Abstract
Background:
Osteochondritis dissecans (OCD) of the knee is a challenging condition for adolescent athletes, often requiring surgery or months of non-surgical treatment, with unpredictable healing rates and timing for return to sport.
Hypothesis:
The hypothesis was that diagnosis / treatment recommendations for knee OCD would be associated with increased levels of psychological stress, anxiety, depression, and symptoms of post-traumatic stress disorder (PTSD) in adolescents that persist for more than 3 months.
Methods:
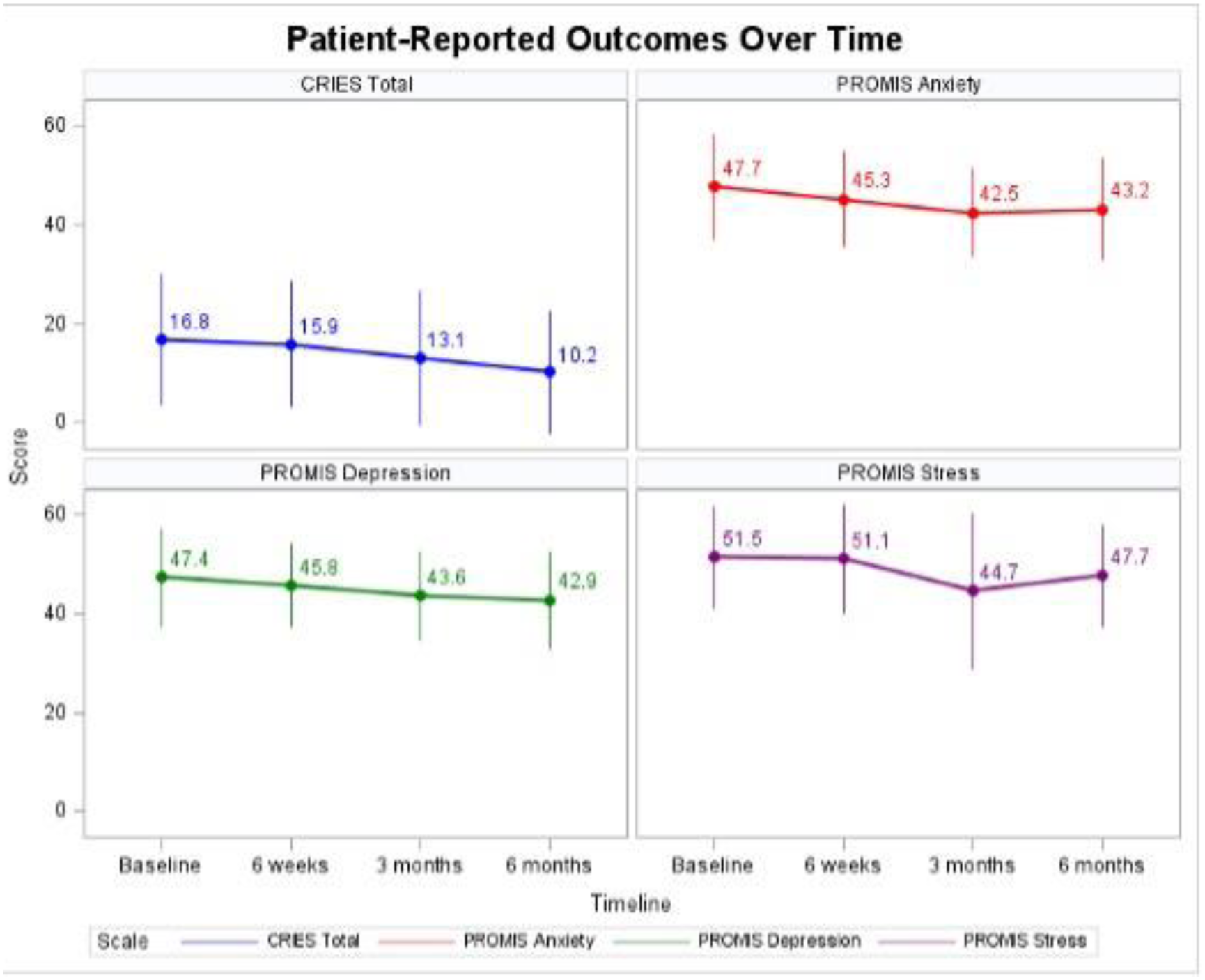
Patients aged 11-19 years were prospectively enrolled at the time of knee OCD diagnosis/consultation for definitive treatment at two pediatric orthopedic sports medicine centers. Patient reported outcomes (PROs) included Children’s Revised Impact of Events (CRIES), in which a value of > 30 is indicative of PTSD symptoms, PROMIS Psychological Stress Experiences (PSE), PROMIS Depression, PROMIS Anxiety, IKDC, KOOS, and Pedi-FABS. PROs at enrollment, 6 weeks, 3 & 6 months post-treatment initiation were summarized and compared across sex, and PROMIS measures were compared to the established normative score of 50.
Results:
Amongst 124 participants (median age 13.0 years, 68% male), 15% of patients scored >30 on the CRIES measure. These patients with PTSD symptoms had significantly poorer PROMIS-PSE, PROMIS Depression, PROMIS Anxiety, and IKDC scores at time of treatment initiation, with PROMIS-Depression and Anxiety remaining significantly poorer than patients without initial PTSD symptoms at 6 months.
