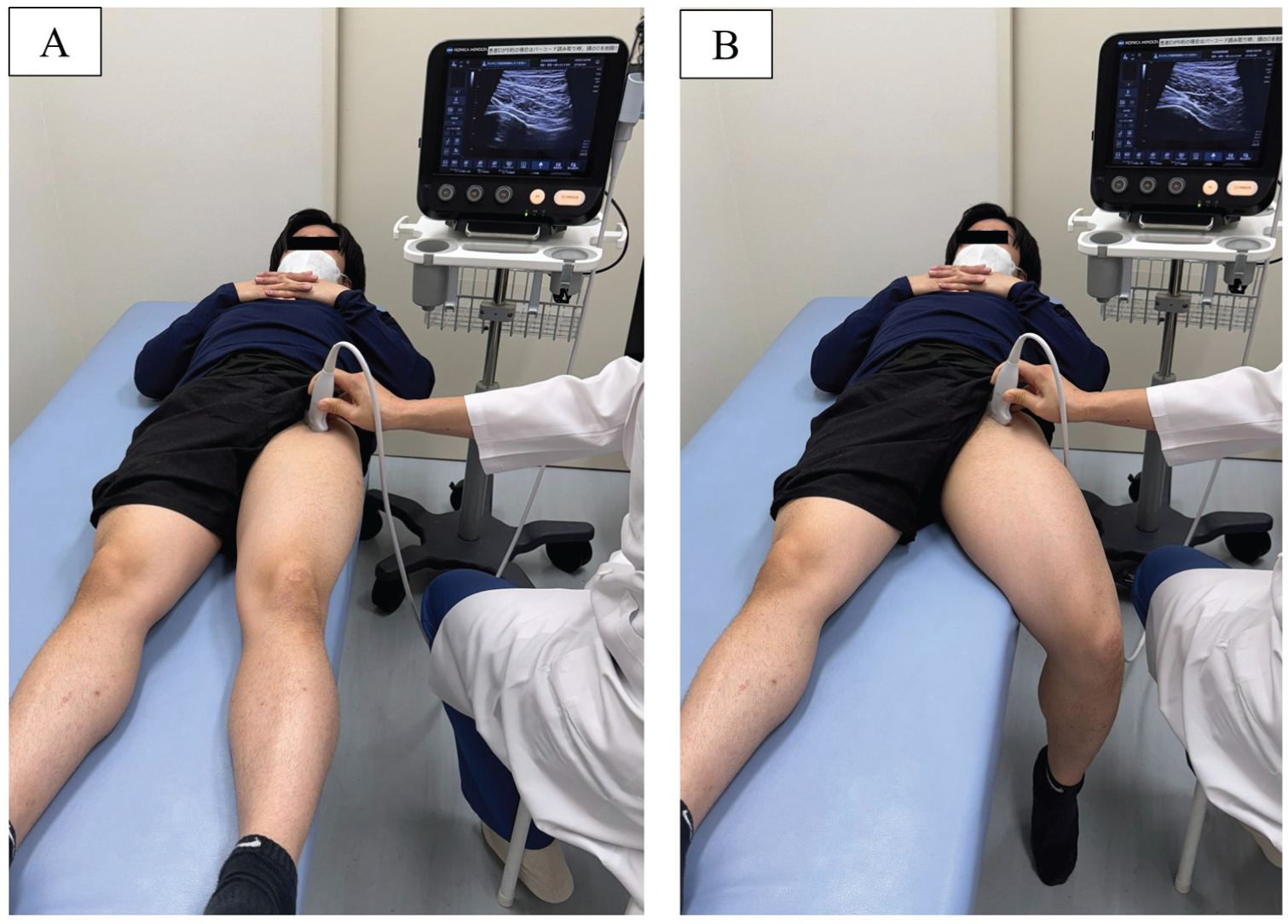
Ultrasound imaging positions at (A) neutral (0°) and (B) 15° of hip extension. Participants were positioned supine on a bed (approximately 55 cm high). In the 0° view, the left hip was in neutral rotation, with the toes pointing upward. For the 15° extension view, the left leg was lowered off the bed with the foot flat on the floor, maintaining neutral rotation when possible; minimal abduction and external rotation were permitted only when necessary to place the foot down. This position allowed anterior exposure of the femoral head-neck junction and enhanced the visualization of the anterolateral contour.
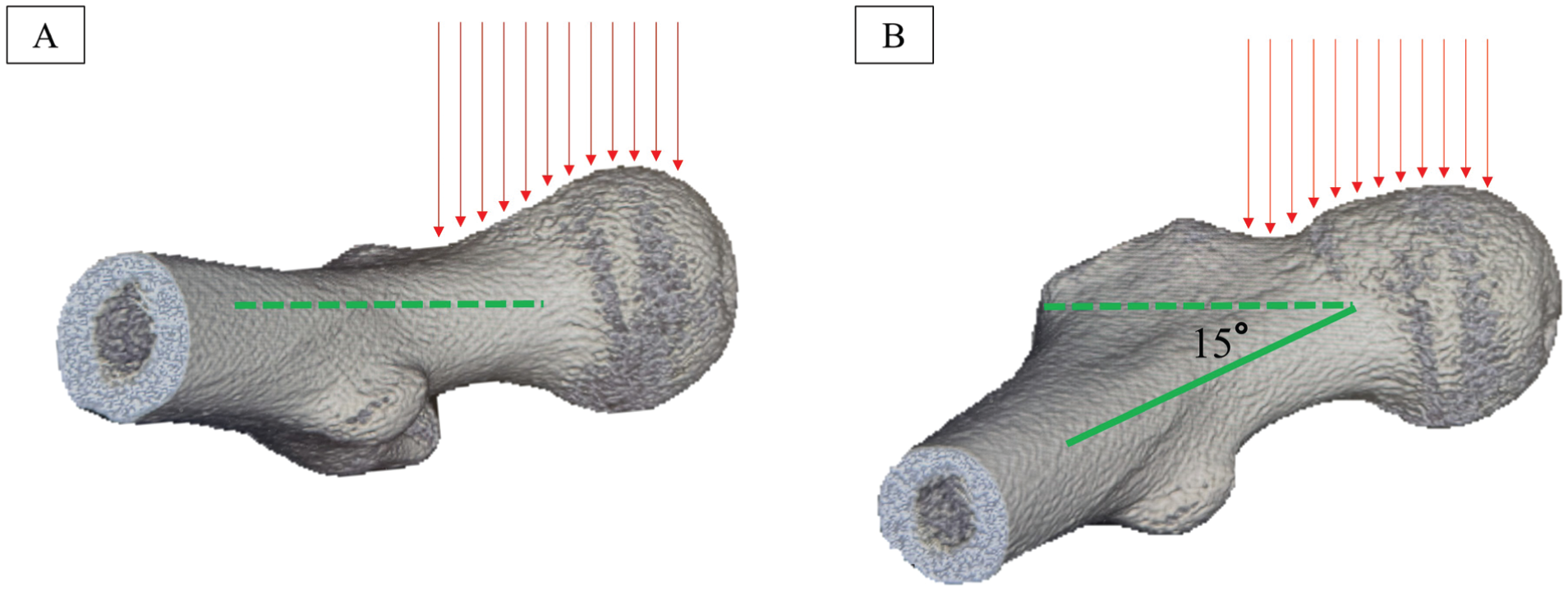
Three-dimensional computed tomography of the proximal femur showing the anterior femoral head-neck junction morphology in the axial view, similar to the ultrasound long-axis scanning plane, at (A) neutral (0°) and (B) 15° of hip extension. The dotted green line indicates the femoral neck axis at neutral 0°, whereas the solid green line indicates the femoral neck axis at 15° of hip extension. Red arrows indicate the direction of ultrasound waves.
