
Abstract
Background:
Recurrent anterior shoulder instability is a common problem in athletes, especially those in contact, collision, or overhead sports. Anterior shoulder instability remains the predominant injury pattern in athletes, accounting for the majority of subluxations and dislocations. Return-to-sport (RTS) outcomes vary across techniques, and the relative effectiveness of these procedures in athletes has not been well established.
Purpose/Hypothesis:
Our study aimed to compare rates of RTS after anterior shoulder stabilization surgery. It was hypothesized that the Bristow-Latarjet procedure would have the highest RTS.
Study Design:
Systematic review; level of evidence, 3.
Methods:
A systematic review and meta-analysis of randomized controlled trials and cohort studies were performed according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Studies on surgical stabilization of anterior shoulder instability in athletes that reported return to sport were included. Nineteen studies met the inclusion criteria, comprising 1,850 patients with an average age of 22.8 (13-46). Pooled proportions for RTS were calculated. Subgroup analysis was performed based on the surgical procedure.
Results:
Full RTS across all patients was 79% (95% CI, 0.70-0.87). Full cessation of sport was 10% (95% CI, 0.04-0.16). Although indications for procedures varied, the Bristow-Latarjet stabilization demonstrated a significantly higher full RTS rate compared with Bankart (0.92; 95% CI, 0.83-0.98, versus 0.71; 95% CI, 0.56-0.83; respectively, P = .002).
Conclusion:
Athletes undergoing surgical stabilization for anterior shoulder instability achieved high rates of RTS. The Bristow-Latarjet procedure was associated with significantly higher rates of full RTS than Bankart repairs in anterior shoulder instability, despite variability in patient indications across procedures.
Shoulder injuries are common among athletes due to the glenohumeral joint structural anatomy and high demands of sport.13,27 The prevalence of shoulder injuries in athletes ranges from 28% to 50%, with overhead and throwing sports having the highest incidence.7,14,28,43 Glenohumeral instability (dislocation or subluxation) accounts for up to 23% of all shoulder injuries.29,38 The management of glenohumeral instability is multifactorial, but many ultimately require surgery to restore stabilization and prevent recurrent symptoms that impede athletic performance. 46 Anterior instability represents the predominant pattern of glenohumeral instability in athletes, particularly in young and contact populations, with substantially higher incidence rates compared with other forms of instability. 12
Common surgical procedures for anterior shoulder instability include the Bristow-Latarjet procedure and Bankart repair, which may be performed using open, arthroscopic, or combined techniques. The Bristow-Latarjet, first reported in 1958, involves the transfer of the coracoid process to stabilize the glenohumeral joint with an associated bony defect. 32 The Bankart technique, originally pioneered by Arthur Sidney Blundell Bankart in 1923, is performed for anterior shoulder instability. 41 The goal is to mobilize, tension, and refix the torn anteroinferior glenoid labrum, with current techniques using suture anchors. Over the past decades, this technique has evolved primarily into an arthroscopic technique and can be performed with or without an infraspinatus remplissage. 8
These stabilization procedures require substantial recovery but are associated with high patient satisfaction and generally favorable postoperative outcomes.11,25 Return to sport (RTS) remains a central measure of success in athletic populations, with overall RTS rates ranging from 50% to 100% and return to preinjury level of play ranging10,37,47,50 from 20% to 100%. Multiple factors may contribute to variability in results, including the amount of glenoid bone loss, sport, level of play, and rehabilitation. 34
RTS outcomes vary widely among athletes undergoing shoulder stabilization, and given the range of available surgical techniques, understanding RTS is critical for informed surgical decision-making and patient counseling. This study aimed to compare RTS rates after shoulder stabilization surgery in an athletic population and to analyze differences between the Bristow-Latarjet and Bankart techniques.
Methods
Search Strategy
A systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist, including studies published from January 2005 to June 2025. This review was registered in the Prospective Register of Systematic Reviews (PROSPERO) (CRD420251089641). The PICO (Population, Intervention, Comparison, Outcome) strategy was used to develop a targeted search. This review will mainly address the following research question: “What are the RTS outcomes of various stabilization surgeries when performed on adolescent and young adult athletes?” The target population comprised adolescent and young adult athletes. The intervention being studied was surgical stabilization procedures of the glenohumeral joint. The comparison studied was between various surgical stabilization procedures, including Bristow-Latarjet, Bankart, and mixed procedure arthroscopies. The primary outcome analyzed was RTS (no return, partial return, or full return).
Eligibility Criteria
The inclusion criteria were as follows: clinical studies involving human participants (including randomized controlled and nonrandomized trials); studies that included athletes as their target population (regardless of what sport); studies that had a mean population age of <30-years; studies that report on surgical stabilization procedures of the glenohumeral joint; studies that report on shoulder instability procedures; studies that include data on surgical outcomes, with a minimum reporting on RTS time; studies that report on preoperation shoulder metrics; studies in English; studies with levels of evidence 1 to 3. The exclusion criteria were as follows: studies that included multidirectional instability, posterior instability, or revision surgeries; reviews; case reports; technical reports; conference abstracts; letters; and editorials.
Study Selection Process
Three independent authors (T.H., A.B., and E.M.) performed the literature search. In June 2025, Scopus and PubMed databases were accessed. Details of the Scopus and PubMed literature searches, including keywords, inclusion and exclusion criteria, Boolean operators, and filters, are provided in Supplementary Appendix 1. The authors (T.H., A.B., and E.M.) independently screened titles and abstracts to identify potentially eligible articles. The full-text articles of interest were reviewed based on inclusion and exclusion criteria. Disagreements over which studies to include were resolved collectively by the authors. Studies performed by the same institution and authors with overlapping enrollment periods were assessed for potential overlap by comparing enrollment date, inclusion criteria, procedure types, and study characteristics. Each reviewer used the open-source citation management tool, Zotero, to organize the articles during the screening process. Data extraction records were organized in Microsoft Excel spreadsheets, with access restricted to the review team only. Nineteen studies met the inclusion criteria and were included in the final analysis. The study selection process is illustrated in a PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 2020 flow diagram (Figure 1).
