Abstract
Background:
Although the medial patellofemoral ligament (MPFL) has traditionally received the most attention as the primary patella stabilizer, other structures such as the medial patellotibial ligament (MPTL) contribute to patellar control, especially at higher flexion angles. Despite its clinical importance, the MPTL biomechanics and anatomic relationship to the physis remain poorly defined.
Hypothesis:
1) The MPTL will exhibit age-dependent variation in its insertional anatomy and relationship to the physis in skeletally immature knees.
2) Biomechanical testing of MPTL will demonstrate consistent properties across pediatric specimens.
Methods:
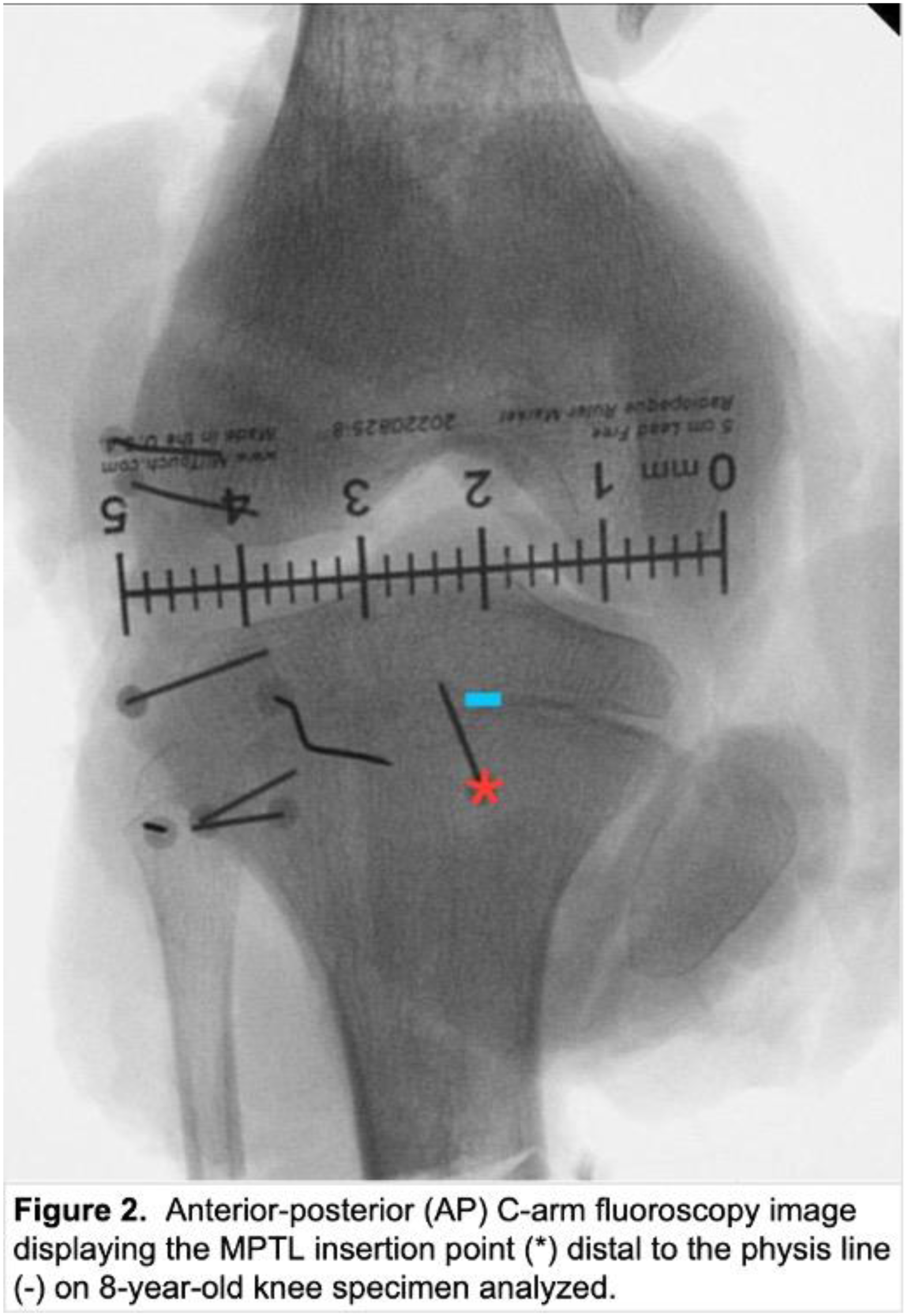
Seven fresh-frozen pediatric cadaveric knees (ages 8–16) underwent stepwise dissection to assess dimensional measurements and identify MPTL origins and insertions. C-arm fluoroscopy was used to evaluate the relationship between the MPTL tibial insertion to the physis. The MPTL was isolated and tested through preconditioning, cyclic loading (500 cycles, 10–30 N), and pull-to-failure (100 mm/min). Displacement, stiffness, and maximum load were recorded. Data was summarized using descriptive statistics.
Results:
Average MPTL length was 27.1 ± 9.9 mm and thickness 4.1 ± 1.3 mm. Widths were 9.5 ± 3.2 mm at patellar origin, 9.2 ± 3.0 mm at midpoint, and 8.1 ± 1.8 mm at tibial insertion. MPTL insertion was distal to the tibial physis in 6 out of the 7 specimens, with one specimen demonstrating insertion at the level of the physis. Physeal proximity was found to be 3.2 ± 1.4 mm on fluoroscopy lateral view and 6.1 ± 2.1 mm on anterior-posterior view.
The MPTL had an average failure load of 90.9 ± 23.8 N. Cyclic elongation at 30 N was 1.0 ± 0.9 mm, and stiffness was 50.2 ± 19.4 N/mm. Failures most frequently occurred at the tibial insertion or involved both the tibial and patellar insertions, and mode of failure involved true ligamentous tear.
Conclusion:
The MPTL consistently demonstrated insertion distal to the tibial physis, with one specimen showing insertion at the level of the physis. Furthermore, the MPTL was found to have substantial native strength in skeletally immature knees. These findings support the anatomic and biomechanical considerations of MPTL reconstruction for patella stabilization. These data can support reconstructive strategies that avoid physeal injury and inform graft options that meet or exceed the biomechanical performance of the native MPTL.