Longitudinal images were obtained along the femoral head-neck axis, with 1 image captured at each position on both hips, yielding 4 images per participant. All US scans were performed by 3 sports orthopaedic surgeons (M.S., M.H., and Y.T.), each with >10 years of clinical experience in musculoskeletal US.
The acquired images were anonymized and later reviewed by a hip specialist (M.S.) with >15 years of experience, who was blinded to participant information. Radiographic morphology classifications were adapted for US evaluation and scored semiquantitatively by consensus using a 3-point scoring system (Figure 3).1,5 The anterior head-neck junction was classified as follows:
Normal: symmetric concavity along the anterior femoral head-neck junction on the longitudinal scan
Flattening: reduced or nearly absent concavity of the anterior head-neck junction
Prominence: convex or bulging anterior contour instead of a concavity
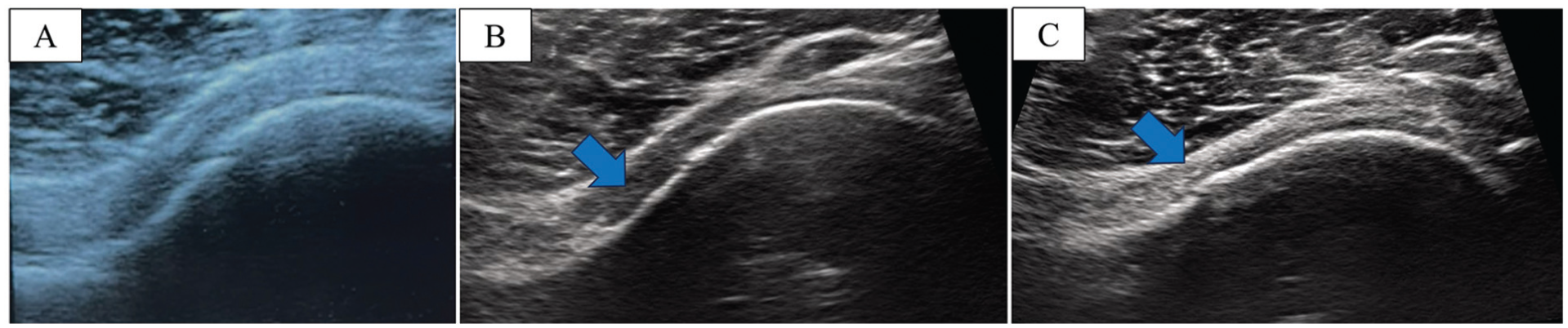
Ultrasound classification of the anterior femoral head-neck junction morphology. Representative longitudinal ultrasound images illustrating (A) normal, (B) flattened, and (C) prominent morphologies. The normal morphology shows a symmetric concavity along the anterior femoral head-neck junction on the longitudinal scan. Flattening shows reduced or nearly absent concavity of the anterior head-neck junction (arrow), whereas prominence demonstrates a convex or bulging anterior contour instead of a concavity (arrow). Flattening and prominence were classified as US-based morphologic abnormalities and grouped as cam-positive findings for the purposes of this study.
Flattening and prominence were classified as US-based morphologic abnormalities at the anterior femoral head-neck junction. For the purposes of this study, these findings were grouped as cam-positive, with prominence indicating a more distinct bony protrusion. A hip was considered cam-positive or prominence-positive if the finding was present in the 0° or 15° extension positions, respectively.
The intra- and interobserver reliability for this 3-grade classification was evaluated by assessing US images from 30 randomly selected hips under blinded conditions. Observer information and player identifiers were concealed during the assessment. Intraobserver reliability was examined 4 weeks after the initial evaluation. The quadratic-weighted Cohen kappa coefficients were 0.80 (95% CI, 0.57-0.94) for intraobserver reliability and 0.75 (95% CI, 0.40-0.97) for interobserver reliability, indicating acceptable reproducibility of the morphological classification.
Symptom Assessment
Symptoms were assessed using a structured questionnaire and standardized physical examination.
All participants completed a questionnaire addressing 4 items (yes/no): (1) current groin pain, (2) current pinching sensation without pain, (3) past groin pain, and (4) past pinching sensation without pain. Groin pain was defined as pain in the groin region during soccer or daily living activities. A pinching sensation was defined as a nonpainful feeling of blockage or discomfort during hip flexion or rotation. In addition to the questionnaire, physical examinations were performed by experienced sports orthopaedic surgeons (M.S., M.H., and Y.T.). The examiners evaluated groin pain and pinching sensations using the flexion, adduction, and internal rotation (FADIR) tests at 90° and 120° of hip flexion (Appendix Figure A1). A hip was classified as having current pain or pinching sensation if it was reported on the questionnaire, elicited during the 90° or 120° FADIR test, or both. Past symptoms were defined based solely on questionnaire responses.