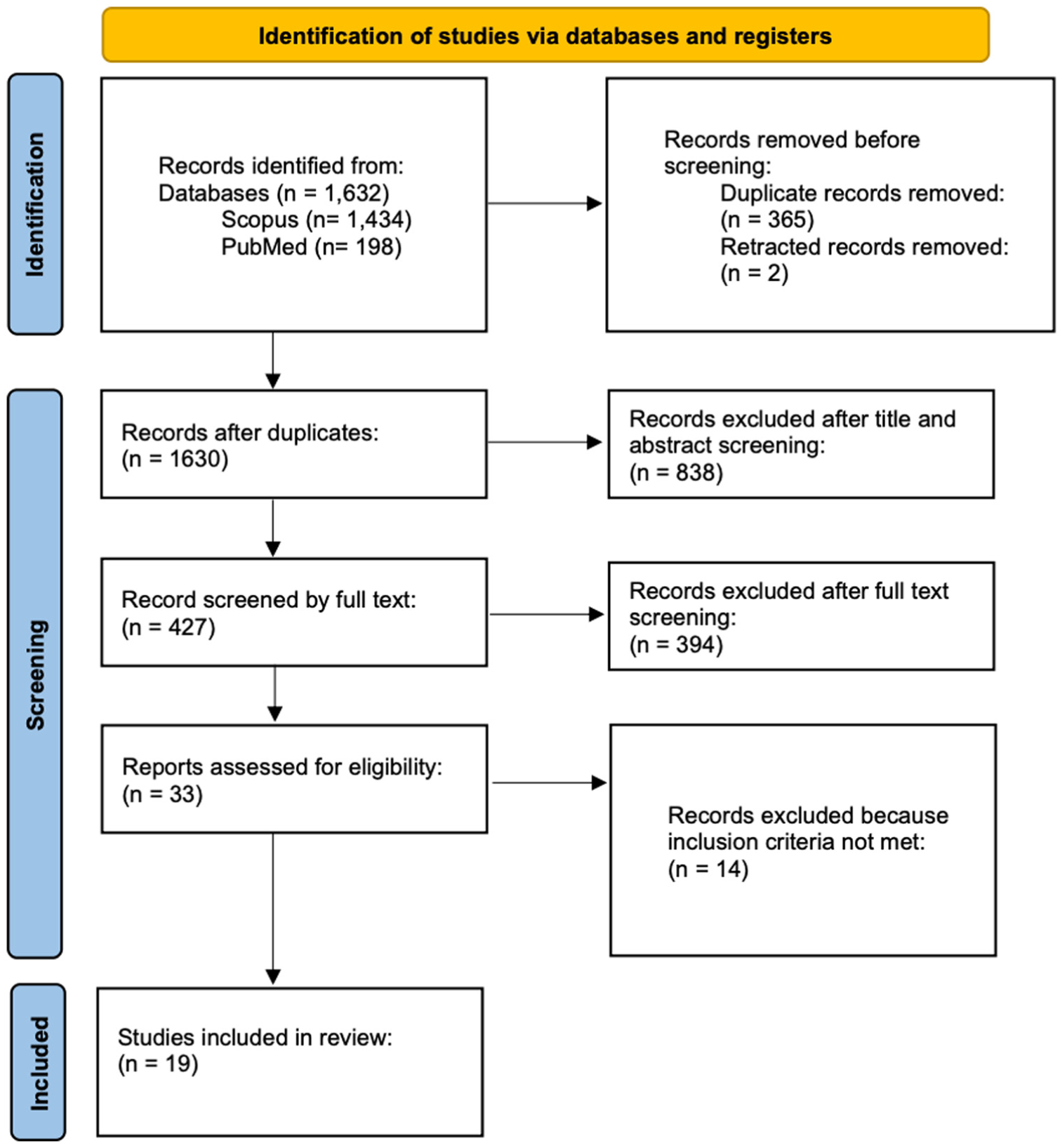
PRISMA 2020 flow diagram detailing the identification, screening, eligibility, and inclusion of studies. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Data Extraction
Data extraction was independently performed by 3 reviewers using a standardized method and included: study characteristics (author, year, study design); surgery performed; population information (size of cohort, mean age, age range, months after surgery for the final follow-up appointment); RTS data (no return, partial return, full return); re-operation events. When multiple RTS definitions were reported, return to preinjury or presymptom level was preferentially extracted.
Risk of Bias
Because all included studies were observational, risk of bias was assessed using the Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I) tool. Each study was evaluated across 7 domains: confounding; participant selection; classification of interventions; deviations from intended interventions; missing data; measurement of outcomes; and selective reporting. Two reviewers independently assigned risk-of-bias ratings of low, moderate, serious, or critical, with disagreements resolved by consensus or third-party arbitration. Visual summaries of risk-of-bias assessments were generated using the ROBVIS tool to provide a transparent representation of domain-level and overall study quality (Figure 2).