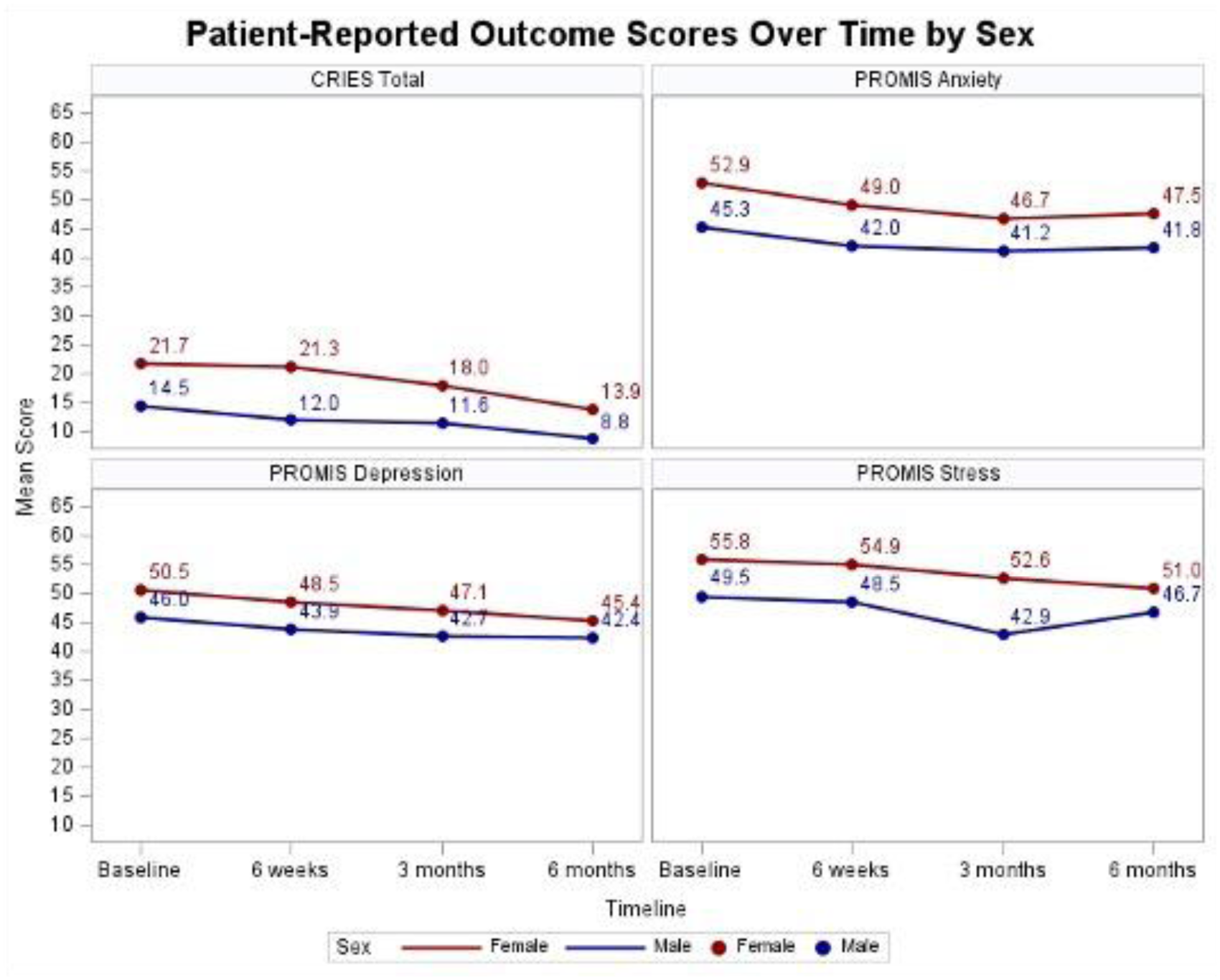
At enrollment, females had poorer median psychological stress score than males (55 vs 50; p=0.01) and the normative mean (p=0.008). Female anxiety scores (median 53) were poorer than males (median 46; p<0.001). Males had a significantly better depression score (median=44) compared to normative means (p=0.006).
No significant differences were detected across sex in KOOS, IKDC, or Pedi-FABS scores at initiation of treatment.
By 6 months, 60% of participants experienced improvement in PROMIS Stress scores. 57% experienced improvement in PROMIS Depression and Anxiety scores.
By 6 months, previously noted sex-based differences in the full cohort in PROMIS-PSE, Depression, Anxiety, and CRIES were no longer statistically significantly different.
Conclusion:
The stress/anxiety from the diagnosis/treatment associated with knee OCD varies amongst adolescents. 15% of adolescents reported PTSD symptoms and had increased anxiety and depressive symptoms with slower recovery at follow up compared with peers. Females report more stress, anxiety, and PTSD symptoms when diagnosed with knee OCD but these parameters become similar between sexes by 6 months. Follow up data from this study will help delineate if short-term psychological factors can predict differences in treatment outcomes.