
Abstract
Background:
Acetabular wave signs represent a form of cartilage delamination and may progress to more extensive chondral damage in patients with femoroacetabular impingement (FAI). The current lack of high-quality evidence supporting an optimal surgical strategy underscores the need to investigate reverse microfracture as a viable, safe, cost-effective, and cartilage-preserving treatment option.
Purpose/Hypothesis:
The purpose of this study is to evaluate the clinical and imaging outcomes of arthroscopic treatment of acetabular wave signs using a reverse drilling technique performed from the supralabral region of the acetabulum without damaging the articular cartilage. It was hypothesized that this technique would provide clinical improvement without additional cartilage damage.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 40 patients (mean age, 40.2 ± 9.2 years; 24 women and 16 men) underwent hip arthroscopy with concomitant FAI treatment and reverse microfracture, with a minimum follow-up of 2 years. Outcomes included Harris Hip Score (HHS), visual analog scale (VAS), lateral center-edge angle (LCEA), alpha angle, and magnetic resonance imaging (MRI).
Results:
The HHS increased from 68.88 ± 10.81 to 97.90 ± 2.22 (P < .001), and the VAS score decreased from 7.40 ± 1.03 to 1.35 ± 1.08 (P < .001). The alpha angle decreased from 61.88°± 2.50° to 50.05°± 1.75° (P < .001), and the LCEA decreased from 36.75°± 4.66° to 32.43°± 1.92° (P < .001). MRI demonstrated no deterioration in cartilage quality or additional lesions after the procedure, with cartilage appearance similar to adjacent noninjured areas and no evidence of delamination.
Conclusion:
Reverse microfracture may represent a potential treatment option for acetabular wave signs. In this retrospective series, the procedure was associated with improvement in pain and functional scores, and no evidence of additional cartilage deterioration was observed on postoperative MRI during a minimum 2-year follow-up. However, given the absence of a control group, the specific contribution of the drilling technique to the observed clinical improvements cannot be determined.
Clinical improvement likely reflects the combined effect of comprehensive arthroscopic management of FAI rather than the isolated effect of reverse drilling.
Acetabular chondral lesions, particularly wave signs, have a low preoperative diagnostic accuracy and are more reliably identified intraoperatively. 3 These lesions are characterized by focal delamination of the cartilage, creating an appearance similar to that of a wave or blister.5,9 Magnetic resonance imaging (MRI) is useful for assessing acetabular cartilage thickness and quality1,10 but has limited sensitivity for detecting wave signs. When associated with cam-type femoroacetabular impingement (FAI), these lesions may progress to full-thickness chondral defects and osteoarthritis. 12
A therapeutic option for managing wave signs is the reverse microfracture technique, in which retrograde drilling is performed through the subchondral bone toward the blister without violating the cartilage surface, thereby decompressing the lesion. The goal is to allow clot formation, which facilitates adherence of the cartilage to the underlying bone during the ossification of the perforations. 9
Despite increasing recognition of acetabular wave signs during hip arthroscopy, the optimal management of this pathology remains unclear. Most available studies consist of technical descriptions or retrospective case series, and there is limited evidence specifically evaluating treatment strategies directed at the delaminated cartilage itself. Consequently, there is a need for further investigation into surgical techniques that aim to stabilize the chondral lesion while preserving articular cartilage integrity. The purpose of the present study was therefore to evaluate the clinical and imaging outcomes of acetabular wave signs treated with a reverse drilling technique at a minimum 2-year follow-up, using the Harris Hip Score (HHS), visual analog scale (VAS), and pre- and postoperative MRI to assess functional improvement and cartilage preservation.
We hypothesized that reverse microfracture of the subchondral bone for the treatment of acetabular wave signs would be associated with improvement in clinical outcomes without evidence of additional cartilage deterioration on postoperative MRI.
Methods
We retrospectively reviewed the medical records of 380 patients who underwent hip arthroscopy for FAI between January 2015 and December 2020. Patients’ quality of life and pain levels were assessed retrospectively using the HHS 7 and VAS. 6
The appearance of the acetabular cartilage was evaluated using a standardized 3-T hip MRI protocol2,17 that included both anatomical and fluid-sensitive sequences. All examinations were interpreted by the same senior musculoskeletal radiologist who was blinded to patient identity, clinical outcomes, and the temporal sequence of the scans. This approach ensured intraobserver consistency, with all postoperative assessments performed at least 2 years after surgery.
As no standardized, universally accepted scoring system exists for acetabular wave signs, a structured qualitative MRI assessment was employed.
The hip MRI protocol consisted of conventional morphological T1-weighted and proton density T2-weighted fat-suppressed sequences, 17 which were used to compare cartilage thickness and quality across the acetabular surface and determine whether reverse microfracture resulted in additional chondral damage or preserved cartilage morphology at the 2-year follow-up.
This structured evaluation included analysis of signal characteristics, cartilage thickness, surface morphology, and integrity of the chondro-subchondral interface. The methodology followed previously described approaches for postoperative imaging assessment in hip arthroscopy. 5
Patients diagnosed with acetabular wave signs according to the Haddad classification 18 (grade 1) were treated using reverse microfracture (retrograde drilling).
Surgical Technique
All procedures were performed by the same senior surgeon (L.C.D.L.) with the patient in the supine position on a hip arthroscopy traction table, under fluoroscopic guidance to achieve a minimum of 2 cm of joint distraction. Standard anterolateral (ALP) and midanterior portals were used with a 70° arthroscope. Before wave sign treatment, all underlying structural abnormalities were addressed: femoral osteoplasty was performed in patients with cam or mixed-type FAI using a motorized bur to restore a normal alpha angle, and acetabular rim trimming was performed in patients with pincer or mixed-type FAI to normalize the lateral center-edge angle (LCEA). The wave sign was then identified by systematic probing of the acetabular cartilage; the lesion was recognized as a blister-like focal delamination that ripples under probe pressure without breach of the cartilage surface.