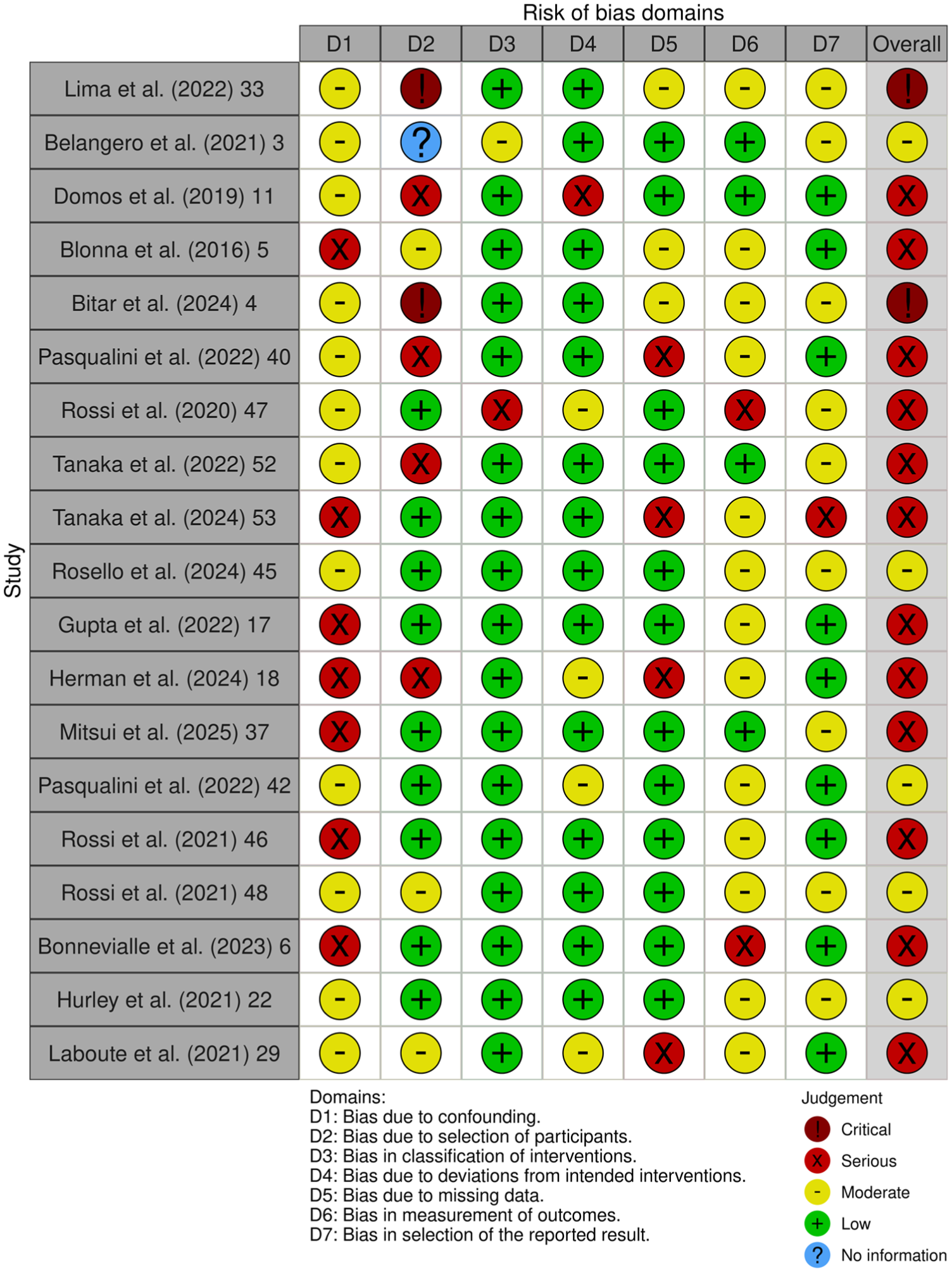
Risk of bias assessment of included nonrandomized studies using the ROBINS-I tool across 7 bias domains, with an overall risk-of-bias judgment for each study. ROBINS-I, Risk Of Bias In Non-randomized Studies of Interventions.
Statistical Analysis
All analyses were performed in R (R Foundation for Statistical Computing) using the meta and metafor packages. Pooled RTS proportions were calculated with random-effects models to account for expected heterogeneity across study populations and surgical techniques. Proportions were synthesized using appropriate variance-stabilizing transformations and presented with 95% CIs. Subgroup analyses compared RTS outcomes among Bristow-Latarjet and Bankart procedures. Heterogeneity was assessed using the I2 statistic and interpreted according to standard thresholds.
Results
Across all included studies, 1850 athletes were analyzed. The cohort included 653 patients undergoing the Bristow-Latarjet procedure and 921 undergoing Bankart repair (Table 1). The mean age of included patients was 22.8 years (range, 13-46 years), with Bristow-Latarjet and Bankart cohorts demonstrating similar mean ages (22.8 and 23.5 years) (standardized mean difference, 0.16). The mean follow-up duration across all studies was 48.7 months (Table 2).
Included Patient Characteristics a
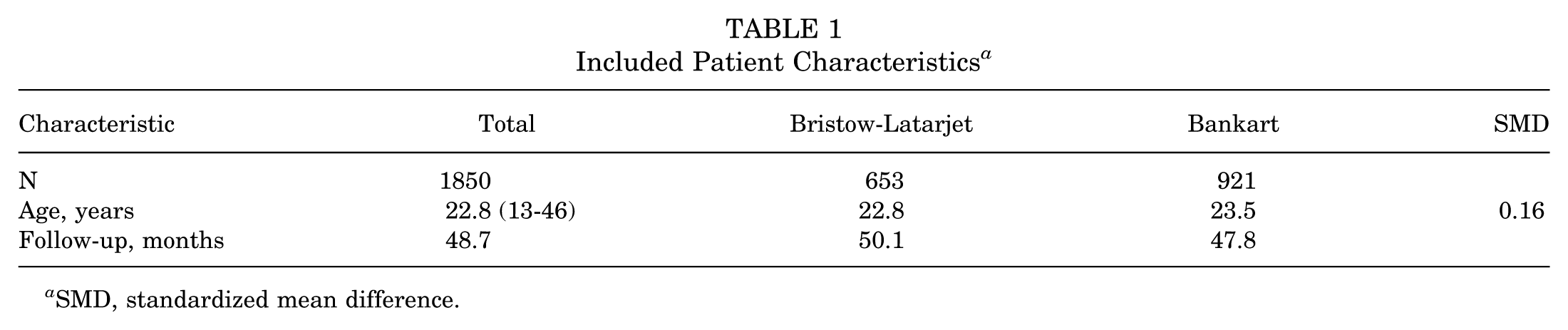
SMD, standardized mean difference.