Functional Assessment
Four functional parameters were evaluated: hip abductor weakness, active straight-leg raise (ASLR) deficit, ASLR reverse action, and a positive pelvic mobility (PM) test. All tests were conducted by 3 orthopaedic surgeons (M.S., M.H., and Y.T.), each with >10 years of clinical experience in sports medicine. Before data collection, all examiners attended a training session that used printed reference materials and on-site demonstrations to standardize testing procedures and ensure consistency across examiners.
Hip abductor weakness was assessed using the manual muscle test (MMT) in the side-lying position with the hip in 20° abduction and 10° internal rotation (Appendix Figure A2). The examiner placed one hand on the pelvis to stabilize it, and the other hand on the distal thigh to apply maximal manual resistance. If the participant could not maintain the abducted position against this maximal resistance, the test was graded as MMT 4 and defined as having abductor weakness (+). If the participant was able to maintain the position steadily against maximal resistance without drift, it was graded as MMT 5 and defined as abductor weakness (−). 28
ASLR deficit was evaluated in the supine position with both upper limbs placed alongside the trunk on the bed (Appendix Figure A3A). With the knee extended and hip flexed to 20°, the examiner applied maximal manual resistance. If the participant was unable to maintain the position, the test result was graded as MMT 4 and defined as an ASLR deficit (+). If the participant maintained the position without drift against maximal resistance, it was graded as MMT 5 and defined as ASLR deficit (−).
The ASLR reverse action was assessed by observing compensatory pelvic or trunk movements during the resisted ASLR maneuver (Appendix Figure A3B). The test was defined as a reverse action (+) if pelvic rotation or trunk extension occurred during the maneuver. Absence of compensatory motion was defined as reverse action (−). A positive reverse action indicates inefficient transmission of force from the trunk to the lower limb, in which the trunk moves prematurely ahead of the limb. This finding reflected a disruption in the coordinated motion of the trunk, pelvis, and hip.
The PM test evaluated the posterior pelvic tilt during hip flexion (Appendix Figure A4). The examiner placed the thumb on the anterior superior iliac spine and the index finger on the iliac crest and measured the craniocaudal distance between them. When the participants flexed their hip to 120° and the distance decreased by <50% of the starting position, the test was defined as PM (+) (limited posterior pelvic tilt). If the distance decreased by ≥50%, the test was defined as PM (−) (adequate posterior pelvic tilt). A positive PM test indicates insufficient posterior pelvic tilt at maximal hip flexion, resulting in impaired ability to maintain hip joint centration during flexion and decreased coordination and stability of the lumbopelvic-hip complex.17,23
The hip internal rotation (IR) angle was also assessed. With the participant in the prone position, the hip was maintained at 0° flexion (extension) and the knee was flexed to 90°. The examiner stabilized the pelvis to minimize compensatory motion and measured hip internal rotation using a goniometer. Measurements were taken bilaterally, and both the absolute IR angle on each side and the side-to-side differences were recorded.
Statistical Analysis
Power analysis was conducted using G*Power software (Version 3.1; Heinrich Heine University) for the McNemar test, to compare cam detection between the 0° and 15° hip extension views. Assuming a discordant proportion of 11% (approximately 10% newly positive at 15° and 1% newly negative), which corresponded to an odds ratio (OR) of 10.0, and using a 2-sided α of .05 and a power of 0.80, the required total sample size was 82 paired hips. The final data set included 110 hips, exceeding the required sample size.
All statistical analyses were performed using R software (R Foundation for Statistical Computing). Continuous variables were expressed as the mean ± SD, and categorical variables were presented as counts and percentages. Univariate analyses were conducted to examine differences between hips with and without US-based cam-positive morphology and between those with and without prominence. The normality of continuous variables (height, weight, body mass index [BMI], hip IR angle, and side-to-side IR difference) was assessed using the Shapiro-Wilk test, and comparisons were made using either the Student t test or the Mann-Whitney U test, as appropriate. For categorical variables—including current groin pain, current pinching sensation, past groin pain, past pinching sensation, results of each functional test (abductor weakness, ASLR deficit, ASLR reverse action, and PM test), and the coexistence of ≥2 or ≥3 functional deficits—the chi-square test or Fisher exact test was used, as appropriate.
Multivariate logistic regression analyses were conducted within cam-positive hips to identify the factors associated with current groin pain and pinching sensation. Candidate predictors included 4 functional parameters (hip abductor weakness, ASLR deficit, ASLR reverse action, and positive PM test), the coexistence of ≥2 or ≥3 functional deficits, hip internal rotation angle, and side-to-side difference in internal rotation. Variables showing a univariate association with the outcome at P < .05 were entered into the multivariable model, with age and BMI included a priori, regardless of significance. The results were expressed as ORs with 95% CI. Model assumptions were evaluated by assessing multicollinearity using the variance inflation factor, linearity of the logit for continuous predictors, goodness of fit using the Hosmer-Lemeshow test, and discrimination using the area under the receiver operating characteristic curve (AUC).
A similar 2-step approach was applied to identify factors associated with current groin pain and pinching sensation. The same candidate predictors were used, and variables meeting the univariate threshold of P < .05 were entered into the multivariable logistic regression model, with age and BMI incorporated into the model again. ORs with 95% CIs, and indices of model fit and discrimination were reported similarly.
A P value < .05 was considered statistically significant for all tests.
There were no missing data for any of the variables included in the analyses; therefore, no imputation procedures were required.