Reverse microfracture was performed through a proximal anterolateral accessory portal, positioned approximately 30° to 45° proximal and anterior to the ALP. A cannulated introducer was advanced under direct arthroscopic visualization to the supra-acetabular bone, targeting the region overlying the wave lesion at a safe distance of approximately 2 mm from the chondrolabral junction. A 4.5-mm working cannula was placed over a nitinol guidewire, and a 2.3-mm drill bit was advanced in low-rotation mode from the extra-articular surface toward the cartilage interface, creating multiple perforations spaced 2 to 3 mm apart across the full extent of the lesion. Pump pressure was then reduced to confirm bone marrow bleeding through the drill holes. The biological rationale of the technique is based on decompressing the intralesional pressure within the blister and inducing a local marrow clot, which acts as a biological adhesive to promote re-adhesion of the delaminated cartilage to the subchondral bone without violating the intact articular surface. (Figure 1). 9
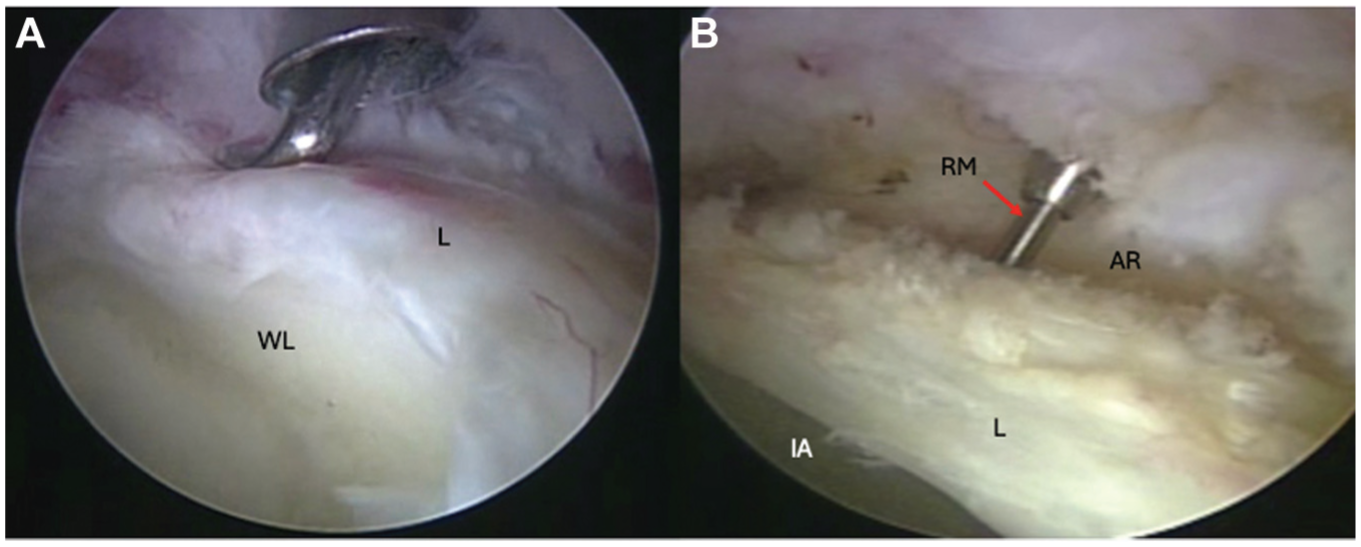
(A) Wave sign (bubble). (B) Microfracture in the supra-acetabular region, between the labrum and the capsule, toward the wave sign. AR, acetabular rim; IA, intra-articular; L, labrum; RM, reverse microfracture; WL, wave sign.
All patients followed a standardized postoperative rehabilitation protocol adopted by our institution, based on previously published hip arthroscopy rehabilitation guidelines 29 (Table 1). The protocol consisted of a progressive, phase-based program emphasizing early protection of the cartilage and labrum, gradual restoration of range of motion, progressive strengthening, and return to sport activities.
Standardized Postoperative Physical Therapy Protocol a
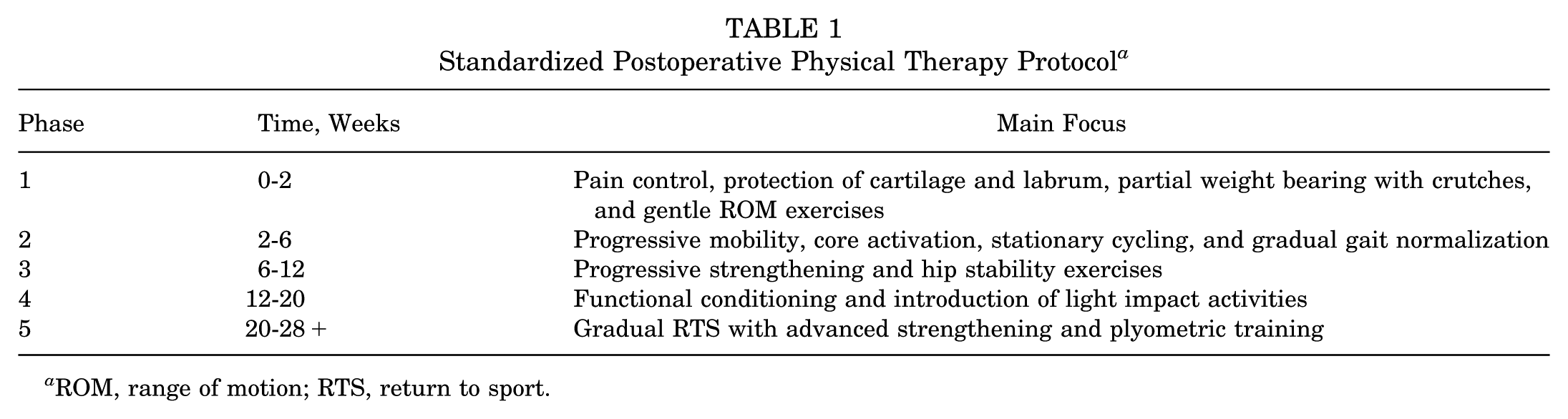
ROM, range of motion; RTS, return to sport.
Follow-up Protocol
The primary outcome of the present study was improvement in hip function as measured by the HHS between the preoperative assessment and the final follow-up.
Secondary outcomes included changes in VAS pain scores, postoperative MRI evaluation of cartilage integrity, presence of additional chondral lesions, and complications or need for revision surgery.
All patients were followed postoperatively through routine clinical evaluations. Clinical outcomes were recorded preoperatively and at the final follow-up.
Patients underwent postoperative MRI evaluation at a minimum of 24 months after surgery to assess cartilage integrity and to identify potential progression of chondral damage.
Clinical outcome measures (HHS and VAS) and postoperative MRI were obtained at the same follow-up visit performed at a minimum of 24 months after surgery. Therefore, a single postoperative assessment point was used to analyze both clinical and imaging outcomes.
Statistical Analysis
The data were analyzed descriptively, presenting the mean, standard deviation, minimum, and maximum values for numerical variables, and the number and percentage for categorical variables to verify whether the data followed a normal distribution. Graphical methods (histograms and boxplots) and the Shapiro-Wilk test 27 were used.
Because the distributions were not normal, inferential comparisons between the pre- and postoperative paired measurements (HHS, VAS, LCEA, and alpha angle) were performed using the Wilcoxon signed-rank test.
A significance level of P < .05 was considered statistically significant, and all tests were 2-tailed.
The effect size was reported as the rank-biserial correlation, derived from the Wilcoxon signed-rank test. This measure reflects the magnitude and direction of the paired differences between pre- and postoperative values. For interpretation of magnitude, conventional thresholds proposed by Cohen were adopted: 0.10, small; 0.30, medium; and 0.50, large. Accordingly, |r| = 1 was interpreted as the maximum possible effect size for this metric. 8
A post hoc power analysis was also performed in R (R Foundation for Statistical Computing) to determine the maximum observed effect size (|r| = 1). Statistical power was estimated using the pwr package in R based on the observed effect sizes and the available sample size. For these comparisons, the estimated statistical power exceeded 99.9%.