Included Studies a
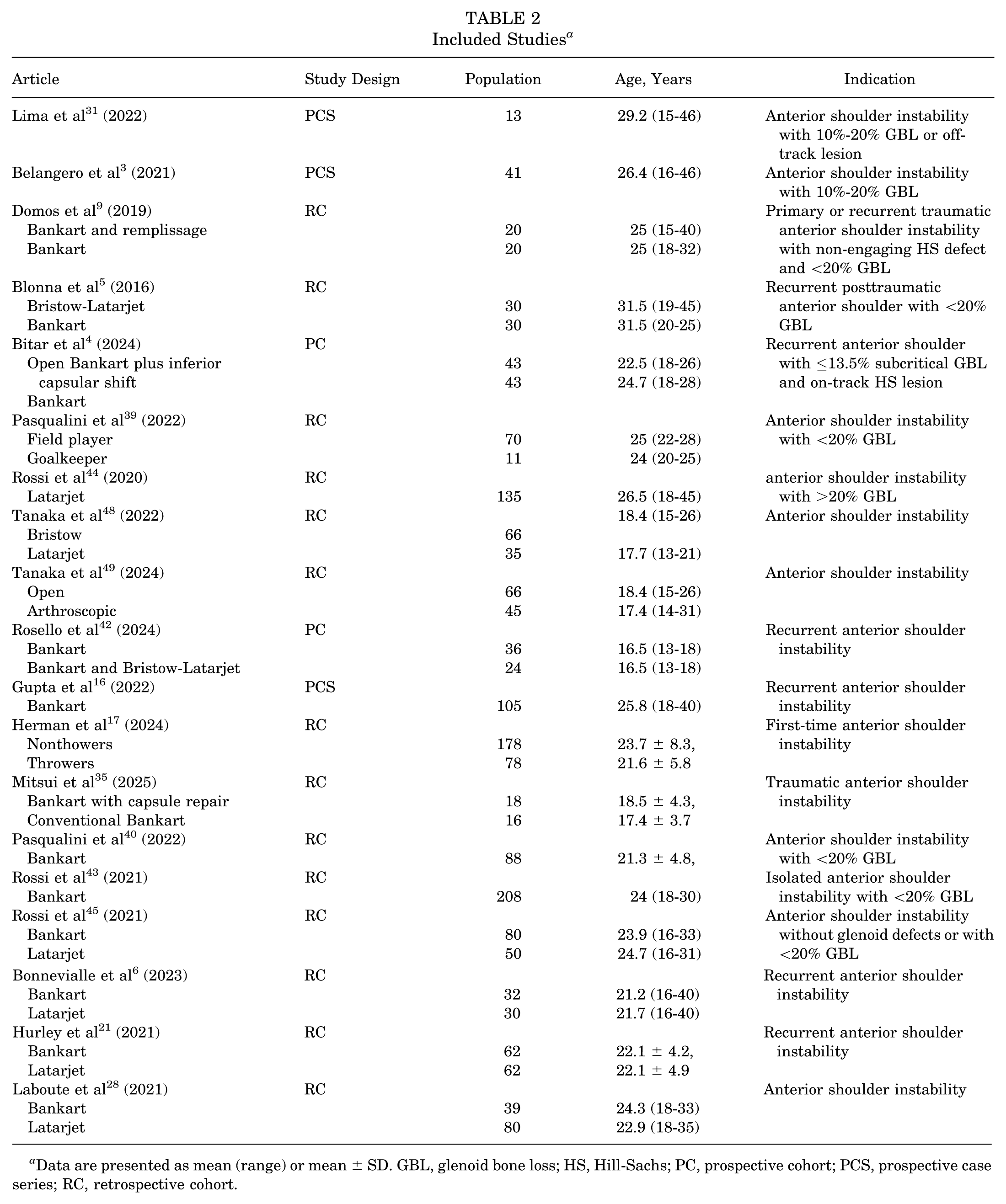
Data are presented as mean (range) or mean ± SD. GBL, glenoid bone loss; HS, Hill-Sachs; PC, prospective cohort; PCS, prospective case series; RC, retrospective cohort.
Across included anterior instability studies, indications for the Bristow-Latarjet procedure included recurrent anterior shoulder instability with varying degrees of glenoid bone loss. Bankart repair was performed for similar indications, most commonly anterior shoulder instability with absent or subcritical glenoid bone loss (generally <20%) and on-track Hill-Sachs lesions. Overall, indications were comparable across procedures and corresponded primarily to the direction of instability and the presence or magnitude of glenoid bone loss.
Full RTS was achieved by 79% of athletes overall (95% CI, 0.70-0.87) (Figure 3). Athletes who underwent Bristow-Latarjet stabilization had the highest rates of full RTS (0.92; 95% CI, 0.83-0.98), which was significantly greater than those treated with Bankart repair (0.71; 95% CI, 0.56-0.83; P = .002) (Figure 4).