Results
All 55 rostered players participated in the screening session, and no players met the exclusion criteria; therefore, all 55 players (110 hips; mean age, 19.5 ± 1.1 years) were included in the final analysis. Participant characteristics, including height, weight, and BMI, are summarized in Table 1. US-based cam-positive morphology was identified in 97 of the 110 hips (88%), whereas prominence was observed in 53 hips (48%) (Table 1). The detection rate of US-based cam-positive morphology increased from 79% at 0° to 88% with the addition of a 15° extension view (P = .02). Similarly, the detection rate of prominence increased from 25% at 0° to 48% when a 15° extension view was used (P < .0001).
Participant Characteristics and Frequency of Ultrasound-Based Cam-Positive Morphology and Prominence in 110 Hips of 55 Male Collegiate Soccer Players a
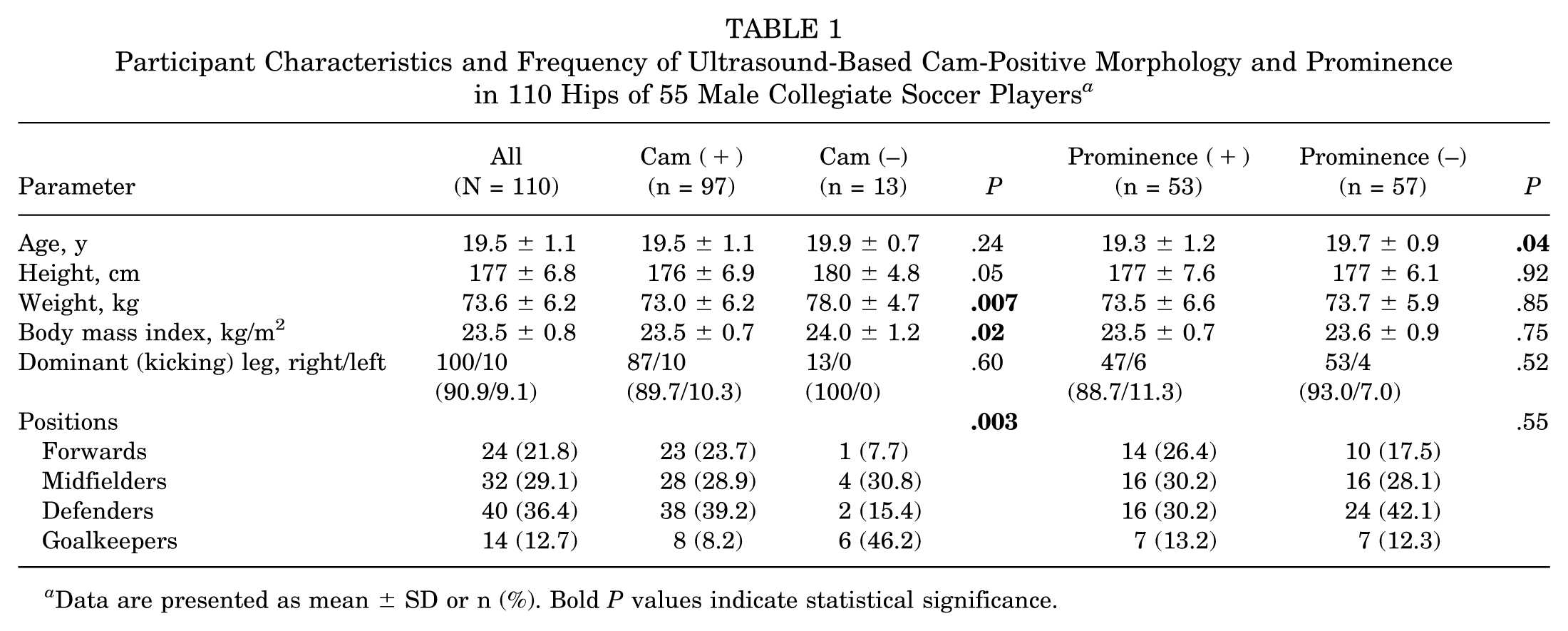
Data are presented as mean ± SD or n (%). Bold P values indicate statistical significance.
Comparisons of symptoms and functional findings between hips with and without cam morphology or prominence are summarized in Table 2. Groin pain was not significantly different between the groups, whereas the prevalence of a pinching sensation was significantly higher in hips with cam morphology and prominence (P = .006 and P = .002, respectively).