All analyses were conducted using 25 R software, Version 4.3.2. The Wilcoxon signed-rank test was computed using native R functions, effect sizes were calculated using the ggstatsplot package, 23 and the post hoc power analysis was performed using the pwr package in R.
Results
Among the 380 patients initially evaluated, 40 met the inclusion criteria, were diagnosed with an acetabular wave sign, and underwent reverse microfracture during the study period, as illustrated in the flowchart (Figure 2). Of these, 22 patients underwent cam osteoplasty combined with reverse microfracture, 17 underwent combined cam and pincer osteoplasty with reverse microfracture, and 1 underwent isolated pincer osteoplasty with reverse microfracture.
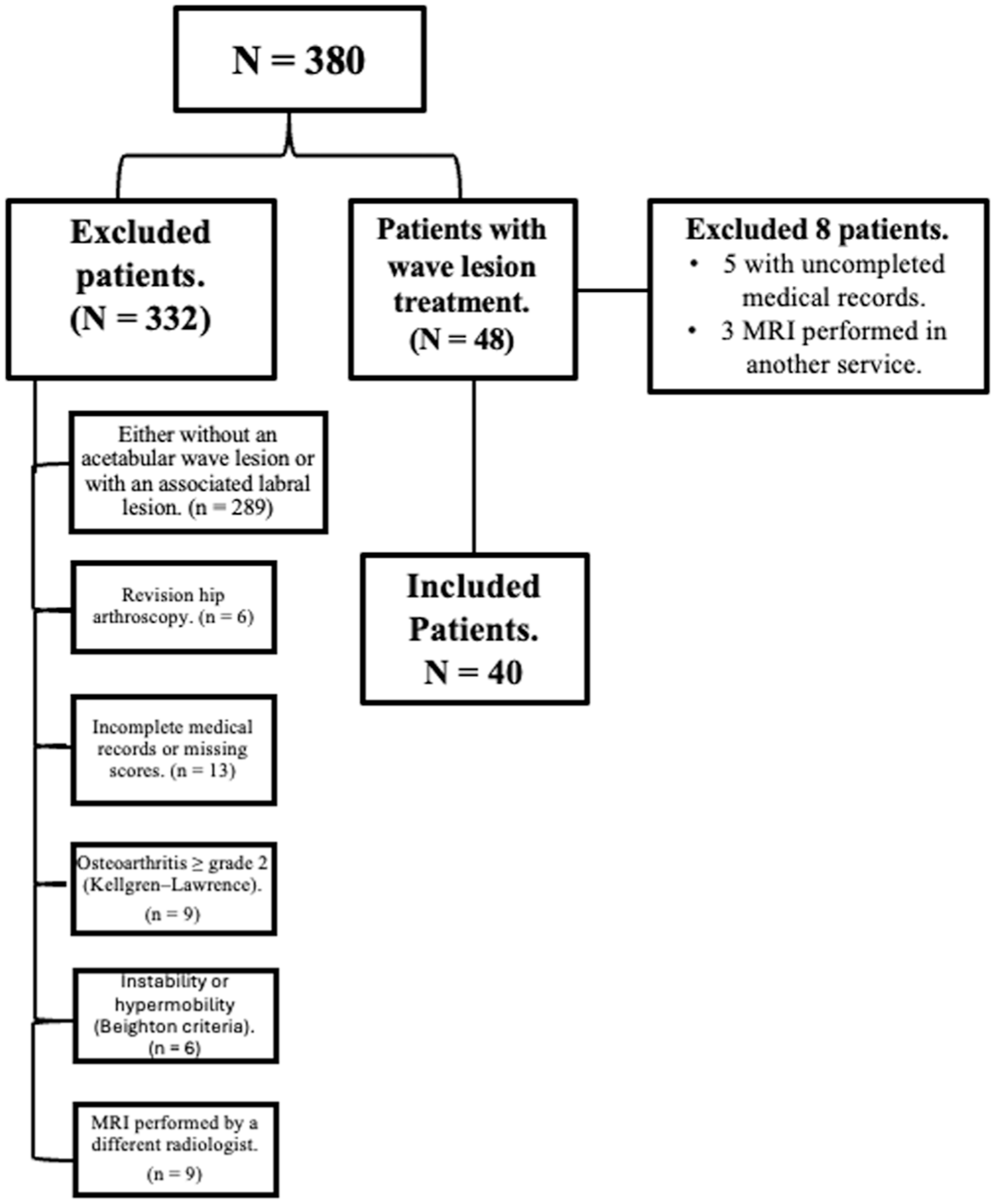
A flowchart of the inclusion and exclusion criteria.
Statistical analyses were performed in 2 steps: a descriptive analysis of demographic and clinical variables and a comparison of pre- and postoperative scores using the Wilcoxon signed-rank test for numerical variables (Table 2).
