Abstract
Background:
Extensive research has been conducted to develop and optimize standardized return-to-play (RTP) tests following anterior cruciate ligament reconstruction (ACLR) [1]. However, objective functional tests are lacking for determining RTP readiness in individuals with patellofemoral instability following medial patellofemoral ligament reconstruction (MPFLR) [2].
Hypothesis:
To assess differences in movement strategy during sport-like tasks between individuals following an ACLR versus MPFLR at the time of RTP clearance. It was hypothesized that significant differences would be observed between the ACLR and MPFLR groups.
Methods:
Individuals following unilateral ACLR or MPFLR were tested in a motion capture lab upon clinical clearance for RTP. They completed six tasks outlined in the PRiSM Protocol [3]: heel touch (HT), drop vertical jump (DVJ), single leg hop (SLH), lateral shuffle (LSH), forward deceleration (DEC), and run cut (CUT). Kinematic and kinetic thresholds were used to calculate movement strategy scores across five different categories (Hip Stability, Pelvic Stability, Trunk Stability, Shock Absorption, and Hip Strategy) for the affected and unaffected limbs. Total scores for each movement category were computed. Individual category scores and cumulative task scores were reported as percentages of total possible points. Scores ≥90% were classified as high quality, while scores <70% were classified as low quality. Group differences were assessed using Mann-Whitney U tests (α=0.05).
Results:
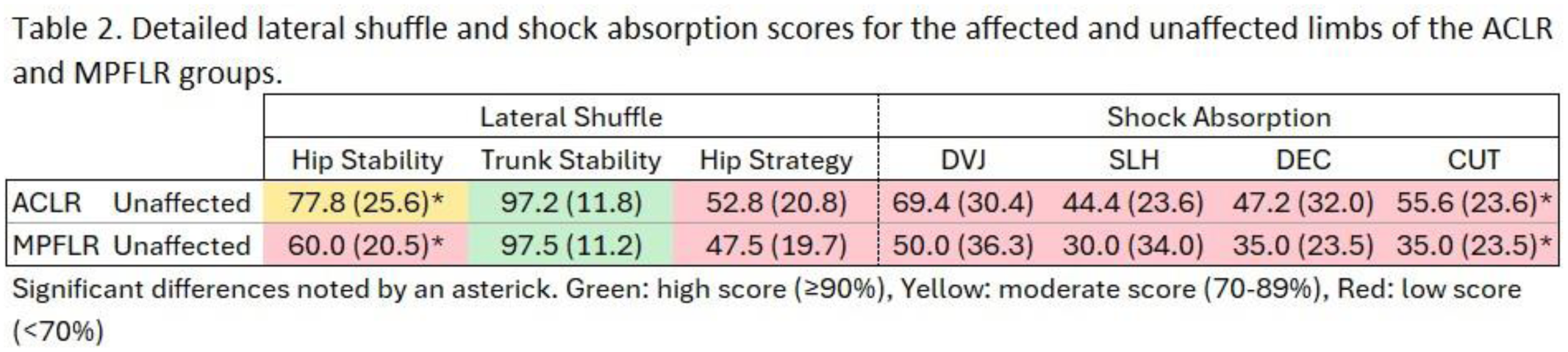
Eighteen patients were included in each group (ACLR: 10 female, 15.0±1.8 years, 11.0±2.2 months to RTP; MPFLR: 10 female, 15.0±1.4 years, 5.9±1.1 months to RTP). No differences were observed between groups for overall scores or movement quality categories for the affected limb (Table 1). However, for the unaffected limb, the MPFLR group demonstrated lower scores during the LSH compared to the ACLR group (ACLR: 75.9%, MPFLR: 68.3%), along with reduced shock absorption across all tasks (ACLR: 54.2%, MPFLR: 37.5%). Further analysis of the LSH task revealed reduced hip stability in the MPFLR group (ACLR: 77.8%, MPFLR: 60.0%) with no group differences in trunk stability or hip strategy (Table 2). Within the shock absorption category, scores during the CUT were lower for the MPFLR group (ACLR: 55.6%, MPFLR: 35.0%) with no differences in the DVJ, SLH, and DEC tasks.
Conclusion:
Findings highlight subtle but meaningful movement deficits in the unaffected limb of individuals following MPFLR compared to ACLR patients, particularly in tasks requiring hip stability and shock absorption. Clinically, this suggests that patients following MPFLR may benefit from targeted neuromuscular training focusing on bilateral hip control and dynamic loading mechanics.