Comparison of Groin Symptoms and Functional Findings Between Hips With and Without Ultrasound-Based Cam-Positive Morphology and Prominence a
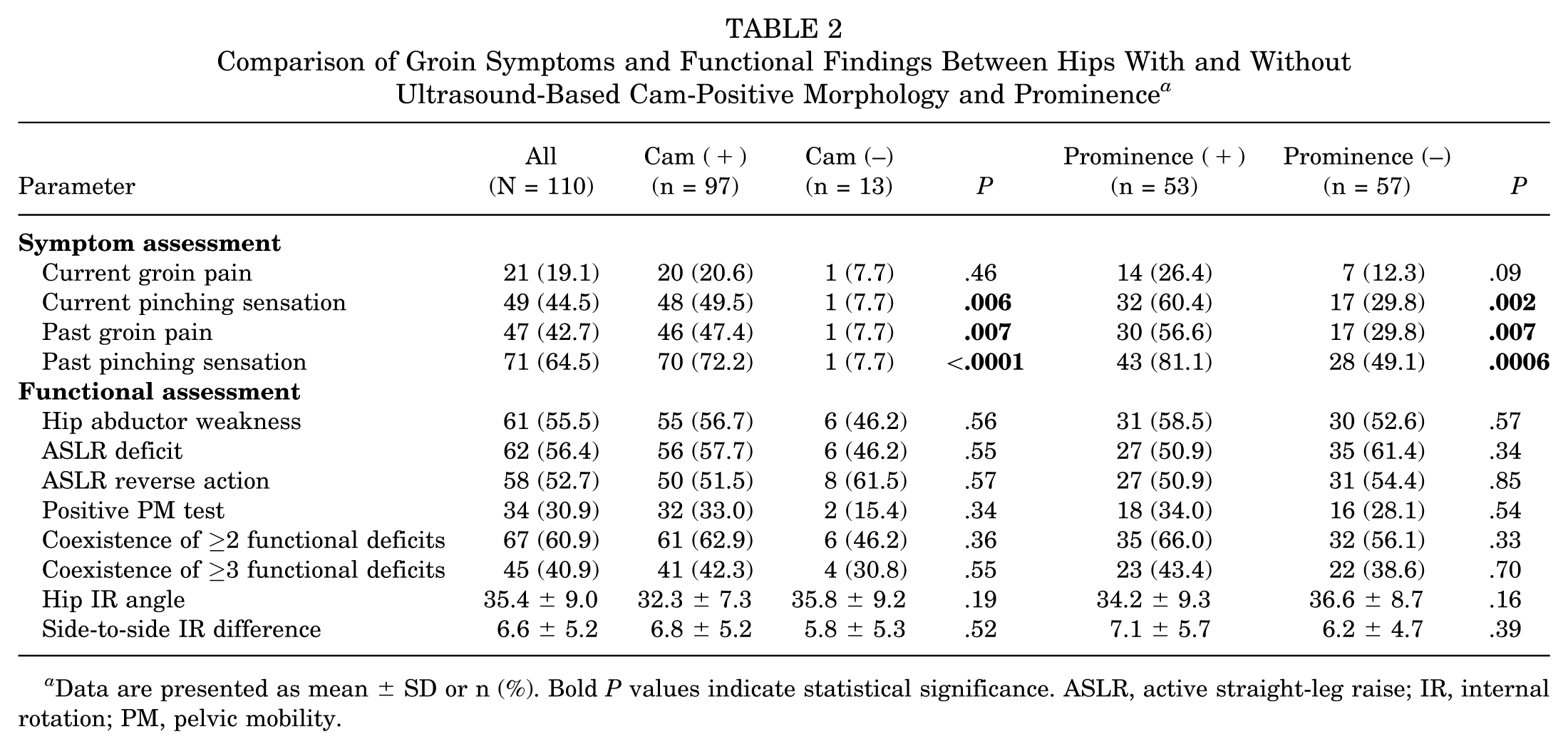
Data are presented as mean ± SD or n (%). Bold P values indicate statistical significance. ASLR, active straight-leg raise; IR, internal rotation; PM, pelvic mobility.
Among the 97 cam-positive hips, the coexistence of multiple functional deficits and greater side-to-side internal rotation differences was associated with symptoms (Table 3). In the multivariate analysis adjusted for age and BMI, ≥3 functional deficits (OR, 5.0) and side-to-side internal rotation difference (OR, 1.2) were independent predictors of groin pain, and the same 2 factors (OR, 10.2 and 1.1, respectively) were also associated with current pinching sensation (Table 4).
Univariate Analyses for Factors Associated With Current Groin Pain and Pinching Sensation in Cam-Positive Hips (n = 97) a
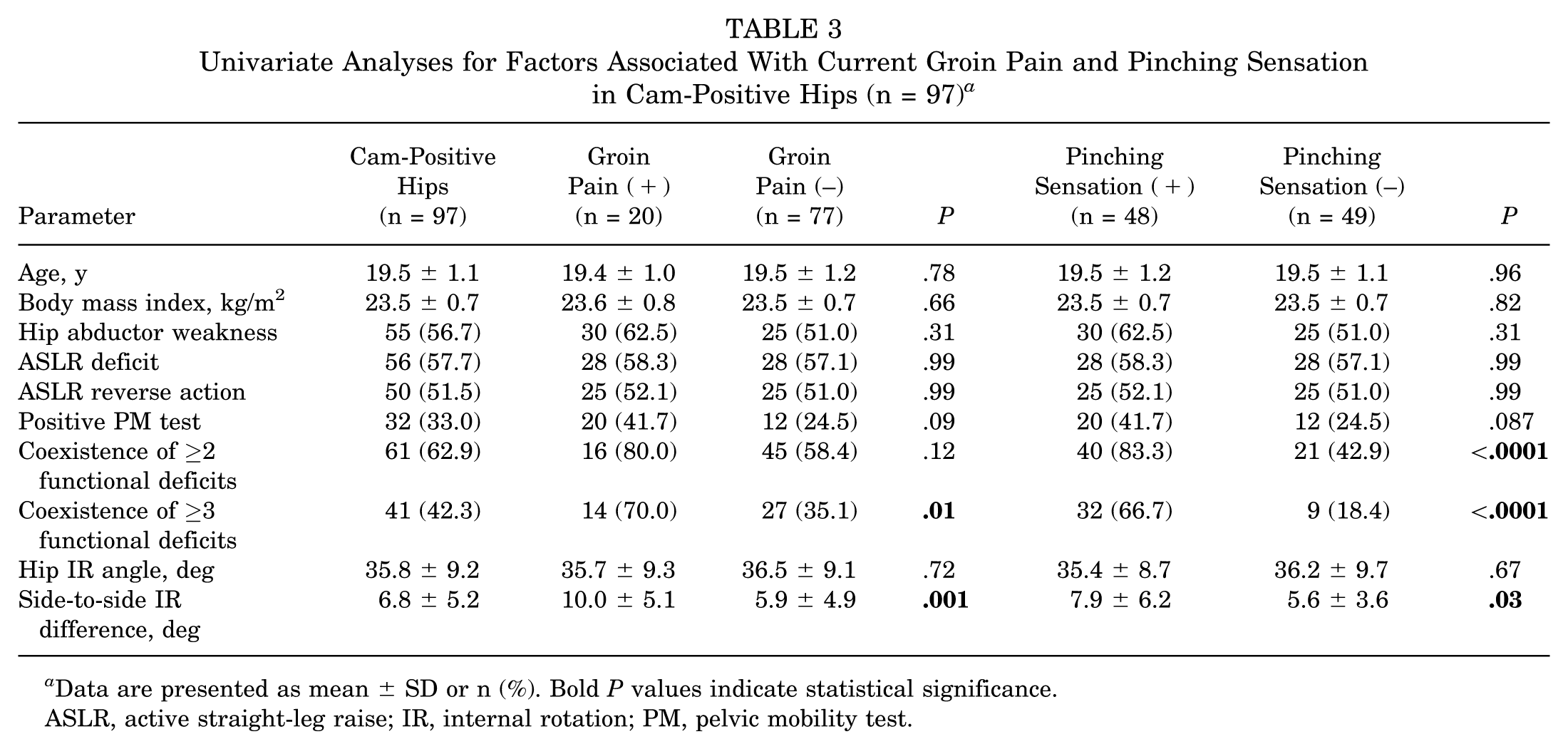
Data are presented as mean ± SD or n (%). Bold P values indicate statistical significance.