Descriptive Analysis of Demographic and Clinical Data a
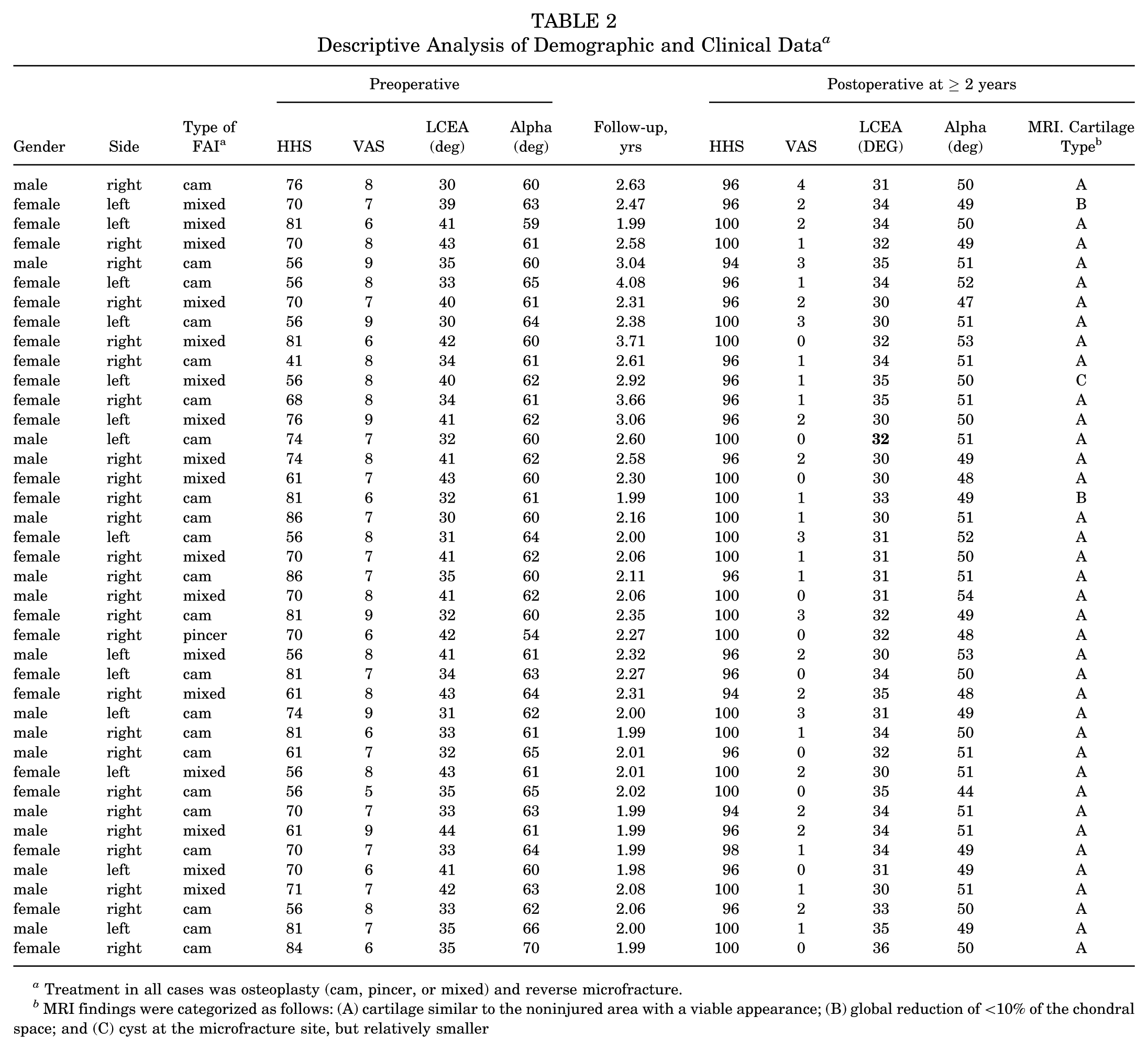
Treatment in all cases was osteoplasty (cam, pincer, or mixed) and reverse microfracture.
MRI findings were categorized as follows: (A) cartilage similar to the noninjured area with a viable appearance; (B) global reduction of <10% of the chondral space; and (C) cyst at the microfracture site, but relatively smaller
The sample consisted of 40 patients, predominantly women (60%), with right hip involvement in most cases (65%). Wilcoxon signed-rank tests were used to compare functional (HHS) and pain (VAS) scores between the preoperative period and >2 years postoperatively. A significant improvement in the HHS score was observed (P < .001), with the mean increasing from 68.88 to 97.90. A significant reduction in the VAS score was also observed (P < .001), with a mean decreasing from 7.40 to 1.35.
The mean alpha angle decreased from 61.88°± 2.50° preoperatively to 50.05°± 1.75° postoperatively (Wilcoxon P < .001; rank-biserial correlation = 1), while the mean LCEA decreased from 36.75°± 4.66° to 32.43°± 1.92° (Wilcoxon P < .001; rank-biserial correlation = 0.81). Although the effect size for the LCEA was large according to the Cohen criteria, it was not maximal because acetabular rim trimming was performed only in patients with pincer or mixed FAI (Cohen, 1988). Consequently, not all patients underwent acetabular correction, resulting in smaller or absent changes in the LCEA in some cases.
AppendixTable A1 presents the baseline demographic and clinical characteristics of the study population, including sex distribution, laterality, and FAI type. Table 3 summarizes postoperative outcomes, including patient-reported outcome measures (HHS and VAS) and MRI-based cartilage findings assessed at follow-up after ≥2 years.
Outcomes at Follow-up After >2 Years a
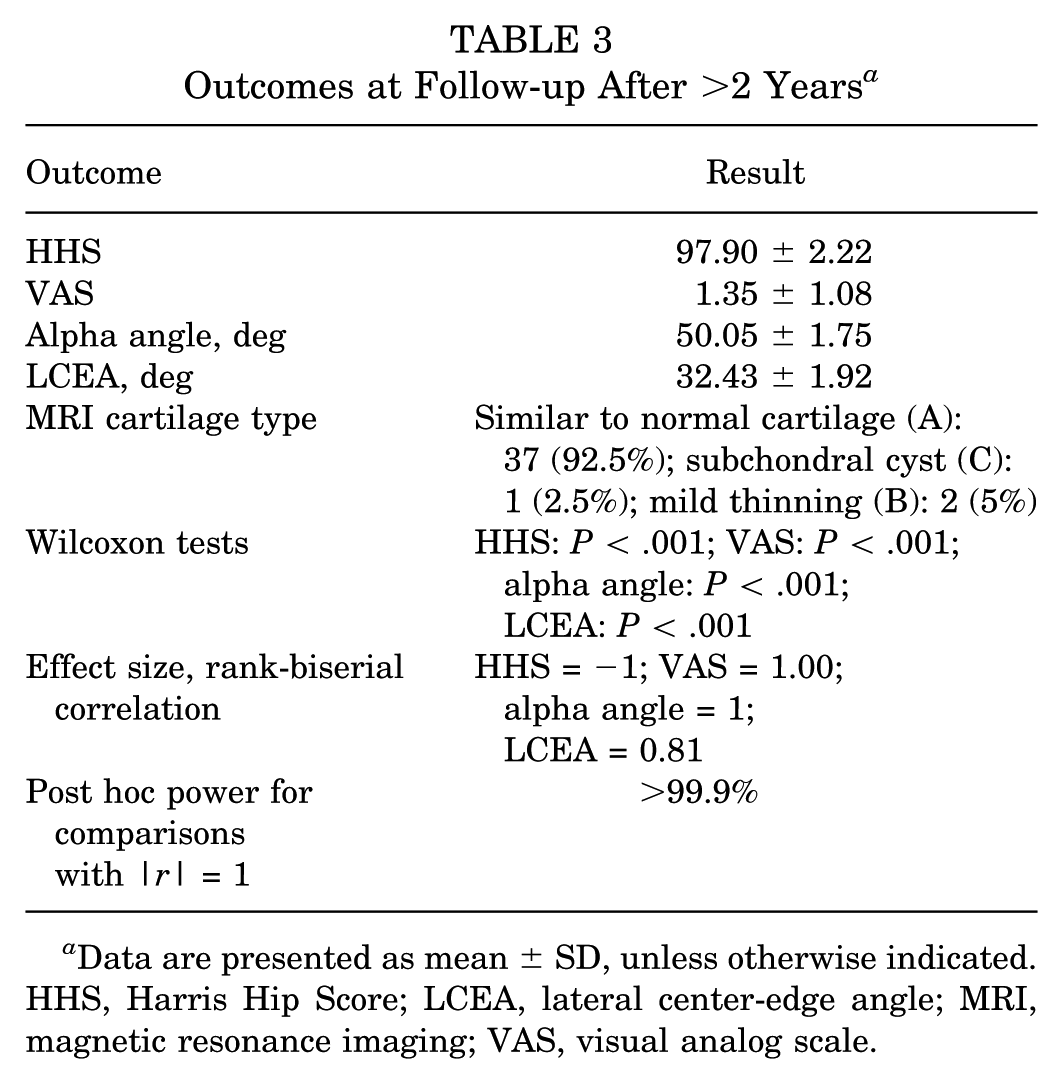
Data are presented as mean ± SD, unless otherwise indicated. HHS, Harris Hip Score; LCEA, lateral center-edge angle; MRI, magnetic resonance imaging; VAS, visual analog scale.
