Abstract
Background:
Current guidelines on when patients with adolescent idiopathic scoliosis (AIS) can return to sports after posterior spinal fusion (PSF) are limited and subjective. While a PSF may optimize standing balance, it is unknown how the resultant loss in trunk range of motion (ROM) after fusion might affect dynamic tasks required for evaluation of return-to-sport (RTS) readiness for this population. Motion capture-based RTS testing is a useful tool to quantitatively identify movement deficits that have been shown to lead to injury. However, no study to date has evaluated patients with AIS pre- and post-surgery using this technique.
Hypothesis:
The study’s purpose is to evaluate RTS readiness in athletes with AIS. We hypothesized that after PSF, RTS test scores, trunk motion during RTS tasks, and patient-reported outcomes would be reduced compared to preop levels.
Methods:
AIS (age range: 10 to 18 years) patients who compete in sports at a competitive level were enrolled. Patients completed a motion capture-based RTS test developed by the PRISM research interest group as well as the PROMIS Peer, Pain, and Mobility surveys before PSF and six months postop. For the RTS test, athletes performed six dynamic sports tasks (heel touch, side-step cut, lateral shuffle, deceleration, single hop and drop jump) while trunk/lower-body kinematics and ground-reaction forces were collected. Various biomechanics metrics were computed and used in the custom scoring algorithm established by PRISM. RTS scores, RTS biomechanics metrics, and PROMIS scores were compared pre- and postop with a paired t-test.
Results:
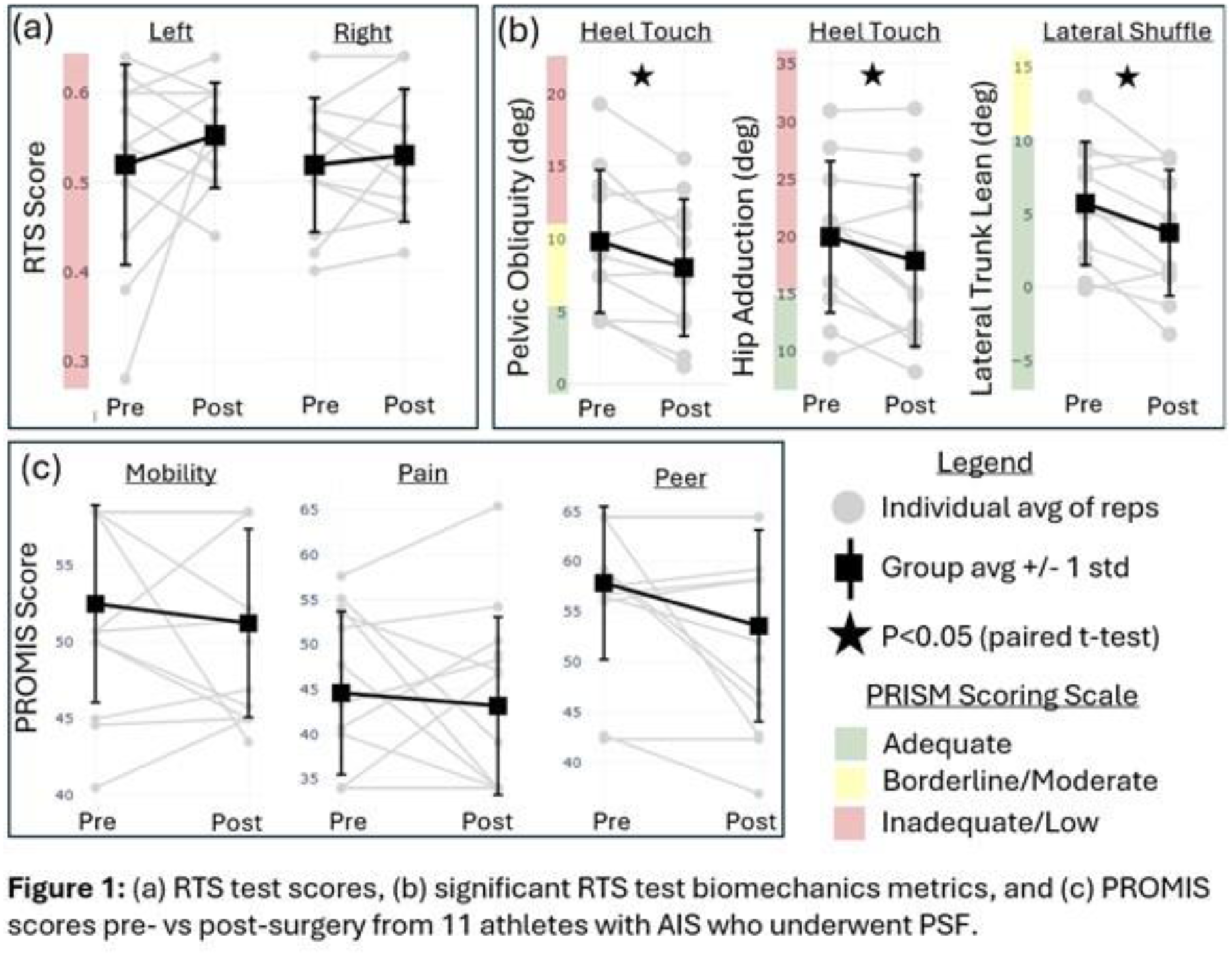
Eleven patients (1 male, 10 females; 14.5 +/- 1.8 years) were included in the analysis. There was no significant difference between the overall RTS score preop vs. postop (5 patients improved, 5 patients worsened, and 1 remained unchanged) (Fig. 1a). Patients performed the left-sided heel touch with significantly reduced pelvic obliquity and hip adduction, and the right-sided lateral shuffle with significantly reduced lateral trunk lean (Fig. 1b). No other metrics for any task were significantly different preop vs. postop. PROMIS scores (mobility, pain, and peer) were reduced but not statistically different preop vs. postop (Fig 1c).
Conclusion:
The reduced pelvic obliquity and lateral trunk lean during select tasks may be due to the lost ROM from PSF. However, these changes were not significant across metrics or tasks for this small cohort. With a larger population (goal N = 40), analyses for factors of lost ROM, lowest instrumented vertebra, and sport might further elucidate results.