ASLR, active straight-leg raise; IR, internal rotation; PM, pelvic mobility test.
Multivariable Logistic Regression Analyses for Current Groin Pain and Pinching Sensation in Cam-Positive Hips (n = 97) a
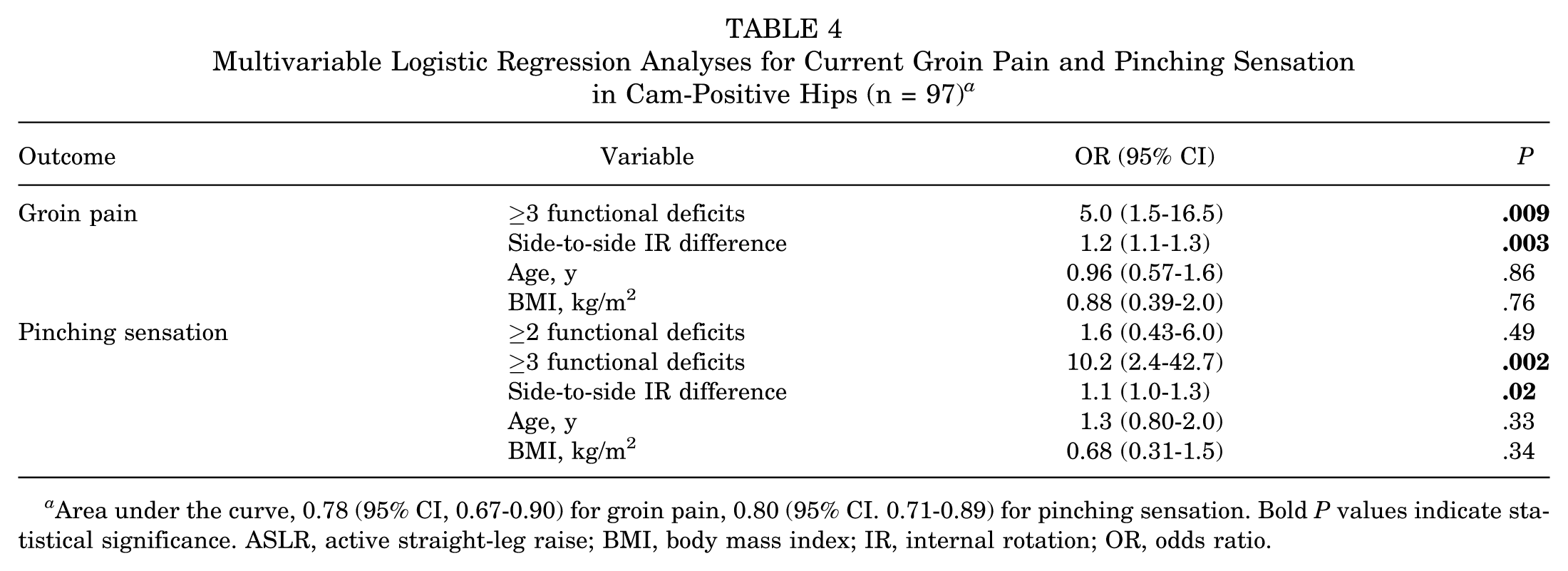
Area under the curve, 0.78 (95% CI, 0.67-0.90) for groin pain, 0.80 (95% CI. 0.71-0.89) for pinching sensation. Bold P values indicate statistical significance. ASLR, active straight-leg raise; BMI, body mass index; IR, internal rotation; OR, odds ratio.
Similarly, in the 53 prominence-positive hips, both ≥2 and ≥3 functional deficits were related to groin pain and pinching sensation in the univariate analysis (Table 5); however, only ≥3 functional deficits (OR, 6.5 and 6.9, respectively) remained significant in the adjusted model (Table 6).
Univariate Analyses for Factors Associated With Groin Pain and Pinching Sensation in Prominence-Positive Hips (n = 53) a
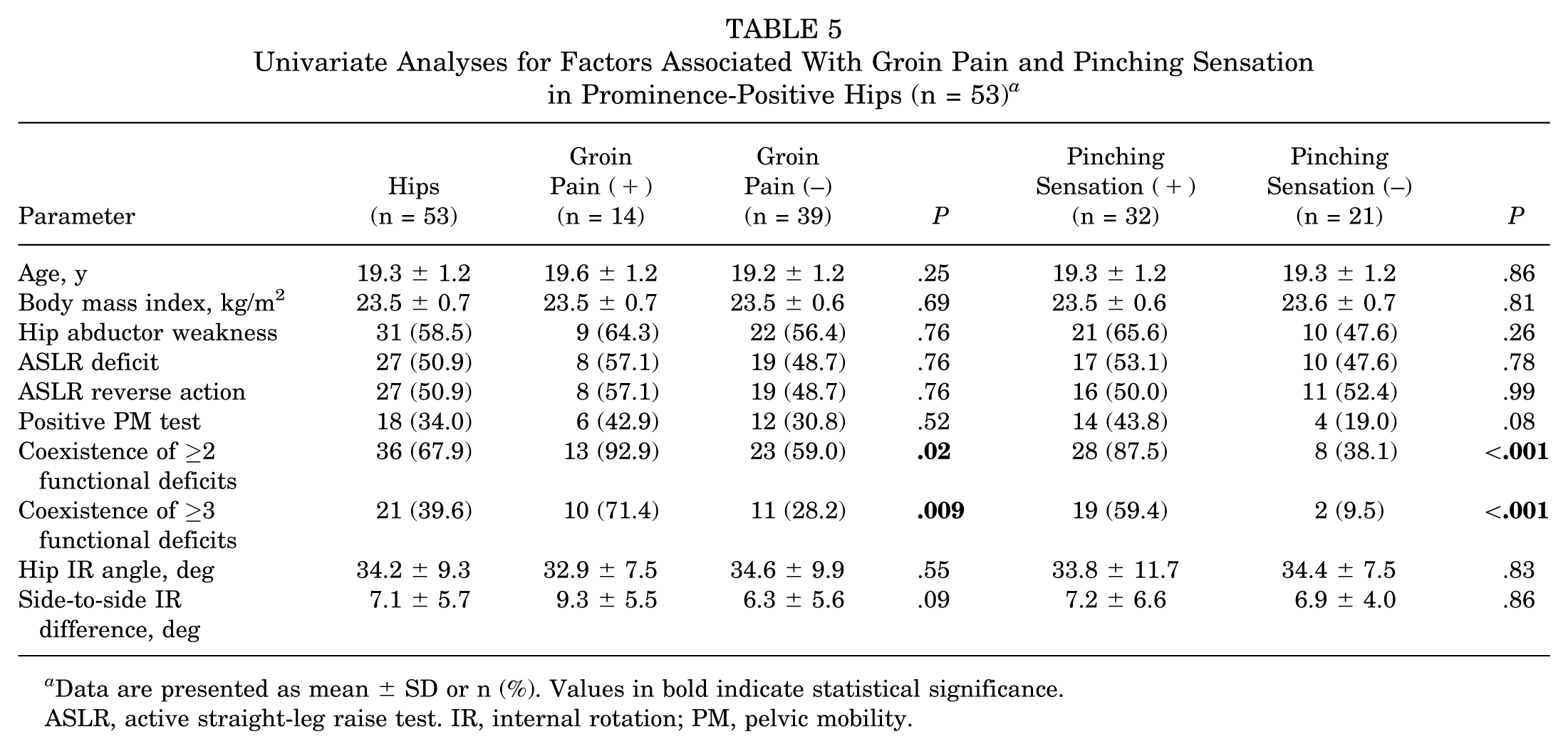
Data are presented as mean ± SD or n (%). Values in bold indicate statistical significance.
ASLR, active straight-leg raise test. IR, internal rotation; PM, pelvic mobility.
Multivariable Logistic Regression Analyses for Current Groin Pain and Pinching Sensation in Prominence-Positive Hips (n = 53) a