Patients with cam, mixed, or pincer-type FAI underwent osteochondroplasty to correct bone deformities. Capsular closure was not performed because there were no clinical criteria for hypermobility or microinstability; none underwent labral repair.
One patient demonstrated a small cyst formation (2 × 3 mm) at the microfracture site that remained radiologically stable over a 2-year follow-up period. Two patients exhibited a global reduction of <10% in joint space thickness compared with baseline. No patient progressed to total hip arthroplasty.
One patient required revision hip arthroscopy 29 months after the index surgery, after a traumatic labral tear sustained during a running training session, which was managed with arthroscopic labral repair using suture anchors. Intraoperative inspection of the previously treated area during revision served as an incidental second-look assessment. It demonstrated chondral adhesions at the site of the wave sign, consistent with biological healing of the delaminated cartilage. The mean follow-up duration was 2.41 years (median, 2.24 years; range, 2.01-4.14 years). All patients had a minimum follow-up of 2-year, as per the study's inclusion criteria. The distribution of follow-up times is illustrated in Figure 3, and the individual follow-up values are reported in Table 2.
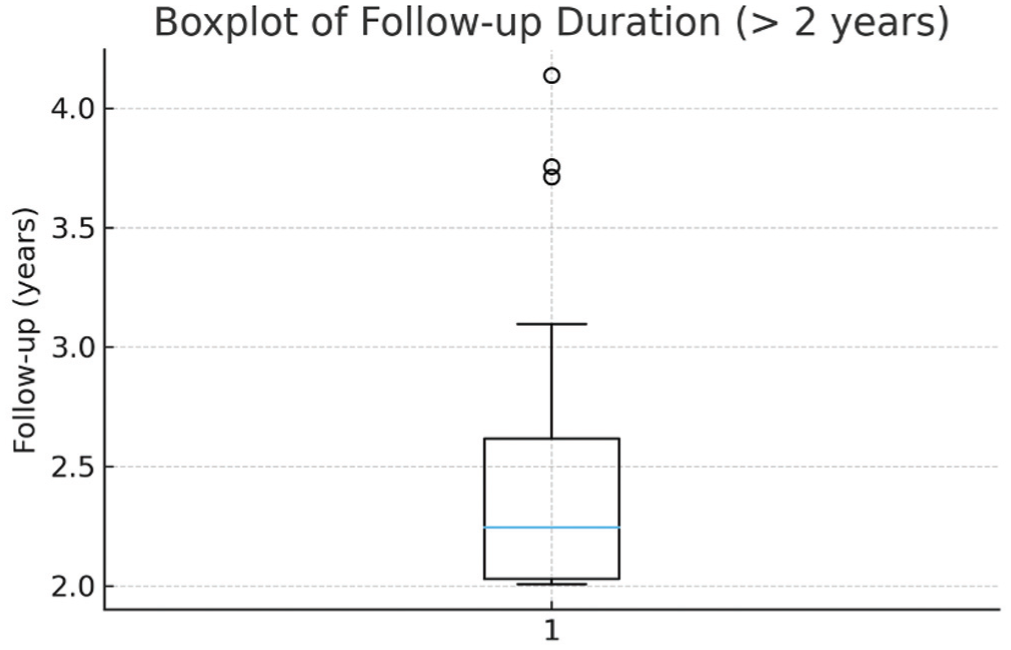
Boxplot illustrating the distribution of postoperative follow-up duration (in years) for all included patients. HHS,
Wilcoxon signed-rank tests demonstrated statistically significant improvements in all four outcomes between the preoperative period and the minimum two-year follow-up (all P < .001). Descriptive statistics, effect sizes, and post hoc power estimates for each outcome are summarized in Table 4. Effect sizes were large across all comparisons; HHS, VAS, and alpha angle reached the maximum rank-biserial correlation magnitude (|r| = 1), whereas the LCE angle showed a large but non-maximal effect (|r| = 0.81), reflecting the fact that acetabular rim trimming was performed only in patients with pincer or mixed FAI. Post hoc power analysis for outcomes with |r| = 1 indicated statistical power greater than 99.9%.
Descriptive Statistics of the Score Measures Used a
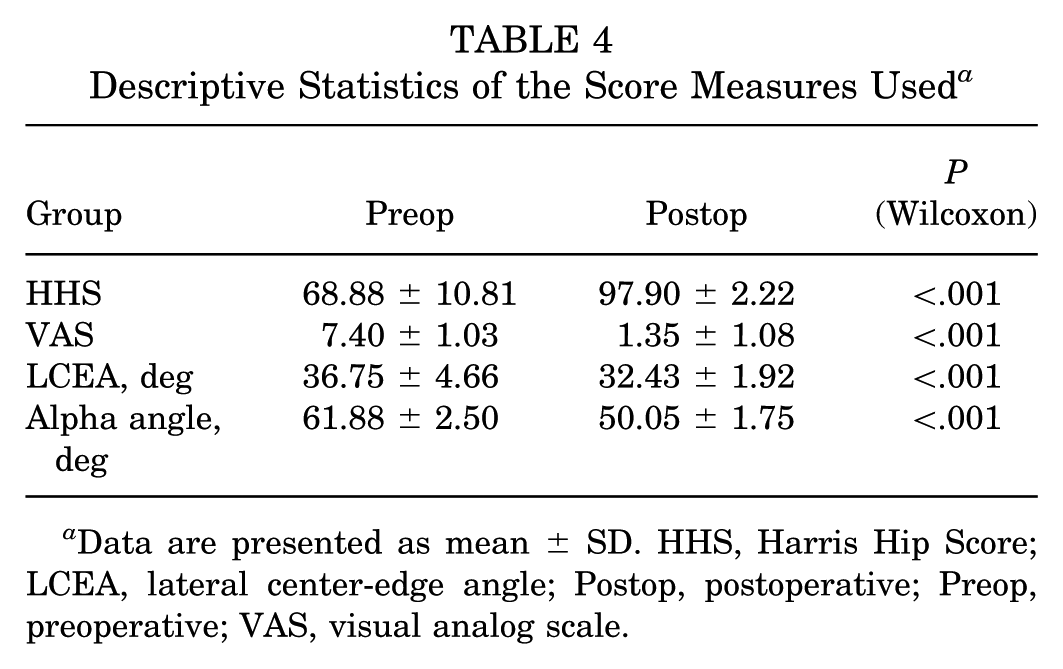
Data are presented as mean ± SD. HHS, Harris Hip Score; LCEA, lateral center-edge angle; Postop, postoperative; Preop, preoperative; VAS, visual analog scale.