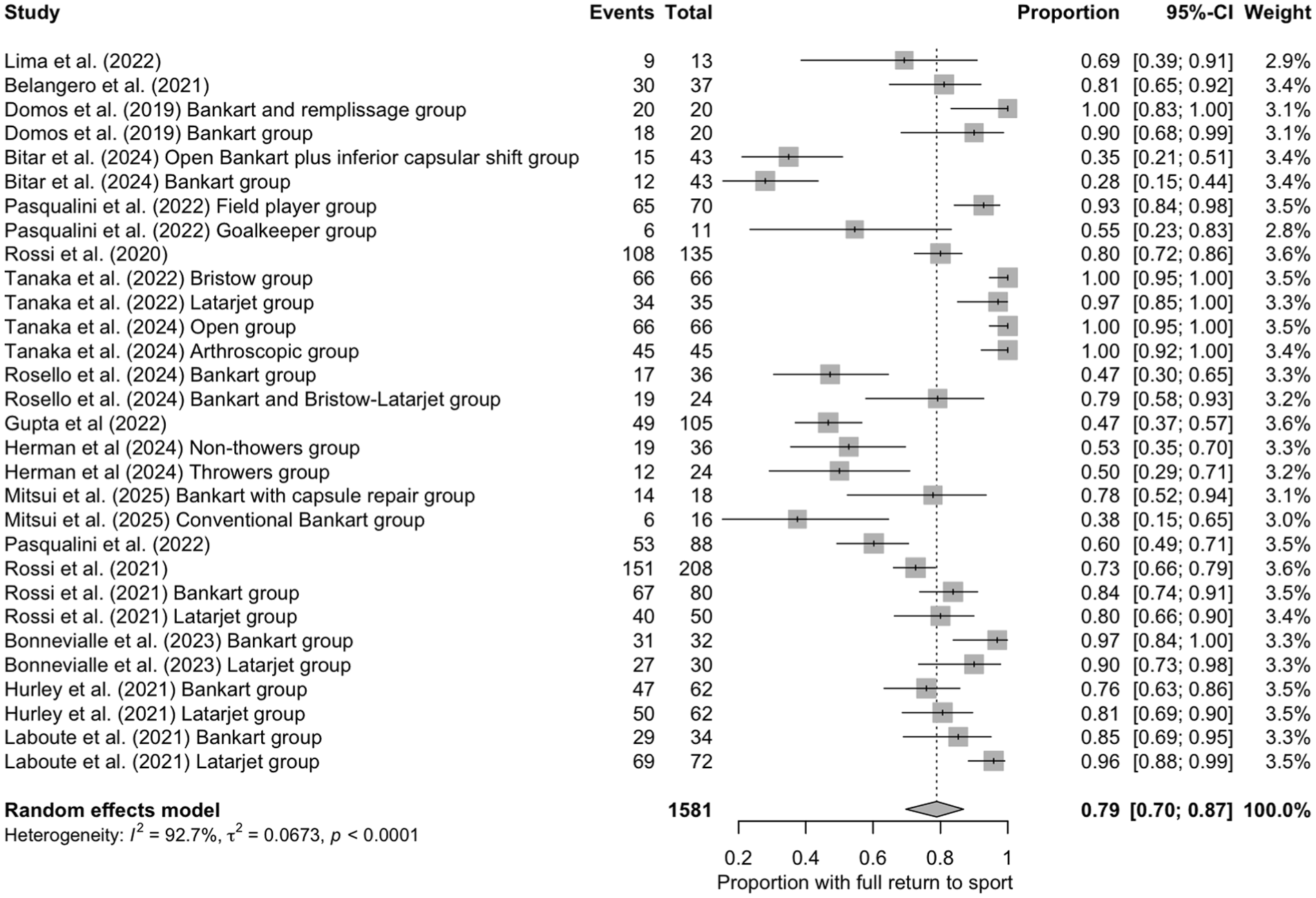
Forest plot demonstrating pooled proportions of athletes achieving full RTS after anterior shoulder stabilization procedures. Individual study estimates are presented with 95% CIs, and the pooled estimate was calculated using a random-effects model. RTS, return to sport.
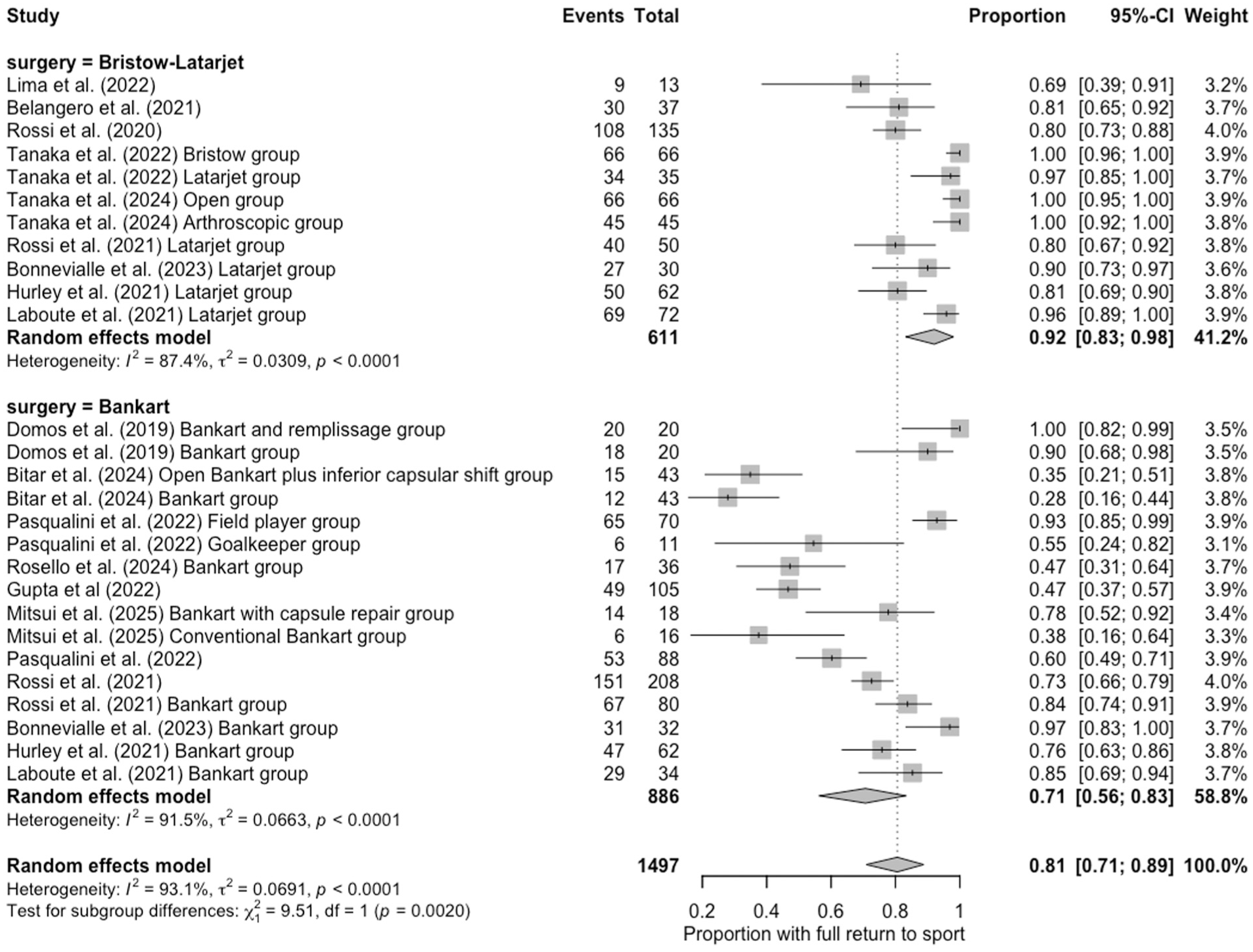
Forest plot of pooled proportions of athletes achieving full RTS after anterior shoulder stabilization, stratified by surgical technique (Bristow-Latarjet vs Bankart). Individual study estimates with 95% CIs are shown, with pooled estimates calculated using a random-effects model. RTS, return to sport.