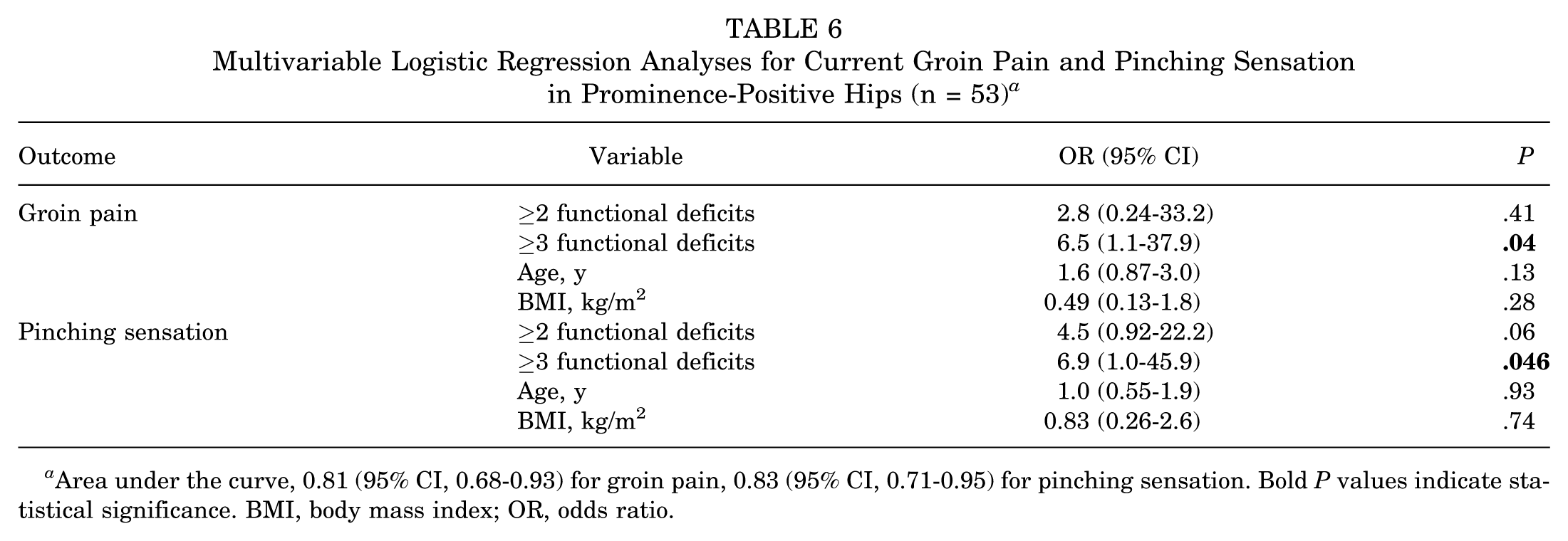
Area under the curve, 0.81 (95% CI, 0.68-0.93) for groin pain, 0.83 (95% CI, 0.71-0.95) for pinching sensation. Bold P values indicate statistical significance. BMI, body mass index; OR, odds ratio.
All logistic regression models met the statistical assumptions, and the Hosmer-Lemeshow test indicated an adequate fit (P > .05). AUC values for groin pain and pinching sensation were 0.78 and 0.80, respectively, in cam-positive hips, and 0.81 and 0.83, respectively, in prominence-positive hips.
Discussion
This study showed that US-detected cam-related morphology was frequently present in this cohort of male collegiate soccer players. The addition of a 15° hip extension view improved the detection of anterolateral cam-related morphology compared with the neutral 0° position and significantly increased the observed prevalence of prominent morphology. Although cam-positive morphology was not significantly associated with groin pain, it was significantly related to impingement sensation. Furthermore, the coexistence of multiple functional impairments was associated with a higher likelihood of groin pain and impingement sensation, similar to that observed in hips with prominent morphology.