Table 4 shows the distributions of the variables HHS pre-surgery and HHS more than two-years after surgery, and the VAS pre-surgery and VAS more than two-years after surgery, with a significant improvement in scores two years after surgery.
Temporal Analysis of Scores
Longitudinal analysis revealed a significant improvement in clinical scores between the preoperative period and the 2-year follow-up. There was an increase in the mean HHS score and a marked reduction in the VAS score. The means and standard deviations for each variable at both time points are presented in Table 4.
MRI Analysis
Comparative MRI analyses performed preoperatively and at 2-year follow-up did not reveal new structural chondral defects in the treated region, including flap lesions or progressive cartilage thinning. Cartilage thickness and signal characteristics appeared similar to those observed in the initial examination.
Although conventional MRI has limited sensitivity for directly identifying acetabular wave signs, representative pre- and postoperative MRI images from the same hips demonstrated preservation of cartilage morphology without evidence of persistent delamination or progressive structural cartilage deterioration at the treated site (Figure 4). MRI findings were categorized as follows: (A) cartilage similar to the noninjured area with a viable appearance; (B) global reduction of <10% of the chondral space; and (C) cyst at the microfracture site, but relatively smaller (Table 2).
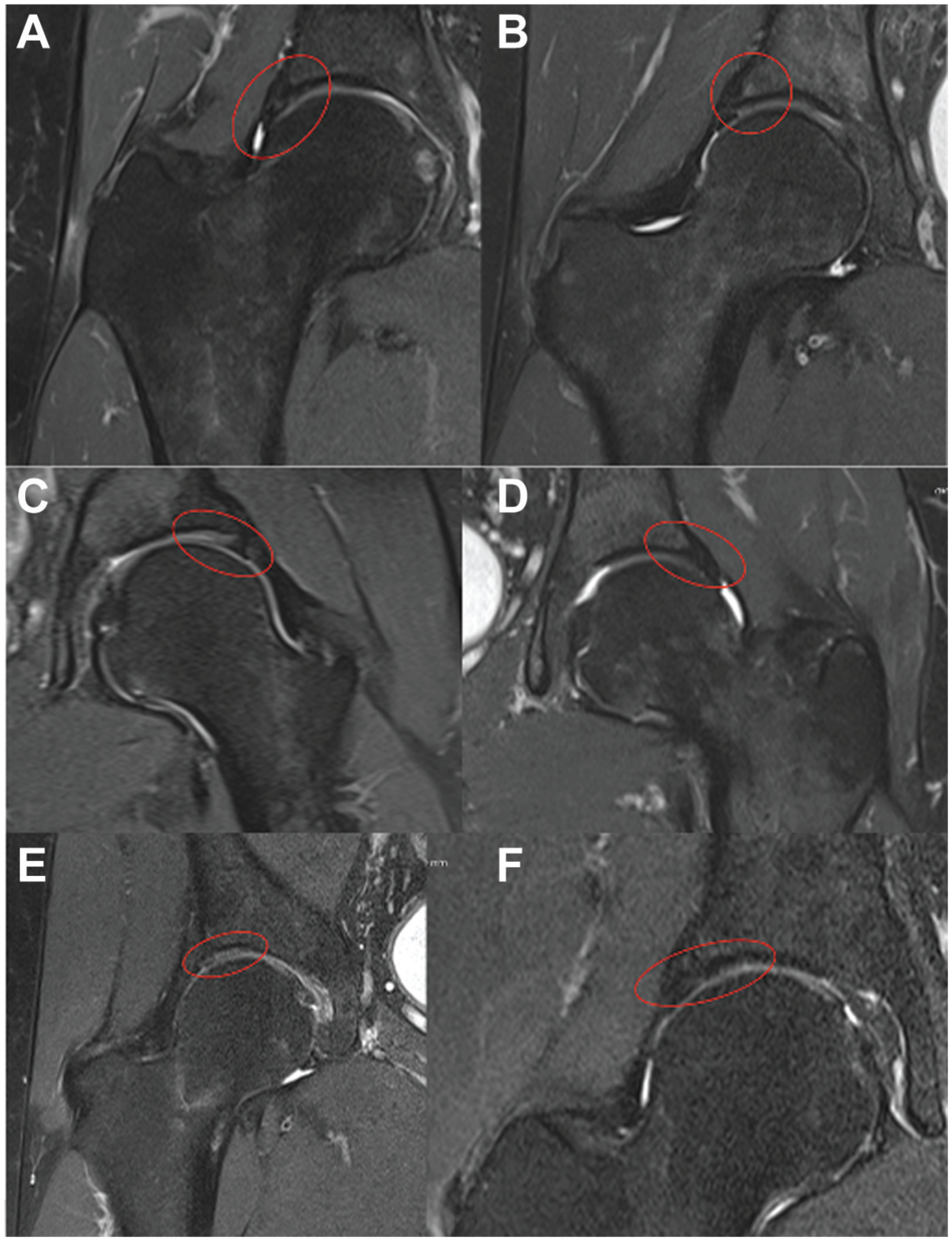
Pre- and postoperative MRI of 3 representative hips treated with reverse microfracture for acetabular wave signs. Each pair of images corresponds to the same hip of the same patient. (A) Patient 1, preoperative MRI demonstrating a wave sign and (B) postoperative MRI showing preservation of cartilage morphology after reverse microfracture. (C) Patient 2, preoperative wave sign and (D) postoperative appearance of the treated region. Patient 3, preoperative wave sign (E) and postoperative appearance of the treated region (F). MRI, magnetic resonance imaging.
Discussion
The most important finding of the present study is that arthroscopic treatment of acetabular wave signs using reverse drilling, combined with correction of the underlying FAI morphology, was associated with significant improvements in patient-reported outcomes and no evidence of progressive cartilage deterioration on postoperative MRI during mid-term follow-up.
FAI is widely recognized as a major contributor to acetabular cartilage injury and the development of wave signs. The randomized trial published in The Lancet 14 demonstrated that arthroscopic management of FAI requires systematic correction of the underlying structural abnormalities, including cam and pincer morphology, as well as addressing associated chondral and labral pathology. Ayeni et al 4 demonstrated that, in most clinical studies evaluating cartilage treatment during hip arthroscopy, it is difficult to isolate the specific contribution of a single chondral intervention from the overall effect of the comprehensive arthroscopic procedure.
