Abstract
Background:
Minimal clinically important differences (MCID) have been established for adult questionnaires administered following anterior cruciate ligament reconstruction (ACLR) and medial patellofemoral ligament reconstruction (MPFLR), but MCID remains unquantified in pediatric-specific patient-reported outcome (PRO) instruments [1,2].
Hypothesis:
We hypothesized that MCIDs could be established for the HSS Pedi-FABS, Pedi-IKDC, and pediatric and parent-proxy PROMIS pain interference, mobility, and physical activity scores in pediatric patients who underwent primary knee surgery.
Methods:
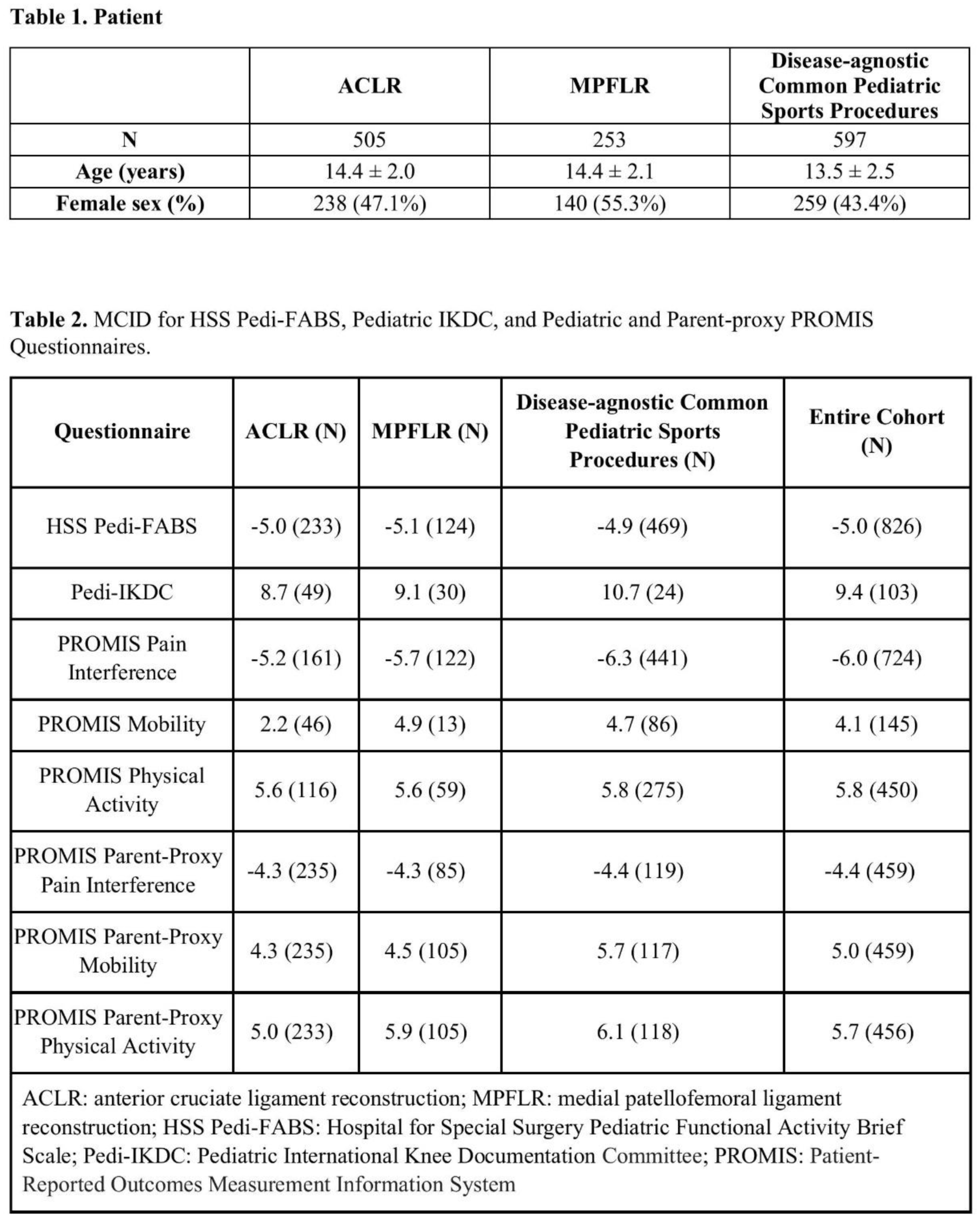
Patients <18 years who underwent surgery with one of two pediatric orthopedic surgeons between 2016-2023 were retrospectively reviewed. Demographic and clinical factors were collected. Available preoperative and postoperative HSS Pedi-FABS, Pedi-IKDC, and pediatric and parent-proxy PROMIS PI, physical activity, and mobility questionnaire scores were collected. MCID was determined using the distribution-based method: MCID was calculated as half the standard deviation of preoperative scores in patients undergoing ACLR, MPFLR, and other common procedures. The MCID for each outcome measure was also calculated for the entire cohort to serve as a standard reference for future research. Negative MCID was reported for pediatric PROMIS PI since a lower postoperative score compared to preoperative score denotes an improvement in pain. A negative MCID was reported for the HSS Pedi-FABS because it measures function at the patient’s healthiest, preinjury state. Therefore, a successful outcome typically reflects a return to preinjury activity levels rather than a postoperative score increase.
Results:
505 patients underwent ACLR, 253 patients underwent MPFLR, and 597 patients underwent other common pediatric sports procedures (Table 1). Meniscus repair and osteochondritis dissecans surgeries were most common in this group (20.9% and 18.9%, respectively). For all groups, MCID was established for HSS Pedi-FABS, Pedi-IKDC, PROMIS pain interference, mobility, and physical activity, and PROMIS Parent-proxy questionnaires (Table 2).
Conclusion:
MCID has been reported for adult knee questionnaires. However, studies on pediatric knee injuries have used adult knee questionnaires and MCIDs calculated from adult questionnaires, which may not be appropriate for younger patients. This study establishes novel MCID values for HSS Pedi-FABS, Pedi-IKDC, and pediatric and parent-proxy PROMIS PI, physical activity, and mobility questionnaires in pediatric patients undergoing ACLR, MPFLR, and other common procedures for conditions such as meniscus injury, knee articular damage, and osteochondritis dissecans. MCID for pediatric-specific knee questionnaires provides pediatric-specific thresholds for achievement of postoperative MCID and will inform power calculations when designing prospective studies on pediatric knee injuries.