A plausible explanation for why the additional 15° extension view improved detection in this cohort can be drawn from previous imaging studies. Previous MRI research has shown that oblique axial images aligned with the femoral neck axis primarily depict the anterior 3-o’clock region, which can result in underestimation of cam deformities compared with radial MRI sequences that capture the anterosuperior 1:30 region where cam morphology develops most commonly.9,19 Radial MRI studies and systematic reviews consistently demonstrate that maximal deformities localize to this 1:30 region.9,12 Because longitudinal US scanning parallel to the femoral neck axis conceptually resembles the oblique axial MRI plane, anterosuperior cam lesions may not be sufficiently detected when evaluating cam morphology solely with this long-axis view. This may be partly because some anterolateral deformities are located in a relatively covered portion of the femoral head-neck junction in the neutral position, where US visualization may be limited by acoustic shadowing from the acetabular rim. To explore this positional limitation, we reproduced the US scanning plane on 3-dimensional computed tomography (3D-CT) axial images, as illustrated in Figure 2, and compared the morphology between 0° and 15° of hip extension. The 15° extension position made the anterolateral bump more conspicuous on 3D-CT, suggesting that a similar improvement in visualization may occur during US evaluation. Consistent with this interpretation, adding the 15° extension view increased the detection rates of cam morphology and prominence to levels comparable with radiographic studies of similar athletic populations. 25 These findings collectively support the notion that incorporating a modest degree of hip extension can enhance the visualization of anterolateral cam deformities that may be overlooked in the neutral position.
In this study, goalkeepers showed a lower prevalence of cam morphology than the field players (Table 1). This finding may be related to the differences in hip loading patterns and movement demands associated with the playing position. Cam morphology typically develops during late adolescence when the proximal femoral physis remains open, and its formation is promoted by repetitive and high-magnitude hip motion and loading. 18 Unlike field players, goalkeepers experience less cumulative hip motion and impact exposure during training and match-play, which may partly explain the lower prevalence observed in this group. In addition, body weight and BMI were significantly higher in the cam-negative group, which could partly reflect the inclusion of goalkeepers who generally have larger body sizes than field players.
As shown in Table 2, the prevalence of current groin pain did not differ between hips with and without cam-positive morphology, whereas a pinching sensation was more frequently reported in cam-positive and prominence-positive hips. Notably, approximately 80% of the players with cam-positive morphology reported no groin pain, indicating that the majority of cam-positive athletes remained free of current groin pain even when pain was actively assessed during screening. The rate of symptomatic cases likely overestimated the proportion of athletes who voluntarily sought clinical evaluation for hip pain, as the present study was conducted in a medical screening setting where examiners performed the FADIR test to elicit impingement-related discomfort. These findings support the notion that cam-related morphology may represent a common, largely physiological adaptation among soccer players and that only a subset of individuals experience pain or functional limitations associated with it.10,11 In addition, players with a cam or prominent morphology reported a history of groin pain and pinching sensation more frequently, suggesting that transient symptoms may have occurred earlier, even if no current pain was present. The higher prevalence of a pinching sensation in cam-positive hips may represent an early mechanical manifestation of FAI preceding the development of persistent groin pain.
Tables 3 to 6 analyzed only cam- or prominence-positive hips; therefore, the models identified factors that differentiate athletes with current symptoms from those without symptoms after the deformity had developed. In both analyses, the coexistence of multiple dysfunctional patterns consistently predicted groin pain and pinching sensation, whereas asymmetry in hip internal rotation showed an association only in cam-positive hips. These findings indicate that after cam-type deformities develop, symptom onset depends less on the morphology itself and more on the presence of dysfunctional movement and limited joint mobility. However, the potential contribution of minor rotational asymmetry should be interpreted cautiously because the mean side-to-side difference was <5°, suggesting limited clinical relevance. Such dysfunctions often precede pain and represent a subclinical state described in the Selective Functional Movement Assessment as “dysfunctional and nonpainful”—a movement pattern that lacks pain but exhibits poor control or restriction. 8 Cook et al emphasized that identifying and correcting dysfunctional and nonpainful patterns before pain emerges is a cornerstone of preventive screening.6,7 A meta-analytic study has further supported this preventive rationale, demonstrating that low functional movement scores are associated with an elevated risk of future musculoskeletal injury. 4 In this context, the current results suggest that in elite athletes, where cam-related morphology is frequently observed, the detection and correction of dysfunctional and nonpainful patterns may be crucial to prevent the transition from dysfunction to pain. Therefore, functional assessment focusing on movement quality should be considered a core component of secondary prevention strategies for FAI.
Limitations
This study has some limitations. First, because of its cross-sectional design, causal relationships between morphological features, functional impairments, and symptom onset could not be established. Second, although a greater side-to-side difference in hip internal rotation was significantly associated with symptoms in cam-positive hips, the mean difference was <5°, which may not represent a clinically meaningful limitation in mobility. Third, in the present US-based classification, hips with a flattened contour at the femoral head-neck junction were grouped as cam-positive for analytic purposes. However, because an alpha angle was not measured, some of these cases may not represent true cam morphology. In addition, the present study did not determine which clock-face sector was actually represented by the ultrasound long-axis view in the 15° extension position. Although previous MRI literature suggests that extension may shift the visualized region toward the anterosuperior region, this positional effect has not been validated, and future imaging studies integrating US with 3D-CT or radial MRI are needed to clarify the precise correspondence between joint position and clock-face orientation. Finally, all participants were elite male soccer players; therefore, the findings may not be generalizable to female athletes, athletes in other sports, or recreational populations.
Conclusion
Adding a 15° hip extension view improved the US detection of anterolateral cam-related morphology, which may be underdiagnosed in the neutral position. In this cohort, current symptoms were more strongly associated with coexisting functional impairments than with morphology alone.
Footnotes
Appendix
Final revision submitted March 14, 2026; accepted April 7, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.T. reports a relationship with Zimmer Biomet Japan that includes consulting or advisory and speaking and lecture fees.
Ethical approval for this study was obtained from Hokusuikai Kinen Hospital (approval No. 115).