Some surgeons advocate correction of the underlying mechanical pathology without directly addressing the wave sign, reporting satisfactory clinical outcomes. Makovicka et al 19 demonstrated that femoral osteoplasty alone, without direct chondrolabral stabilization, yielded significant improvements in patient-reported outcomes at a minimum 2-year follow-up in patients with the wave sign, supporting the view that eliminating the cam deformity may be sufficient in selected cases. However, the same study also showed superior functional scores and lower revision rates when direct chondrolabral stabilization was added, suggesting that addressing the wave sign directly may confer additional benefit. 19 Comparative studies evaluating the outcomes of treating versus leaving wave signs untreated remain limited. The systematic review by Onggo et al 22 explicitly noted that no study in the current literature has investigated the natural history and progression of the wave sign with or without treatment, underscoring the need for further evidence to guide surgical decision-making in this setting.
Makovicka et al 19 compared hip arthroscopy for FAI performed with and without direct treatment of acetabular wave signs using suture anchor fixation. The authors reported improved clinical outcomes in patients who underwent direct stabilization of the chondral lesion.
These findings suggest that, in selected cases, addressing the wave sign itself may provide additional benefit beyond correction of the underlying mechanical pathology alone.
In the present series, all patients underwent arthroscopic correction of FAI morphology, combined with treatment of the acetabular wave sign using reverse drilling. The correction of cam or pincer deformities was considered essential because persistent mechanical conflict may promote progression of cartilage delamination to more advanced chondral damage, including flap formation or segmental cartilage loss. Therefore, osteochondroplasty primarily addresses the pathological biomechanical environment rather than directly restoring cartilage quality. This approach is consistent with previously reported surgical strategies for wave signs, in which simultaneous correction of FAI deformities was routinely performed. 16
The clinical improvements observed in our cohort are consistent with previously published reports describing favorable outcomes following minimally invasive stabilization techniques for acetabular cartilage lesions. Arriaza et al 3 and Makovicka et al 19 reported encouraging clinical and arthroscopic findings after treatment of wave signs using techniques aimed at stabilizing the chondrolabral interface. In particular, Makovicka et al 19 described cases in which revision arthroscopy demonstrated restoration of cartilage adherence to the subchondral bone after chondrolabral stabilization. A similar observation was made in the single patient in our series who underwent revision arthroscopy, in which the previously delaminated cartilage appeared firmly reattached to the underlying subchondral bone.
Several surgical strategies have been proposed for the management of acetabular wave signs, including fibrin adhesive fixation, chondrolabral stabilization, and marrow stimulation procedures. While fibrin adhesive techniques have demonstrated promising results, concerns remain about the long-term stability of cartilage repair and the difficulty of confirming true biological healing without histological evaluation or revision arthroscopy.15,28
Reverse drilling represents an alternative approach aimed at stimulating subchondral bone vascularization while preserving the intact cartilage surface, potentially promoting biological adhesion of the delaminated cartilage.9,10
The association between cam-type morphology and acetabular cartilage injury has been widely reported in the literature and was also observed in the present cohort. Cam morphology was identified in approximately half of our patients, supporting the concept that abnormal femoral head–neck offset may contribute to shear forces at the acetabular cartilage surface and predispose to delamination injuries.22,26 These biomechanical considerations further support the importance of addressing the underlying impingement mechanism during surgical treatment.
Previous studies have also reported improvements in patient-reported outcomes after arthroscopic management of acetabular cartilage lesions. Rafi et al 26 in a prospective randomized trial demonstrated significant postoperative improvements in HHS and VAS scores after hip arthroscopy for FAI-associated pathology. Although the design of the present study does not allow isolation of the specific contribution of reverse drilling to these improvements, the magnitude of clinical improvement observed in our cohort is consistent with previously reported results in similar patient populations.20,24
Imaging evaluation of acetabular cartilage lesions has also evolved substantially in recent years. Gao et al 13 in a study published in the Orthopaedic Journal of Sports Medicine, demonstrated that modern MRI techniques can provide a reliable assessment of cartilage integrity in both the pre- and postoperative settings. Additional advances in cartilage imaging—including quantitative MRI sequences and dedicated cartilage mapping software—have further improved the ability to detect subtle changes in cartilage morphology and composition. 26
In our series, postoperative MRI demonstrated no evidence of cartilage thinning, deterioration of chondral quality, or recurrent delamination at the treated site, findings consistent with previously reported imaging outcomes after treatment of acetabular cartilage lesions.3,11
From a technical standpoint, the procedure described in this study is more accurately characterized as reverse drilling rather than classic microfracture. Unlike conventional microfracture techniques that penetrate the cartilage surface to access the subchondral bone, reverse drilling is performed from the subchondral side toward the cartilage–bone interface to stimulate subchondral vascular channels while preserving the integrity of the overlying cartilage. However, the technique requires careful control of drilling depth and orientation to avoid iatrogenic cartilage injury.
From an anatomical perspective, acetabular wave signs represent a specific form of cartilage delamination in which the articular cartilage separates from the underlying subchondral bone while the chondrolabral junction remains intact. This unique pathology may limit the effectiveness of conventional cartilage repair techniques applied from the articular surface. Reverse drilling attempts to address this pathology by promoting subchondral bone stimulation without disrupting the intact cartilage layer.
Importantly, to date, no prospective randomized clinical trials specifically evaluating the treatment of acetabular wave signs have been identified in the literature. Most published studies addressing this pathology consist of retrospective case series or observational analyses, including those reported by several experienced authors in the field. Therefore, the methodological design of the present study is consistent with the current literature on the surgical management of wave signs.
Nevertheless, several limitations of the present study must be acknowledged. First, the retrospective design and reliance on electronic medical records may introduce potential sources of bias. Second, the absence of a control group prevents the determination of the specific contribution of the reverse drilling technique to the observed clinical improvements, which may also reflect the effect of comprehensive arthroscopic treatment of FAI. Third, no a priori sample size calculation was performed because the study included all consecutive eligible patients treated during the study period. Nevertheless, a post hoc power analysis based on the observed effect sizes demonstrated that the available sample provided greater than 99% statistical power for the primary comparisons. Additionally, histological confirmation of cartilage repair was not available except in a single patient who underwent revision arthroscopy.
Another limitation relates to the use of HHS and VAS as outcome measures. Although these instruments remain commonly reported, contemporary hip preservation studies frequently use more specific PROMs such as the International Hip Outcome Tool or Copenhagen Hip and Groin Outcome Score. Because the present investigation is a retrospective analysis of patients treated over several years, the HHS and VAS were used as they were the standardized outcome instruments included in the institutional protocol during the study period. Therefore, more modern PROMs were not consistently available for all patients.
Finally, although no patient required conversion to total hip arthroplasty during follow-up, the relatively limited follow-up duration warrants cautious interpretation regarding long-term cartilage preservation.