Full cessation of sport across all studies was 10% (95% CI, 0.04-0.16) (Figure 5). The Bristow–Latarjet procedure demonstrated the lowest rate of sport cessation, with a pooled estimate of 5% (95% CI, 0.01-0.12) (Figure 6). Bankart repairs showed a higher rate of full cessation at 13% (95% CI, 0.04-0.25). Although Bristow–Latarjet procedures tended to result in fewer athletes fully discontinuing sport than Bankart procedures, subgroup differences were not statistically significant (P = .10).
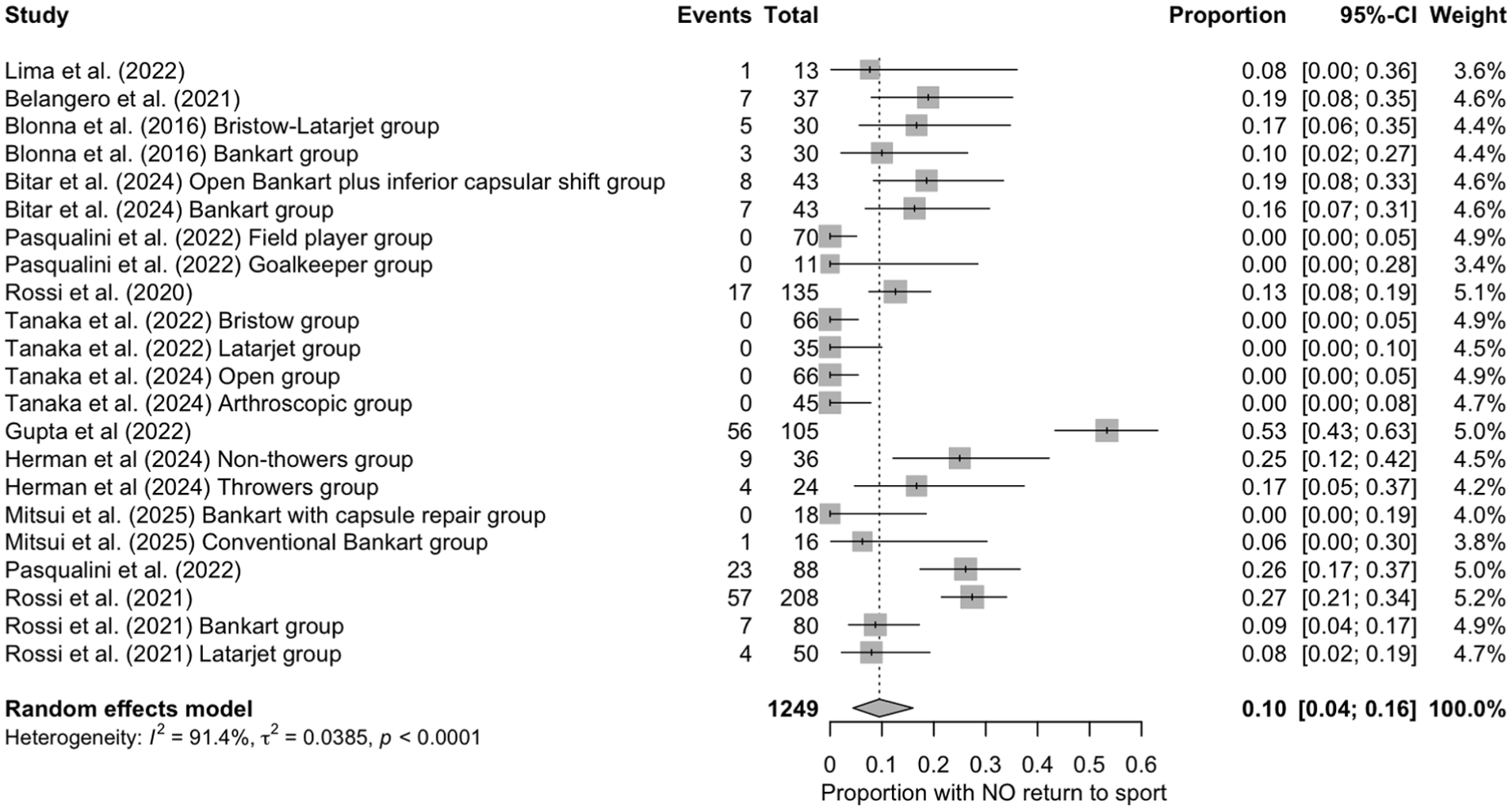
Forest plot demonstrating pooled proportions of athletes who did not achieve full RTS after anterior shoulder stabilization procedures. Individual study estimates are presented with 95% CIs, and the pooled estimate was calculated using a random-effects model. RTS, return to sport.
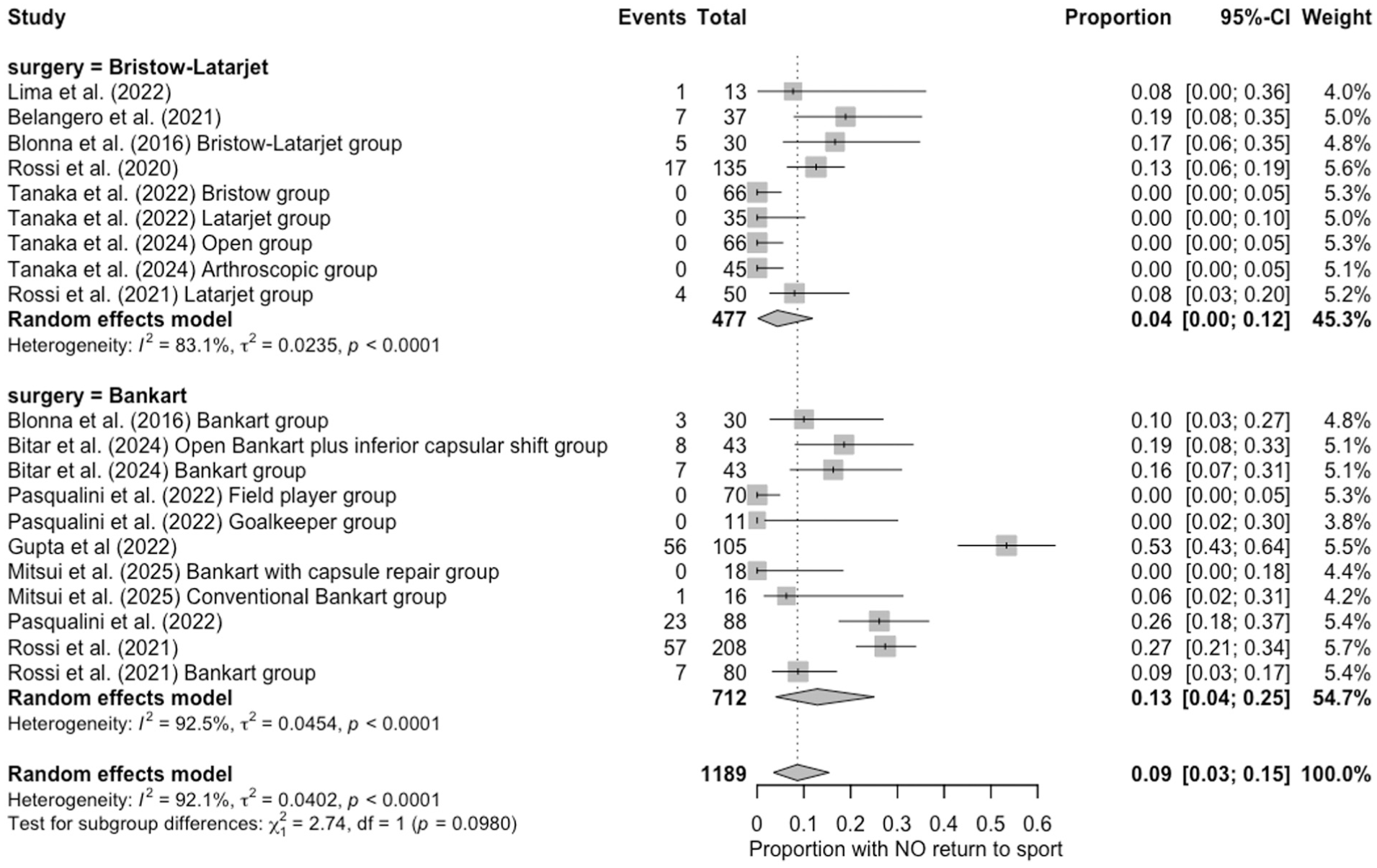
Subgroup forest plot demonstrating pooled proportions of athletes who did not achieve full RTS after anterior shoulder stabilization, stratified by surgical technique (Bristow-Latarjet vs Bankart). Individual study estimates with 95% CIs are shown, with pooled estimates calculated using a random-effects model. RTS, return to sport.
Discussion
In this systematic review and meta-analysis of athletes undergoing surgical stabilization for anterior shoulder instability, RTS was high, and cessation of sport was low across all procedures. The consistently high RTS rates across both procedures highlight the overall effectiveness of surgical stabilization in athletes. Athletes treated with Bristow-Latarjet were significantly more likely to return to their previous level of play and were also less likely to discontinue sport entirely. Although both procedures remain effective options for managing shoulder instability in competitive athletes, the observed differences suggest that the choice of stabilization technique may meaningfully influence postoperative athletic performance and long-term participation.
Our findings expand upon the existing literature evaluating RTS in athletes undergoing surgical stabilization for anterior shoulder instability. Broadly, these findings are consistent with previous meta-analyses evaluating RTS after shoulder stabilization, which have similarly reported high rates of postoperative athletic participation across both bone-block and soft-tissue procedures.7,20,36 To further contextualize these findings, we performed a subgroup analysis comparing outcomes between the Bristow-Latarjet and Bankart procedures. Direct comparison between these techniques can be challenging, as substantial efforts have been made over time to refine surgical indications for each procedure based on factors such as glenoid bone loss, Hill–Sachs lesions, and instability severity.23,24 Nevertheless, evaluating outcomes across procedures remains valuable for understanding the broader success of contemporary stabilization strategies in athletes. The Bristow-Latarjet procedure has been shown to have significantly lower rates of instability recurrence and eventual reoperation than Bankart repair in general and athletic populations.19,26
While recurrence and reoperation rates after Bristow-Latarjet and Bankart repair have been well characterized, particularly in the general population, patient-reported outcomes in athletes, such as RTS, remain less well defined. Two meta-analyses by Noyes et al 36 and Hurley et al 20 have examined this comparison in the athletic population, each showing a trend favoring the Latarjet for RTS but failing to reach statistical significance. The present study strengthens the comparison between the Bristow-Latarjet and Bankart procedures by drawing from a substantially larger cohort of athletes than previously available. By incorporating more studies and a larger overall population of competitive athletes, our analysis yields more precise pooled estimates and increases the statistical power needed to identify true differences in RTS outcomes. Additional studies have evaluated Bankart repair combined with remplissage, which addresses engaging Hill-Sachs lesions through posterior capsulotenodesis of the infraspinatus. In a multicenter retrospective study, Horinek et al 18 reported that arthroscopic Bankart repair with remplissage produced functional outcomes comparable or superior to Latarjet, with higher RTS rates among overhead and contact athletes and fewer complications despite greater bipolar bone loss in the remplissage cohort. 18 A meta-analysis by Davis et al 7 reported that the addition of remplissage to Bankart repair significantly improved RTS rates compared with isolated Bankart repair. Relatively few studies in the present analysis included remplissage, which may partly explain the lower RTS rates observed after Bankart repair and underscores an important consideration when interpreting comparisons with the Bristow-Latarjet procedure.