Furthermore, the generalizability of these findings should be interpreted with caution. The present study included a relatively small, carefully selected cohort of patients undergoing hip arthroscopy for symptomatic FAI with acetabular wave signs. Therefore, the results may not be directly applicable to broader patient populations or to cases with more advanced cartilage degeneration.
Future investigations should focus on prospective comparative studies evaluating reverse drilling against other stabilization techniques—including fibrin adhesive fixation and chondrolabral repair—to better define the optimal treatment strategy for acetabular wave signs.
Clinical Relevance
Acetabular wave signs represent a challenging form of cartilage injury encountered during hip arthroscopy. The reverse-drilling technique described in this study may represent a minimally invasive approach to stimulate subchondral bone healing while preserving the intact cartilage surface. Although causal relationships cannot be established in the absence of a control group, the present findings suggest this technique can be performed safely and may be associated with favorable clinical evolution without evidence of additional cartilage deterioration at mid-term follow-up.
Conclusion
Reverse microfracture appears to be a safe surgical option for the treatment of acetabular wave signs. In this cohort, patients demonstrated significant improvement in clinical outcomes, reflected by substantial increases in HHS and reductions in VAS pain scores at follow-up. MRI performed 2 years after surgery showed preservation of cartilage morphology in the treated region, without evidence of cartilage thinning, structural deterioration, or recurrent delamination, suggesting potential restoration of cartilage adherence to the subchondral bone.
Although these findings are encouraging, the present results should be interpreted with caution due to the retrospective design and the absence of a control group. Further studies with larger patient cohorts, controlled comparative designs, and longer follow-up periods are necessary to better determine the durability and long-term clinical impact of this technique.
Footnotes
Appendix
Baseline Demographic and Clinical Characteristics a
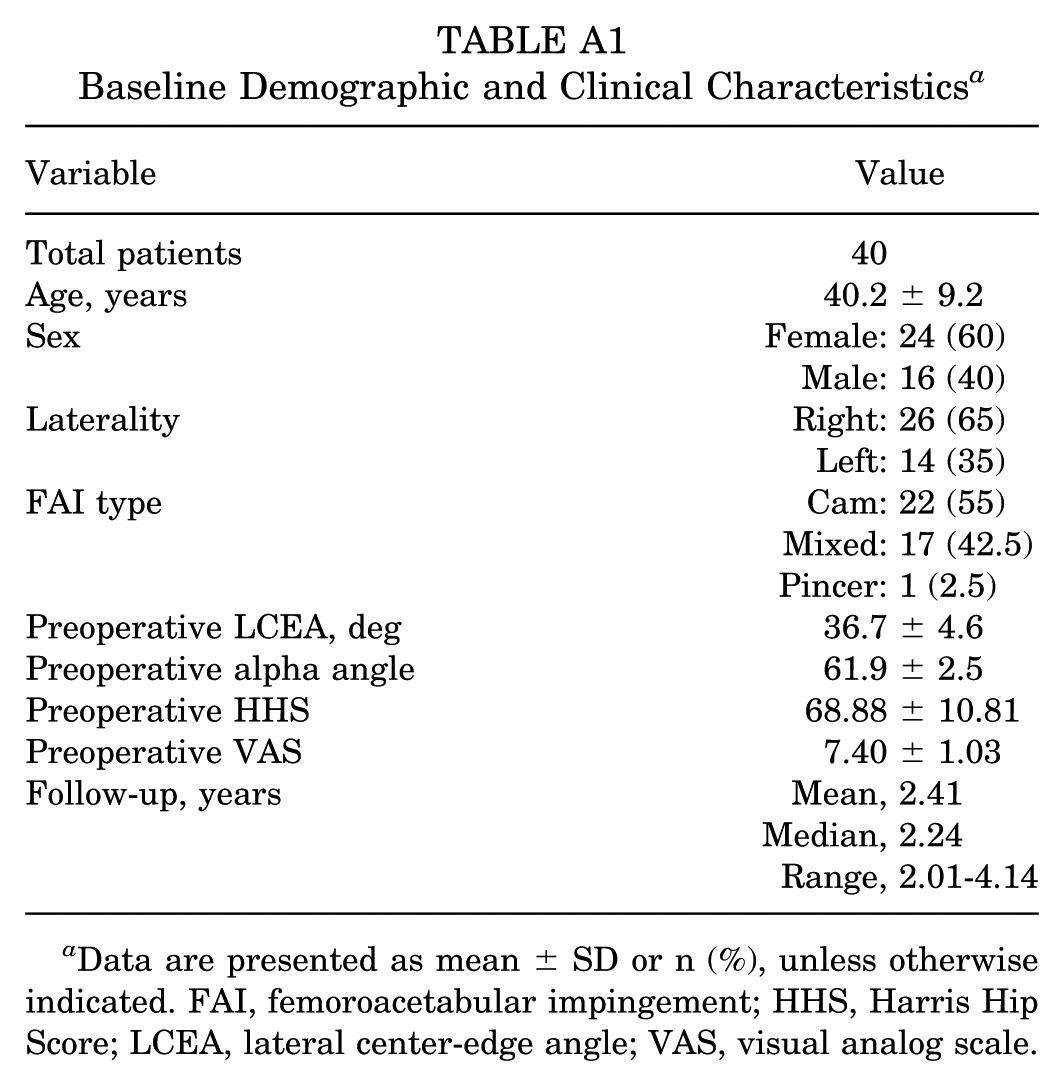
| Variable | Value |
|---|---|
| Total patients | 40 |
| Age, years | 40.2 ± 9.2 |
| Sex | Female: 24 (60) |
| Male: 16 (40) | |
| Laterality | Right: 26 (65) |
| Left: 14 (35) | |
| FAI type | Cam: 22 (55) |
| Mixed: 17 (42.5) | |
| Pincer: 1 (2.5) | |
| Preoperative LCEA, deg | 36.7 ± 4.6 |
| Preoperative alpha angle | 61.9 ± 2.5 |
| Preoperative HHS | 68.88 ± 10.81 |
| Preoperative VAS | 7.40 ± 1.03 |
| Follow-up, years | Mean, 2.41 |
| Median, 2.24 | |
| Range, 2.01-4.14 |
Data are presented as mean ± SD or n (%), unless otherwise indicated. FAI, femoroacetabular impingement; HHS, Harris Hip Score; LCEA, lateral center-edge angle; VAS, visual analog scale.
Acknowledgements
The authors would like to thank the Orthopaedic Residency Service and Radiology Service of Hospital São Lucas for their collaboration in analyzing the MRIs. The authors would also like to thank the multidisciplinary team involved in the clinical follow-up of patients.
Final revision submitted April 16, 2026; accepted April 27, 2026.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from Centro Universitário Padre Albino–UNIFIPA (reference No.: 7.085.450).