Several factors may explain why athletes undergoing the Bristow-Latarjet procedure demonstrate higher rates of full RTS. The Latarjet provides stability through coracoid transfer augmentation and a dynamic sling effect, offering robust resistance to anterior translation, particularly in athletes with substantial glenoid bone loss, high contact-sport demands, or prior failed soft-tissue repairs.15,52 These biomechanical advantages have contributed to excellent long-term outcomes, leading to increased popularity of the procedure and expanded indications in athletic populations.14,22 Another consideration is that the indications for Latarjet are more clearly defined for collision athletes, critical bone loss >15% to 20%, and off-track Hill-Sachs lesions. 24 Differences in surgical indications and biomechanical stabilization mechanisms may therefore contribute to the higher RTS rates observed after the Bristow-Latarjet procedure in this analysis.
Patients who are unable to fully RTS may require revision surgery. 51 Reoperation after failed primary stabilization carries meaningful health care costs and generally results in worse outcomes than the index procedure.30,33 Additionally, revision procedures are often more complex, may require additional bone grafting, and are associated with higher failure rates compared with primary stabilization. 1 An additional point to consider is that some stabilization techniques, such as the Latarjet, offer more limited revision pathways if the index procedure fails. 2
This study has several limitations. Heterogeneity in study design, surgical technique, postoperative rehabilitation, and outcome reporting limits the ability to draw definitive comparisons. Several research groups have published extensively on this topic, and, as with any meta-analysis, it is not possible to completely exclude the potential for inadvertent patient cohort overlap or double-counting. To mitigate this risk, we carefully reviewed study characteristics, recruitment periods, and institutional overlap to minimize the likelihood of duplicate inclusion. All included studies were nonrandomized, with the inherent risk of selection bias, particularly given that Latarjet is often performed in higher-risk instability patterns. Additionally, the use of a Bankart repair with remplissage was inconsistently reported, which may influence RTS rates in the Bankart cohort. Furthermore, sport type and competition level were not uniformly reported, precluding detailed subgroup analysis. RTS rates in collision and throwing sports may be lower than pooled estimates due to the increased functional demands of these activities. The lack of uniform reporting on bone loss, Hill-Sachs engagement, and previous instability episodes further limits interpretation. Despite these limitations, this review synthesizes the best available evidence and highlights meaningful differences in RTS outcomes across common stabilization procedures.
Future research should prioritize well-designed comparative studies that directly evaluate the Bankart and Latarjet procedures in athletic populations, using standardized definitions of instability, bone loss, and RTS outcomes. Randomized or rigorously matched prospective cohorts are needed to minimize selection bias and clarify whether the observed differences in RTS are attributable to procedure-specific biomechanics or underlying patient factors. Incorporating sport type, competition level, and objective performance metrics will further strengthen comparisons. Additionally, future studies should evaluate other bone-block procedures to determine whether similar RTS patterns are observed across alternative stabilization strategies.
Conclusion
Surgical stabilization for anterior shoulder instability in athletes was associated with high overall RTS rates across both procedures. Athletes treated with the Bristow-Latarjet procedure achieved significantly higher rates of full RTS than those undergoing Bankart repair. Despite variability in indications, results support the Bristow-Latarjet as a strong option for competitive athletes in whom durable stability and RTS potential are critical considerations. Future studies are needed that use rigorous comparative methodology with standardized reporting of instability patterns, bone loss, and RTS outcomes to more clearly define the relative effectiveness of Bankart and Latarjet procedures in athletes.
Footnotes
Supplementary Appendix 1: Search Strategies
Complete search strategies for all databases are provided below. Boolean operators, field tags, and filters were customized for each database to ensure accuracy and reproducibility.
Scopus final search:
(ALL("shoulder instability")
AND ALL(adolescen* OR “young adult”)
AND ALL(arthroscop* AND surg*)
AND ALL(sport* OR "sports-related" OR Baseball OR Basketball OR Swimming OR Football OR Wrestling OR Handball OR Volleyball OR Cricket OR Hockey OR Tennis OR "Table Tennis" OR Rugby OR Golf OR Boxing OR MMA OR "Mixed Martial Arts" OR Soccer OR Crossfit OR "Weight lifting")
AND ALL(outcome* OR “return-to-sport”)
AND LANGUAGE(english)
AND PUBYEAR > 2004
AND NOT TITLE(elbow OR hip OR knee OR review OR epidemiolog* OR "case report*" OR "technique guide*" OR clavicl* OR "ac joint" OR "acromioclavicular joint" OR humerus OR biceps OR triceps OR sternoclavicular OR "thoracic outlet" OR "brachial plexus" OR replacement OR fusion OR osteotomy OR "open reduction" OR "hardware removal" OR "conservative treatment" OR geriatr* OR cadaver* OR animal* OR biomechanic* OR tumor OR cancer OR infection OR congenital OR rheumatoid OR scapula OR acromion OR ulna OR radius OR wrist OR hand OR finger OR pelvis OR femur OR tibia OR fibula OR ankle OR foot OR toe OR "joint replacement" OR prosthesis OR implant OR amputation OR "nerve transfer" OR "spine surgery" OR laminectomy OR stroke OR paralysis OR "multiple sclerosis" OR "cerebral palsy" OR "genetic disorder" OR malformation OR dysplasia OR spasticity OR infant OR neonatal OR adult OR elderly OR aging OR ovine OR porcine OR canine OR feline OR murine OR rodent OR radiologic OR "CT scan" OR MRI OR ultrasound OR "anatomical study" OR editorial OR commentary OR letter OR opinion OR guideline OR "white paper" OR protocol OR "conference abstract" OR "global health" OR suture* OR knot* OR "meta-analysis" OR psychologic* OR socioeconomic OR "acr appropriateness criteria" OR epilep* OR "computed tomography" OR talus*)
Final revision submitted April 9, 2026; accepted April 13, 2026.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.